
Abstract
Caffeine has been shown to reverse some of the performance-impairing effects of ethanol. However, it is not known whether this antagonistic effect of caffeine is mediated by a reduction in sleepiness. The present study assessed physiological alertness/sleepiness, memory, and psychomotor performance following the administration of placebo, ethanol, and caffeine+ethanol combinations. A total of 13 healthy individuals (21–35 years old) underwent four conditions presented in a Latin Square Design: placebo–placebo, ethanol (0.5 g/kg)–placebo, ethanol (0.5 g/kg)–caffeine 150 mg, and ethanol (0.5 g/kg)–caffeine 300-mg. The Multiple Sleep Latency Test (MSLT), psychomotor performance battery, memory test, and mood/sleepiness questionnaires were administered following each condition. The peak breadth ethanol concentration (BrEC) was 0.043±0.0197% and did not differ among the three caffeine treatments. As expected, ethanol reduced mean latency on the MSLT. The lowest caffeine dose reversed this effect and the highest dose increased mean latency (greater alertness) significantly beyond placebo levels. Ethanol also impaired psychomotor performance and memory. The 300-mg caffeine dose restored performance and memory measures to placebo levels. Although visual analog ratings of dizziness were increased by ethanol, they were not diminished by either caffeine dose. In conclusion, Low-dose caffeine prevented the sleepiness and performance impairment associated with a moderate dose of ethanol. Thus, caffeine, similar to other stimulants, can reverse the physiologically sedating effects of ethanol, although other negative effects remain.
Similar content being viewed by others


INTRODUCTION
The sedating and performance-impairing effects of ethanol are well documented (Roehrs and Roth, 2001). Even low to moderate doses of ethanol (0.2–0.6 g/kg) can produce significant performance decrements such as slowed reaction time, decreased attention, and impaired driving (Moskowitz et al, 1985; Roehrs et al, 1989,1992; Roehrs et al, 1994a; Arnedt et al, 2000,2001; Weiler et al, 2000). The Multiple Sleep Latency Test (MSLT; Carskadon et al, 1986) is a commonly used measure for the assessment of physiological sleepiness and it has been used in a number of studies to assess the sedative effects of ethanol. Sleepiness on the MSLT is determined by averaging the latency to electroencephalographically defined sleep on a series of 4–5 standardized nap opportunities equally spaced throughout the day (Carskadon et al, 1986). The increased sensitivity, rigorous standardization, and objectivity of the MSLT provide advantages over subjective measures of sleepiness (Carskadon and Dement, 1987; Drake et al, 2001). Ethanol has been shown to increase objectively measured sleepiness (antonym to alertness) on the MSLT and it does so in a dose-dependent manner (Williams et al, 1983; Zwyghuizen-Doorenbos et al, 1988; Arnedt et al, 2001). The temporal pattern of the sedative effects of ethanol has also been studied (Nicholson et al, 1992). Specifically, during the first ∼1.5 h postconsumption (on the rising phase of BrECs) ethanol produces physiological alertness (Papineau et al, 1998). However, 2–6 h postconsumption ethanol's sedative effects become apparent with significant reductions in physiological alertness even after BrECs are near zero (Papineau et al, 1998; Roehrs et al, 1992, 1994b). In addition, ethanol-related decrements in alertness and performance can carry over into the following day even after moderate doses and in the absence of hangover effects (Roehrs et al, 1994b). The sedative effects of ethanol are thought to result, in part, from the stimulation of inhibitory GABA receptors as well as the antagonism of glutamate's NMDA receptor subtype (Roehrs and Roth, 2001).
The effects of caffeine on sleepiness and performance have also been widely studied. In contrast to ethanol, low-dose caffeine (75–250 mg) has been shown to have alerting and performance-enhancing effects in normal and sleep-deprived individuals (Johnson et al, 1990a,1990b; Walsh et al, 1990; Zwyghuizen-Doorenbos et al, 1990; Kerr et al, 1991; Rosenthal et al, 1991; Hasenfratz et al, 1993; Penetar et al, 1993; Bonnet and Arand, 1994a,1994b; Bonnet et al, 1995; Wright et al, 1997a,1997b; De Valck and Cluydts, 2001; Kruk et al, 2001; Van Dongen et al, 2001). Specifically, caffeine can improve auditory vigilance (Zwyghuizen-Doorenbos et al, 1990), and has been shown to increase MSLT scores substantially (Zwyghuizen-Doorenbos et al, 1990; Rosenthal et al, 1991). While the specific mechanism(s) of caffeine's effects on alertness and performance are still being investigated, increased plasma catecholamines (Nehlig et al, 1992; Kamimori et al, 2000), adenosine A(2A) receptor blockade (Basheer et al, 2000; El Yacoubi et al, 2000; Van Dongen et al, 2001) and effects on circadian rhythms (Pelissier et al, 1999; Wright et al, 2000; Antle et al, 2001) have all been implicated. Studies have shown that caffeine can facilitate performance and improve subjective and physiological measures of alertness during prolonged sleep deprivation (Penetar et al, 1993; Bonnet and Arand, 1994a,1994b; Bonnet et al, 1995; Horne and Reyner, 1996; Sicard et al, 1996; Reyner and Horne, 1997; Wright et al, 1997a,1997b; Kamimori et al, 2000; De Valck and Cluydts, 2001; Van Dongen et al, 2001). In addition, several studies have assessed the ability of caffeine to reverse the performance and alertness-impairing effects of benzodiazepines (Mattila and Nuotto, 1983; Roache and Griffiths, 1987; Johnson et al, 1990a,1990b).
As both caffeine and ethanol are among the most widely used drugs in modern society, studies have investigated the combined effects of these substances on several physiological and behavioral measures (Franks et al, 1975; Nuotto et al, 1982; Oborne and Rogers, 1983; Kerr et al, 1991; Hasenfratz et al, 1993; Marsden and Leach, 2000). Several studies have found that caffeine can reverse many of the performance-impairing effects of ethanol (Franks et al, 1975; Kerr et al, 1991; Hasenfratz et al, 1993; Azcona et al, 1995; Liguori and Robinson, 2001). Although some studies of the effects of caffeine on alcohol-induced impairment have not found caffeine to reverse performance deficits (Nuotto et al, 1982; Oborne and Rogers, 1983), differences in basal caffeine intake, dosages, sample size and the specific tasks measured are likely to be responsible for the discrepancies. In a recent study of caffeine antagonism of ethanol effects on driving, caffeine attenuated the impairing effects of ethanol on ‘brake latency’, but performance impairment on a choice reaction time task was unaffected. Moreover, while impairment was attenuated, ‘brake latency’ deficits remained in comparison to placebo, indicating that caffeine up to 400 mg was unable to fully counteract driving impairment induced by ethanol (0.6 g/kg) (Liguori and Robinson, 2001). Another study found that a high dose of caffeine (400 mg) reversed the impairment of simple reaction time induced by a moderate dose of ethanol (Azcona et al, 1995). However, in that study the subjective feeling of ‘tiredness’ and ‘drunkenness’ remained despite the performance reversal. It is not known whether daytime sleepiness was present along with these subjective feelings of tiredness as no standardized measures of sleepiness were administered. It could be argued that subjective measures of alertness may be contaminated by feelings of ‘drunkenness’ in such studies. Therefore, the use of objective measures of sleepiness such as the MSLT are necessary to determine if physiological sleepiness induced by ethanol can be reversed with caffeine.
Many of the ethanol effects that are reversed with caffeine such as reductions in psychomotor vigilance, slowed reaction time and memory impairment are also influenced by manipulations of sleepiness (Drake et al, 2001). In contrast, other effects of ethanol such as dizziness/drunkenness (Azcona et al, 1995), body sway/steadiness (Franks et al, 1975; Nuotto et al, 1982; Liguori and Robinson, 2001) and increased risk-taking (Greenwald et al, 1999) that are not reversed by caffeine may be unrelated to sleepiness. This pattern of results along with caffeine's known alerting effects suggests that caffeine may reverse ethanol–induced impairment in performance through its effects on sleepiness. At present, the degree to which caffeine reverses ethanol effects through a reduction in sleepiness is unknown, as previous studies of ethanol-caffeine interactions have not employed standardized measures of physiological sleepiness such as the MSLT. We hypothesized that caffeine would be able to reverse the physiological sleepiness induced by a moderate dose of ethanol and that it will do so in a dose-dependent manner.
METHOD
In all, 13 healthy individuals (seven females, six males) aged 21–35 years (mean 27.5±5.4 years) were studied. Participants were required to be free from medical or psychiatric disease as determined by physical exam and clinical evaluation, body mass index between 19.8 and 27.5, with a total caffeine consumption of <150 mg/day, alcohol consumption of <14 drinks per week, and no history of drug or alcohol abuse. Participants were also required to pass a urine drug screen and a medical evaluation (tests included: liver function, electrolytes, cholesterol, glucose, triglycerides, kidney, urinalysis, hematology, blood chemistries and a pregnancy test) prior to experimental procedures. Individuals using central nervous system acting drugs or scoring outside the normal range (T score >70) on the Minnesota Multiphasic Personality Inventory (clinical scales excluding M-F) or the Cornell Medical Index were excluded. In addition, participants were required to have nocturnal sleep times of 7–8 h per night, sleep latencies of <30 min, consistent bedtimes and rise times (not varying night to night by >2 h over a 1-week period), and no habitual napping. Participants were instructed to maintain their regular bedtimes and rise times for 1 week before and throughout the study period (including between laboratory intervals). All had normal sleep on an 8-h nocturnal polysomnogram (see the screening section below) and an average daily sleep latency on the MSLT of 8–14 min. The hospital's Institutional Review Board approved study procedures. All participants provided written informed consent and were paid for their participation.
Participants reported to the laboratory at 2200 h and were screened within 1 month of beginning the study using an 8-h nocturnal polysomnogram that was scheduled close to self-reported bedtimes and waketimes (2300–0700). Recordings included electroencephalograms (C3, C4, and OZ referenced to mastoid), two electro-oculograms (EOG; bilateral horizontal), submental electromyogram (EMG) and electrocardiogram (V5 lead), and were scored in 30-s epochs according to standard procedures (Rechtschaffen and Kales, 1968). In addition, leg movements were monitored with a tibialis EMG and respiration with a nasal/oral thermistor. Recordings were made using Grass model 78-D or Nihon Kohden (models 4312 and 4212) polygraphs. All electrode impedances were <10 000 Ω and the paper speed was 10 mm/s. There was no evidence of clinically significant apnea/hypopnea (apnea hypopnea index >10) or periodic leg movements during sleep (>10 h−1) for any of the participants.
At screening, participants were tested using a five-trial (0930, 1130, 1330, 1530, and 1730 h) MSLT that was administered and scored according to standard criteria (Carskadon et al, 1986). In accordance with standard procedures, sleep latency was scored as the time from the start of the MSLT to the first epoch of any stage of sleep. Each sleep latency test was discontinued following three consecutive epochs of stage 1 sleep or one epoch of any other stage of sleep. Each participant was required to have a sleep efficiency >85% at screening and an average daily MSLT sleep latency of 8–14 min. The MSLT range was used to exclude individuals in the upper and lower quartiles of MSLT latency in order to maintain a more representative study sample with respect to physiological sleepiness (Drake et al, 2002). All participants were practiced on each of the performance tasks twice at screening in order to minimize the possibility of practice effects. A total of 12 individuals were excluded from participation due to polysomnographic exclusionary criteria.
Protocol
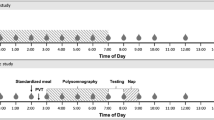
Participants arrived ∼1 h prior to their scheduled bedtime (2300 h) for the attachment of electrodes and preparation for polysomnographic recording. Bedtime was set at 2300 h and wake time was set at 0700 h. Recordings proceeded according to standardized screening procedures as above. On each study day after awakening, participants were given a breakfast consisting of a roll and orange juice to standardize stomach content and minimize differences in ethanol absorption rate. Participants underwent each of four conditions presented in a Latin Square Design: placebo–placebo, ethanol (0.5 g/kg)–placebo, ethanol (0.5 g/kg)–caffeine 150 mg, and ethanol (0.5 g/kg)–caffeine 300 mg. The study was performed in a double-blinded manner. Figure 1 provides a graphical representation of the study timeline during each experimental day. On each of four mornings following an 8-h time-in-bed, placebo or ethanol was administered at 0900–0930 h and at 0900 h a caffeine or placebo capsule was given (identical capsules prepared by the hospital pharmacy). The ethanol used was 80-proof vodka, mixed at a 1:4 ratio with carbonated tonic water, and served with 1 oz of either lemon or lime juice per participant preference. Placebo and ethanol beverage volumes were identical. The placebo beverage was masked with 4–5 drops of ethanol. The ethanol dose was equivalent to three 12-oz US beers for a 150-lb person. Generally, participants took the entire 30 min to consume the study beverage. During the study, participants were instructed to avoid all caffeinated or alcoholic beverages other than the study beverage provided for them in the laboratory as described above. BrECs were measured at 0945, 1145, 1345, and 1545 h using an Alco-Sensor III (Intoxometers, Inc., Richmond) calibrated weekly. MSLT trials were performed at 1000, 1200, 1400, and 1600 during each study day. Each MSLT was performed according to standardized criteria (see the screening section).

Timeline of experimental manipulations and daytime testing during each condition.
Performance Assessments
During the probed-recall memory (PRM) task, participants were exposed to a written list of four word-pairs for 30 s. After 15 min participants were provided with one of the words in each pair and asked to recall the paired words within a 30s time limit. Performance was measured as number correct per trial. A previous study has found this task to be sensitive to the effects of sleep deprivation (Dinges et al, 1997).
Participants completed a divided attention task at 1030 and 1430 h on each testing day. This 15-min task required participants to track a moving target across a video screen using a joystick while simultaneously responding with a button press (non dominant index finger) to the appearance of stimuli in the center of the target or periphery of the screen. A total of 52 stimuli were presented at random intervals throughout each task period. Dependent measures for this task were reaction time (sec) to central and peripheral stimuli and tracking deviations measured in pixels.
Subjective Measures
The Profile of Mood States (POMS) was administered at 1030 and 1430 h each day in order to assess subjective sleepiness, and mood effects. The POMS is a validated measure that has been used in numerous studies evaluating the effects of sleep loss and pharmacological challenges on mood and performance (Bishop et al, 1997; Dinges et al, 1997; Wright et al, 1997a,1997b; Roehrs et al, 1999). Mean T-scores for each standard POMS scale (fatigue/inertia, vigor/activity, confusion/bewilderment, tension/anxiety, anger/hostility, depression/dejection) were calculated for each study day. A visual analog scale was also used to assess the subjective effects of ethanol and caffeine (ie, dizziness, energy, stimulated, high, jittery). Finally, the Stanford Sleepiness Scale was used as an additional measure of subjective sleepiness (Hoddes et al, 1972).
Statistical Analyses
Repeated measures analysis of variance (ANOVA) using the General Linear Model function of Systat, version 9.0 for PC (SPSS, Inc., Chicago, III) was used to test differences between conditions. Planned comparisons using contrasts for repeated measures designs were performed where significant omnibus-F values were found. The examination of contrasts was made contingent upon a significant omnibus-F value in order to decrease the probability of Type I error given the multiple measures assessed. Specifically, three comparisons were performed for measures with a significant omnibus F: (1) a comparison between placebo and ethanol to determine the presence of ethanol effects at the dosage used, (2) a comparison of placebo to ethanol+caffeine (150-mg) and (3) a comparison of placebo to ethanol+caffeine (300-mg). Post hoc trend analyses were performed on measures where significant ethanol effects were detected in order to examine the consistency of patterns of change across measures with increased caffeine doses. Log-base 10 or reciprocal transformations were performed on data when frequency distributions differed from normality (MSLT and tracking deviations). Raw data are presented in the table and figures. Morning and afternoon data were analyzed separately for performance, memory and subjective measures. ‘Reversal of ethanol effects,’ was operationally defined as a comparison where ethanol effects that were previously significantly different from placebo were not significantly different from placebo with the addition of a given caffeine dose.
RESULTS
MSLT Alertness and BrEC
Mean BrEC±SD was 0.043±0.0197% at 0945 h, declined to 0.024±0.0135% at 1145 h, and reached 0.0 by 1345 h. BrEC did not differ in the three caffeine treatments. Means and SDs for each dependent measure across the four conditions are presented in Table 1 (objective measures) and Figure 2. As expected, ethanol alone reduced mean latency on the MSLT when compared to the placebo condition (p<0.05). There was no significant difference between the placebo and ethanol+caffeine (150 mg) conditions, indicating that the lowest caffeine dose reversed the effect of ethanol on the MSLT. The combination of ethanol and the highest dose (300 mg) increased mean latency (reduced sleepiness) significantly beyond placebo levels (p<0.05) (Table 1 and Figure 2). Caffeine also reversed the effects of ethanol on the MSLT in a dose-related manner as evidenced by a significant primary linear polynomial trend (p<0.05). Thus, each dose of caffeine incrementally and linearly improved physiological alertness above levels induced by ethanol.

Means±SE for placebo (PLAC), ethanol (ETOH) and ethanol+caffeine (ETOH Caf 150; ETOH Caf 300) conditions. Daily mean is presented for the MSLT, and am data are presented for central reaction time (CRT), PRM (Memory), tracking deviations (Tracking), Stanford Sleepiness Scale (SSS), and subjective ratings of dizziness (Dizzy); asterisks indicate p<0.05 compared to placebo condition (repeated measures contrast, pairwise comparison).
Performance Measures
Means and SDs for each performance measure across the four conditions are presented in Table 1. Ethanol alone slowed down peripheral and central reaction time and impaired tracking on the divided attention task during the morning session when compared to the placebo condition (p<0.05 for all). No significant difference in reaction times (PRT or CRT) was found for the comparisons between the placebo and ethanol+caffeine (150 mg), or between placebo and ethanol+caffeine (300 mg), indicating that both caffeine doses eliminated the detrimental effects of ethanol on reaction time (Table 1 and Figure 2). Similar to the MSLT results, caffeine reversed the effects of ethanol on reaction time in a dose-related manner as evidenced by significant primary linear trends on both peripheral and central reaction time measures (p<0.05 for both).
Memory
Means and SDs for the PRM task across the four conditions are presented in Table 1. Accuracy on the memory task was impaired by ethanol alone during the morning testing session when compared to the placebo condition (p<0.05). The comparison between placebo and ethanol+caffeine (150 mg) was also significant (p<0.05), indicating that the lowest caffeine dose was unable to reverse the detrimental effect of ethanol on the recall memory task. No significant difference was found for the comparison between placebo and ethanol+caffeine (300 mg), indicating that the detrimental effect of ethanol on the recall task was eliminated by the highest caffeine dose (Figure 2). In addition, caffeine reduced the effects of ethanol in a dose-related manner as indicated by a significant primary linear trend across each of the three ethanol conditions for the morning trial of the PRM task (p<0.05). No effect of ethanol on memory was found during the 1430 h trial.
Subjective Measures
Significant omnibus-F values were obtained for five of the morning rating scales: Fatigue, F(3,36)=4.80, p<0.05; Dizzy, F(3,36)=3.87, p<0.05; Energy, F(3,36)=2.94, p<0.05; High, F(3,36)=3.15, p<0.05; and the Stanford Sleepiness Scale, F(3,36)=4.01, p<0.05. Comparisons revealed that ratings for each scale were significantly impaired by ethanol alone when compared to the placebo condition (p<0.05). The comparisons between placebo and ethanol+caffeine (150 or 300 mg) were not significant (p>0.05), indicating that both caffeine doses reversed the effects of ethanol on ratings of fatigue. Impairments on ratings of energy and subjective sleepiness on the Stanford Sleepiness Scale were also reversed by each caffeine dose (p>0.05). Caffeine reversed ethanol's effects on subjective sleepiness in a dose-related manner as evidenced by a significant linear (p=0.05) trend across each of the three ethanol conditions. Ratings of fatigue also showed a significant primary linear trend (p<0.05). Although visual analog ratings of dizziness were increased by ethanol (p<0.05), they were not diminished by either caffeine dose. None of the omnibus-F values were significant for the afternoon ratings (p>0.05 for all).
DISCUSSION
This is the first study to show that caffeine can reverse the sedative effects of moderate ethanol consumption and does so in a dose-related manner. Caffeine also reversed the effects of ethanol on recall memory. Similar to previous studies, caffeine reversed the performance-impairing effects of ethanol (Kerr et al, 1991; Hasenfratz et al, 1993; Azcona et al, 1995). The present study adds to the literature by demonstrating that the antagonistic effects of caffeine on ethanol-induced performance impairment extend to a standardized measure of daytime alertness and that the attenuations of performance deficits are present even with small doses of caffeine. The performance and memory measures assessed in the present study were selected based on their sensitivity to variations in physiological alertness (Drake et al, 2001). Caffeine's reversal of ethanol's effects on these measures provide evidence for the hypothesis that caffeine reverses ethanol-induced impairment through a reduction in sleepiness. The consistent linear dose-related effects of caffeine on alertness and performance measures following ethanol administration provide additional support for this possibility. These findings in conjunction with previous research that has demonstrated a reversal of ethanol-induced performance impairment with a short nap (Roehrs et al, 1993) suggest that the performance impairment associated with ethanol may be related to increased physiological sleepiness.
In contrast to the reversal of physiological sleepiness, reduced psychomotor performance, and memory impairment, some of the subjective effects of ethanol remained despite caffeine administration up to 300 mg. Although the operational definition of ‘drunkenness’ is not uniform throughout the literature, we considered the visual analog scales ‘dizziness’ and ‘high’ to be measures of drunkenness/intoxication. The low dose of caffeine reversed the ‘high’ associated with ethanol, whereas neither dose of caffeine impacted the subjective feeling of ‘dizziness’. Thus, caffeine similar to other stimulants (Stein et al, 1996; Bishop et al, 1997) appears to reverse some aspects of ‘drunkenness’, but other negative effects remain. These results are consistent with previous research on the interaction of similar caffeine and ethanol doses, where it has been demonstrated that caffeine can reduce some specific performance impairments induced by moderate ethanol consumption without reducing particular subjective effects (Liguori and Robinson, 2001).
While the specific mechanisms by which caffeine attenuates the performance and alertness-impairing effects of ethanol are unknown, pharmacodynamic rather than pharmacokenetic interactions have been proposed (Dar, 1988). Although caffeine is a benzodiazepine receptor antagonist, this property is only present at toxic levels of plasma caffeine (File et al, 1982) and cannot explain the effects observed in the present study. Recent research suggests that antagonism of adenosine A(2a) receptors (Pedata et al, 1984; Varani et al, 2000; Scammell et al, 2001) or an increase in sympathetic activation/catecholamines (Kamimori et al, 2000) may be involved.
It must be emphasized that, while the performance and sedative effects of moderate alcohol consumption were reversed with low-dose caffeine, other measures such as driving ability were not studied and thus generalization to such situations is unwarranted. Also, as in previous studies, feelings of ‘drunkenness’ remained after caffeine ingestion, indicating that specific negative effects of ethanol continued to be present and would clearly have the potential to adversely affect judgment and thus driving ability. Also, while ethanol adversely affected most measures, the dose used in the present study was in the low-to-moderate range and produced BrECs below the legal limit in most states. Additional studies using a range of ethanol doses are needed to determine the limits of caffeine's ability to reverse the sedative effects of ethanol. Finally, the modest effect of ethanol on MSLT latency (decrease of ∼2 min) observed in the present study suggests that our results pertain to the lower end of this continuum (ie, low-to-moderate ethanol impairment).
Similar to previous studies (Azcona et al, 1995; Kerr et al, 1991; Hasenfratz et al, 1993), the present results demonstrate caffeine antagonism of ethanol-induced impairment. Other studies have found only partial antagonism of ethanol's effects on performance (Burns and Moskowitz, 1989/90; Rush et al, 1993; Forney and Hughes, 1965; Franks et al, 1975; Nuotto et al, 1982; Oborne and Rogers, 1983; Liguori and Robinson, 2001). This discrepancy between studies may be related to the doses of each substance used, differences in prior habitual caffeine and/or ethanol intake of participants and the sensitivity of tests of impairment. One limitation of the present study is that only one dose of ethanol was used, and in previous studies where ethanol-induced impairment remained following caffeine intake, relatively higher doses of ethanol were administered. One significant strength of the present study is that habitual caffeine use history was carefully assessed and individuals who reported >200 mg/day were excluded from participation, thus reducing the variability in caffeine response between participants.
In the present study a moderate dose (0.5 g/kg) of ethanol produced impairments in alertness, memory, and performance similar to those seen in previous studies. However, following low (150 mg), and moderate (300 mg) doses of caffeine, many of these impairments were reversed, and in some cases measures of alertness improved (ie, MSLT). Despite this antagonistic effect of caffeine, a measure of the subjective effect of ethanol, ‘dizziness’, was unaffected by either caffeine dose. Thus, while caffeine is effective at reversing several of the specific effects of ethanol, other negative effects that may be unrelated to sleepiness remain. These results suggest that many of the performance impairments induced by moderate doses of alcohol may be due to increased physiological sleepiness.
References
Antle MC, Steen NM, Mistlberger RE (2001). Adenosine and caffeine modulate circadian rhythms in the Syrian hamster. Neuroreport 12: 2901–2905.
Arnedt JT, Wilde GJ, Munt PW, MacLean AW (2000). Simulated driving performance following prolonged wakefulness and alcohol consumption: separate and combined contributions to impairment. J Sleep Res 9: 233–241.
Arnedt JT, Wilde GJ, Munt PW, MacLean AW (2001). How do prolonged wakefulness and alcohol compare in the decrements they produce on a simulated driving task? Accid Anal Prev 33: 337–344.
Azcona O, Barbanoj MJ, Torrent J, Jane F (1995). Evaluation of the central effects of alcohol and caffeine interaction. Br J Clin Pharmacol 40: 393–400.
Basheer R, Porkka-Heiskanen T, Strecker RE, Thakkar MM, McCarley RW (2000). Adenosine as a biological signal mediating sleepiness following prolonged wakefulness. Biol Signals Recept 9: 319–327.
Bishop C, Roehrs T, Rosenthal L, Roth T (1997). Alerting effects of methylphenidate under basal and sleep-deprived conditions. Exp Clin Psychopharmacol 5: 344–352.
Bonnet MH, Arand DL (1994a). Impact of naps and caffeine on extended nocturnal performance. Physiol Behav 56: 103–109.
Bonnet MH, Arand DL (1994b). The use of prophylactic naps and caffeine to maintain performance during a continuous operation. Ergonomics 37: 1009–1020.
Bonnet MH, Gomez S, Wirth O, Arand DL (1995). The use of caffeine versus prophylactic naps in sustained performance. Sleep 18: 97–104.
Burns M, Moskowitz H (1989/90). Two experiments on alcohol–caffeine interaction. Alcohol Drugs and Driving 5/6: 303–315.
Carskadon MA, Dement WC (1987). Daytime sleepiness: quantification of a behavioral state. Neurosci Biobehav Rev 11: 307–317.
Carskadon MA, Dement WC, Mitler MM, Roth T, Westbrook PR, Keenan S (1986). Guidelines for the multiple sleep latency test (MSLT). a standard measure of sleepiness. Sleep 9: 519–524.
Dar MS (1988). The biphasic effects of centrally and peripherally administered caffeine on ethanol-induced motor incoordination in mice. J Pharm Pharmacol 40: 482–487.
De Valck E, Cluydts R (2001). Slow-release caffeine as a countermeasure to driver sleepiness induced by partial sleep deprivation. J Sleep Res 10: 203–209.
Dinges DF, Pack F, Williams K, Gillen KA, Powell JW, Ott GE et al (1997). Cumulative sleepiness, mood disturbance, and psychomotor vigilance performance decrements during a week of sleep restricted to 4–5 h per night. Sleep 20: 267–267.
Drake CL, Roehrs T, Burduvali E, Bonahoom A, Rosekind M, Roth T (2001). Effects of rapid versus slow accumulation of eight hours of sleep loss. Psychophysiology 38: 979–987.
Drake CL, Roehrs T, Richardson G, Roth T (2002). Epidemiology and morbidity of excessive daytime sleepiness. Sleep 25:92–93.
El Yacoubi M, Ledent C, Menard JF, Parmentier M, Costentin J, Vaugeois JM (2000). The stimulant effects of caffeine on locomotor behaviour in mice are mediated through its blockade of adenosine A(2A) receptors. Br J Pharmacol 129: 1465–1473.
File SE, Bond AJ, Lister RG (1982). Interaction between effects of caffeine and lorazepam in performance tests and self-ratings. J Clin Psychopharmacol 2: 102–106.
Forney RB, Hughes FW (1965). Effect of caffeine and alcohol on performance under stress of audiofeedback. Q J Stud Alcohol 26: 206–212.
Franks HM, Hagedorn H, Hensley VR, Hensley WJ, Starmer GA (1975). The effect of caffeine on human performance, alone and in combination with ethanol. Psychopharmacologia 45: 177–181.
Greenwald MK, Roehrs T, Turner L, Furcron E, Roth T (1999). Living on the edge: effects of ethanol, caffeine, and basal sleepiness on risk-taking behavior. Sleep 22: 8S88.
Hasenfratz M, Bunge A, Dal Pra G, Battig K (1993). Antagonistic effects of caffeine and alcohol on mental performance parameters. Pharmacol Biochem Behav 46: 463–465.
Hoddes E, Dement W, Zarcone V (1972). The development and use of the Stanford Sleepiness Scale (SSS). Psychophysiology 9: 150.
Horne JA, Reyner LA (1996). Counteracting driver sleepiness: effects of napping, caffeine, and placebo. Psychophysiology 33: 306–309.
Johnson LC, Spinweber CL, Gomez SA (1990a). Benzodiazepines and caffeine: effect on daytime sleepiness, performance, and mood. Psychopharmacology 101: 160–167.
Johnson LC, Spinweber CL, Gomez SA, Matteson LT (1990b). Daytime sleepiness, performance, mood, nocturnal sleep: the effect of benzodiazepine and caffeine on their relationship. Sleep 13: 121–135.
Kamimori GH, Penetar DM, Headley DB, Thorne DR, Otterstetter R, Belenky G (2000). Effect of three caffeine doses on plasma catecholamines and alertness during prolonged wakefulness. Eur J Clin Pharmacol 56: 537–544.
Kerr JS, Sherwood N, Hindmarch I (1991). Separate and combined effects of the social drugs on psychomotor performance. Psychopharmacology 104: 113–119.
Kruk B, Chmura J, Krzeminski K, Ziemba AW, Nazar K, Pekkarinen H et al (2001). Influence of caffeine, cold and exercise on multiple choice reaction time. Psychopharmacology (Berl) 157: 197–201.
Liguori A, Robinson JH (2001). Caffeine antagonism of alcohol-induced driving impairment. Drug Alcohol Depend 63: 123–129.
Marsden G, Leach J (2000). Effects of alcohol and caffeine on maritime navigational skills. Ergonomics 43: 17–26.
Mattila MJ, Nuotto E (1983). Caffeine and theophylline counteract diazepam effects in man. Med Biol 61: 337–343.
Moskowitz H, Burns MM, Williams AF (1985). Skills performance at low blood alcohol levels. J Stud Alcohol 46: 482–485.
Nehlig A, Daval JL, Debry G (1992). Caffeine and the central nervous system: mechanisms of action, biochemical, metabolic and psychostimulant effects. Brain Res Brain Res Rev 17: 139–170.
Nicholson ME, Wang M, Airhihenbuwa CO, Mahoney BS, Christina R, Maney DW (1992). Variability in behavioral impairment involved in the rising and falling BAC curve. J Stud Alcohol 53: 349–356.
Nuotto E, Mattila MJ, Seppala T, Konno K (1982). Coffee and caffeine and alcohol effects on psychomotor function. Clin Pharmacol Ther 31: 68–76.
Oborne DJ, Rogers Y (1983). Interactions of alcohol and caffeine on human reaction time. Aviat Space Environ Med 54: 528–534.
Papineau KL, Roehrs TA, Petrucelli N, Rosenthal LD, Roth T (1998). Electrophysiological assessment (The Multiple Sleep Latency Test) of the biphasic effects of ethanol in humans. Alcohol Clin Exp Res 22: 231–235.
Pedata F, Pepeu G, Spignoli G (1984). Biphasic effect of methylxanthines on acetylcholine release from electrically stimulated brain slices. Br J Pharmacol 83: 69–73.
Pelissier AL, Gantenbein M, Bruguerolle B (1999). Caffeine-induced modifications of heart rate, temperature, and motor activity circadian rhythms in rats. Physiol Behav 67: 81–88.
Penetar D, McCann U, Thorne D, Kamimori G, Galinski C, Sing H et al (1993). Caffeine reversal of sleep deprivation effects on alertness and mood. Psychopharmacology 112: 359–365.
Rechtschaffen A, Kales A (1968). A Manual of Standardized Terminology, Techniques, and Scoring Systems for Sleep Stages of Human Subjects. BIS/BRI: UCLA, Los Angeles.
Reyner LA, Horne JA (1997). Suppression of sleepiness in drivers: combination of caffeine with a short nap. Psychophysiology 34: 721–725.
Roache JD, Griffiths RR (1987). Interactions of diazepam and caffeine: behavioral and subjective dose effects in humans. Pharmacol Biochem Behav 26: 801–812.
Roehrs T, Beare D, Zorick F, Roth T (1994a). Sleepiness and ethanol effects on simulated driving. Alcohol Clin Exp Res 18: 154–158.
Roehrs T, Claiborue D, Knox M, Roth T (1994b). Residual sedating effects of ethanol. Alcohol Clin Exp Res 18: 831–834.
Roehrs T, Claiborue D, Knox M, Roth T (1993). Effects of ethanol, diphenhydramine, and triazolam after a nap. Neuropsychopharmacology 9: 239–245.
Roehrs T, Papineau K, Rosenthal L, Roth T (1999). Ethanol as a hypnotic in insomniacs: self administration and effects on sleep and mood. Neuropsychopharmacology 20: 279–286.
Roehrs T, Roth T (2001). Sleep, sleepiness, and alcohol use. Alcohol Res Health 25: 101–109.
Roehrs T, Zwyghuizen-Doorenbos A, Knox M, Moskowitz H, Roth T (1992). Sedating effects of ethanol and time of drinking. Alcohol Clin Exp Res 16: 553–557.
Roehrs T, Zwyghuizen-Doorenbos A, Timms V, Zorick F, Roth T (1989). Sleep extension, enhanced alertness and the sedating effects of ethanol. Pharmacol Biochem Behav 34: 321–324.
Rosenthal L, Roehrs T, Zwyghuizen-Doorenbos A, Plath D, Roth T (1991). Alerting effects of caffeine after normal and restricted sleep. Neuropsychopharmacology 4: 103–108.
Rush CR, Higgins ST, Hughes JR, Bickel WK, Wiegner MS (1993). Acute behavioral and cardiac effects of alcohol and caffeine, alone and in combination, in humans. Behavioral Pharmacology 4: 562–572.
Scammell TE, Gerashchenko DY, Mochizuki T, McCarthy MT, Estabrooke IV, Sears CA et al (2001). An adenosine A2a agonist increases sleep and induces Fos in ventrolateral preoptic neurons. Neuroscience 107: 653–663.
Sicard BA, Perault MC, Enslen M, Chauffard F, Vandel B, Tachon P (1996). The effects of 600 mg of slow release caffeine on mood and alertness. Aviat Space Environ Med 67: 859–862.
Stein MA, Krasowski M, Leventhal BL, Phillips W, Bender BG (1996). Behavioral and cognitive effects of methylxanthines. A meta-analysis of theophylline and caffeine. Arch Pediatr Adolesc Med 150: 284–288.
Van Dongen HP, Price NJ, Mullington JM, Szuba MP, Kapoor SC, Dinges DF (2001). Caffeine eliminates psychomotor vigilance deficits from sleep inertia. Sleep 24: 813–819.
Varani K, Portaluppi F, Gessi S, Merighi S, Ongini E, Belardinelli L et al (2000). Dose and time effects of caffeine intake on human platelet adenosine A(2A) receptors: functional and biochemical aspects. Circulation 102: 285–289.
Walsh JK, Muehlbach MJ, Humm TM, Dickins QS, Sugerman JL, Schweitzer PK (1990). Effect of caffeine on physiological sleep tendency and ability to sustain wakefulness at night. Psychopharmacology 101: 271–273.
Weiler JM, Bloomfield JR, Woodworth GG, Grant AR, Layton TA, Brown TL et al (2000). Effects of fexofenadine, diphenhydramine, and alcohol on driving performance. A randomized, placebo-controlled trial in the Iowa driving simulator. Ann Intern Med 132: 354–363.
Williams DL, MacLean AW, Cairns J (1983). Dose–response effects of ethanol on the sleep of young women. J Stud Alcohol 44: 515–523.
Wright Jr KP, Badia P, Myers BL, Plenzler SC (1997a). Combination of bright light and caffeine as a countermeasure for impaired alertness and performance during extended sleep deprivation. J Sleep Res 6: 26–35.
Wright Jr KP, Badia P, Myers BL, Plenzler SC, Hakel M (1997b). Caffeine and light effects on nighttime melatonin and temperature levels in sleep-deprived humans. Brain Res 747: 78–84.
Wright Jr KP, Myers BL, Plenzler SC, Drake CL, Badia P (2000). Acute effects of bright light and caffeine on nighttime melatonin and temperature levels in women taking and not taking oral contraceptives. Brain Res 873: 310–317.
Zwyghuizen-Doorenbos A, Roehrs T, Lamphere J, Zorick F, Roth T (1988). Increased daytime sleepiness enhances ethanol's sedative effects. Neuropsychopharmacology 1: 279–286.
Zwyghuizen-Doorenbos A, Roehrs TA, Lipschutz L, Timms V, Roth T (1990). Effects of caffeine on alertness. Psychopharmacology 100: 36–39.
Acknowledgements
This research was supported by NIH, NIAAA Grant R01-AA11264 and NIH-NIDA Grant R01-DA11448.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Drake, C., Roehrs, T., Turner, L. et al. Caffeine Reversal of Ethanol Effects on the Multiple Sleep Latency Test, Memory, and Psychomotor Performance. Neuropsychopharmacol 28, 371–378 (2003). https://doi.org/10.1038/sj.npp.1300026
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.npp.1300026
Keywords
This article is cited by
-
Adenosine A2A receptor mediates hypnotic effects of ethanol in mice
Scientific Reports (2017)
-
Effects of caffeine on alcohol reinforcement: beverage choice, self-administration, and subjective ratings
Psychopharmacology (2017)
-
Effects of caffeine on alcohol-related changes in behavioural control and perceived intoxication in light caffeine consumers
Psychopharmacology (2012)
-
Acute and residual interactive effects of repeated administrations of oral methamphetamine and alcohol in humans
Psychopharmacology (2012)
-
Activation of Adenosine A1 Receptors Reduces Anxiety-Like Behavior During Acute Ethanol Withdrawal (Hangover) in Mice
Neuropsychopharmacology (2006)
