
Abstract
The SYNTAX [Synergy Between percutaneous coronary intervention (PCI) With Taxus and coronary artery bypass surgery (CABG)] score is a decision-making tool in interventional cardiology. However, several facts still remain to be addressed: What about PCI or CABG with a low versus a high score respectively? And what about PCI with a low score versus CABG with a high score? Electronic databases were carefully searched for relevant publications. Odds ratios (OR) with 95% confidence intervals (CIs) were calculated and the analysis was carried out by RevMan 5.3. Eleven studies with a total number of 11,037 patients were included. In terms of clinical outcomes, this analysis showed PCI to have significantly favored patients with a low versus a high SYNTAX score. In patients who were re-vascularized by CABG, mortality and major adverse cardiac events were significantly lower with a low SYNTAX score. However, when PCI with a low SYNTAX score was compared with CABG with a high SYNTAX score, no significant difference in mortality and combined death/stroke/myocardial infarction were observed. In conclusion, the SYNTAX score might be considered useful in interventional cardiology. Nevertheless, the fact that it has limitations when compared to newer tools should also not be ignored.
Similar content being viewed by others

Introduction
Cardiovascular disease (CVD), which might become the number one cause of death in the coming years, continues to affect a large population worldwide1. This chronic disease, which develops through different intravascular mechanisms in the elderly, and which often occurs as a long-term complication in patients with type 2 diabetes mellitus, is either treated by percutaneous coronary intervention (PCI) or coronary artery bypass surgery (CABG), based on several factors such as the severity of the disease, the health conditions and the preferences of the patients2,3.
New scientific research has shown SYNTAX [Synergy Between PCI With Taxus and CABG] score to be an essential decision-making tool in interventional cardiology4. In several recently published studies, PCI was suggested to be a more appropriate revascularization procedure in patients with a lower SYNTAX score whereas in patients with a high score, revascularization with CABG would probably be a better choice5. However, several facts still remain to be addressed: What about PCI or CABG with a low versus a high score respectively? And what about PCI with a low score versus CABG with a high score? In order to answer these interesting questions, we aimed to systematically carry out this meta-analysis.
Methods
Searched Databases and Searched Strategies
The following electronic databases: Medline (PubMed) database of medical research articles, EMBASE database and the Cochrane database of randomized controlled trials (RCTs) were carefully searched for English language publications [RCTs and observational studies (OS)] comparing:
-
a
CABG versus PCI based on the SYNTAX score;
-
b
PCI in patients with a low versus a high SYNTAX score;
-
c
CABG in patients with a low versus a high SYNTAX score.
This search process was carried out using the terms ‘coronary artery bypass surgery, percutaneous coronary intervention, and the SYNTAX score’. Abbreviations of the above-mentioned terms: ‘CABG and PCI’ were also used during this search process. In addition, reference lists of relevant articles were also reviewed for suitable publications.
Inclusion and Exclusion criteria
Studies were included if:
-
a
They were randomized trials or observational research cohorts comparing CABG with PCI based on the SYNTAX score, or comparing PCI and CABG in patients with a low versus a high SYNTAX score respectively.
-
b
They reported adverse clinical outcomes following the respective interventional or surgical procedures.
Studies were excluded if:
-
a
They were meta-analyses, case studies or letters to editors, even though their main focus was on CABG, PCI and the SYNTAX score.
-
b
They did not report adverse clinical outcomes following the corresponding interventional or surgical procedures.
-
c
They were duplicates or they were associated with the same trials.
-
d
They reported data (for example hazard ratios) in a form that could not be used in this current analysis.
Definitions, reported outcomes and follow ups
The endpoints were:
-
a
Mortality (all-cause death);
-
b
Myocardial infarction (MI);
-
c
Repeated revascularization including target vessel revascularization (TVR) and target lesion revascularization (TLR);
-
d
Major adverse cardiac events (MACEs), defined as a combination of death, MI, and repeated revascularization. Since major adverse cerebrovascular and cardiovascular events (MACCEs) were reported only in one study, MACCEs and MACEs were combined together in one subgroup and analyzed;
-
e
Death/stroke/MI;
-
f
Stent thrombosis.
The respective outcomes and follow-up periods have been listed in Table 1.
Data extraction and Review
(PKB and CMY) independently reviewed the trials and the OS which were qualified for this analysis. The authors’ names, the types of study reported (RCT or OS), the revascularization strategies (CABG or PCI) involved, the outcomes and the respective follow up periods reported, the total number of patients assigned to the PCI group, the CABG group, the low and the high SYNTAX score groups respectively, and data reporting the total number of events observed in the experimental and the control groups were carefully extracted by the same two authors. Any disagreement which followed was carefully discussed with the third author (FH) and a final decision was made. The bias risk observed among the trials (excluding OS) was assessed in accordance to the Cochrane Collaboration6, and the preferred reporting items in systematic reviews and meta-analyses (PRISMA) guideline was followed7.
Statistical Analysis
Because studies are diverse clinically and methodologically in systematic reviews and meta-analyses, heterogeneity across the studies, should be expected. In general, heterogeneity assesses the null hypothesis to know if all the studies that have been included in an analysis are evaluating the same effect.
In this analysis, heterogeneity was assessed by two simple statistical methods: the Cochrane Q-statistic or chi-squared (χ2 or Chi2) test and the I2 statistic test.
Since this meta-analysis included only a small number of studies which might as a consequence, result in a low power of testing true heterogeneity, the I2 test was carried out in order to facilitate the assessment of inconsistency across the studies included.
I2 was calculated using this simple formula: I2 = 100% × [equation 1: (Q − df)/Q], whereby Q signified the Cochrane’s heterogeneity statistic and df signified the degree of freedom which could be represented by equation 2: (df = k − 1).
Negative I2 value if obtained (in exceptional cases), would automatically be changed to zero, so that the I2 value only remained between 0 and 100%.
An I2 value less than 25% represented a low heterogeneity, a value about 50% (greater than 25% but less than 75%) represented a moderate level of heterogeneity whereas an I2 value greater than 75% represented a high level of heterogeneity.
In addition, an I2 value equal to 50% was considered as a cut-off point for the use of a fixed effects model (I2 < 50%) or a random effects model (I2 > 50%) during the subgroup analysis.
It should also be noted that the interpretation of a given degree of heterogeneity across the studies which were analyzed might differ in accordance to whether the estimates showed a similar direction of effect.
In this analysis, a P value less than or equal to 0.05 (P ≤ 0.05) was considered significant statistically.
Odds ratios (OR) with 95% confidence intervals (CIs) were considered as the statistical parameters, and the pooled analysis was carried out with RevMan 5.3 software.
Estimation of publication bias
This research consisted of only a small sample size of patients which were obtained from the few relevant studies which were selected for this analysis. Because of this reason, Begg’s and Egger’s tests as well as the Duval trim and fill methods were not effective to assess publication bias8. Instead, publication bias was estimated through funnel plots which were obtained from the Revman software.
Results
Outcome of the searched strategy
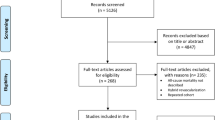
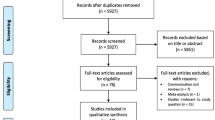
A total number of 241 publications were obtained from the electronic databases. Following a careful assessment of the titles and abstracts, 218 articles were eliminated since they were outside the scope of this research. In addition, another 10 articles were eliminated because they were: meta-analysis (1), letters to editors (3), case reports (2), studies that did not report the relevant clinical outcomes or data (4) associated with the same trial or cohort (2). Finally, only 11 relevant publications were included in this current analysis (Fig. 1).

Flow diagram representing the study selection.
General features of the studies included
Eleven thousand and thirty-seven (11,037) patients [6893 patients assigned to the control group and 4144 patients assigned to the experimental group], which were obtained from 5 randomized trials and 6 OS were included in this analysis.
In order to answer the first question of this analysis, which was based on only those patients who were treated by PCI, 5521 patients with a low SYNTAX score were compared to 2531 patients with a high SYNTAX score;
To answer the second question of this analysis, which was based on those patients who were treated only by CABG, 1132 patients with a low SYNTAX score were compared with 773 patients with a high SYNTAX score;
To answer the third question of this analysis, 1200 patients with a low SYNTAX score who were assigned to PCI, were compared to 840 patients with a high SYNTAX score who were assigned to CABG.
When considering PCI with a low versus a high SYNTAX score, four studies [Garg9, Garg10, Wykrzykowska11 and Yadav12], which were classified to the same subgroup, involved a low score of ≤17, versus a high score above 17, whereas two studies [Capodanno13 and Kim14] which were included in another subgroup, involved a low score of ≤36 versus a high score above 34. Further details were summarized in Table 2.
Baseline features of the studies included
The baseline features have been summarized in Table 3. The patients had a mean age which varied from 62.0 to 71.4 years (except study Wykrzykowska11 which included younger patients). All of the studies contained more male patients than female patients: (study Garg9: 72.9% versus 76.6%, study Garg10: 78.8% versus 74.1%, study Wykrzykowska11: 73.8% versus 73.8%, study Yadav12: 70.4% versus 66.0%, study Kim14: 51.4% versus 66.2%, study Cho15: 79.1% versus 73.6%, study Gannot17: 80.0% versus 82.0%, study Miyagi18: 85.7% versus 81.6%, study Capodanno13: 79.4% versus 75.9%, and study Shiomi19: 77.0% versus 71.0% male patients in the experimental versus the control group respectively). The percentage of patients with co-morbidities and other cardiovascular risk factors (hypertension, dyslipidemia, smoking, diabetes mellitus) was also listed (Table 3). The highest number of patients with hypertension (85% versus 86.0%) within both the experimental and control groups respectively, were observed in Study Shiomi19 whereas majority of patients with diabetes mellitus (53.0% versus 51.6%) within both the experimental and control groups respectively were observed in Study Miyagi18.
Nevertheless, even if the differences varied from study to study, there were almost no significant differences observed in the baseline features of patients who were assigned to the control (low score) and the experimental (high score) groups.
Percutaneous coronary intervention in patients with a low versus a high SYNTAX score
At first, this analysis compared PCI in patients with a low versus a high SYNTAX score. In the beginning, a low score limit of ≤12, versus a high score limit of >12 was set. Results of this analysis showed PCI to have significantly favored patients with a low SYNTAX score whereby mortality, MACEs, TVR, TLR, repeated revascularization (combined TVR + TLR) and stent thrombosis were significantly lower (OR: 2.55, 95% CI: 1.78–3.66; P < 0.00001), (OR: 2.33, 95% CI: 1.94–2.80; P < 0.00001), (OR: 1.94, 95% CI: 1.42–2.64; P < 0.0001), (OR: 1.92, 95% CI: 1.39–2.65; P < 0.0001), (OR: 2.08, 95% CI: 1.70–2.54; P < 0.00001) and (OR: 3.13, 95% CI: 2.22–4.42; P < 0.00001) respectively as illustrated in Fig. 2.

Outcomes associated with percutaneous coronary intervention following a low versus a high SYNTAX score.
MI was also significantly higher with a high SYNTAX score (OR: 1.81, 95% CI: 1.14–2.88; P = 0.01) [Fig. 3].

Myocardial infarction associated with percutaneous coronary intervention following a low versus a high SYNTAX score.
When a low score limit of ≤36 versus a high score limit of >34 was considered as the score range, mortality was still significantly higher in patients with a high SYNTAX score following PCI (OR: 3.66, 95% CI: 1.59–8.43; P = 0.002) as shown in Fig. 4.

Mortality associated with percutaneous coronary intervention following a low versus a high SYNTAX score.
Coronary artery bypass surgery in patients with a low versus a high SYNTAX score
Another analysis was carried out comparing CABG in patients with a low versus a high SYNTAX score. Results of this analysis showed that when a low score of <23, and a high score of ≥22 were considered, mortality and MACEs significantly favored a low SYNTAX score (OR: 1.87, 95% CI: 1.34–2.62; P = 0.0002) and (OR: 2.15, 95% CI: 1.46–3.15; P < 0.0001) respectively as shown in Fig. 5.

Outcomes associated with coronary artery bypass surgery following a low versus a high SYNTAX score.
However, following CABG, the results showed MI not to be significantly different with a low versus a high SYNTAX score (OR: 1.84, 95% CI: 0.25–13.59; P = 0.55), but this specific subgroup was accompanied by a high level of heterogeneity (Fig. 6).

Myocardial infarction associated with coronary artery bypass surgery following a low versus a high SYNTAX score.
When a low score limit of <33, and a high score limit of ≥33 were considered, no significant difference was observed in mortality following CABG (OR: 1.30, 95% CI: 0.73–2.31; P = 0.37) [Fig. 7].

Mortality associated with coronary artery bypass surgery following a low versus a high SYNTAX score.
Percutaneous coronary intervention with a low SYNTAX score versus coronary artery bypass surgery with a high SYNTAX score
Research has shown that the main purpose of the SYNTAX score was to stratify those patients who would benefit most from PCI and CABG respectively. According to literatures, PCI should be recommended to patients who were allocated a low score whereas CABG might be considered more appropriate to patients with a high score.
This current analysis has confirmed the statements published in previous literatures showing no significant difference in mortality, and the combined outcomes of death/stroke/MI observed between PCI with low SYNTAX score versus CABG with high SYNTAX score, (OR: 1.17, 95% CI: 0.61–2.23; P = 0.64), and (OR: 1.22, 95% CI: 0.46–3.22; P = 0.69) respectively as shown in Fig. 8.

Outcomes associated with percutaneous coronary intervention in patients with a low SYNTAX score versus coronary artery bypass surgery in patients with a high SYNTAX score.
Study Kim14 was thought to have possibly been introducing bias within this current analysis of PCI versus CABG. Therefore, another analysis was carried out but this time without including study Kim14. Nevertheless, a similar mortality rate observed between PCI with a low SYNTAX score versus CABG with a high SYNTAX score (OR: 0.82, 95% CI: 0.57–1.18; P = 0.29) [Fig. 9] and with a very low level of heterogeneity further confirmed the above-shown result.

Mortality associated with percutaneous coronary intervention in patients with a low SYNTAX score versus coronary artery bypass surgery in patients with a high SYNTAX score.
Based on a visual inspection of the funnel plots obtained through RevMan, a low level of publication bias was observed among most of the studies which were involved while carrying out this analysis (Figs 10 and 11).

Funnel plot showing publication bias.

Funnel plot showing publication bias.
Discussion
This study aimed to answer three major questions: the outcomes following PCI with a low versus a high SYNTAX score, the outcomes following CABG with a low versus a high SYNTAX score, and the outcomes following PCI with a low SYNTAX score versus CABG with a high SYNTAX score.
Results of this analysis showed a low SYNTAX score to be associated with significantly lower adverse outcomes compared to a high SYNTAX score following PCI (20% versus 49.2% for mortality, 9.4% versus 19.4% for MACEs, 6.3% versus 11.6% for TVR, 3.6% versus 6.7% for TLR, 3.53% versus 5.93% for MI, and 1.21% versus 3.65% for stent thrombosis), clearly answering the first question.
Following revascularization with CABG, a low SYNTAX score was associated with significantly lower mortality (10.0% versus 15.9%) and MACEs (10.4% versus 19.1%) when compared to a high score, providing an answer to the first part of the second question. However, when a higher limit of scores was considered, no significant difference was observed in the mortality rate (9.82% versus 11.3%), further answering the second question. Comparing a low score with a high score showed the former to be associated with a favorable outcome. However, when two high score limits were compared (for example, a low score of <34 was compared with a high score of >34), the difference was not significant.
In response to the third question, the current results showed that when PCI with a low SYNTAX score was compared to CABG with a high SYNTAX score, a similar mortality rate (16.1% versus 14.3%) was observed following the respective revascularization procedures.
To further support this analysis, the SHINANO registry showed SYNTAX score to be beneficial in predicting the incidence of MACEs following PCI20. That particular registry included patients with prior heart failure and coronary artery disease. A high SYNTAX score was associated with higher prediction of MACEs. According to what they have observed in their results, the authors suggested SYNTAX score to be a useful parameter in order to improve risk stratification in patients with complex coronary diseases.
In addition, the five-year follow-up of the SYNTAX trial showed that in patients who were allocated a low SYNTAX score, PCI was an acceptable revascularization strategy when compared to CABG; but with a high rate of late repeated revascularization. Other studies showed patients with low SYNTAX scores to have similar rates of MACCEs following either PCI or CABG further supporting this current analysis21.
Our results showed PCI with a low SYNTAX score to be comparable to CABG with a high SYNTAX score. To again support this point, the Evaluation of XIENCE versus Coronary Artery Bypass Surgery for Effectiveness of Left Main Revascularization (EXCEL) trial which randomly assigned 1905 patients with left main coronary disease showed that PCI with everolimus eluting stents was non-inferior to CABG22.
Nevertheless, even if a recently published systematic review showed that the SYNTAX score was comparable to the clinical SYNTAX scoring system in predicting soft endpoints such as TVR and MACEs, the same study stated that clinical SYNTAX score was even better in predicting prognosis since it involved patients with important clinical risk factors23. Another study showed the Logistic Clinical SYNTAX score to further enhance the prediction of mortality following PCI24.
The SYNTAX score II which is another potential tool combining clinical predictors with anatomical factors showed robust and more accurate prognosis compared to the SYNTAX score25. The benefits of the SYNTAX score II were further supported by other studies especially in patients with left main coronary diseases and other complex coronary artery diseases26,27.
Furthermore, the New Risk Stratification (NERS) score which encompasses clinical, procedural and angiographic characteristics showed a higher predictive ability of MACEs when compared to the SYNTAX score28. However, new research should be expected to boost/support and further address these comments29.
Conclusion
Since a high SYNTAX score was associated with significantly higher adverse outcomes irrespective of which revascularization procedure was involved (PCI or CABG), and because no significant difference in mortality was observed with a low SYNTAX score following PCI compared to a high SYNTAX score following CABG, the SYNTAX score should be considered among the important decision-making tools which might be used to stratify patients who would most probably benefit from PCI and CABG respectively, or to select patients who would probably be susceptible to unfavorable clinical outcomes following these revascularization procedures. Nevertheless, we should also not ignore the fact that the SYNTAX score has limitations when compared to newer tools.
Additional Information
How to cite this article: Bundhun, P. K. et al. Percutaneous Coronary Intervention, Coronary Artery Bypass Surgery and the SYNTAX score: A systematic review and meta-analysis. Sci. Rep. 7, 43801; doi: 10.1038/srep43801 (2017).
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
Heidenreich, P. A. et al. Forecasting the future of cardiovascular disease in the United States: a policy statement from the American Heart Association. Circulation. 123(8), 933–44 (2011).
Bundhun, P. K. et al. Adverse Cardiovascular Outcomes associated with Coronary Artery Bypass Surgery and PercutaneousCoronary Intervention with Everolimus Eluting Stents: A Meta-Analysis. Sci Rep. 6, 35869 (2016).
Pandey, A. et al. Revascularization Trends in Patients With Diabetes Mellitus and Multivessel Coronary Artery Disease Presenting With Non-ST Elevation Myocardial Infarction: Insights From the National Cardiovascular Data Registry Acute Coronary Treatment and Intervention Outcomes Network Registry-Get with the Guidelines (NCDR ACTION Registry-GWTG). Circ Cardiovasc Qual Outcomes. 9(3), 197–205 (2016).
Franzone, A. et al. Angiographic complexity of coronary artery disease according to SYNTAX score and clinical outcomes after revascularisation with newer-generation drug-eluting stents: a substudy of the BIOSCIENCE trial. EuroIntervention. 12(5), e595–604 (2016).
Amsterdam, E. A. et al. American College of Cardiology; American Heart Association Task Force on Practice Guidelines; Society for Cardiovascular Angiography and Interventions; Society of Thoracic Surgeons; American Association for Clinical Chemistry. 2014 AHA/ACC Guideline for the Management of Patients with Non-ST-Elevation Acute CoronarySyndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 64(24), e139–228 (2014).
Higgins, J. P. et al. Assessing risk of bias in included studies, in Cochrane handbook for systematic reviews of interventions. Wiley. 187–241 (2008).
Liberati, A. et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. Bmj. 339, b2700 (2009).
Sterne, J. A., Egger, M. & Smith, G. D. Systematic reviews in health care: Investigating and dealing with publicationand other biases in meta-analysis. BMJ. 323(7304), 101–5 (2001).
Garg, S. et al. Prediction of 1-year clinical outcomes using the SYNTAX score in patients with acute ST-segmentelevation myocardial infarction undergoing primary percutaneous coronary intervention: a substudy of the STRATEGY (Single High-Dose Bolus Tirofiban and Sirolimus-Eluting Stent Versus Abciximab and Bare-Metal Stent in Acute Myocardial Infarction) and MULTISTRATEGY (Multicenter Evaluation of Single High-Dose Bolus Tirofiban Versus Abciximab With Sirolimus-Eluting Stent or Bare-Metal Stent in Acute Myocardial Infarction Study) trials. JACC Cardiovasc Interv. 4(1), 66–75 (2011).
Garg, S. et al. The prognostic utility of the SYNTAX score on 1-year outcomes after revascularization with zotarolimus- and everolimus-eluting stents: a substudy of the RESOLUTE All Comers Trial. JACC Cardiovasc Interv. 4(4), 432–41 (2011).
Wykrzykowska, J. J. et al. Value of the SYNTAX score for risk assessment in the all-comers population of the randomized multicenter LEADERS (Limus Eluted from A Durable versus ERodable Stent coating) trial. J Am Coll Cardiol. 56(4), 272–7 (2010).
Yadav, M. et al. SYNTAX score and the risk of stent thrombosis after percutaneous coronary intervention in patients with non-ST-segment elevation acute coronary syndromes: an ACUITY trial substudy. Catheter Cardiovasc Interv. 85(1), 1–10 (2015).
Capodanno, D. et al. Usefulness of SYNTAX score to select patients with left main coronary artery disease to be treated with coronary artery bypass graft. JACC Cardiovasc Interv. 2(8), 731–8 (2009).
Kim, Y. H. et al. Validation of SYNTAX (Synergy between PCI with Taxus and Cardiac Surgery) score for prediction of outcomes after unprotected left main coronary revascularization. JACC Cardiovasc Interv. 3(6), 612–23 (2010).
Cho, Y. et al. The SYNTAX score is correlated with long-term outcomes of coronary artery bypass grafting for complexcoronary artery lesions. Interact Cardiovasc Thorac Surg. 23(1), 125–32 (2016).
Farooq, V. et al. The CABG SYNTAX Score - an angiographic tool to grade the complexity of coronary disease followingcoronary artery bypass graft surgery: from the SYNTAX Left Main Angiographic (SYNTAX-LE MANS) substudy. EuroIntervention. 8(11), 1277–85 (2013).
Gannot, S. et al. Higher Syntax score is not predictive of late mortality in “real-world” patients with multivessel coronaryartery disease undergoing coronary artery bypass grafting. Isr Med Assoc J. 16(12), 764–7 (2014).
Miyagi, T. et al. Validation of the Coronary Artery Bypass Graft SYNTAX Score (Synergy Between PercutaneousCoronary Intervention With Taxus) as a Prognostic Marker for Patients With Previous Coronary ArteryBypass Graft Surgery After Percutaneous Coronary Intervention. Circ Cardiovasc Interv. 9(9) (2016).
Shiomi, H. et al. Comparison of Percutaneous Coronary Intervention With Coronary Artery Bypass Grafting in Unprotected Left Main Coronary Artery Disease - 5-Year Outcome From CREDO-Kyoto PCI/CABG Registry Cohort-2. Circ J. 79(6), 1282–9 (2015).
Minamisawa, M. et al. Prediction of 1-year clinical outcomes using the SYNTAX score in patients with prior heart failure undergoing percutaneous coronary intervention: sub-analysis of the SHINANO registry, doi: 10.1007/s00380-016-0896-9 (2016).
Head, S. J. et al. Coronary artery bypass grafting vs. percutaneous coronary intervention for patients with three-vesseldisease: final five-year follow-up of the SYNTAX trial. Eur Heart J. 35(40), 2821–30 (2014).
Stone, G. W. et al. Everolimus-Eluting Stents or Bypass Surgery for Left Main Coronary Artery Disease. N Engl J Med. 375(23), 2223–2235 (2016).
Chen, J. et al. Validation of the Ability of SYNTAX and Clinical SYNTAX Scores to Predict Adverse Cardiovascular EventsAfter Stent Implantation: A Systematic Review and Meta-Analysis. Angiology. 67(9), 820–8 (2016).
Farooq, V. et al. Combined anatomical and clinical factors for the long-term risk stratification of patients undergoingpercutaneous coronary intervention: the Logistic Clinical SYNTAX score. Eur Heart J. 33(24), 3098–104 (2012).
Madeira, S. et al. Potential Utility of the SYNTAX Score 2 in Patients Undergoing Left Main Angioplasty. Arq Bras Cardiol. 106(4), 270–8 (2016).
Farooq, V. et al. Anatomical and clinical characteristics to guide decision making between coronary artery bypass surgeryand percutaneous coronary intervention for individual patients: development and validation of SYNTAXscore II. Lancet. 381(9867), 639–50 (2013).
Salvatore, A. et al. Usefulness of SYNTAX score II in complex percutaneous coronary interventions in the setting of acute coronary syndrome. J Saudi Heart Assoc. 28(2), 63–72 (2016).
Chen, S. L. et al. Comparison between the NERS (New Risk Stratification) score and the SYNTAX (Synergy between Percutaneous Coronary Intervention with Taxus and Cardiac Surgery) score in outcome prediction for unprotected left main stenting. JACC Cardiovasc Interv. 3(6), 632–41 (2010).
Kappetein, A. P. et al. Design and rationale for a randomised comparison of everolimus-eluting stents and coronary artery bypass graft surgery in selected patients with left main coronary artery disease: the EXCEL trial. EuroIntervention. 12(7), 861–72 (2016).
Acknowledgements
This research was supported by Youth Science Foundation of Guangxi Medical University (No. GXMUYSF201308), Scientific Project of Guangxi Higher Education (No. KY2015ZD028) and National Natural Science Foundation of China (No. 81560046). There was no external source of funding for this research.
Author information
Authors and Affiliations
Contributions
P.K.B., C.M.Y., and F.H. were responsible for the conception and design, acquisition of data, analysis and interpretation of data, drafting the initial manuscript and revising it critically for important intellectual content. P.K.B. wrote the final manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Bundhun, P., Yanamala, C. & Huang, F. Percutaneous Coronary Intervention, Coronary Artery Bypass Surgery and the SYNTAX score: A systematic review and meta-analysis. Sci Rep 7, 43801 (2017). https://doi.org/10.1038/srep43801
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep43801
This article is cited by
-
Interventional therapy of acute coronary syndromes in very old patient population and results of 2 years follow-up
The Egyptian Heart Journal (2023)
-
Surgical and percutaneous revascularization outcomes based on SYNTAX I, II, and residual scores: a long-term follow-up study
Journal of Cardiothoracic Surgery (2021)
-
Ten-Year Outcomes of Percutaneous Coronary Intervention Versus Coronary Artery Bypass Grafting for Patients with Type 2 Diabetes Mellitus Suffering from Left Main Coronary Disease: A Meta-Analysis
Diabetes Therapy (2021)
-
Clinical outcome comparison of percutaneous coronary intervention and bypass surgery in diabetic patients with coronary artery disease: a meta-analysis of randomized controlled trials and observational studies
Diabetology & Metabolic Syndrome (2019)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
