
Abstract
Association between physical activity and mortality has rarely been investigated among the Chinese population. Furthermore, the most appropriate amount of physical activity for longevity benefits remains unclear. We used data from the Dongfeng-Tongji cohort, including 24,606 middle-aged and older retired adults in 2008 and followed to 2013, to quantify linear and non-linear dose-response relationships between regular physical activity and mortality risks by Cox proportional hazards model. Compared with participants who did not engage in regular physical activity, those performing regular physical activity had significantly 46%, 56%, and 49% decreased risks of mortality from all causes, circulatory, and respiratory diseases, respectively. Each one-SD increase in regular physical activity was associated with 32% decrease of respiratory disease mortality. There were significant nonlinear dose-response associations between regular physical activity and mortality from all causes and circulatory diseases. Mortality risks decreased monotonically with increased regular physical activity amount, and appeared to reach a threshold at around 100 MET-hours/week. More mortality benefits were found among non-smokers than that among current and former smokers. Our results suggest that middle-aged and older Chinese adults can achieve mortality benefits from regular physical activity at the WHO recommended minimum, and the benefit threshold appears at approximately 100 MET hours/week.
Similar content being viewed by others

Introduction
Physical activity has been associated with decreased risk of mortality from all causes, cardiovascular diseases and cancers1,2,3. According to data from the World Health Organization (WHO), lack of physical activity has been identified as the fourth leading risk factor for death globally4. It was estimated that 3.2 million deaths were attributed to insufficient physical activity every year5. WHO recommends that adults do at least 150 minutes of moderate intensity (3 to <6 metabolic equivalent tasks [MET, a physiological measure, can express the energy cost of physical activities. A MET equals one kcal per hour for per kilogram of bodyweight]) or 75 minutes of vigorous intensity (≥6 METs) aerobic physical activity throughout a week (≥7.5 MET hours/week) or an equivalent combination of moderate and vigorous intensity activity6. In China, over 66% of the general population participated in physical activity beyond the WHO recommended minimum7. Currently, no guidelines for physical activity are available in China, and whether Chinese adults can benefit from physical activity according to the WHO recommendation remains unclear.
Cumulative evidence has shown that physical activity can decrease mortality; however, the health benefits among elderly remain fairly sparse. While the health benefits appear greater among older populations than younger adults8, adverse effects of physical activity are also found among the elderly population as it can be of trigger of sudden deaths9,10,11. Therefore, it is of importance and interest to identify if there is a threshold for mortality risk associated with physical activity especially among elderly. To date, only one study among the US general populations reported that an upper threshold for mortality benefits occurred at 22.5 to 40.0 MET-hours/week, though leisure-time physical activity of more than 40 MET-hours/week did not appear to be associated with elevated mortality risk12. However, this study did not account for non-leisure time activities especially occupational physical activity, which might result in exposure misclassification. A clearer separation of occupational and non-occupational physical activity benefits is needed to be addressed.
In this study, we investigated the associations between regular physical activity and risks from total and cause-specific mortality in the Dongfeng-Tongji (DFTJ) cohort of 24 606 middle-aged and older retired Chinese. Both linear and nonlinear dose-response analyses were conducted to quantify the associations and identify potential thresholds for mortality risk associated with regular physical activity.
Results
Table 1 summaries selected characteristics of the study participants by regular physical activity. Over 44.3% of the participants were males. Mean age of all the participants was 63 ranging from 45 to 95 years. Approximately 95% of the participants performed physical activity less than 75 MET-hours/week, including 2862 participants who reported no regular physical activity. There are 82.2% of subjects performing equal to or more than the WHO recommended minimum (7.5 MET-hours/week). Among all the participants, 41.2% were overweight (28 > BMI ≥ 25) or obese (BMI ≥ 28), 2.6% were underweight, and 2.5% were without data on BMI. Current and former smokers accounted for 29.5% of all participants, while current and former drinker accounted for 26.6%.
Mortality rates by regular physical activity is presented in Table 2. There were 125,591 person-years in total. The overall mortality was 10.0 per 1000 person-years. The identified 1267 deaths included 436 (mortality rate: 3.5 per 1000 person-years) deaths from neoplasms, 458 (3.6) from circulatory diseases, 84 (0.7) from respiratory diseases, 37 (0.3) from digestive diseases, 46 (0.4) from external causes of morbidity and mortality.
Table 3 shows results of the dose-response analyses for regular physical activity and mortality risk. Compared with no regular physical activity, participants reporting regular physical activity show a significant 46%, 56%, and 49% decrease of mortality from all causes, circulatory diseases and respiratory diseases, respectively. Each one-SD increase (24.3 MET-hours/week) in regular physical activity was associated with 22%, 30%, and 32% decrease of mortality from all causes, circulatory diseases and respiratory diseases, respectively. The categorical analyses also showed similar results with significant decreasing Hazard Ratio (HR) trends for categories of regular physical activity in relation to total and cause-specific mortality. Participants performing regular physical activity but less than 7.5 MET-hours/week (the WHO recommended minimum) were also significantly associated with reductions of mortality risk from total and circulatory diseases (HR: 0.69 [0.54–0.88] and 0.65 [0.44–0.95] respectively). No significant associations were observed between lower mortality risks from neoplasms and respiratory diseases and increasing regular physical activity amount until 37.5 to 75 MET-hours/week. The results also showed that total and neoplasms mortality risks decreased monotonically with increasing regular physical activity amount. For circulatory diseases and respiratory diseases, the mortality risks decreased and appeared to reach a threshold among participants performing 35.7 to 75 MET-hours/week regular physical activity. The results of sensitivity analysis among those who are in normal retirement age (more than 60 years old for male and 50 for female in China) are similar to those in the whole participants (data not shown).
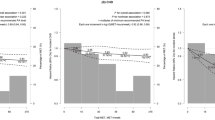
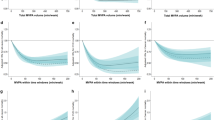
We further examined the nonlinear dose-response associations for regular physical activity and risks of mortality by the penalized spline models. There were significant nonlinear dose-response associations for regular physical activity and risks of mortality from all causes, circulatory diseases, ischaemic heart diseases and cerebrovascular diseases (all p values for nonlinear trend <0.05) (Fig. 1). The results showed that total mortality risk decreased monotonically, and appeared to reach a threshold at around 100 MET-hours/week. No significant nonlinear associations were observed between regular physical activity amount and risks of mortality from neoplasms and respiratory diseases.

Abbreviations: MET, metabolic equivalent. SD, standard deviation. The causes of death were coded according to the 10th version of the International Classification of Diseases (ICD-10). Hazard ratios were estimated by using the Cox proportional hazards model, with adjustment for sex, age, BMI, marriage, education, smoking status, and drinking status at baseline. The horizontal dotted red line in each panel represents a HR of 1.0. Solid lines represent HRs, with dotted lines indicating the 95% CI.
As shown in Table 4, stratified analyses gave similar dose-response associations between regular physical activity and total mortality risk by age, BMI, marriage status, education, and drinking status; however, we observed different associations modified by smoking status (p effect modification = 0.04). Regular physical activity appeared to decrease total mortality risk more among non-smokers than ever smokers (including current and former smokers).
Discussion
In this prospective cohort study of 24 606 middle-aged and older Chinese retired adults, we observed significant dose-response associations between regular physical activity and decreased risks of mortality from all diseases, neoplasms, circulatory diseases and respiratory diseases. The association can be modified by smoking. We also found Chinese middle-aged and older adults can achieve mortality benefits from regular physical activity at the WHO recommended minimum, and the benefit threshold appears at approximately 100 MET hours/week.
Many studies have demonstrated that increased physical activity was associated with total mortality risk decline. A dose-response meta-analysis of 80 cohort studies reported that physical activity at the highest level can lower 35% risk of total mortality when compared with the lowest level8. A pooled analysis from six studies in United States and Europe to conduct the dose-response relationship between physical activity and mortality, reporting a lower risk between 20 and 39% of total mortality among those with physical activity compared with those reporting no physical activity12. Our findings showed that participants with regular physical activity were associated with a 31 to 61% lower risk of total mortality when compared with those who did not engage in regular physical activity, which are higher than the results from Arem et al. and Wen et al.12,13. An important reason is the different measurement of physical activity amount between the studies. According to the WHO recommendation, physical activity includes leisure-time physical activity, transportation, occupational, household chores, exercise, and community activities14. Arem et al. and Wen et al. assessed the effects of leisure-time physical activity on mortality, while in this study we focused on regular physical activities not only leisure-time physical activity, but also transportation and exercise. Another possible reason for more mortality benefits in regular physical activity in this study is that types and intensity of physical activity among the Chinese population are different from adults in some Western studies. Chinese people prefer moderate intensity physical activities such as walking, biking, and tai chi to vigorous intensity activities15. A few studies have assessed the effects of physical activity intensity independently on mortality risk, but the results are inconsistent. A study among late middle aged adults showed that moderate physical activity was associated with a 33% decreased risk of mortality, while no significant association was observed between vigorous activity and mortality16. In contrast, several studies have concluded that vigorous intensity physical activity may have a greater benefit for reducing risk of mortality than moderate intensity among adults aged between 28 and 868,17. Age is another factor affecting the association between physical activity and mortality. A larger reduction in mortality tends to be observed among older than younger adults8,18. In our study, 62% of the participants were aged over 60. Stratified analyses suggested that each one-SD increase in regular physical activity was associated with a 16–28% reduction of total mortality among adults aged over 60, whilst there was 19% reduction among those aged under 60 in this study. This may have been due to retirement transition in the elderly as physical activity patterns and amount can alter after retirement. All the subjects enrolled in this study are all in retirement. Chinese older people who are retired do not go to work, therefore they will spend more time on mild or moderate physical activity such as walking, dancing, or playing tai chi, compared to those are working. Barnett et al. reported that the amount of exercise and leisure-time physical activity increases after the retirement transition19. Similarly, a recent longitudinal study has confirmed this and observed that the amount and intensity of physical activity could change by the type of transition out of full-time employment among middle-aged and older adults20. All participants enrolled in this study were retired workers, who have no occupational physical activity and may spend more time on regular non-occupational physical activity, gaining more mortality benefits from physical activity than those in other studies.
Physical activity is believed to help reduce cancer risk, but the results are inconsistent among studies in the elderly1,12,21,22. A cohort study of Japanese elderly adults reported no clear associations between an overall index of physical activity and cancer mortality, although a moderate reduction of risk was observed22; while Wu et al. found frequency of physical activity were associated with a lower cancer mortality21. In our study, we did not observe a significant association between neoplasms mortality and physical activity amount among lower than 37.5 MET-hour/week groups. A remarkable reduction of neoplasms mortality was observed when participants performed more than 37.5 MET-hours/week physical activity. A possible reason is the relatively small sample size for neoplasms, because the association between regular physical activity and neoplasm mortality is likely to be weak and difficult to detect. Further studies with larger sample sizes are needed to examine possible effects of physical activity on cancer mortality among elderly.
Our findings show that performing regular physical activity is an efficient way to reduce the risk of dying from diseases of the circulatory system, which are similar to previous studies23,24. Santulli et al. conducted a review on the benefits of moderate-intensity physical activity and found positive associations between physical training and aging25. According to Shiroma et al., the most active individuals have a 30 to 40% risk reduction of CHD and CVD, compared with the least active26. In our study, we found a 56% reduction of mortality from circulatory system diseases. It suggests that Chinese adults can benefit more from physical activity. Race may influence the dose-response association between risk of mortality from heart diseases and physical activity amount. Nonblack individuals more likely benefit from physical activity than blacks, but the association among Asians is still not clear because of rarely examined27.
We also noted that smoking was a potential effect modifier of the association. A greater reduction of mortality risk is associated with increased regular physical activity amount among non-smokers compared with those among smokers, which is similar to a cross-sectional and longitudinal analyses among Swedish adults28. Both smoking and physical inactivity can increase mortality risk independently. In this study, smokers typically participated in less physical activities compared with non-smokers, which might lead to greater reduction of total mortality among non-smokers. However, a study among 40–60 year-old employees in Finland reported that physical activity amount can lower mortality risk among smokers, but no association was found among non-smokers29.
Our findings show that regular physical activity can decrease mortality risk among middle-aged and older Chinese adults, suggesting that intervention strategies to promote regular physical activity should be a major health priority. Until now, there are no guidelines for physical activity levels in the mainland of China. In the present study, the regular physical activity levels lower than the WHO recommended minimum (0.1 to 7.4 MET-hours/week) are observed to be associated with a 31% reduction in risk of total mortality, which is higher than that from the report of the Physical Activity Guidelines Advisory Committee30. Furthermore, an increase in the amount of physical activity is associated with an additional reduction of total mortality risk at smaller magnitudes, but it seems that 7.5 MET-hours/week of physical activity is effective in reducing mortality and should be achievable among middle-aged and older retired adults in China. We also noted that the benefit threshold of regular physical activity appears to be 100 MET-hours/week. There are few studies which focus on the upper threshold of physical activity12, however, one study which pooled data from 6 studies in the National Cancer Institute Cohort Consortium reported that a threshold for mortality benefit occurred at 3–5 times the WHO recommendation. The study reported a reduction of mortality risk at the highest physical activity of equal or more than 75 MET-hours/week, but there was no detail on mortality benefit for physical activity beyond 75 MET-hours/week. Our results confirm and extend the previous study to calculate the upper threshold by using both categorical and non-linear models. We still observed a reduced risk of total mortality at more than 5 times the recommended minimum and a higher upper threshold appeared at 100 MET-hours/week12. This indicates that people can achieve more mortality benefits through performing more regular physical activity up to 100 MET-hours/week. These findings have important public health implications on future guidelines of regular physical activity, especially in China.
There are some strengths of this study. First, all participants enrolled in this study are retired workers, eliminating potential confounding by occupational physical activity. Second, we had a wide range of regular physical activity amount, which enabled us to examine the upper threshold of mortality benefits. Finally, we quantified the dose-response relationship between regular physical activity and mortality by both linear and non-linear analyses, and the results from the different models are consistent. Meanwhile, nonlinear analyses represent a detail dose-response association between regular physical activity and mortality, especially at high level of physical activity.
One limitation in our study is that the relatively short follow-up time. All the information about physical activity is self-reported. Recall bias on duration of regular physical activity, especially in earlier years may exist. Moreover, we did not measure the accurate intensity of certain type of regular physical activity. Instead, we assessed the physical activity intensity by types of physical activity according to MET equivalents of common physical activities classification. Furthermore, in this study, we included participants in early retirement. According to the State Council Provisional Regulations on Retirement and Resignation of Workers in China, males who are reaching the age of 50, females 45, with a seniority of ten years of continuous service, certified in hospital and confirmed by the labor appraisal committee as being completely incapacitated should retire. Younger subjects in our study may cause bias on the relationship. However, we excluded those suffering severe diseases which may affect physical activities in the present study. Meanwhile, we conducted a sensitive analysis to quantify the association between mortality risks and regular physical activity among those a participants retired in the normal age (more than 60 years old for male and 50 for female), and the results are similar to those among whole subjects. Another limitation is that we did not examine any effects of types, intensity, duration, or frequency of physical activity independently, although we considered all of them when estimating the physical activity amount. The types and intensity of physical activity among Chinese adults maybe different from individuals in Western countries. Further studies are needed to investigate the associations between types or intensity of physical activity and mortality risk among Chinese adults.
In conclusion, regular physical activity is negatively associated with total and cause-specific mortality risks, and the benefit threshold from regular physical activity appears at approximately 100 MET hours/week among middle-aged and older Chinese retired adults. Non-smokers might gain more health benefits from regular physical activity. Regular physical activity should therefore be encouraged to promote positive health outcomes in China.
Methods
Study design, setting and participants
This study included 24 606 participants from the DFTJ cohort, which has been described elsewhere31. In brief, the cohort included 27 009 residents in retirement and from different communities in Shiyan city, China. It was established and collected for baseline information between September 2008 and June 2010, and then followed up until October 31, 2013. A total of 25 978 participants (96.2%) completed the follow-up, yielding in 125 591 person-years with a median of 5.1 years follow-up. Trained investigators used questionnaires to collect information on demographics, education, marriage status, smoking, alcohol consumption, regular physical activity, and vital status. By excluding 479 participants with a diagnosis of malignant neoplasms and 893 participants without information on regular physical activity, 24 606 participants were included in the final analysis.
Ethics Statement
The research protocol was approved by the Ethics and Human Subject Committee of Tongji Medical College, Huazhong University of Science and Technology, P.R. China. The methods were carried out in accordance with the relevant guidelines. All participants enrolled gave written informed consent for participation.
Exposure assessment
We collected baseline self-reported information on regular physical activity from each participant through the questionnaire by asking five questions: “Did you do regular physical activity in the past six month, which lasts at least 20 minutes each time?”, “Which type of physical activity did you do? (Including leisure-time physical activity, transportation and exercises)”, “How many times did you do on regular physical activity each week?” “How long did you spend on physical activity each time?”, “How many years have you done regular physical activity?” We considered 9 types of regular physical activity, including walking, biking, dancing, tai chi, doing exercise in gym, playing ball games, jogging, swimming, and climbing. For each participant, energy expended by each type of physical activity was calculated by multiplying estimated metabolic equivalent (MET) value by the duration in hours/week. The estimated MET hours/week for regular physical activities were 3 for walking, 4 for biking, 4.5 for tai chi, 7.5 for jogging or swimming, 5 for dancing, 4.5 for climbing, 6 for playing ball games or doing exercise in gym32,33. We then summed across all types of regular physical activities for each subject to estimate the overall energy expenditure in MET hours/week.
Outcomes
Each subject has a unique medical insurance card number in the medical insurance system. We used this system to track each subject’s vital status, and obtained underlying cause of death for each deceased. The 10th version of the International Classification of Diseases (ICD-10) was used to code the causes of death. In this study, we divided causes of death into those resulting from all causes (ICD-10: A00-Y98), and specific diseases including Neoplasms (C00-C97), diseases of the circulatory system (I00-I99), and diseases of the respiratory system (J00-J99).
Statistical analysis
We conducted quantitative dose-response analyses using the Cox proportional hazards model. HR and 95% confidence intervals (CIs) for mortality risk with regular physical activity were estimated, with adjustment for sex, age, BMI, marriage status, education, smoking status, and drinking status. By including regular physical activity as a dichotomized variable (yes/no), we estimated the HR for regular physical activity in relation to mortality risk in comparison with no regular physical activity. We also estimated the HR associated with each one-standardized deviation (SD) increase in regular physical activity, by including regular physical activity as a continuous variable in the model. To examine shape of the dose-response relationship, we conducted categorical analyses by dividing regular physical activity into six categories, including no regular physical activity (0), 0.1 to <7.5, 7.5 to <22.5, 22.5 to <37.5, 37.5 to <75, and ≥75 MET-hours/week. The cutpoints of these categories were 1, 3, 5, and 10 times the recommended minimum of WHO physical activity guidelines (7.5 MET-hours/week), respectively. In addition, we examined nonlinearity of the dose-response relationships by integrating penalized splines in the Cox proportional hazards model. Furthermore, we conducted a sensitivity analysis to explore the potential effect of physical activity on mortality among those who were in early retirement.
We conducted stratified analyses by using Cox proportional hazards models to investigate whether covariates modified the association between regular physical activity and total mortality risk, Effect modification of each stratification variable was performed by likelihood ratio tests by comparing two nested multivariate models with and without an interaction term of regular physical activity and the stratification variable. A p value larger than 0.05 was considered no significant effect modification. We conducted all data analyses using R 3.2.3 software. All p values were 2-sided.
Additional Information
How to cite this article: Zhou, Y. et al. Association of regular physical activity with total and cause-specific mortality among middle-aged and older Chinese: a prospective cohort study. Sci. Rep. 7, 39939; doi: 10.1038/srep39939 (2017).
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
Li, T. et al. The dose-response effect of physical activity on cancer mortality: findings from 71 prospective cohort studies. British journal of sports medicine, doi: 10.1136/bjsports-2015-094927 (2015).
Loprinzi, P. D. & Davis, R. E. Effects of individual, combined, and isolated physical activity behaviors on all-cause mortality and CVD-specific mortality: Prospective cohort study among U.S. adults. Physiology & behavior 151, 355–359, doi: 10.1016/j.physbeh.2015.07.032 (2015).
Moore, S. C. et al. Leisure time physical activity of moderate to vigorous intensity and mortality: a large pooled cohort analysis. PLoS medicine 9, e1001335, doi: 10.1371/journal.pmed.1001335 (2012).
World Health Organization. Global Strategy on Diet, Physical Activity and Health. http://www.who.int/dietphysicalactivity/pa/en/ (2011).
World Health Organization. Global Strategy on Diet, Physical Activity and Health. http://www.who.int/dietphysicalactivity/factsheet_inactivity/en/ (2011).
World Health Organization. Global recommendations on physical activity for health. http://www.who.int/dietphysicalactivity/leaflet-physical-activity-recommendations.pdf?ua=1.
Muntner, P. et al. Prevalence of physical activity among Chinese adults: results from the International Collaborative Study of Cardiovascular Disease in Asia. American journal of public health 95, 1631–1636, doi: 10.2105/AJPH.2004.044743 (2005).
Samitz, G., Egger, M. & Zwahlen, M. Domains of physical activity and all-cause mortality: systematic review and dose-response meta-analysis of cohort studies. International journal of epidemiology 40, 1382–1400, doi: 10.1093/ije/dyr112 (2011).
Durakovic, Z., Durakovic, M. M., Skavic, J. & Gojanovic, M. D. Physical activity and sudden cardiac death in elders–a Croatian study. Collegium antropologicum 35, 103–106 (2011).
Maron, B. J. The paradox of exercise. The New England journal of medicine 343, 1409–1411, doi: 10.1056/NEJM200011093431911 (2000).
Albert, C. M. et al. Triggering of sudden death from cardiac causes by vigorous exertion. The New England journal of medicine 343, 1355–1361, doi: 10.1056/NEJM200011093431902 (2000).
Arem, H. et al. Leisure time physical activity and mortality: a detailed pooled analysis of the dose-response relationship. JAMA internal medicine 175, 959–967, doi: 10.1001/jamainternmed.2015.0533 (2015).
Wen, C. P. et al. Minimum amount of physical activity for reduced mortality and extended life expectancy: a prospective cohort study. Lancet 378, 1244–1253, doi: 10.1016/S0140-6736(11)60749-6 (2011).
World Health Organization. Global Strategy on Diet, Physical Activity and Health. http://www.who.int/dietphysicalactivity/factsheet_adults/en/. Global Strategy on Diet, Physical Activity and Health (2011).
Yucheng Guo, Haiyang Shi, Dinghai Yu & Pixiang Qiu . Health benefits of traditional Chinese sports and physical activity for older adults: A systematic review of evidence Journal of Sport and Health Science 5, 270–280 (2016).
Sabia, S. et al. Effect of intensity and type of physical activity on mortality: results from the Whitehall II cohort study. American journal of public health 102, 698–704, doi: 10.2105/AJPH.2011.300257 (2012).
Gebel, K. et al. Effect of Moderate to Vigorous Physical Activity on All-Cause Mortality in Middle-aged and Older Australians. JAMA internal medicine 175, 970–977, doi: 10.1001/jamainternmed.2015.0541 (2015).
Bembom, O., van der Laan, M., Haight, T. & Tager, I. Leisure-time physical activity and all-cause mortality in an elderly cohort. Epidemiology 20, 424–430, doi: 10.1097/EDE.0b013e31819e3f28 (2009).
Barnett, I., van Sluijs, E. M. & Ogilvie, D. Physical activity and transitioning to retirement: a systematic review. American journal of preventive medicine 43, 329–336, doi: 10.1016/j.amepre.2012.05.026 (2012).
Feng, X., Croteau, K., Kolt, G. S. & Astell-Burt, T. Does retirement mean more physical activity? A longitudinal study. BMC public health 16, 605, doi: 10.1186/s12889-016-3253-0 (2016).
Wu, C. Y. et al. The association of physical activity with all-cause, cardiovascular, and cancer mortalities among older adults. Preventive medicine 72, 23–29, doi: 10.1016/j.ypmed.2014.12.023 (2015).
Ueshima, K. et al. Physical activity and mortality risk in the Japanese elderly: a cohort study. American journal of preventive medicine 38, 410–418, doi: 10.1016/j.amepre.2009.12.033 (2010).
Nocon, M. et al. Association of physical activity with all-cause and cardiovascular mortality: a systematic review and meta-analysis. European journal of cardiovascular prevention and rehabilitation: official journal of the European Society of Cardiology, Working Groups on Epidemiology & Prevention and Cardiac Rehabilitation and Exercise Physiology 15, 239–246, doi: 10.1097/HJR.0b013e3282f55e09 (2008).
Sofi, F., Capalbo, A., Cesari, F., Abbate, R. & Gensini, G. F. Physical activity during leisure time and primary prevention of coronary heart disease: an updated meta-analysis of cohort studies. European journal of cardiovascular prevention and rehabilitation : official journal of the European Society of Cardiology, Working Groups on Epidemiology & Prevention and Cardiac Rehabilitation and Exercise Physiology 15, 247–257, doi: 10.1097/HJR.0b013e3282f232ac (2008).
Santulli, G., Ciccarelli, M., Trimarco, B. & Iaccarino, G. Physical activity ameliorates cardiovascular health in elderly subjects: the functional role of the beta adrenergic system. Frontiers in physiology 4, 209, doi: 10.3389/fphys.2013.00209 (2013).
Shiroma, E. J. & Lee, I. M. Physical activity and cardiovascular health: lessons learned from epidemiological studies across age, gender, and race/ethnicity. Circulation 122, 743–752, doi: 10.1161/CIRCULATIONAHA.109.914721 (2010).
Folsom, A. R. et al. Physical activity and incidence of coronary heart disease in middle-aged women and men. Medicine and science in sports and exercise 29, 901–909 (1997).
Johansson, S. E. & Sundquist, J. Change in lifestyle factors and their influence on health status and all-cause mortality. International journal of epidemiology 28, 1073–1080 (1999).
Lallukka, T., Rahkonen, O., Lahelma, E. & Lahti, J. Joint associations of smoking and physical activity with disability retirement: a register-linked cohort study. BMJ open 5, e006988, doi: 10.1136/bmjopen-2014-006988 (2015).
Washington (District of Columbia): US Department of Health and Human Services. Physical Activity Guidelines Advisory Committee (2008) Physical Activity Guidelines Advisory Committee report (2008).
Wang, F. et al. Cohort Profile: the Dongfeng-Tongji cohort study of retired workers. International journal of epidemiology 42, 731–740, doi: 10.1093/ije/dys053 (2013).
Ainsworth, B. E. et al. Compendium of Physical Activities: a second update of codes and MET values. Medicine and science in sports and exercise 43, 1575–1581, doi: 10.1249/MSS.0b013e31821ece12 (2011).
Chen, M. et al. Different physical activity subtypes and risk of metabolic syndrome in middle-aged and older Chinese people. PloS one 8, e53258, doi: 10.1371/journal.pone.0053258 (2013).
Acknowledgements
We thank the study participants from Dongfeng-Tongji cohort for their help. This work was supported by the Natural Science Foundation of China (81573121), the 111 Project (B12004), the Program for Changjiang Scholars, the Innovative Research Team in University of Ministry of Education of China (IRT1246), and China Medical Board (12–113).
Author information
Authors and Affiliations
Contributions
Y.Z. contributed to data collection, conducted data analysis, interpreted the results, and wrote the manuscript. R.Z and Y.L. conducted data analysis, interpreted the results, and revised the manuscript. Y.G., D.W., M.H., J.Y., Y.L., X.Z., Y.W., H.G., S.W., X.M., and P.Y. helped to collect data and revised the manuscript. T.W. and W.C. designed the study, collected the data, interpreted the results, and revised the manuscript. All author have read the submitted manuscript and approved the final submission. W.C. is the guarantor of this work and has full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Zhou, Y., Zhang, R., Liu, Y. et al. Association of regular physical activity with total and cause-specific mortality among middle-aged and older Chinese: a prospective cohort study. Sci Rep 7, 39939 (2017). https://doi.org/10.1038/srep39939
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep39939
This article is cited by
-
Could the complying with WHO physical activity recommendations improve stress, burnout syndrome, and resilience? A cross-sectional study with physical education teachers
Sport Sciences for Health (2023)
-
Risk and protective factors for anxiety during COVID-19 pandemic
BMC Public Health (2021)
-
Objective evaluation of physical activity pattern using smart devices
Scientific Reports (2019)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
