
Abstract
The aim of this retrospective study was to characterise intrapartum and neonatal outcomes in women with an antenatally recorded Edinburgh Postnatal Depression Score (EPDS) ≤ 9 compared with women with a score of ≥12 at a major Australian tertiary maternity hospital. Women with scores ≥12 are at particularly high risk of major depressive symptomatology. There were 20512 (78.6%) women with a score ≤ 9 and 2708 (10.4%) had a score ≥ 12. Category 1 caesarean sections where there was immediate threat to life (maternal or fetal) were more common in women with EPDS scores ≥12 (5.2% vs. 4.3%, OR 1.24 95% CI 1.03–1.49, p = 0.024). Pre-term birth (<37 weeks) was also more common (11.7% vs. 8.6%, OR 1.38 95% CI 1.21–1.57, p < 0.001). Women with high scores had higher rates of babies with birth weights <5th centile (6.2% vs. 4.4%, p < 0.001). Apgar score < 7 at 5 minutes were more frequent in the high EPDS group (3.1% vs. 2%, OR 1.52 95% CI 1.18–1.93, p < 0.001). Resuscitation at birth (34.4% vs. 30.6%, p < 0.001) and neonatal death (0.48% vs. 0.13%, OR 2.52 95% CI 1.2–5.0, p < 0.001) were higher in babies of these women. These results suggest poorer intrapartum and neonatal outcomes for women with high EPDS scores.
Similar content being viewed by others


Introduction
The most common perinatal mental health disorders are depression and anxiety, however other conditions such as eating, personality and bipolar disorders, schizophrenia and psychotic illnesses are also not uncommon during pregnancy and the post-partum period1. The prevalence of major or minor depressive episodes during pregnancy is in the region of 6.5–12.9%, with almost 19% of women having a major episode in the first three months post-partum2. Risk factors for depression during pregnancy include low socioeconomic status, smoking, young age, unintended pregnancy, low income, lack of social support, life stress and domestic violence. There is evidence that obstetric and perinatal outcomes are worse in women3 with mental health problems with increased rates of complications such as preterm birth, low birth weight, neonatal intensive care unit (NICU) admission as well as increased risks of operative deliveries4,5,6,7. However not all studies have replicated these findings suggesting that the link between depression and adverse obstetric and perinatal outcomes may not be entirely straightforward8,9.
There are several screening tools that have been validated for use during pregnancy and the postpartum period to assist with identifying women, either at risk of, or suffering from perinatal depression10. However despite this, screening for depression is controversial because it has not been consistently shown to be of benefit and this uncertainty is reflected in various national guidelines and policies11.
The 10-item Edinburgh Postnatal Depression Scale (EPDS) is a widely used screening tool for depressive symptomatology and has been validated, both as an antenatal and postpartum screen for minor or major depression12. Although the EPDS is a screening tool for postpartum depression and not necessarily diagnostic for antenatal depression, it is generally accepted that high scores (≥12) are strongly indicative of major or minor depressive symptomatology. The EPDS is easy to administer and effective in its function, with high sensitivity and specificity. In addition, there is also evidence that the EPDS also measures symptoms of anxiety13,14 and therefore could serve as a proxy for both depression and anxiety. The purpose of this study was thus to correlate the results of the EPDS with intrapartum and neonatal outcomes at a major tertiary centre in Australia.
Materials and Methods
This was a retrospective observational study of women birthing under the public health system at the Mater Mothers’ Hospital in Brisbane, Australia between October 2007 and December 2013. Only women with non-anomalous pregnancies without documented pre-existing mental health issues were included in the study. The Mater Mothers’ Hospital is one of the largest tertiary obstetric hospitals in Australia with almost 10000 births per year. Maternal demographic, intra-partum and neonatal outcome data were collected from the hospital’s electronic maternity database. Gestational age was calculated from either the last menstrual period or earliest ultrasound examination. Maternal body mass index (BMI) was calculated based on measurement of height and weight recorded at the booking visit.
Demographic information collected included maternal age, body mass index (BMI), ethnicity, and country of birth, parity and maternal medical conditions (hypertension, gestational diabetes, thyroid disease). Intra-partum outcomes included mode of delivery, duration of labour and length of stay in hospital. Caesarean sections were categorised as planned or emergency including the degree of urgency. Classification of the degree of urgency of caesarean section is generally based on one of four categories15: Category 1 - immediate threat to life (maternal or fetal); Category 2 - maternal or fetal compromise that is not immediately life-threatening; Category 3 - needing early delivery but no maternal or fetal compromise; or Category 4 - delivery at the convenience of the patient or obstetric team. Professional bodies such as the American College of Obstetrics and Gynaecology, National Institute of Clinical Excellence in the United Kingdom and the Royal Australian and New Zealand College of Obstetricians and Gynaecologists all have broadly similar recommendations in that the decision to delivery interval for Category 1 caesarean sections should be no longer than 30 minutes. Perinatal outcome data included gestation at delivery, birth weight, Apgar scores < 7 at 5 min, umbilical artery pH < 7.2 and/or lactate > 4 mmol/L, need for resuscitation at birth, respiratory distress, infection, admission to the neonatal intensive care unit (NICU) and neonatal death.
All women completed the EPDS questionnaire at their booking visit regardless of gestation. For the majority of women this took place at <20 weeks gestation. Each of the 10 questions was scored by the patient on a 4-point scale from 0–3 with a possible total score ranging from 0 to 30. We stratified our study cohort into two groups: low score (≤9) and high score (≥12). This categorisation has been shown to be predictive of the severity of depression with scores ≥12 indicating particularly high risk of major depressive symptomatology16.
Statistical analysis for this study was performed using the R and the R commander program (R Foundation for Statistical Computing, Vienna, Austria). Categorical variables were compared using a Chi-squared test. Continuous normally distributed variables were compared using a two sample t test and non-normally distributed variables were compared using a Wilcoxon rank-sum test. Multivariate logistic regression, adjusted for maternal age, BMI and parity was used to examine the effect of EPDS scores on intra-partum and neonatal outcomes. The level of significance was set at 0.05. Summary statistics are reported as number (percentage) and median (inter-quartile range) as appropriate.
Ethical and governance approvals were granted by the Mater Human Research Ethics Committee and Research Governance Office respectively (Ref no: HREC/14/MHS/63).
Results
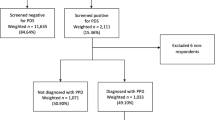
Over the study period there were 31071 non anomalous, public births at the Mater Mothers’ Hospital. We excluded 4961 women who did not have a recorded EPDS score leaving a final study cohort of 26110. There were 2708 women (10.4%) with an EPDS score ≥ 12, 2890 women (11.1%) with a score of 9–11 and 20512 women (78.5%) with a score of <9. The majority of women (88%) had the EPDS recorded at <20 weeks gestation.
Maternal demographics
Women with EPDS scores ≥ 12 were younger, born outside Australia and be significantly more obese (BMI > 40 kg/m2) compared to women with a score of <9. There was also a higher prevalence of indigenous women in this group. Maternal medical diseases (hypertension and thyroid disease) were more common in women with high EPDS scores. These women also had a longer hospital stay Table 1.
Intrapartum outcomes
There was no difference in the rates of normal vaginal deliveries, instrumental births or planned caesarean sections in women with high EPDS scores compared with women with low scores. Emergency caesarean section rates were however higher in women with scores >12 compared to those with scores <9 (19% vs. 17.5%, OR 1.16 95% CI 1.04–1.29, p = 0.006). Category 1 caesarean sections where there was immediate threat to life (maternal or fetal) were more common in women with EPDS scores ≥ 12 (5.2% vs. 4.3%, OR 1.24 95% CI 1.03–1.49, p = 0.024) Table 2.
Neonatal outcomes
Gestation at delivery was similar in both groups although there were greater rates of pre-term deliveries (<37 weeks) in women with EPDS scores ≥ 12 compared to those with scores <9 (11.7% vs. 8.6%, OR 1.38 95% CI 1.21–1.57, p < 0.001). Overall, women with high scores had babies with lower median birth weights (3330 g, IQR 2950–3696.3 g vs. 3420 g, IQR 3066–3765 g, p < 0.001), higher rates of babies with birth weights <10th centile (12.6% vs. 9.2%, p < 0.001) and <5th centile (6.2% vs. 4.4%, p < 0.001). Neonates with an Apgar score <7 at 5 minutes were also more frequent in the high EPDS group (3.1% vs. 2%, OR 1.52 95% CI 1.18–1.93, p < 0.001). Rates of NICU admission (4.7% vs. 3.7%), need for resuscitation at birth (34.4% vs. 30.6%, p < 0.001) and neonatal death (0.48% vs. 0.13%, OR 2.52 95% CI 1.2–5.0, p < 0.001) were all greater in women with high EPDS scores Table 3.
Discussion
The results from this study demonstrate that women with high EPDS scores have higher rates of emergency caesarean section particularly for concerns of fetal wellbeing. Our results also indicate that these women were significantly obese (BMI > 40 kg/m2), younger, of indigenous origin or more likely to have been born outside Australia. We also found a higher prevalence of maternal medical diseases (hypertension and thyroid disease) in women with high EPDS scores. We also found an association with low birth weight and pre-term birth and high maternal EPDS (≥12) scores. More worryingly however we demonstrate a higher prevalence of poorer newborn condition at birth, higher rates of NICU admission and neonatal death. To our knowledge some of these findings have not been previously reported.
Perinatal mental health disorders are important clinically, as up to 15–20% of women may be affected and this can impact maternal, fetal and neonatal outcomes. There is also a higher prevalence of depression and anxiety in women from low and middle income countries compared to those from high-income countries17. It is frequently unrecognized in pregnancy because depressive symptoms such as insomnia, poor appetite and decreased libido may be attributed to the normal physiological changes that occur during pregnancy and the puerperium. Furthermore, many women may be reluctant to report changes in their mood. Perinatal depression is often associated with poorer outcomes for mother–infant bonding and subsequent relationship and marital quality. There is good evidence that women with chronic psychotic conditions particularly schizophrenia are more likely to have adverse obstetric and neonatal outcomes including congenital malformations, preterm birth, fetal growth restriction, stillbirth, neonatal and sudden infant deaths. Some of these complications may however be related to the medication these women receive18,19,20,21.
In some other studies antenatal depression has not been shown (in contrast to our study) to be associated with hypertensive disorders, low Apgar scores or admission to NICU22. Although the risk of low birth weight and preterm birth may be increased in women with depression, the magnitude of this effect appears to be influenced to some degree by socioeconomic status and country of origin, with an increased risk seen in low and middle income countries (LMIC)23.
Some researchers have attempted to correlate fetal and neonatal outcomes with the use of antidepressants in pregnancy rather than with an actual diagnosis of depression. Although this is usually because of the availability of data of prescribing trends, it is nevertheless difficult to disentangle the effect of antidepressants, life style confounders, and depression24,25.
Depression and anxiety are both associated with increased concentrations of stress hormones. In particular, norepinephrine can cause uterine artery constriction5 which may reduce both antenatal and intrapartum utero-placental perfusion. This could potentially impair fetal growth and increase the risk of intrapartum fetal compromise precipitated by uterine contractions in labour. Another hormone released during stress is corticotrophin-releasing hormone (CRH) with higher concentrations found in women with depression and anxiety disorders. As CRH is a key modulator of parturition and cervical ripening its higher concentrations in the context of women with depression and anxiety could explain the increased risk of preterm birth seen in these women26,27. However, not all studies have shown an increase in CRH levels in women with depression28.
One possibility to explain the disparities in neonatal outcomes seen in our study is the “weathering hypothesis”29. In our study there were greater numbers of indigenous and Asian women as well as those born outside of Australia in the public cohort. Given that Australia accepts a large number of migrants and refugees from some of the most socially disadvantaged regions of the world, the psychosocial stress resulting from their cumulative experiences may prematurely “age or weather” the reproductive system, contributing to the increased rates of poorer outcomes seen in this study29,30. Although it may be speculative at this stage, it is possible that factors influencing perinatal outcomes may go beyond ethnicity, insurance status, maternal co-morbidities and age but may also include a woman’s previous social and psychological experiences.
Health professionals should be cognizant of the perinatal complications of mental health disorders both in pregnant women as well as women contemplating pregnancy so that appropriate surveillance, both maternal and fetal can be instituted. Women also need to be counselled about some of the potential intrapartum and perinatal complications associated with mental health problems and this is particularly important in the context of those on psychotropic medication. Although there isn’t robust evidence to suggest that preconception stabilisation of mental health improves perinatal outcomes, as a general principle this should be the aim. In addition, post conception professional and family support as well as optimisation of medication is critical in the management of these women.
The strengths of our study are the large sample size with prospectively collected EPDS scores at the booking visit and detailed perinatal outcomes. The limitations of our study include its retrospective nature, the lack of additional information on lifestyle, smoking, socioeconomic status, family support, substance abuse and use of non disclosed psychotropic or other medication, all of which could have influenced our results. Our results could also have been confounded if depression occurred after the initial EPDS screen. Nevertheless, our key findings particularly the increased risk of emergency caesarean section for fetal concerns and the adverse neonatal outcomes especially neonatal death are worrying and warrant further investigation.
Additional Information
How to cite this article: Navaratne, P. et al. Impact of a high Edinburgh Postnatal Depression Scale score on obstetric and perinatal outcomes. Sci. Rep. 6, 33544; doi: 10.1038/srep33544 (2016).
References
Howard, L. M. et al. Non-psychotic mental disorders in the perinatal period. Lancet. 384, 1775–1788 (2014).
Gavin, N. I. et al. Perinatal depression: a systematic review of prevalence and incidence. Obstet Gynecol. 106, 1071–1083 (2005).
Alder, J. et al. Depression and anxiety during pregnancy: a risk factor for obstetric, fetal and neonatal outcome? A critical review of the literature. J Matern Fetal Neonatal Med. 20, 189–209 (2007).
Orr, S. T., James, S. A. & Blackmore Prince, C. Maternal prenatal depressive symptoms and spontaneous preterm births among African-American women in Baltimore, Maryland. Am J Epidemiol. 156, 797–802 (2002).
Martini, J. et al. Anxiety disorders before birth and self-perceived distress during pregnancy: associations with maternal depression and obstetric, neonatal and early childhood outcomes. Early Hum Dev. 86, 305–310 (2002).
Hernandez-Martinez, C. et al. Relation between positive and negative maternal emotional states and obstetrical outcomes. Women Health. 51, 124–135 (2011).
Pavlov, M. et al. Obstetric and neonatal outcome in patients with anxiety disorders. J Matern Fetal Neonatal Med. 27, 1339–1342 (2014).
Andersson, L. et al. Neonatal outcome following maternal antenatal depression and anxiety: a population-based study. Am J Epidemiol. 159, 872–881 (2004).
Choi, S. K. et al. Impact of antenatal depression on perinatal outcomes and postpartum depression in Korean women. J Res Med Sci. 19, 807–812 (2014).
Screening for Perinatal Depression. Community Opinion No. 630. American College for Obstetricians and Gynecologists. Obstet Gynecol. 125, 1268–1271 (2015).
Thombs, B. D. et al. Diagnostic accuracy of the Edinburgh Postnatal Depression Scale (EPDS) for detecting major depression in pregnant and postnatal women: protocol for a systematic review and individual patient data meta-analyses. BMJ Open. 5, e009742, 10.1136/bmj-open-2015-009742 (2015).
Bowen, A. & Muhajarine, N. Prevalence of antenatal depression in women enrolled in an outreach program in Canada. J Obstet Gynecol Neonatal Nurs. 2006 35, 491–498 (2006).
Matthey, S., Fisher, J. & Rowe, H. Using the Edinburgh postnatal depression scale to screen for anxiety disorders: conceptual and methodological considerations. J Affect Disord. 146, 224–230 (2013).
Brouwers, E. P., van Baar, A. L. & Pop, V. J. Does the Edinburgh Postnatal Depression Scale measure anxiety? J Psychosom Res. 51, 659–663 (2001).
Grace, L., Greer, R. M. & Kumar, S. Perinatal consequences of a category 1 caesarean section at term. BMJ Open. 5, e007248, 10.1136/bmjopen-2014-007248 (2015).
Meijer, J. L. et al. Predictive accuracy of Edinburgh postnatal depression scale assessment during pregnancy for the risk of developing postpartum depressive symptoms: a prospective cohort study. BJOG. 121, 1604–1610 (2014).
Parsons, C. E. et al. Postnatal depression and its effects on child development: a review of evidence from low- and middle-income countries. Br Med Bull. 101, 57–79 (2012).
Howard, L. M., Goss, C., Leese, M. & Thornicroft, G. Medical outcome of pregnancy in women with psychotic disorders and their infants in the first year after birth. Br J Psychiatry. 182, 63–67 (2003).
Jablensky, A. V. et al. Pregnancy, delivery, and neonatal complications in a population cohort of women with schizophrenia and major affective disorders. Am J Psychiatry. 162, 79–91 (2005).
Webb, R., Abel, K., Pickles, A. & Appleby, L. Mortality in offspring of parents with psychotic disorders: a critical review and meta-analysis. Am J Psychiatry. 162, 1045–1056 (2005).
Bennedsen, B. E., Mortensen, P. B., Olesen, A. V. & Henriksen, T. B. Congenital malformations, stillbirths, and infant deaths among children of women with schizophrenia. Arch Gen Psychiatry. 58, 674–679 (2001).
Grigoriadis, S. et al. The impact of maternal depression during pregnancy on perinatal outcomes: a systematic review and meta-analysis. J Clin Psychiatry. 74, e321–e341, 10.4088/JCP.12r07968 (2013).
Grote, N. K. et al. A meta-analysis of depression during pregnancy and the risk of preterm birth, low birth weight, and intrauterine growth restriction. Arch Gen Psychiatry. 67, 1012–1024 (2010).
Grigoriadis, S. et al. Prenatal exposure to antidepressants and persistent pulmonary hypertension of the newborn: systematic review and meta-analysis. BMJ. 348, f6932, 10.1136bmj.f6932 (2014).
Stein, A. et al. Effects of perinatal mental disorders on the fetus and child. Lancet. 384, 1800–1819 (2014).
Hobel, C. J. et al. Maternal plasma corticotropin-releasing hormone associated with stress at 20 weeks’ gestation in pregnancies ending in preterm delivery. Am J Obstet Gynecol. 180, S257–S263 (1999).
Dayan, J. et al. Role of anxiety and depression in the onset of spontaneous preterm labor. Am J Epidemiol. 155, 293–301 (2002).
Smith, R. et al. Mood changes, obstetric experience and alterations in plasma cortisol, beta-endorphin and corticotrophin releasing hormone during pregnancy and the puerperium. J Psychosom Res. 34, 53–69 (1990).
Geronimus, A. T. The weathering hypothesis and the health of African-American women and infants: evidence and speculations. Ethnicity & disease. 2, 207–221 (1992).
Geronimus, A. T. Understanding and eliminating racial inequalities in women’s health in the United States: the role of the weathering conceptual framework. Journal of the American Medical Women’s Association. 56, 133–136 (2001).
Acknowledgements
The authors acknowledge the support of the Mater Foundation for this research project.
Author information
Authors and Affiliations
Contributions
P.N. – Data collection and analysis, manuscript author. X.Y.F. – Data analysis and manuscript author. S.K. – Concept, data collection, data analysis and manuscript author.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Navaratne, P., Foo, X. & Kumar, S. Impact of a high Edinburgh Postnatal Depression Scale score on obstetric and perinatal outcomes. Sci Rep 6, 33544 (2016). https://doi.org/10.1038/srep33544
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep33544
This article is cited by
-
Racial Differences in the Risk of Prenatal Depression Among Women Experiencing Childhood and Adult Stressors
Maternal and Child Health Journal (2022)
-
The impact of maternal prenatal mental health disorders on stillbirth and infant mortality: a systematic review and meta-analysis
Archives of Women's Mental Health (2021)
-
Antepartum Depression and Preterm Birth: Pathophysiology, Epidemiology, and Disparities due to structural racism
Current Psychiatry Reports (2021)
-
The association between symptoms of depression during pregnancy and low birth weight: a prospective study
BMC Pregnancy and Childbirth (2020)
-
Impact of maternal depression on perinatal outcomes in hospitalized women—a prospective study
Archives of Women's Mental Health (2019)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
