
Abstract
Research on the association between ambient temperature and cerebrovascular morbidity is scarce in China. In this study, we applied mixed generalized additive model (MGAM) to daily counts of cerebrovascular disease of Shanghai residents aged 65 years or older from 2007–2011, stratified by gender. Weighted daily mean temperature up to lags of one week was smoothed by natural cubic spline and was added into the model to assess both linear and nonlinear effects of temperature. We found that when the mean temperature increased by 1 °C, the male cases of cerebrovascular disease reduced by 0.95% (95% Confidence Interval (CI): 0.80%, 1.10%) or reduced by 0.34% (95% CI: −0.68, 1.36%) in conditions of temperature was below or above 27 °C. However, for every 1 °C increase in temperature, the female cases of cerebrovascular disease increased by 0.34% (95% CI: −0.26%, 0.94%) or decreased by 0.92% (95% CI: 0.72, 1.11%) in conditions of temperature was below or above 8 °C, respectively. Temperature and cerebrovascular morbidity is negatively associated in Shanghai. MGAM is recommended in assessing the association between environmental hazards and health outcomes in time series studies.
Similar content being viewed by others


Introduction
Cerebrovascular disease is a leading cause of disability in adults1. Every year, millions of stroke survivors have to adapt to a life with restrictions in activities of daily living as a consequence of cerebrovascular disease. Older age has long been recognized as a risk factor for developing cerebrovascular disease and the risk goes up significantly for those aged 65 years or older. Men and women tend to have different risks in developing cerebrovascular disease as they differ in socio-economic status, comorbidities and sex steroids2,3,4,5. The prevention of cerebrovascular disease is of pivotal importance in maintaining good quality of life in both older men and women.
The incidence of cerebrovascular disease shows a seasonal pattern and is likely to associate with ambient temperature6,7. Understanding of the association between transient exposure of temperature and occurrences of cerebrovascular disease might lead to timely implementation of preventive measures and appropriate allocation of medical resources. Although several prior studies have been conducted to evaluate the association of temperature and cerebrovascular morbidity, yet these studies have given conflicting results. For example, Goggins et al. found a negative linear association between daily mean temperature and hospital admissions for cerebrovascular diseases in Hong Kong8. Low et al. suggested a positive association of mean temperature and stroke risk in US9. Field et al. found no relationship between weather and stroke occurrences in Calgary10.
One possible reason for the conflicting results may be that various statistical methods were used to investigate the association of temperature and incidence of cerebrovascular disease. Some studies have investigated the association using generalized linear model (GLM, e.g. Poisson regression)11. However, GLM is a set of classic probability-based models assuming independence of observations, therefore GLM might not be appropriate to fit auto-correlated time series data such as incidences of cerebrovascular disease. Generalized additive model (GAM) is another set of probability-based models and has been commonly adopted in assessing the association between environmental factors and health outcomes of both communicable and non-communicable diseases12,13. The advantage of GAM over GLM lies in its ability to adjust for both linear and non-linear association of measured and unmeasured confounding factors with health outcomes. However, the selection of appropriate degrees of freedom to adjust for confounders remains controversial. Over-adjustment of confounders may lead to underestimation of true effect, as some variations caused by exposure of interest were absorbed by confounders. Likewise, under-adjustment of confounders could cause spurious association between exposure of interest and health outcome12. Therefore, GLM and GAM were relatively simple statistical methods and may fail to take into account the complicating factors including non-linearity, seasonality, autocorrelation and confounding. Recent development of biostatistics suggests that mixed generalized additive model (MGAM) might be a better choice to assess the association between environmental factors and health outcomes, because MGAM includes an autoregressive term as random effect to adjust for autocorrelation of observations and has a robust approach to select appropriate degrees of freedom to adjust for confounders14,15,16.
The primary objective of this study is to assess the association between ambient temperature and cerebrovascular morbidity in the Shanghai residents aged 65 years or older for both men and women. The secondary objective is to compare the performance of GAM and MGAM in assessing the association between temperature and incidence of cerebrovascular disease.
Methods
Data
Shanghai is a subtropical city, located in eastern China. It has a total area of 6,341 km2 with a total resident population of 14.2 million by the end of 201115. Daily numbers of emergency patients and hospitalized patients diagnosed of cerebrovascular disease in men and women aged 65 years or older from 2007 to 2011 were retrieved from the Official Medicare Database in Shanghai. The official Medicare Database contained medical records in all public hospitals who had Shanghai medical insurance. Two groups of people could have Shanghai medical insurance: residents who have Shanghai household registration or employees who have job contracts longer than six months. The diagnoses of cerebrovascular disease were coded in the International Classification of Diseases, Tenth Revision (ICD10 I60–I69).
Averages of daily mean temperatures measured at all monitoring sites in Shanghai were obtained from the Shanghai Meteorological Bureau. Daily concentrations of particular matters up to 10 micrometers in size (PM10), Sulfur dioxide (SO2) and nitrogen dioxide (NO2) were obtained from the Shanghai Environmental Monitoring Center. Previous studies have indicated that particular matters up to 2.5 micrometers in size (PM2.5) was an confounder in assessing the association between temperature and cerebrovascular morbidity17. But unfortunately, Shanghai did not start PM2.5 surveillance until 2012 that we were unable to adjust for it in the current study. The population sizes from 2007 to 2011 for men and women aged 65 years or older of Shanghai residents were obtained from the Shanghai Research Center on Aging18.
Statistical Analysis
In this study, we used MGAM19 to assess the association between ambient temperature and cerebrovascular morbidity in the elderly, stratified by gender. The mathematical representation of MGAM was as follows:

a
Yt denotes the daily cases of cerebrovascular diseases in the elderly men or women, which was assumed to follow Poisson distribution with mean equaling to . tempt was the weighted average of daily mean temperature considering the lag effect of temperature in one week, represented as
. tempt was the weighted average of daily mean temperature considering the lag effect of temperature in one week, represented as  and
and  . Weighted mean temperature was included into the model using natural cubic spline to account for both linear and non-linear association between temperature and cerebrovascular morbidity. We adjusted for the unmeasured confounding of long term and seasonal trends using natural cubic spline (ns(t)) and measured confounding of PM10 using natural cubic spline (ns(pmt)) and day of the week as a dummy variable (DOWt) in the model. Daily concentrations of SO2 and NO2 were not included into the final model because they were almost all statistically insignificant (Table S1). df1, df2 and df3 denote the degrees of freedom (df) for temperature, trends and PM10, respectively. df1 and df3 was chosen to minimize the Akaike information criterion. df2 was chosen to ensure the seasonal pattern of temperature across years, with detailed methodology described in our previous papers14,15.
. Weighted mean temperature was included into the model using natural cubic spline to account for both linear and non-linear association between temperature and cerebrovascular morbidity. We adjusted for the unmeasured confounding of long term and seasonal trends using natural cubic spline (ns(t)) and measured confounding of PM10 using natural cubic spline (ns(pmt)) and day of the week as a dummy variable (DOWt) in the model. Daily concentrations of SO2 and NO2 were not included into the final model because they were almost all statistically insignificant (Table S1). df1, df2 and df3 denote the degrees of freedom (df) for temperature, trends and PM10, respectively. df1 and df3 was chosen to minimize the Akaike information criterion. df2 was chosen to ensure the seasonal pattern of temperature across years, with detailed methodology described in our previous papers14,15.  was considered as the random effect to account for the dependence nature of time series data. The coefficients and weights for temperature were estimated by maximum partial likelihood using Newton’s Method.
was considered as the random effect to account for the dependence nature of time series data. The coefficients and weights for temperature were estimated by maximum partial likelihood using Newton’s Method.
Comparison of MGAM and GAM
Although MGAM was believed to outperform the traditional GAM20, we repeated the analysis using GAM and compared their performances. The mathematical representation of GAM model was as follows:

The major difference of MGAM and GAM was that GAM did not have random effect  to adjust for the autocorrelation. The performance of GAM and MGAM was assessed by plots of residual autocorrelation function (ACF) and partial autocorrelation function (PACF) considering the lags up to 30 days (around one month). The selected model with better ACF and PACF was adopted to examine the estimated spline for temperature effect on cerebrovascular morbidity in the elderly men and women.
to adjust for the autocorrelation. The performance of GAM and MGAM was assessed by plots of residual autocorrelation function (ACF) and partial autocorrelation function (PACF) considering the lags up to 30 days (around one month). The selected model with better ACF and PACF was adopted to examine the estimated spline for temperature effect on cerebrovascular morbidity in the elderly men and women.
The study was approved by the Institute Review Board (IRB) of the School of Public Health, Fudan University. As aggregated data with no personal information were involved, this study was exempt from obtaining informed consent. All statistical analyses were conducted using R software (version 3.1.2).
Results
Descriptive statistics
In Shanghai, there were a total of 146,548 and 181,147 episodes of cerebrovascular diseases for men and women aged 65 years or older from 2007 to 2011. In the elderly men, the number of cerebrovascular diseases decreased from 30,700 to 28,100 from 2007 to 2011 and the corresponding rate decreased from 32.3 to 26.0 per 1,000 population (Table 1). In the elderly women, the number and rate of cerebrovascular disease were 37,000 and 31.9 per 1,000 population in 2007 and increased slightly in 2008, but decreased to 34,800 and 27.4 per 1,000 population in 2011 (Table 1). Women had higher rates of cerebrovascular disease than men, except in 2007 when the rate was 0.4 per 1,000 lower in women than in men (Table 1).
Shanghai had a mild subtropical climate with clear four seasons in a year. The four seasons were usually defined as spring from March–May, summer from June–August, autumn from September–November and winter from December to February. The average of daily mean temperature for the whole study period was around 17 °C and were 16 °C, 28 °C, 20 °C and 6 °C from spring to winter season. Temperature was negatively correlated with daily numbers of cerebrovascular disease (Spearman correlation=−0.4, P < 0.05), with more cases occurred in winter and spring seasons than in summer and autumn seasons.
Association between temperature and cerebrovascular morbidity
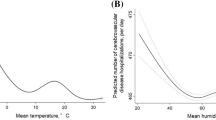
In general, MGAM well fitted the daily counts of cerebrovascular disease in both elderly men and women (Fig. 1). Temperature had an acute effect on cerebrovascular morbidity in women as the weights of temperature for one day lag was over 0.5 (Fig. 2). However, the weights of temperature were less various in males as all the weights were below 0.3 (Fig. 2). The risk of cerebrovascular disease was negatively associated with temperature (Fig. 3). In the elderly men, the risk of cerebrovascular disease decreased steadily as the temperature increased from the lowest to around 27 °C, but it became stable when the mean temperature exceeded from 27 °C (Fig. 3). By using the 27 °C as the cutoff point for two different linear effects of temperature, when the mean temperature increased 1 °C, the male cases of cerebrovascular disease reduced by 0.95% (95% Confidence Interval (CI): 0.80%, 1.10%) if the temperature was below 27 °C and reduced by 0.34% (95% CI: −0.68, 1.36%) if the temperature was above 27 °C. In the elderly women, the risk of cerebrovascular disease increased slightly as the temperature rose to around 8 °C and then decreased as the temperature continued increasing (Fig. 3). For every 1 °C increase in temperature, the female cases of cerebrovascular disease increased by 0.34% (95% CI: −0.26%, 0.94%) but decreased by 0.92% (95% CI: 0.72, 1.11%) in conditions of temperature was below or above 8 °C, respectively.

Observed and fitted daily counts of cerebrovascular diseases from MGAM in Shanghai residents aged 65 years or older, 2007–2011.
(A) Men; (B) Women.

Weights of daily temperature with lags up to one week for males (A) and females (B).

Estimated spline for temperature effect on cerebrovascular morbidity in Shanghai residents aged 65 years or older by gender, 2007–2011.
Performance of GAM and MGAM
Figures 4 and 5 show the residual ACF and PACF of GAM and MGAM in the elderly men and women, respectively. The residual ACF and PACF of GAM exceeded the boundary of 0.1 for many lags in both elderly men and women, implying the GAM was not appropriate without considering the internal dependence of time series data. In contrast, MGAM performed well as the residual ACF fell within ±0.1 for nonzero lags and the residual PACF fell within ±0.1 for all lags, partially demonstrating the validity of MGAM in this study.

Plots of residual autocorrelation function and partial autocorrelation function of generalized additive model and mixed generalized additive model in the elderly men.

Plots of residual autocorrelation function and partial autocorrelation function of generalized additive model and mixed generalized additive model in the elderly women.
Discussion
Our study reveals an inverse association between temperature and incidence of cerebrovascular disease. The finding is in line with the findings from Japanese studies, with cerebrovascular morbidity peak occurring in winter/spring months and trough occurring in summer months21,22. Similarly, studies from Australia, Sweden, Finland and Argentina also reported higher incidences of cerebrovascular disease in winter23,24,25,26. An early Framingham study in US did not indicate any seasonal pattern of incidence of total cerebrovascular diseases, but reported a winter peak for cerebral embolism cases27. The different proportions of subtypes of cerebrovascular disease might explain the inconsistency of winter peak of total cerebrovascular diseases in Shanghai and US. In 2000, another study compromised of veterans in US demonstrated the association between incidence of cerebrovascular disease and season, which showed the occurrence of ischemic stroke peaking in Mid-May and bottomed in December28. Likewise, the association between temperature and mortality of cerebrovascular disease varied across the world. An epidemiologic study in five cities (Beijing, Tianjin, Shanghai, Wuhan and Guangzhou) in China showed statistical significantly association of cold temperature with cerebrovascular mortality while hot effect was absent29. A study in California suggested a negative but not significant association between temperature and cerebrovascular mortality30. A study from Russian suggested a U-shape relationship between temperature and cerebrovascular mortality with the temperature threshold set at 18 °C31. A study from England also suggested an increased cerebrovascular mortality and elevated ambient temperature32. However, our study does not suggest the “heat-effect” of increased cerebrovascular disease morbidity and elevated ambient temperature. The “heat-effect” phenomenon might be explained by the population’s adaption to the environment. Both Russian and England are located at high latitude, so the residents might have already adapted to the cold environment, but very sensitive to the hot weather. Shanghai, on the other hand, is relatively warm, so the residents might not quite sensitive to hot climate, but susceptible to cold weather. Nevertheless, the diverse seasonal pattern of cerebrovascular morbidity and mortality in globe requires further investigation.
Our study found different temperature splines on cerebrovascular morbidity for men and women, particularly in cold climate. The cerebrovascular morbidity decreased in men while surprisingly increased in women when the temperature increased to around 8 °C. The gender difference might be explained by the different social behavior in elderly men and women. The elderly women might prefer staying indoors with air conditions during very cold days and later exposed to cold weather as the temperature increased a little bit. The elderly men, however, might be not used to the air condition and exposed to the environment regardless of the temperature.
The biological mechanisms for elevated risks of cerebrovascular disease in winter are complex. Low temperature is likely to induce vasoconstriction, resulting to increased blood pressure33. Cold exposure may also activate the sympathetic nervous system34, with enhanced platelet aggregation. Fibrinogen has been reported to be a risk factor for cerebrovascular disease35 and the fibrinogen plasma level was 23% higher in the colder months than in warmer months in the elderly as reported by Crawford36. Other biological factors could be increases levels of C-reactive protein in winter months37,38. All these factors could affect the blood supply to brain in winter and finally caused cerebrovascular disease. A recent study was conducted to investigate the pathophysiologic mechanisms underlying the association of temperature and cerebrovascular hemodynamics based on an elderly cohort, which revealed that temperature was negatively associated with cerebral blood flow velocity and cerebrovascular vasoreactivity and positively associated with cerebrovascular resistence39.
Although GAM has been widely accepted in assessing the association between environmental hazards and health outcomes, our study clearly illustrated that GAM could result to inaccurate association if autocorrelation was not appropriately adjust for. MGAM which takes the autocorrelation nature of time series data as random effect, is recommended in future environmental time series modeling.
Our study has several limitations. Firstly, this is an ecologic study which cannot rule out the ecologic fallacy. Individual factors such as socioeconomic status and chronic health conditions cannot be adjusted for in the ecologic study design. Secondly, PM2.5 was considered as a confounder in many studying assessing the association between the temperature and cerebrovascular morbidity. But unfortunately, PM2.5 cannot be adjusted for in the current study due to the data availability. Third, we could not rule out the disease misclassification for cerebrovascular disease although the rate of misclassification is usually low. Fourth, we did not separate the cerebrovascular disease by subtypes of ischemic stroke or hemorrhagic stroke. We cannot exclude the possibility that the association of cerebrovascular disease and temperature varied by subtypes.
In conclusion, our study suggests a higher cerebrovascular morbidity in cold weather and a lower cerebrovascular morbidity in warm weather. Women tended to have a higher cerebrovascular morbidity than men. For the public health significance, our findings will assist the policy-makers to give appropriate public health education or instructions to people at high risk to develop cerebrovascular disease at different seasons. From the methodology aspect, our study recommends to use MGAM in future environmental time series modeling.
Additional Information
How to cite this article: Zhang, X.-J. et al. Time series analysis of the association between ambient temperature and cerebrovascular morbidity in the elderly in Shanghai, China. Sci. Rep. 6, 19052; doi: 10.1038/srep19052 (2016).
References
Truelsen, T., Begg, S. & Mathers, C. The global burden of cerebrovascular disease, < http://www.who.int/healthinfo/statistics/bod_cerebrovasculardiseasestroke.pdf?ua=1> (2006) (Date of access: March 17, 2015).
Tang, Z. et al. Risk factors for cerebrovascular disease mortality among the elderly in Beijing: a competing risk analysis. PLoS One 9, e87884, doi: 10.1371/journal.pone.0087884 (2014).
Petrea, R. E. et al. Gender differences in stroke incidence and poststroke disability in the Framingham heart study. Stroke 40, 1032–1037 (2009).
Hollander, M. et al. Incidence, risk and case fatality of first ever stroke in the elderly population. The Rotterdam Study. J Neurol Neurosurg Psychiatry 74, 317–321 (2003).
Rothwell, P. M. et al. Population-based study of event-rate, incidence, case fatality and mortality for all acute vascular events in all arterial territories (Oxford Vascular Study). Lancet 366, 1773–1783 (2005).
Myint, P. K., Vowler, S. L., Woodhouse, P. R., Redmayne, O. & Fulcher, R. A. Winter excess in hospital admissions, in-patient mortality and length of acute hospital stay in stroke: a hospital database study over six seasonal years in Norfolk, UK. Neuroepidemiology 28, 79–85 (2007).
Hong, Y. C. et al. Ischemic stroke associated with decrease in temperature. Epidemiology 14, 473–478 (2003).
Goggins, W. B., Woo, J., Ho, S., Chan, E. Y. & Chau, P. H. Weather, season and daily stroke admissions in Hong Kong. Int J Biometeorol 56, 865–872 (2012).
Low, R. B. et al. The relation of stroke admissions to recent weather, airborne allergens, air pollution, seasons, upper respiratory infections and asthma incidence, September 11, 2001 and day of the week. Stroke 37, 951–957 (2006).
Field, T. S. & Hill, M. D. Weather, Chinook and stroke occurrence. Stroke 33, 1751–1757 (2002).
Gomes, J. et al. The effect of season and temperature variation on hospital admissions for incident stroke events in Maputo, Mozambique. J Stroke Cerebrovasc Dis 23, 271–277 (2014).
Wang, X. L. et al. Model selection in time series studies of influenza-associated mortality. PLoS One 7, e39423, doi: 10.1371/journal.pone.0039423 (2012).
Ren, C., Williams, G. M. & Tong, S. Does particulate matter modify the association between temperature and cardiorespiratory diseases? Environ Health Perspect 114, 1690–1696 (2006).
Ma, W. et al. Applied mixed generalized additive model to assess the effect of temperature on the incidence of bacillary dysentery and its forecast. PLoS One 8, e62122, doi: 10.1371/journal.pone.0062122 (2013).
Ma, W. P. et al. The use of mixed generalized additive modeling to assess the effect of temperature on the usage of emergency electrocardiography examination among the elderly in Shanghai. PLoS One 9, e100284, doi: 10.1371/journal.pone.0100284 (2014).
Yang, L., Qin, G., Zhao, N., Wang, C. & Song, G. Using a generalized additive model with autoregressive terms to study the effects of daily temperature on mortality. BMC Med Res Methodol 12, 165 (2012).
Leiva, G. M., Santibanez, D. A., Ibarra, E. S., Matus, C. P. & Seguel, R. A five-year study of particulate matter (PM2.5) and cerebrovascular diseases. Environ Pollut 181, 1–6 (2013).
Shanghai Research Center on Aging. Demographics, < http://www.shrca.org.cn/sub02_1_1.html?page=3> (2007) (Date of access: March 11, 2015).
Benjamin, M. A., Rigby, R. A. & Stasinopoulos, D. M. Generalized autoregressive moving average models. J Am Stat Assoc 98, 214–223 (2003).
Hastie, T. & Tibshirani, R. Generalized Additive Models. (Chapman & Hall, 1990).
Shinkawa, A., Ueda, K., Hasuo, Y., Kiyohara, Y. & Fujishima, M. Seasonal variation in stroke incidence in Hisayama, Japan. Stroke 21, 1262–1267 (1990).
Suzuki, K. et al. Clinico-epidemiologic study of stroke in Akita, Japan. Stroke 18, 402–406 (1987).
Wang, Y. et al. Seasonal variation in stroke in the Hunter Region, Australia: a 5-year hospital-based study, 1995-2000. Stroke 34, 1144–1150 (2003).
Khan, F. A., Engstrom, G., Jerntorp, I., Pessah-Rasmussen, H. & Janzon, L. Seasonal patterns of incidence and case fatality of stroke in Malmo, Sweden: the STROMA study. Neuroepidemiology 24, 26–31 (2005).
Jakovljevic, D. et al. Seasonal variation in the occurrence of stroke in a Finnish adult population. The FINMONICA Stroke Register. Finnish Monitoring Trends and Determinants in Cardiovascular Disease. Stroke 27, 1774–1779 (1996).
Diaz, A., Gerschcovich, E. R., Diaz, A. A., Antia, F. & Gonorazky, S. Seasonal variation and trends in stroke hospitalizations and mortality in a South American community hospital. J Stroke Cerebrovasc Dis 22, e66–69 (2013).
Kelly-Hayes, M. et al. Temporal patterns of stroke onset. The Framingham Study. Stroke 26, 1343–1347 (1995).
Oberg, A. L., Ferguson, J. A., McIntyre, L. M. & Horner, R. D. Incidence of stroke and season of the year: evidence of an association. Am J Epidemiol 152, 558–564 (2000).
Zhang, Y. et al. The effects of ambient temperature on cerebrovascular mortality: an epidemiologic study in four climatic zones in China. Environ Health 13, 24 (2014).
Basu, R. & Ostro, B. D. A multicounty analysis identifying the populations vulnerable to mortality associated with high ambient temperature in California. Am J Epidemiol 168, 632–637, doi: 10.1093/aje/kwn170 (2008).
Revich, B. & Shaposhnikov, D. Temperature-induced excess mortality in Moscow, Russia. Int J Biometeorol 52, 367–374 (2008).
Ellis, F. P., Prince, H. P., Lovatt, G. & Whittington, R. M. Mortality and morbidity in Birmingham during the 1976 heatwave. Q J Med 49, 1–8 (1980).
Keatinge, W. R. et al. Increases in platelet and red cell counts, blood viscosity and arterial pressure during mild surface cooling: factors in mortality from coronary and cerebral thrombosis in winter. Br Med J (Clin Res Ed) 289, 1405–1408 (1984).
Hata, T. et al. The seasonal variation of blood pressure in patients with essential hypertension. Clin Exp Hypertens A 4, 341–354 (1982).
Qizilbash, N., Jones, L., Warlow, C. & Mann, J. Fibrinogen and lipid concentrations as risk factors for transient ischaemic attacks and minor ischaemic strokes. BMJ 303, 605–609 (1991).
Stout, R. W. & Crawford, V. Seasonal variations in fibrinogen concentrations among elderly people. Lancet 338, 9–13 (1991).
Cheng, X. & Su, H. Effects of climatic temperature stress on cardiovascular diseases. Eur J Intern Med 21, 164–167 (2010).
Manfredini, R., Gallerani, M., Portaluppi, F., Salmi, R. & Fersini, C. Chronobiological patterns of onset of acute cerebrovascular diseases. Thromb Res 88, 451–463 (1997).
Pan, W. C. et al. Ambient Temperature and Cerebrovascular Hemodynamics in the Elderly. PLoS One 10, e0134034, doi: 10.1371/journal.pone.0134034 (2015).
Acknowledgements
We would like to thank the reviewers whose comments substantially improved the quality of the manuscript.
Author information
Authors and Affiliations
Contributions
X.Z. and N.Z. conceived and designed the study. X.Z. and W.M. provided the data. W.M. and X.W. analyzed the data. X.W. and N.Z. wrote the main manuscript text. All authors reviewed the manuscript.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Electronic supplementary material
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Zhang, XJ., Ma, WP., Zhao, NQ. et al. Time series analysis of the association between ambient temperature and cerebrovascular morbidity in the elderly in Shanghai, China. Sci Rep 6, 19052 (2016). https://doi.org/10.1038/srep19052
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep19052
This article is cited by
-
Time series analysis of temporal trends in the pertussis incidence in Mainland China from 2005 to 2016
Scientific Reports (2016)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
