
Abstract
The aim of this study was to assess the expression patterns of serum galectin-1 (Gal-1), galectin-3 (Gal-3), galectin-9 (Gal-9), and galectin-3 binding protein (Gal-3BP) and their associations with stroke outcome in large artery atherosclerotic (LAA) stroke. The serum levels of Gal-1, Gal-3, Gal-9, and Gal-3BP were measured by ELISA in 130 patients with LAA stroke and 130 age- and sex-matched controls. Serum samples were collected from the patients on day 1, day 6, and in the 4th week after ischaemic stroke (IS). An unfavourable outcome was defined as a modified Rankin Scale score of >2 on day 90 after IS. Our results indicated that the Gal-3 and Gal-9 levels were higher in patients with LAA stroke than in controls. A higher Gal-3 level was independently associated with an unfavourable outcome both on day 1 and day 6 after IS. In addition, Gal-9 and Gal-1 levels were upregulated on day 6 and in the 4th week after IS, respectively. For Gal-3BP, no difference was detected between patients and controls and no predictive value was found in patients. In conclusion, these findings suggest that the serum levels of Gal-1, Gal-3, and Gal-9 may be associated with LAA stroke.
Similar content being viewed by others

Introduction
Galectins (Gals) are a family of β-galactoside-specific lectins that includes at least 15 members that have a conserved carbohydrate recognition domain sequence with different affinities and specificities for β-galactoside1. Gals are expressed intracellularly and extracellularly in different cells and are involved in cell adhesion, migration, activation, proliferation, and apoptosis1,2. Several studies have demonstrated the roles of different members of this family in modulating pathological processes such as inflammation, immunization, and tumour biology3,4,5,6,7,8.
Galectin-1 (Gal-1), galectin-3 (Gal-3), and galectin-9 (Gal-9) are widely studied members of the Gals family. Despite having significant sequence homologies, experimental studies have demonstrated that different Gals may exert diverse and even opposite effects on atherosclerosis. For example, Gal-1 promotes the development of atherosclerosis9; Gal-3 exerts either a facilitating or inhibitory influence on atherosclerosis10,11; and Gal-9 participates in the regulation of atherosclerosis12. In addition, some clinical studies have shown that patients with coronary artery disease (CAD) have higher Gal-3 levels13 and lower Gal-9 levels in the circulation than healthy controls14.
Galectin-3 binding protein (Gal-3BP), which is a member of the macrophage scavenger receptor cysteine-rich domain superfamily of molecules, is a ubiquitously expressed secreted protein15,16. It binds to ligands such as Gal-317 and Gal-118. Recent studies demonstrated that Gal-3BP is expressed in coronary artery plaques19, but its plasma levels do not reflect coronary plaque instability in patients with CAD20. In addition, another study reported that Gal-3BP levels are associated with carotid artery lesions19.
These controversial conclusions might result from heterogeneity among different populations and the diverse clinical conditions in the available studies. Nevertheless, these data implicate a common theme, which is that Gal-1, Gal-3, Gal-9 and Gal-3BP may play indispensable roles in atherosclerosis and may act as biomarkers for the risk and/or prognosis of atherosclerosis-related diseases. Furthermore, studies concerning the circulating levels of these biomarkers in patients with ischaemic stroke (IS) are limited.
On the other hand, evidence from experimental studies implicates different roles for the Gals family members in the progression of brain damage after IS. For example, Gal-1 is increased after IS and is implicated in neuroprotection against ischaemia21,22; Gal-3 is actively released under ischaemia/stroke conditions and amplifies and prolongs the inflammatory response7; and the expression of Gal-9 is increased after IS and is involved in neuronal injury23. However, these studies were performed primarily in animal models or in vitro, and few studies have investigated whether these biomarkers in circulation are associated with the stroke severity and/or outcomes in human after IS.
Therefore, the aim of this study was to evaluate the serum levels of Gal-1, Gal-3, Gal-9, and Gal-3BP in patients with large artery atherosclerotic (LAA) stroke and in age- and sex-matched controls, and to determine the long-term changes in the levels of these biomarkers on day 6 and in the 4th week after IS. We also investigated whether these biomarkers were independently associated with stroke severity and functional outcomes at 90 days after IS.
Results
Baseline characteristics of the study participants
The study included 130 patients with LAA stroke and 130 age- and sex-matched non-stroke controls. All the participants are of the Han nationality. The basic characteristics of the study subjects are shown in Table 1. Compared with the controls, the LAA patients had higher systolic blood pressure (SBP), fasting blood glucose (FBG), and high-sensitivity C-reactive protein (hs-CPR) levels and included a greater percentage of smokers.
Correlations between the serum Gal-1, Gal-3, Gal-9, and Gal-3BP levels
In both the control and stroke groups, the serum levels of Gal-9 were significantly correlated with the Gal-1 (controls, r = 0.324, p < 0.001; patients, r = 0.339, p < 0.001) and Gal-3 levels (controls, r = 0.382, p < 0.001; patients, r = 0.215, p = 0.014), and the Gal-3 levels were correlated with the Gal-3BP levels (controls, r = 0.181, p = 0.040; patients, r = 0.180, p = 0.041). In addition, the Gal-1 levels were correlated with the Gal-3 levels in the stroke group (r = 0.178, p = 0.043). No other correlations were found within Gal-related or Gal-3BP-related parameters (Supplementary Table S1).
Higher serum levels of Gal-3 and Gal-9 were associated with LAA stroke
The serum levels of Gal-3, Gal-9, and Gal-3BP were significantly higher in the patients than in the controls (Figs 1a and 2b, c; Table 2). After adjusting for age, sex, body mass index, hypertension, diabetes, dyslipidaemia, smoking, drinking, homocysteine, creatinine, and hs-CPR, both Gal-3 and Gal-9 remained independent markers of LAA stroke, whereas Gal-3BP did not (Table 2). No difference was found in the Gal-1 levels between the patients and the controls (Fig. 1d).

In the box-and-whisker plots, the lower and upper ends of the box represent the 25th and 75th percentiles, respectively; the horizontal line inside the box represents the median value; and the peripheral lines extending to the outer fences represent the 10th and 90th percentiles. Differences between the two groups were compared using Student’s t-test (a,b,d) or the Mann-Whitney U test (c). *p < 0.05, **p < 0.01. Abbreviations: galectin-3BP, galectin-3 binding protein.

(a and c) comparisons of galectin-9 and galectin-1 levels between day 1 and day 6 after stroke in 109 patients. The differences were compared using the Wilcoxon signed-rank test (a) or a matched t-test (c). *p < 0.05. (b and d), comparison of galectin-9 and galectin-1 levels between day 1, day 6, and 4 weeks after stroke in 39 patients. The differences between the three time points were compared using the Friedman M test with post hoc Wilcoxon signed-rank tests (b) and repeated measures ANOVA with post hoc matched t-tests (d). #p < 0.0125 was considered statistically significant after the Bonferroni correction.
No correlations were found between the Gal-1, Gal-3, Gal-9, or Gal-3BP levels and stroke severity, which was defined by the stroke volumes and the National Institutes of Health Stroke Scale (NIHSS) scores in the patients (Supplementary Table S2).
A higher serum level of Gal-3 was associated with an unfavourable outcome on day 90 after IS
Of the Gals and Gal-3BP parameters, the serum levels of Gal-3 were significantly higher in the patients with an unfavourable outcome than in the patients with a favourable outcome, according to the univariate analysis (Table 3; day 1, 7.48 ± 1.64 ng/ml vs. 8.25 ± 1.66 ng/ml, p = 0.013; day 6, 7.64 ± 1.80 ng/ml vs. 8.52 ± 2.03 ng/ml, p = 0.024), and the clinical variables associated with an unfavourable outcome were older age and higher NIHSS scores (Table 3). After adjusting for these clinical variables, a higher Gal-3 level independently predicted an unfavourable outcome on day 90 after IS (day 1, adjusted odds ratio [95% confidence interval], 1.966 [1.136, 3.401], p = 0.016; day 6, 1.946 [1.042, 3.636], p = 0.037). No association was found between the stroke outcomes and the Gal-1, Gal-3BP, and Gal-9 levels (Table 3).
A total of 12 patients (10.3%) died within the 90 day period after IS. Due to the relatively low mortality, the overall ability to distinguish the survivors from the non-survivors in the present study could not be estimated.
Serum levels of Gal-9 and Gal-1 were upregulated on day 6 and in the 4th week after IS
The time-course analysis showed that the serum Gal-9 levels were higher on day 6 after IS than on day 1 (in 109 patients; Fig. 2a, p = 0.016) and remained at higher levels in the 4th week after IS (in 39 patients; Fig. 2b, 4 weeks vs. day 6, p = 0.040). There was no difference in the Gal-1 levels between day 1 and day 6 after IS (Fig. 2c, p = 0.181); however, the Gal-1 levels were higher in the 4th week after IS (Fig. 2d, 4 weeks vs. day 6, p = 0.001). The serum levels of Gal-3 and Gal-3BP remained stable throughout day 1, day 6, and 4th week after IS.
Discussion
The major findings of this study are as follows: (1) the serum levels of Gal-3 and Gal-9 were significantly higher in the patients with LAA stroke than in the controls; (2) the higher Gal-3 level independently predicted an unfavourable outcome on day 90 after IS; and (3) the serum levels of Gal-1 and Gal-9 were upregulated after IS.
Given that Gal-1, Gal-3, Gal-9, and Gal-3BP may play different roles in atherosclerosis9,11,12,19, which is a major cause of cardiovascular disease (CVD), and that the levels of some of these parameters in CVD patients have been determined to be different from healthy controls and/or are associated with surrogate markers of atherosclerosis13,19,24, we postulated that the concentrations of Gal-1, Gal-3, Gal-9, and Gal-3BP might differentiate LAA stroke patients from healthy controls and might as predictors for stroke severity and/or outcomes; however, no published reports have previously assessed these levels in LAA stroke patients. In the present study, we demonstrated that patients with LAA stroke have higher Gal-3 levels than controls. Thrombosis or embolism secondary to atherosclerosis of large arteries is the most important underlying pathology of LAA stroke25. The role of Gal-3 in atherosclerosis has been highlighted recently. Some experimental studies have demonstrated the pro-atherosclerotic effects of Gal-3, such as attracting monocytes and macrophages26, enhancing macrophage phagocytosis, accelerating macrophage transformation into foam cells11,27, and inducing the proliferation of vascular smooth muscle cells28. In addition, a clinical study suggested that Gal-3 levels are increased in patients with carotid atherosclerosis29, who are significantly predisposed to experience cerebral ischaemic events30. Additional studies have demonstrated that Gal-3 levels are significantly higher in patients with CAD and are correlated with the severity of CAD13,24. Together with the present study, these findings may support the assumption that Gal-3 is linked to atherosclerosis. Additionally, we also discovered that patients with LAA stroke have higher Gal-9 levels than controls. In general, Gal-9 appears to play a role in immunity and inflammatory processes, particularly in regulatory T cell development and homeostasis31. Regulatory T cells mediate the immune responses that participate in the development of atherosclerosis32,33.
It should be noted that these data should be interpreted cautiously given that these measurements were obtained after the stroke event had occurred. Indeed, the Gal-9 levels were increased on day 6, and thus it is impossible to determine whether the Gal-9 levels had already changed before the measurements were acquired. The Gal-3 levels remained stable after IS in our study. In addition, a recent prospective study reported that higher Gal-3 levels are potentially a predictive marker for stroke in female patients who have undergone carotid endarterectomy34.
On the other hand, given that the expression of Gal-1, Gal-3, and Gal-9 are unregulated in the brain after IS and exert either neuroprotective or neurotoxic functions7,21,22,23,35,36, we postulated that these biomarkers in the circulation might be potential predictors for stroke outcomes; however, these associations have not been previously confirmed in stroke patients. In the current study, we found that a higher level of only Gal-3 was independently associated with an unfavourable outcome on day 90 after IS. Several studies have demonstrated that the level of Gal-3 is an independent predictor of cardiovascular events and/or death in patients with heart failure37,38, CAD39,40, and peripheral artery disease29. Furthermore, Gal-3 can also predict all-cause and/or cardiovascular-related death and the risk of new-onset heart failure in healthy subjects13,41,42. Our findings reveal the adverse prognostic role of higher Gal-3 levels in patients with IS. The possible function and role of Gal-3 in the central nervous system has not been completely elucidated. The prevailing hypothesis in the literature is that Gal3-dependent TLR4 activation after IS could contribute to enhanced microglia activity, which would expand and prolong the inflammatory response in the brain7 and the post-ischaemic inflammatory response that is closely related to the adverse outcomes of stroke43.
Our study failed to show a significant association between Gal-1 or Gal-9 levels and short-term stroke outcomes in patients with IS; however, both the Gal-1 and Gal-9 levels were upregulated after IS and were significantly correlated with the Gal-3 levels. Several previous studies have shown that the expression of Gal-1 and Gal-9 are significant increased and exert differential functions in the brain after ischaemic brain injury. Gal-1 plays a role in facilitating long-term neuroprotection and improving functional recovery21,22,35,36 and Gal-9 is involved in the inflammatory response and neuronal injury23. In addition, previous evidence has shown that brain ischaemic injury stimulates angiogenesis for the formation of new brain microvessels44,45, which become evident within 2 weeks after IS in animal models46. The pro-angiogenesis and pro-arteriogenesis effects of the Gal family (including Gal-1 and Gal-9) have been widely studied47. Taken together, all these data implicate roles of the increased levels of Gal-1 and Gal-9 in stroke rather than simple acute behaviors after IS, although these specific prognostic values still need to be clarified, perhaps in studies investigating long-term functional outcomes or other aspects of post-stroke prognosis, such as cognition. Furthermore, cerebral ischaemia can trigger biological reactions in both the brain and systemic circulation. It is unclear whether the increased levels of Gal-1 and Gal-9 are predominantly from the brain due to the breakdown of the blood-brain barrier or from any other tissues, or from overlap during recovery.
There are currently no data reported available regarding Gal-3BP in IS. The present study expands the knowledge of the role of Gal-3BP in patients with LAA stroke. We did not find any differences in the Gal-3BP levels between the patients and controls or that Gal-3BP was related to stroke severity or outcomes in patients. This result is consistent with a previous study in patients with cardiovascular disease that found Gal-3BP levels did not differ between patients with or without CAD20.
This study has several limitations. First, although our results were significant, our sample size was relatively small. Further studies utilizing a larger sample size are necessary to confirm our findings. Second, we did not assess the differences based on the location of the atherosclerosis. The greater prevalence of intracranial atherosclerosis rather than extracranial atherosclerosis in Asian populations48 may limit the extrapolation of our findings to other populations. Third, because the earliest serum samples were obtained on day 1 after the IS had already occurred, we cannot determine whether the measurements obtained at this time point reflect pre-stroke levels or changes that occurred within the first 24 h. A longitudinal study including serial measurements of serum levels (particularly within the first 24 h after IS) may better identify certain changes that occur secondary to IS. Fourth, the patients who had three blood samples had relatively mild symptoms (lower NIHSS and the modified Rankin Scale (mRS) scores) than the whole patients, which might result in bias of the results. Finally, due to the clinical relevance of our study, we did not completely elucidate the pathophysiological mechanism underlying these findings. Nevertheless, this study constitutes the first evaluation of serum levels of Gal-1, Gal-3, Gal-9, and Gal-3BP in humans with LAA stroke.
In conclusion, our study provides preliminary evidence that the serum levels of Gal-3 are higher in patients with LAA stroke and a higher Gal-3 level might be an independent prognostic marker for IS in this population. These findings are consistent with the hypothesis that the Gal-3 might be used as a non-traditional risk factor for atherosclerosis and might participate in the pathological processes after LAA stroke, which suggests that therapies designed to suppress Gal-3 might have a role in the prevention and treatment of CVD. In addition, our study showed that the Gal-1 and Gal-9 levels are upregulated after IS; however, neither Gal-1 nor Gal-9 are associated with the short-term prognosis of stroke. Further studies are needed not only to provide the exact effect and potential biological mechanisms of Gals in the pathogenesis of atherosclerosis and IS, but also to provide deeper insight into the sources and effects of increased levels of these Gals after IS to determine if they are protective, detrimental or neutral.
Methods
Study subjects
The present study was performed in accordance with the ethical guidelines of the 1975 Declaration of Helsinki and was approved by the Medical Ethics Committee of Taizhou Hospital. All participants or their relatives provided written informed consent.
A total of 130 patients with LAA stroke were consecutively recruited from the Department of Neurology of Taizhou Hospital, Zhejiang, China, from December 2014 to August 2015.
In this study, acute IS was diagnosed according to the World Health Organization criteria49 combined with the confirmation from brain computed tomography or magnetic resonance imaging. LAA stroke was defined according to TOAST (Trial of Org 10172 in Acute Stroke Treatment) criteria25. At least two neurologists reviewed the clinical features and diagnostic test results before assigning the subtype classifications.
Patients were included if they met the following criteria: first-time IS, admission within 24 h after symptom onset, and absence of thrombolysis or interventional therapy. In addition, the following exclusion criteria were applied: any history of stroke, severe coronary heart disease or arrhythmia, a history of tumours, severe hepatic or renal insufficiency, haematological disease, autoimmune disease, chronic inflammation or recent infection, or recent surgery.
Controls consisted of 130 age-matched (blocks of 5 years) and sex-matched healthy individuals who were recruited during physical check-ups and were free of the conditions stated in the exclusion criteria.
Determination of the severity and functional outcome of acute IS
Stroke severity was assessed based on infarct volume and the National Institutes of Health Stroke Scale (NIHSS; scores range from 0 to 42, with higher scores indicating greater deficits)50. We calculated the NIHSS scores on day 1 after IS for all patients and on day 6 after IS for the 109 patients who had second blood samples available on day 6. Stroke volume was evaluated based on initial diffusion-weighted imaging lesion volume (in 118 patients) by an experienced neuroradiologist who was unaware of the clinical and laboratory results, and it was calculated as the sum of the infarction areas on each slice multiplied by the slice thickness.
Using the mRS, functional outcome was assessed on day 90 after IS by a neurologist who was blinded to the clinical presentations and biochemical results of patients. The mRS scores of ≤2 and >2 corresponded to favourable and unfavourable outcomes, respectively.
Sample collection and measurement
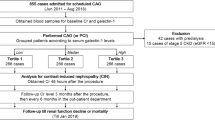
A flow chart of the study is shown in Fig. 3. Blood samples were collected in the morning after an overnight fast from 130 patients on day 1 after IS and were also collected from 109 patients on day 6 after IS. In the group of 130 patients, 4 patients died and 17 patients had been discharged or transferred within the first six days following admission. The characteristics of the latter subjects did not significantly differ from those of the 130 patients (Supplementary Table S3). Furthermore, the third blood samples from 39 patients were obtained in the 4th week after IS during their follow-up reviews. These 39 patients had lower NIHSS and mRS scores than those of the 109 patients (Supplementary Table S4). Blood samples were drawn from the control subjects during their physical check-ups after overnight fast.

LAA stroke, large artery atherosclerotic stroke; NIHSS, National Institutes of Health Stroke Scale; mRS, modified Rankin Scale.
Measurements of biochemical parameters, such as FBG, triglycerides, and total cholesterol (TC), were performed at the clinical laboratory in the hospital.
Serum samples were stored at −80 °C before being analysed. All samples were thawed only once prior to use. Gal-1, Gal-3, Gal-9, and Gal-3BP levels were measured using commercially available enzyme-linked immunosorbent assay (ELISA) kits (R&D Systems, Minneapolis, MN, USA; Catalogue number DGAL10, DGAL30, DGAL90, and DGBP30B). According to the instructions, the intra-assay and inter-assay coefficients of variation are, respectively, 5.7–8.8% and 7.5–9.5% for Gal-1, 3.0–4.4% and 6.8–8.6% for Gal-3, 3.4–3.7% and 5.2–5.6.0% for Gal-9, and 2.7–3.6% and 4.8–10.0% for Gal-3BP. The mean minimum detectable concentrations of Gal-1, Gal-3, Gal-9, and Gal-3BP are 22 pg/ml, 16 pg/ml, 8 pg/ml, and 22 pg/ml, respectively.
Data collection and definition
Baseline information was obtained at admission, including race, age, sex, history of health and medication use, smoking status, and alcohol use.
BMI was calculated as measured weight (kg) divided by the square of measured height (m2). The risk factors were defined as follows: hypertension (SBP/average diastolic blood pressure (DBP) ≥140/90 mmHg based on the average of two measurements, a history of hypertension, or use of antihypertensive medications), diabetes mellitus (FBG level ≥7 mmol/L, a history of diabetes, or use of antidiabetic treatments), dyslipidaemia (serum triglycerides ≥1.69 mmol/L, low-density lipoprotein cholesterol ≥3.37 mmol/L, high-density lipoprotein cholesterol ≤0.91 mmol/L, or the use of lipid-lowering drugs), smokers (who were currently smoking or had quit smoking within the past year), and alcohol consumers (who consumed ≥2 standard alcoholic beverages per day).
Statistical analysis
Continuous variables with a normal distribution are expressed as the means ± standard deviations, variables with a skewed distribution are expressed as medians (interquartile range), and variables with a skewed distribution normalized through a log10 transformation were expressed as the geometric means ± approximate SD. Categorical data are presented as counts and proportions. For univariate analysis, differences in the clinical data were analysed by Student’s t-test, the Mann-Whitney U test, and Pearson’s chi-square statistic, as appropriate. The time-course data between two time points were analysed by a matched t-test or Wilcoxon signed-rank test, and data between three time points were compared by a repeated measurement ANOVA with post hoc matched t-tests or the Friedman M test with post hoc Wilcoxon signed-rank tests, using the Bonferroni correction for p. Correlation analyses were assessed using either Pearson’s correlation or Spearman’s rank correlation, as appropriate. Multivariate analysis was performed using binary logistic regression analysis adjusted for potential influencing factors. Data analyses were performed using SPSS version 18.0 (SPSS Inc., Chicago, IL, USA). p < 0.05 was considered statistically significant unless otherwise noted.
Additional Information
How to cite this article: He, X.-W. et al. Serum levels of galectin-1, galectin-3, and galectin-9 are associated with large artery atherosclerotic stroke. Sci. Rep. 7, 40994; doi: 10.1038/srep40994 (2017).
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
Perillo, N. L., Marcus, M. E. & Baum, L. G. Galectins: versatile modulators of cell adhesion, cell proliferation, and cell death. J. Mol. Med. 76, 402–412 (1998).
Rabinovich, G. A. Galectins: an evolutionarily conserved family of animal lectins with multifunctional properties; a trip from the gene to clinical therapy. Cell Death Differ. 6, 711–721 (1999).
Dhirapong, A., Lleo, A., Leung, P., Gershwin, M. E. & Liu, F. T. The immunological potential of galectin-1 and -3. Autoimmun. Rev. 8, 360–363 (2009).
Barrionuevo, P. et al. A novel function for galectin-1 at the crossroad of innate and adaptive immunity: galectin-1 regulates monocyte/macrophage physiology through a nonapoptotic ERK-dependent pathway. J. Immunol. 178, 436–445 (2007).
Fusco, O. et al. 90K (MAC-2 BP) gene expression in breast cancer and evidence for the production of 90K by peripheral-blood mononuclear cells. Int. J. Cancer 79, 23–26 (1998).
Hepojoki, J. et al. Acute hantavirus infection induces galectin-3-binding protein. J. Gen. Virol. 95, 2356–2364 (2014).
Burguillos, M. A. et al. Microglia-secreted galectin-3 acts as a toll-like receptor 4 ligand and contributes to microglial activation. Cell Rep. 10, 1626–1638 (2015).
Nielsen, C. T. et al. Plasma levels of galectin-3-binding protein reflect type I interferon activity and are increased in patients with systemic lupus erythematosus. Lupus Sci Med 1, 2014–000026 (2014).
Al-Ansari, S., Zeebregts, C. J., Slart, R. H., Peppelenbosch, M. & Tio, R. A. Galectins in atherosclerotic disease. Trends Cardiovasc. Med. 19, 164–169 (2009).
Iacobini, C. et al. Accelerated lipid-induced atherogenesis in galectin-3-deficient mice: role of lipoxidation via receptor-mediated mechanisms. Arterioscler Thromb Vasc Biol 29, 831–836 (2009).
MacKinnon, A. C. et al. Inhibition of galectin-3 reduces atherosclerosis in apolipoprotein E-deficient mice. Glycobiology 23, 654–663 (2013).
Foks, A. C. et al. T-cell immunoglobulin and mucin domain 3 acts as a negative regulator of atherosclerosis. Arterioscler. Thromb. Vasc. Biol. 33, 2558–2565 (2013).
Ho, J. E. et al. Galectin-3, a marker of cardiac fibrosis, predicts incident heart failure in the community. J. Am. Coll. Cardiol. 60, 1249–1256 (2012).
Zhu, R. et al. Serum Galectin-9 Levels Are Associated with Coronary Artery Disease in Chinese Individuals. Mediators Inflamm 457167, 18 (2015).
Koths, K., Taylor, E., Halenbeck, R., Casipit, C. & Wang, A. Cloning and characterization of a human Mac-2-binding protein, a new member of the superfamily defined by the macrophage scavenger receptor cysteine-rich domain. J. Biol. Chem. 268, 14245–14249 (1993).
Martinez, V. G., Moestrup, S. K., Holmskov, U., Mollenhauer, J. & Lozano, F. The conserved scavenger receptor cysteine-rich superfamily in therapy and diagnosis. Pharmacol. Rev. 63, 967–1000 (2011).
Ho, M. K. & Springer, T. A. Mac-2, a novel 32,000 Mr mouse macrophage subpopulation-specific antigen defined by monoclonal antibodies. J. Immunol. 128, 1221–1228 (1982).
Tinari, N. et al. Glycoprotein 90K/MAC-2BP interacts with galectin-1 and mediates galectin-1-induced cell aggregation. Int. J. Cancer 91, 167–172 (2001).
Shaked, I. et al. Macrophage inflammatory markers are associated with subclinical carotid artery disease in women with human immunodeficiency virus or hepatitis C virus infection. Arterioscler. Thromb. Vasc. Biol. 34, 1085–1092 (2014).
Gleissner, C. A. et al. Galectin-3 binding protein plasma levels are associated with long-term mortality in coronary artery disease independent of plaque morphology. Atherosclerosis 251, 94–100 (2016).
Wang, J. et al. Galectin-1-secreting neural stem cells elicit long-term neuroprotection against ischemic brain injury. Sci. Rep. 5, 9621 (2015).
Yamane, J. et al. Transplantation of human neural stem/progenitor cells overexpressing galectin-1 improves functional recovery from focal brain ischemia in the Mongolian gerbil. Mol Brain 4, 1756–6606 (2011).
Wei, D., Ren, C., Chen, X. & Zhao, H. The chronic protective effects of limb remote preconditioning and the underlying mechanisms involved in inflammatory factors in rat stroke. PLoS One 7, e30892 (2012).
Kusaka, H. et al. Clinical significance of plasma galectin-3 in patients with coronary artery disease. International journal of cardiology 201, 532–534 (2015).
Adams, H. P. Jr. et al. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke 24, 35–41 (1993).
Sano, H. et al. Human galectin-3 is a novel chemoattractant for monocytes and macrophages. J. Immunol. 165, 2156–2164 (2000).
Sano, H. et al. Critical role of galectin-3 in phagocytosis by macrophages. J. Clin. Invest. 112, 389–397 (2003).
Arar, C., Gaudin, J. C., Capron, L. & Legrand, A. Galectin-3 gene (LGALS3) expression in experimental atherosclerosis and cultured smooth muscle cells. FEBS Lett. 430, 307–311 (1998).
Madrigal-Matute, J. et al. Galectin-3, a biomarker linking oxidative stress and inflammation with the clinical outcomes of patients with atherothrombosis. J. Am. Heart Assoc. 3, e000785 (2014).
Hollander, M. et al. Carotid plaques increase the risk of stroke and subtypes of cerebral infarction in asymptomatic elderly: the Rotterdam study. Circulation 105, 2872–2877 (2002).
Wiersma, V. R., de Bruyn, M., Helfrich, W. & Bremer, E. Therapeutic potential of Galectin-9 in human disease. Med. Res. Rev. 33, E102–E126 (2013).
Spitz, C. et al. Regulatory T cells in atherosclerosis: critical immune regulatory function and therapeutic potential. Cell. Mol. Life Sci. 73, 901–922 (2016).
Foks, A. C., Lichtman, A. H. & Kuiper, J. Treating atherosclerosis with regulatory T cells. Arterioscler. Thromb. Vasc. Biol. 35, 280–287 (2015).
Edsfeldt, A. et al. High plasma levels of galectin-3 are associated with increased risk for stroke after carotid endarterectomy. Cerebrovasc. Dis. 41, 199–203 (2016).
Starossom, S. C. et al. Galectin-1 deactivates classically activated microglia and protects from inflammation-induced neurodegeneration. Immunity 37, 249–263 (2012).
Sakaguchi, M. & Okano, H. Neural stem cells, adult neurogenesis, and galectin-1: from bench to bedside. Dev. Neurobiol. 72, 1059–1067 (2012).
Sharma, U. C. et al. Galectin-3 marks activated macrophages in failure-prone hypertrophied hearts and contributes to cardiac dysfunction. Circulation 110, 3121–3128 (2004).
van Kimmenade, R. R. et al. Utility of amino-terminal pro-brain natriuretic peptide, galectin-3, and apelin for the evaluation of patients with acute heart failure. J. Am. Coll. Cardiol. 48, 1217–1224 (2006).
Tunon, J. et al. Usefulness of a combination of monocyte chemoattractant protein-1, galectin-3, and N-terminal probrain natriuretic peptide to predict cardiovascular events in patients with coronary artery disease. Am. J. Cardiol. 113, 434–440 (2014).
Maiolino, G. et al. Galectin-3 predicts long-term cardiovascular death in high-risk patients with coronary artery disease. Arterioscler. Thromb. Vasc. Biol. 35, 725–732 (2015).
Daniels, L. B., Clopton, P., Laughlin, G. A., Maisel, A. S. & Barrett-Connor, E. Galectin-3 is independently associated with cardiovascular mortality in community-dwelling older adults without known cardiovascular disease: the Rancho Bernardo Study. Am. Heart J. 167, 674–682 (2014).
de Boer, R. A. et al. The fibrosis marker galectin-3 and outcome in the general population. Journal of internal medicine 272, 55–64 (2012).
Denes, A., Thornton, P., Rothwell, N. J. & Allan, S. M. Inflammation and brain injury: acute cerebral ischaemia, peripheral and central inflammation. Brain Behav. Immun. 24, 708–723 (2010).
Krupinski, J., Kaluza, J., Kumar, P., Kumar, S. & Wang, J. M. Role of angiogenesis in patients with cerebral ischemic stroke. Stroke 25, 1794–1798 (1994).
Greenberg, D. A. & Jin, K. From angiogenesis to neuropathology. Nature 438, 954–959 (2005).
Chen, H. H., Chien, C. H. & Liu, H. M. Correlation between angiogenesis and basic fibroblast growth factor expression in experimental brain infarct. Stroke 25, 1651–1657 (1994).
van der Hoeven, N. W. et al. The emerging role of galectins in cardiovascular disease. Vascul. Pharmacol. 81, 31–41 (2016).
Feldmann, E. et al. Chinese-white differences in the distribution of occlusive cerebrovascular disease. Neurology 40, 1541–1545 (1990).
Stroke–1989 . Recommendations on stroke prevention, diagnosis, and therapy. Report of the WHO Task Force on Stroke and other Cerebrovascular Disorders. Stroke 20, 1407–1431 (1989).
Brott, T. et al. Measurements of acute cerebral infarction: a clinical examination scale. Stroke 20, 864–870 (1989).
Acknowledgements
This work was supported by the Zhejiang Provincial Scientific Project of Medicine and Health (grant number: 2017KY705; 2016KYA186; 2015KYB435), the Natural Science Foundation of Zhejiang Province (grant number: LY16H070008), and special funds from the Regional Centre for Disease of Zhejiang Province.
Author information
Authors and Affiliations
Contributions
X.W.H. and X.P.J. designed the experiments; X.W.H., W.L.L. and C.L. performed the experiments; P.L. and M.Z. contributed to the specimen collection; X.W.H. and Y.G.S. analysed the data and wrote the manuscript. All authors reviewed and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Supplementary information
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
He, XW., Li, WL., Li, C. et al. Serum levels of galectin-1, galectin-3, and galectin-9 are associated with large artery atherosclerotic stroke. Sci Rep 7, 40994 (2017). https://doi.org/10.1038/srep40994
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep40994
This article is cited by
-
Novel insights into molecular signatures and pathogenic cell populations shared by systemic lupus erythematosus and vascular dementia
Functional & Integrative Genomics (2023)
-
The interplay of galectins-1, -3, and -9 in the immune-inflammatory response underlying cardiovascular and metabolic disease
Cardiovascular Diabetology (2022)
-
Neuroinflammation and galectins: a key relationship in neurodegenerative diseases
Glycoconjugate Journal (2022)
-
Multi-proteomic approach to predict specific cardiovascular events in patients with diabetes and myocardial infarction: findings from the EXAMINE trial
Clinical Research in Cardiology (2021)
-
Galectin-1 is associated with the severity of coronary artery disease and adverse cardiovascular events in patients undergoing coronary angiography
Scientific Reports (2020)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
