
Abstract
Anaphylatoxin C5a, a potent pro-inflammatory peptide produced in the process of complement activation, was proved to have a vital role in tumor initiation and progession by previous investigations. However whether it could act as a prognostic marker remains unknown. Here we retrospectively enrolled 272 ccRCC patients undergoing nephrectomy in Zhongshan Hospital, Shanghai between 2005 and 2007. C5a level was assessed by immunohistochemistry and its association with clinicopathologic features and prognosis were evaluated. Our results indicated that high tumoral C5a level was associated with poor overall survival (OS) (hazard ratio = 1.753, 95% CI 1.068–2.878, P = 0.026). In addition, tumoral C5a could significantly stratify patients’ prognosis both in advanced stage (TNM III + IV) and intermediate/high risk group (SSIGN score ≥4) (P < 0.001 and = 0.008, respectively). Furthermore, incorporating tumoral C5a with other parameters could improve the predicting accuracy, compared with TNM and SSIGN system (c-index = 0.789, 0.713 and 0.727, respectively). In conclusion, tumoral C5a is an independent adverse prognostic biomarker for clinical outcome of ccRCC patients after nephectomy.
Similar content being viewed by others


Introduction
Renal cell carcinoma (RCC), arising from renal tubular epithelial cells, accounts for approximate 2–3% of all malignancies in adults1. In China, over 54 out of 100,000 people are diagnosed with RCC every year2 and most of the cases (70–85%) are clear cell RCC (ccRCC), histologically3. Although incidental RCC has taken up more than 50% of all RCCs due to the widespread use of abdominal imaging4,5, 25–30% of the patients still have the initial diagnosis with metastasis6. Moreover, another 20% of the patients will have a relapse and develop metastatic RCC (mRCC) after curative nephrectomy7. Characterized by the resistance to radiotherapy and chemotherapy, mRCC exhibits an extremely poor prognosis8,9, which makes the predicting system more important.
Currently, some clinical or pathological predicting systems are used to predict outcomes of RCC patients. TNM stage and Fuhrman grade are traditional, but the most common used systems. Meanwhile, integrated systems, including Mayo Clinic stage, size, grade and necrosis (SSIGN) score and University of California integrated Staging System (UISS), are also clinically employed10,11. With these predicting systems, however, accurate prediction remains difficult, thus better or novel predictors of survival of RCC are needed10,12.
Inflammatory microenvironment plays a vital role during tumor initiation and progression13. Renal cell carcinoma also exhibits a strong connection with hypoxia and enhanced inflammatory signaling14. Anaphylatoxin C5a, including C5a itself and its spliced form C5adesArg- being removed of the C-terminal arginine, is another potent pro-inflammatory peptide produced in the process of complement activation15. Growing evidence has suggested that C5a may serve as a negative wrecker in tumor initiation and progression by modulating microenvironment16,17. Additionally, it is reported that high level of C5a receptor (C5aR) is associated with poor clinical outcome in lung cancer18, while no investigations have focused on the prognostic function of C5a. Therefore, we are curious about the association between C5a and ccRCC patients’ prognosis and speculate that C5a could probably function as a prognostic marker.
In this study, we sought to identify the clinical and prognostic value of C5a in ccRCC by immunohistochemical staining. We analysed the association of tumoral C5a level with clinicopathological characteristics and clinical outcomes (OS and RFS). Moreover, C-index was applied to explore the effect of tumoral C5a on prediction accuracy by incorporating it with traditional systems.
Results
Patient characteristics and immunohistochemical findings
The major characteristics of this cohort were shown in Table 1. The median follow-up was 99.0 months (2.6–120.5months) and the median age was 55 years old (15–83 years). Generally, most of the patients were male (69.1%) and tumors were predominantly of well differentiation (Fuhrman grade 1 + 2, 84.2%) and early stage (TNM I + II, 69.9%) and good physical status(ECOG-PS score = 0) prevailed (73.2%). 16 out of 272 (5.9%) patients were identified with lymph node or distant metastasis.
To assess the intensity of C5a in ccRCC patients, anti-C5a IHC staining was performed on tumoral and peritumoral tissues. According to the staining intensity and corresponding IOD score, we divided the tumoral C5a level into high and low groups by X tile (Fig. 1A–D). C5a staining predominantly located on the membrane of tumor cells and extracellular matrix in tumor tissues. In peritumoral tissues, C5a was diffusely distributed in the entire tubular epithelial cells with glomerulus merely being stained (Fig. 1E,F). Albeit the higher IOD score and wider range (mean ± SD: 19530 ± 9741 in peritumor vs 15699 ± 9255in tumor, respectively, P < 0.001, Fig. 1G), we ruled out the necessity of further analyzing peritumoral C5a in its prognostic properties, as the minimum P value was 0.75 by X tile.

Immunohistochemical analyses of C5a in ccRCC specimens.
Representative high C5a level in tumor tissues with (A) ×200 magnification and (B) ×400 magnification; representative low C5a level in tumor tissues with (C) ×200 magnification and (D) ×400 magnification; representative C5a staining in peritumor tissues with (E) ×200 magnification and (F) ×400 magnification; (G) IOD score of C5a level in tumor and non tumor tissue. The three horizontal lines represent mean C5a and ±standard error of mean (SEM). P-value, calculated by Mann Whitney test, <0.05 was regarded as statistically significant.
Associations between C5a and clinicopathological parameters
We further evaluated the associations between clinicopathological features and tumoral C5a level. As shown in Table 1, C5a was only significantly correlated with necrosis in tumors of this cohort (P = 0.026). There was no significant relationship with any other clinicopathological characteristics.
Prognostic significance of C5a
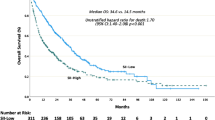
In order to assess whether tumoral C5a has potential significance in predicting clinical outcome of ccRCC patients, Kaplan-Meier analyses were applied to compare OS and DFS in different C5a leveled patients. Compared with those in low level, patients with high level of C5a exhibited a significant poorer OS (P = 0.011; Fig. 2A). However, the two groups divided by C5a were of no statistical difference in DFS-probably due to the limited specimens, since the separating trend could be observed (P = 0.079; Fig. 2B). Therefore, DFS was excluded in the next stratifying analyses.

Kaplan-Meier analyses for OS and DFS of ccRCC patients according to tumoral C5a level.
(A) OS according to tumoral C5a level and; (B) DFS according to tumoral C5a level.
To ascertain what exquisite subgroups the potential prognostic value lied in, we chose TNM stage and SSIGN system to stratify the patients, because TNM stage is the most common used parameter and SSIGN a classical comprehensive system. As the results showed in Fig. 3A,B, high level of C5a strongly correlated with shorter OS in advanced stage (TNM III + IV) subgroups (P < 0.001, Fig. 3B). While discrepancy was not observed in early stage patients (P = 0.845, Fig. 3A). Patients were used to be stratified into low/intermediate/high risk groups as the clinical outcomes were completely different11. However, considering the limited high risk patients (SSIGN score he l6/272, 2.2%) in this cohort, we combined intermediate (SSIGN score 4–7) and high risk patients into one intermediate/high risk group (SSIGN score ≥4). As shown in Fig. 3C,D, patients with high C5a level was also an adverse prognostic factor for OS in intermediate/high risk subgroup (P = 0.008; Fig. 3D), while curves in low risk (SSIGN score 0–3) subgroup were of no difference (P = 0.628; Fig. 3C).

Kaplan-Meier analyses for OS in ccRCC according to tumoral C5a level stratified by TNM stage and SSIGN score.
Kaplan-Meier analyses for OS of ccRCC patients according to C5a level in (A) early-stage (TNM I + II), (B) advanced-stage (TNM III + IV), (C) low risk (SSIGN score 0–3), (D) intermediate/high risk (SSIGN score van stratified groups.
Further, univariate and multivariate analyses were conducted to identify the independence of C5a. Parameters with statistical significance in univariate analyses were brought into the multivariate analyses. But we excluded single T, N and M classification in the multivariate analyses in case of overlap with TNM stage variable. As shown in Table 2, univariate analysis reconfirmed the strong significance between C5a and OS (HR 1.818, 95% CI 1.142–2.894, P = 0.012) and multivariate analysis verified the independence of C5a in predicting ccRCC patients’ OS (HR 1.753, 95% CI 1.068–2.878, P = 0.026), just like TNM stage (P < 0.001), Fuhrman grade (P = 0.002), Necrosis (P = 0.023) and ECOG-PS (P < 0.001).
Collectively, these data demonstrated that C5a level was an independent prognostic factor in ccRCC patients for predicting OS and it performed better in advanced stage and intermediate/high risk patients.
Construction of a novel integrated system and accuracy evaluation
We then sought to integrate the independent characteristics in the multivariate analysis into one system. To achieve this goal, we set up a nomogram for OS and C5a was obviously a negative factor in the nomogram (Fig. 4A). Boottrap validation was performed for calibration of 5- and 8-year survival (Fig. 4B,C). To precisely evaluate the accuracy, we compared the c-index of the novel system with that of TNM stage and SSIGN system. The c-index of our integrated system, TNM stage and SSIGN system was 0.789, 0.713 and 0.727, respectively. These data suggested that the novel integrated system was more accurate than traditional TNM grade and SSIGN system in predicting OS of ccRCC patients.

Nomogram for predicting 5- and 8-year OS in ccRCC patients.
(A) Nomogram for predicting clinical outcomes integrating tumoral C5a level, TNM stage, Fuhrman grade and necrosis; (B) calibration plot for predicted and observed 5-year overall survival rate; and (C) calibration plot for predicted and observed 8-year overall survival rate. The gray line: ideal model, vertical bars: 95% CI and ECOG-PS = Eastern Cooperative Oncology Group performance status.
Discussion
Early staged RCC is a curable disease as the 5-year overall survival rate of patients in early stage (TNM I + II) is about 91% after surgery7,19. However, circumstance changes when it comes to advanced stage (TNM III + IV) patients, as the figure precipitates to 59% in stage III and 20% in stage IV7. Therefore, sharpening the prognostic systems in predicting the clinical outcome, especially outcome of advanced stage patients, seems much more worthwhile. In this study, we for the first time, proposed a new independent biomarker C5a, which was significantly associated with overall survival of ccRCC patients, especially in TNM advanced stage and SSIGN intermediate/high risk patients. Integrating it with other parameters exhibited a more accurate prediction.
Inflammation plays a crucial role in cancer and could provide potential therapeutic targets. During initiation and progression of tumors, produced inflammatory factors (cytokines, chemokines, etc) could provoke the activating, infiltrating and trafficking of various inflammatory immune cells into tumor tissue14,20 to form a tumor-promoting environment. In kidney cancer, several associated inflammatory signaling pathways (VHL, mTOR, TNF, STAT) was proved to be dramatically associated with carcinogenesis14 and targeting vital molecules in these pathways attenuates tumor growth and progression, based on which new drugs are developed14,21,22,23. C5a, a 74-amino-acid glycopeptide produced by the enzymatic cleavage of C5, is a potent inflammatory mediator and chemoattractant that has been reported to be able to regulate anti-tumor response16,17,24. The fact that tumor cells themselves could not only enhance the production of C5a, but also express protecting protein to avoid complement induced lysis suggests a membrane attacking complex (MAC)-independent way16,25. That hypothesis is directly or indirectly supported by many investigations16,17,26,27. This indirect antitumor effect could be abrogated by C5aR knock down or treatment of C5aR antagonist, indicating an important role of C5a/C5aR in tumor microenvironment16,17. Therefore C5a/C5aR axis is a potential therapeutic target in cancer28.
Limitations still exist in our study. First of all, it is a single retrospective cohort with limited patients. We are excited and confident in our principal findings- high C5a level predicts poor prognosis- as it is consistent with the argument of several previous rigorous basic scientific investigations16,17,29. It was the significant correlations between C5a and OS that we conclude from. However, C5a was not associated with DFS statistically in our study and we are inclined to attribute this insignificance to the limited patients of our cohort since a separating tendency could be observed and statistical significance should appeared if we only performed Kaplan-Meier analyses in advanced stage patients (Figure not shown). Therefore we speculate that C5a could be more efficient in pure high risk patients such as advanced stage, even metastatic RCC (mRCC) patients. Actually we have been working on mRCC patients’ follow-up and our next clinical investigation are to focus on the role of tumoral C5a in mRCC patients. Secondly, our study was based on the IHC staining and score, which would be more persuasive by adjuvant measurement of relative mRNA expression, such as complement regulatory gene expression. However, although we are collecting fresh tissue samples for mRNA evaluation, not enough is prepared for the time being. Last but not least, complement is a complicated system involving dozens of proteins, one complement C5a does not represent the entire family. More investigations, especially mechanism researches, are to help with deeper understanding and potential clinical utilization of complement system.
All in all, our study demonstrate that C5a was an adverse prognostic factor in ccRCC patients and further more investigations are supposed to carry on.
Conclusions
Tumoral C5a is a novel prognostic marker in ccRCC patients. High tumoral C5a level is associated with OS and it is better performed in TNM advanced stage and SSIGN intermediate/high risk patients. Integrating tumoral C5a with other clinical parameters could increase the predicting accuracy, which provides an alternative postoperational surveillance system.
Materials and Methods
Patients
A total of 272 patients with pathologically validated ccRCC after partial or radical nephrectomy, between Feb 2005 and Jun 2007, were enrolled from the Department of Urology, Zhongshan Hospital, Fudan University. All methods mentioned in this article were approved by the ethics committee of Zhongshan Hospital (approval number B2015-030) and were carried out in accordance with the approved guidelines and regulations (REMARK criteria). Written informed consent on the use of clinical specimens from each patient was achieved. The inclusion criteria were: no history of other malignant tumors, no history of anticancer therapy, pathologically proven ccRCC and patients after radical or partial nephrectomy. The exclusion criteria were: mixed histological type of primary renal cancer, tumor necrosis area over 80% and patients died within the first month after surgery. Patients were followed up every 3 months and finally ended on January 30, 2015. Patients’ basic information (age, gender, ECOG-PS), tumor pathological information (tumor size, Fuhrman grade, necrosis, TNM stage) and survival or recurrence information (date of death or recurrence, or last follow-up) were recorded. Tumor size was faithfully recorded as the longest diameter described in pathology report. Necrosis, histological type and Fuhrman grade were reassessed by two independent pathologists. Presence of nodal and metastasis was defined according to intraoperative, pathologic and radiographic findings. With radiographic reports and postoperative data, we reassigned the stage according to the 2010 AJCC TNM classification30 and final TNM stage was confirmed by one urologist. OS was defined as the time span from curative surgery to death of any cause. DFS was defined as the time span from curative surgery to recurrence or metastasis. None of the patients in this cohort has ever received targeted therapies before or after surgery.
Immunohistochemistry and evaluation
Tissue microarrays (TMA) were established as previously described31. Primary monoclonal anti-C5a antibody (1:100 dilution, ab11878, Abcam, Cambridge, MA, USA) were applied in the procedure. Three independent shots of C5a staining areas (away from tissue margin, obvious inflammatory and necrotic domains) were taken for analysis. The intensity was analyzed by Image-Pro Plus 6.0 and integrated optical intensity (IOD), representing the staining intensity, was recorded. The TMA slides were observed and evaluated by two investigators unaware of the clinical information. To determine the optimum cutoff IOD score, we performed X tile plot analysis with X tile software 3.6.1 and select the cut point by the rule of “minimum P value”. The cutoff point was 12578 for tumoral C5a staining, but not a significant point was found in peritumoral C5a staining.
Statistical analyses
GraphPad Prism 6, SPSS 19.0 and Stata 12.0 were used to do the statistical analyses of this study. P-value < 0.05 was regarded as statistically significant. Mann-Whitney test was applied to compare the tumoral and peritumoral IOD score. Fisher’s exact method, χ2 test, or Cochran-Mantel-Haenszel χ2 test were applied to analyze the associations between staining level and patients’ clinical features. Kaplan-Meier analyses and log-rank tests were applied for OS and DFS evaluation. Univariate and multivariate Cox proportional hazard models were applied to evaluate the HR and 95% CI. Further nomogram construction and calibration were performed with R software 3.0.2 with the “rms” package. Finally, we compared the Harrell’s concordance index (c-index) of different predicting systems to evaluate the prognostic accuracy.
Additional Information
How to cite this article: Xi, W. et al. High Level of Anaphylatoxin C5a Predicts Poor Clinical Outcome in Patients with Clear Cell Renal Cell Carcinoma. Sci. Rep. 6, 29177; doi: 10.1038/srep29177 (2016).
References
Siegel, R., Ma, J., Zou, Z. & Jemal, A. Cancer statistics, 2014. CA: a cancer journal for clinicians 64, 9–29, doi: 10.3322/caac.21208 (2014).
Yang, L., Parkin, D. M., Ferlay, J., Li, L. & Chen, Y. Estimates of cancer incidence in China for 2000 and projections for 2005. Cancer epidemiology, biomarkers & prevention: a publication of the American Association for Cancer Research, cosponsored by the American Society of Preventive Oncology 14, 243–250 (2005).
Escudier, B. et al. Renal cell carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Annals of oncology: official journal of the European Society for Medical Oncology/ESMO 23, Suppl 7, vii65–71, doi: 10.1093/annonc/mds227 (2012).
Jayson, M. & Sanders, H. Increased incidence of serendipitously discovered renal cell carcinoma. Urology 51, 203–205 (1998).
Tsui, K. H. et al. Renal cell carcinoma: prognostic significance of incidentally detected tumors. The Journal of urology 163, 426–430 (2000).
Gupta, K., Miller, J. D., Li, J. Z., Russell, M. W. & Charbonneau, C. Epidemiologic and socioeconomic burden of metastatic renal cell carcinoma (mRCC): a literature review. Cancer treatment reviews 34, 193–205, doi: 10.1016/j.ctrv.2007.12.001 (2008).
Athar, U. & Gentile, T. C. Treatment options for metastatic renal cell carcinoma: a review. The Canadian journal of urology 15, 3954–3966 (2008).
Linehan, W. M., Walther, M. M. & Zbar, B. The genetic basis of cancer of the kidney. The Journal of urology 170, 2163–2172, doi: 10.1097/01.ju.0000096060.92397.ed (2003).
Linehan, W. M. & Zbar, B. Focus on kidney cancer. Cancer cell 6, 223–228, doi: 10.1016/j.ccr.2004.09.006 (2004).
Sun, M. et al. Prognostic factors and predictive models in renal cell carcinoma: a contemporary review. European urology 60, 644–661, doi: 10.1016/j.eururo.2011.06.041 (2011).
Frank, I. et al. An outcome prediction model for patients with clear cell renal cell carcinoma treated with radical nephrectomy based on tumor stage, size, grade and necrosis: the SSIGN score. The Journal of urology 168, 2395–2400, doi: 10.1097/01.ju.0000035885.91935.d5 (2002).
Eichelberg, C., Junker, K., Ljungberg, B. & Moch, H. Diagnostic and prognostic molecular markers for renal cell carcinoma: a critical appraisal of the current state of research and clinical applicability. European urology 55, 851–863, doi: 10.1016/j.eururo.2009.01.003 (2009).
Shalapour, S. & Karin, M. Immunity, inflammation and cancer: an eternal fight between good and evil. The Journal of clinical investigation 125, 3347–3355, doi: 10.1172/jci80007 (2015).
de Vivar Chevez, A. R., Finke, J. & Bukowski, R. The role of inflammation in kidney cancer. Advances in experimental medicine and biology 816, 197–234, doi: 10.1007/978-3-0348-0837-8_9 (2014).
Manthey, H. D., Woodruff, T. M., Taylor, S. M. & Monk, P. N. Complement component 5a (C5a). The international journal of biochemistry & cell biology 41, 2114–2117, doi: 10.1016/j.biocel.2009.04.005 (2009).
Corrales, L. et al. Anaphylatoxin C5a creates a favorable microenvironment for lung cancer progression. Journal of immunology (Baltimore, Md.: 1950) 189, 4674–4683, doi: 10.4049/jimmunol.1201654 (2012).
Markiewski, M. M. et al. Modulation of the antitumor immune response by complement. Nature immunology 9, 1225–1235, doi: 10.1038/ni.1655 (2008).
Gu, J. et al. Overexpression of CD88 predicts poor prognosis in non-small-cell lung cancer. Lung cancer (Amsterdam, Netherlands) 81, 259–265, doi: 10.1016/j.lungcan.2013.04.020 (2013).
Cohen, H. T. & McGovern, F. J. Renal-cell carcinoma. The New England journal of medicine 353, 2477–2490, doi: 10.1056/NEJMra043172 (2005).
Gabrilovich, D. I., Ostrand-Rosenberg, S. & Bronte, V. Coordinated regulation of myeloid cells by tumours. Nature reviews. Immunology 12, 253–268, doi: 10.1038/nri3175 (2012).
Brotelle, T. & Bay, J. O. [PI3K-AKT-mTOR pathway: Description, therapeutic development, resistance, predictive/prognostic biomarkers and therapeutic applications for cancer]. Bulletin du cancer, doi: 10.1016/j.bulcan.2015.09.011 (2015).
Saran, U., Foti, M. & Dufour, J. F. Cellular and molecular effects of the mTOR inhibitor everolimus. Clinical science (London, England: 1979) 129, 895–914, doi: 10.1042/cs20150149 (2015).
Escudier, B. et al. Sorafenib for treatment of renal cell carcinoma: Final efficacy and safety results of the phase III treatment approaches in renal cancer global evaluation trial. Journal of clinical oncology: official journal of the American Society of Clinical Oncology 27, 3312–3318, doi: 10.1200/jco.2008.19.5511 (2009).
Lu, Y. & Hu, X. B. C5a stimulates the proliferation of breast cancer cells via Akt-dependent RGC-32 gene activation. Oncology reports 32, 2817–2823, doi: 10.3892/or.2014.3489 (2014).
Gorter, A. & Meri, S. Immune evasion of tumor cells using membrane-bound complement regulatory proteins. Immunology today 20, 576–582 (1999).
Guo, R. F. & Ward, P. A. Role of C5a in inflammatory responses. Annual review of immunology 23, 821–852, doi: 10.1146/annurev.immunol.23.021704.115835 (2005).
Markiewski, M. M. & Lambris, J. D. The role of complement in inflammatory diseases from behind the scenes into the spotlight. Am J Pathol 171, 715–727, doi: 10.2353/ajpath.2007.070166 (2007).
Woodruff, T. M., Nandakumar, K. S. & Tedesco, F. Inhibiting the C5-C5a receptor axis. Molecular immunology 48, 1631–1642, doi: 10.1016/j.molimm.2011.04.014 (2011).
Nitta, H. et al. Enhancement of human cancer cell motility and invasiveness by anaphylatoxin C5a via aberrantly expressed C5a receptor (CD88). Clinical cancer research: an official journal of the American Association for Cancer Research 19, 2004–2013, doi: 10.1158/1078-0432.ccr-12-1204 (2013).
Edge, S. B. & Compton, C. C. The American Joint Committee on Cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Annals of surgical oncology 17, 1471–1474, doi: 10.1245/s10434-010-0985-4 (2010).
Zhu, X. D. et al. High expression of macrophage colony-stimulating factor in peritumoral liver tissue is associated with poor survival after curative resection of hepatocellular carcinoma. Journal of clinical oncology: official journal of the American Society of Clinical Oncology 26, 2707–2716, doi: 10.1200/jco.2007.15.6521 (2008).
Acknowledgements
The authors would like to thank Dr. Yuan Ji, Dr. Jun Hou and Ms. Haiying Zeng (Department of Pathology, Zhongshan Hospital of Fudan University) for diagnosis confirmation and technical assistance, respectively. This study was funded by grants from National Basic Research Program of China (2012CB822104), National Key Projects for Infectious Diseases of China (2012ZX10002012-007, 2016ZX10002018-008), National Natural Science Foundation of China (31100629, 31270863, 81372755, 31470794, 81401988, 81402082, 81402085, 81471621, 81472227, 81472376, 31570803, 81501999 and 81572352) and Program for New Century Excellent Talents in University (NCET-13-0146). All these study sponsors have no roles in the study design, in the collection, analysis and interpretation of data.
Author information
Authors and Affiliations
Contributions
W.X. for acquisition of data, analysis and interpretation of data, statistical analysis and drafting of the manuscript; L.L., J.W., Y.X., Q.B., Q.L. and Y.W. for technical and material support; J.X. and J.G. for study concept and design, analysis and interpretation of data, drafting of the manuscript, obtained funding and study supervision. All authors read and approved the final manuscript.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Xi, W., Liu, L., Wang, J. et al. High Level of Anaphylatoxin C5a Predicts Poor Clinical Outcome in Patients with Clear Cell Renal Cell Carcinoma. Sci Rep 6, 29177 (2016). https://doi.org/10.1038/srep29177
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep29177
This article is cited by
-
A novel prognostic N7-methylguanosine-related long non-coding RNA signature in clear cell renal cell carcinoma
Scientific Reports (2023)
-
Context-dependent roles of complement in cancer
Nature Reviews Cancer (2019)
-
Complement in cancer: untangling an intricate relationship
Nature Reviews Immunology (2018)
-
Mesenchymal stem cells alleviate acute kidney injury by down-regulating C5a/C5aR pathway activation
International Urology and Nephrology (2018)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
