
Abstract
This study aimed to investigate the role of AR-V7 in development of castration-resistant prostate cancer (CRPC) and to determine whether the AR-V7 expression in CRPC tissues can predict cancer-specific survival. We enrolled 100 localized prostate cancer (PCa) (cohort 1), 104 newly diagnosed metastatic PCa (cohort 2) and 46 CRPC (cohort 3) patients treated at our institution. The expression of AR-V7 in PCa was assessed by immunohistochemistry. Cox regression models were used to evaluate the predictive role of all covariates for the development of CRPC in cohort 2 and for cancer-specific survival in cohort 3. Time to CRPC and cancer-specific survival curves were estimated using the Kaplan-Meier method. AR-V7 expression rate in cohort 3 was significantly elevated compared with other two cohorts (p < 0.001). Multivariate analysis revealed that AR-V7 was an independent predictive factor for CRPC development (HR = 2.627, p = 0.001) and for cancer specific survival (HR = 2.247, p = 0.033). Furthermore, the AR-V7 expression was associated with shorter survival in CRPC patients. Our results demonstrated protein AR-V7 levels in primary tumors can be used as a predictive marker for the development of CRPC and as a prognostic factor in CRPC patients. Therapy targeting AR-V7 may help prevent PCa progression and improve the prognosis of CRPC patients.
Similar content being viewed by others

Introduction
Prostate cancer (PCa) is the most frequently diagnosed male malignancy in Western countries and represents the second leading cause of cancer-related death1. In China, the incidence of PCa, although lower than in developed countries, has increased remarkably over the past two decades partly attributed to increasing life expectancy, dietary changes and Westernized lifestyle. Furthermore, most newly diagnosed PCa patients already have metastatic disease because of a lack of PCa screening use prostate-specific antigen (PSA) and digital rectal examination in China2. Androgen deprivation therapy remains the mainstay of advanced PCa management; however, almost all patients relapse and progress to castration-resistant prostate cancer (CRPC) within a median of 18–24 months3, which is accompanied by poor outcome and high lethality. To date, the mechanisms underlying the transition to CRPC have not been fully clarified.
Androgen and androgen receptors (ARs) play essential roles in the initiation and progression of PCa. Structurally, the human AR gene is composed of eight exons and encodes a multi-domain protein consisting of an N-terminal transactivation domain (NTD), a central DNA-binding domain (DBD), a hinge region and a C-terminal ligand-binding domain (LBD)4,5. Recent results indicate that the LBD appears to be dispensable for AR transcriptional activity as its deletion leads to constitutive activation of AR transcription capability6,7,8. Constitutively active, ligand-independent AR splice variants were proposed to be partly responsible for the development and growth of CRPC, irrespective of androgen level9,10,11,12,13,14,15. Among more than 20 AR splice variants identified to date, AR-V7 is one of the most abundant and best characterized variants7,14,16. The clinical relevance of AR-V7 has also been characterized in some respects. For instance, it was reported that increased transcription or protein AR-V7 levels has been detected in CRPC metastases and elevated expression of AR-V7 in PCa tissues is associated with biochemical recurrence and shorter survival13,14,17. However, the predictive value of AR-V7 expression in primary PCa for the development of CRPC and its prognostic value for CRPC patients have not been well documented.
In the current study, immunohistochemistry with an AR-V7 specific antibody, which is a feasible technique that is routinely used in clinical diagnosis, was employed to investigate the expression of AR-V7 in different stages of PCa (cohort 1, 100 localized PCa; cohort 2, 104 newly diagnosed metastatic PCa; cohort 3, 46 CRPC). We assessed the association between AR-V7 expression and patient characteristics and evaluated whether AR-V7 expression in primary tumors can predict the development of CRPC after adjusting for current prognostic factors, such as PSA nadir, time to PSA nadir and PSA half-life (PSAHL)18,19,20 in cohort 2. Moreover, we determined whether AR-V7 expression in CRPC tissues can predict cancer-specific survival after transurethral resection of the prostate (TURP) in cohort 3 who underwent TURP due to dysuria at the CRPC stage.
Results
Patient characteristics
The clinicopathological characteristics of the entire cohort are summarized in Table 1. Comparison of patient characteristics according to AR-V7 expression are described in Table 2. Follow-up for cohort 2 and cohort 3 continued until March 2014. During the follow-up period, 91 patients in cohort 2 (87.5%) advanced to the castration-resistant stage and 45 patients in cohort 3 (97.8%) died. All deaths were attributed to PCa or PCa-related complications. The median time to CRPC for cohort 2 was 25 months (range 2–132 months) and the median cancer-specific survival after TURP for cohort 3 was 17 months (range 4–51 months).
Expression of AR-V7 in different stages of PCa
As shown in Figure 1, AR-V7 expression rates in cohort 1, cohort 2 and cohort 3 were 12.0% (12/100), 21.2% (22/104) and 58.7% (27/46), respectively. The AR-V7 expression rate in cohort 3 (CRPC) was significantly elevated compared with other two cohorts (hormone-sensitive PCa) (p < 0.001). Nevertheless, there is no significant difference in AR-V7 expression between cohort 1 and cohort 2 (p = 0.079). Representative images of immunohistochemical staining for AR-V7 in different stages of PCa are shown in Figure 2.

The profile of AR-V7 expression in cohort 1 (localized PCa), cohort 2 (newly diagnosed metastatic PCa) and cohort 3 (CRPC).
PCa, prostate cancer; CRPC, castration-resistant prostate cancer.

Representative images of immunohistochemical staining for AR-V7 in (A) cohort 1 (localized PCa), (B) cohort 2 (newly diagnosed metastatic PCa) and (C) cohort 3 (CRPC) tissues (200×).
PCa, prostate cancer; CRPC, castration-resistant prostate cancer.
Association of AR-V7 expression with castration resistance in cohort 2
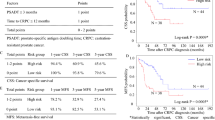
The results of univariate and multivariate Cox regression analysis for time to CRPC are depicted in Table 3. On univariate analysis, AR-V7 expression (hazard ratio [HR] 2.312, 95% confidence interval [CI]: 1.418–3.770, p = 0.001), PSA nadir (HR 1.011, 95% CI: 1.001–1.020, p = 0.023) and PSAHL (HR 1.023, 95% CI: 1.001–1.046, p = 0.041) were significantly correlated with time to CRPC. Multivariate analysis revealed that AR-V7 expression (HR 2.627, 95% CI: 1.480–4.663, p = 0.001) and PSA nadir (HR 1.012, 95% CI: 1.002–1.022, p = 0.019) maintained a significant predictive role for the development of CRPC after adjusting for age, PSA, Gleason score, stage, time to PSA nadir and PSAHL. The median times to CRPC for patients with and without AR-V7 expression were 15 months and 30 months, respectively (p < 0.001). Time to CRPC curves are reported in Figure 3.

Kaplan-Meier analysis for time to CRPC in cohort 2 according to AR-V7 expression.
CRPC, castration-resistant prostate cancer.
Association of AR-V7 expression with a poor prognosis in cohort 3
The results of univariate and multivariate Cox regression analysis for cancer-specific survival after TURP are described in Table 4. The univariate analysis revealed that AR-V7 expression (HR 2.646, 95% CI: 1.348–5.193, p = 0.005), time to CRPC (HR 0.492, 95% CI: 0.264–0.917, p = 0.025), PSADT (HR 0.478, 95% CI: 0.259–0.882, p = 0.018) and M stage at TURP (HR 2.295, 95% CI: 1.081–4.876, p = 0.031) may associated with cancer-specific survival. Subsequent multivariate analysis reserved AR-V7 expression (HR 2.247, 95% CI: 1.066–4.737, p = 0.033), along with time to CRPC (HR 0.397, 95% CI: 0.199–0.793, p = 0.009), as independent prognostic factors of cancer-specific survival after adjusting for possible confounders. The median cancer-specific survival after TURP for patients with and without AR-V7 expression were 14 months and 21 months, respectively (p = 0.003). The time distributions among AR-V7 expression with respect to cancer-specific survival after TURP are displayed in Figure 4.

Kaplan-Meier analysis of AR-V7 expression in cohort 3 versus cancer-specific survival after TURP.
TURP, transurethral resection of the prostate.
Expression of AR-V7 is inversely associated with serum PSA level
We observed that the expression of AR-V7 in 104 newly diagnosed PCa patients was inversely associated with serum PSA level at diagnosis. The median serum PSA level was 84.8 ng/mL in patients with AR-V7 positive expression, which was significantly lower than in patients with AR-V7 negative expression (130.3 ng/mL, p = 0.014; Table 2). Furthermore, the expression of AR-V7 in 46 CRPC tissues was inversely correlated with serum PSA level at surgery. The median serum PSA level at surgery for patients with and without AR-V7 expression were 22.7 ng/mL and 94.0 ng/mL, respectively (p = 0.045; Table 2).
Discussion
The present study describes, for the first time, the AR-V7 expression pattern in different stages of PCa in Chinese patients and investigated its predictive value for the development of CRPC and prognostic value for CRPC patients. In this study, we noted that AR-V7 expression in CRPC was significantly elevated, expression of AR-V7 was an independent predictive factor for the development of CRPC and it was associated with poor prognosis in CRPC patients. In addition, we found that the expression of AR-V7 in primary PCa tissues was inversely correlated with serum PSA level.
Hu et al.14 reported that expression of AR-V7, measured at the mRNA level, demonstrated an average 20-fold higher in CRPC compared with hormone-naïve PCa (p < 0.001) and elevated expression of AR-V7 predicted biochemical recurrence after radical prostatectomy among the hormone-naïve PCa (p = 0.012). Results from a large study containing 429 human PCa specimens showed that AR-V7 was significantly upregulated during PCa progression and expression of AR-V7 in primary prostate tumors was predictable for survival outcome after radical prostatectomy, with a shorter time to biochemical recurrence in individuals with elevated levels (p < 0.001)13. We found that protein expression of AR-V7 was more frequently detected in CRPC compared with hormone-sensitive PCa (p < 0.001) and the expression of AR-V7 in newly diagnosed metastatic PCa was correlated with shorter time to CRPC, with median time to CRPC for patients with and without AR-V7 expression were 15 months and 30 months, respectively (p < 0.001). Furthermore, our data revealed that expression of AR-V7 (HR 2.627, p < 0.001), along with PSA nadir (HR 1.012, p = 0.019), could independently predict the development of CRPC after adjusting for possible confounders. Notably, expression of AR-V7 could better predict the development of CRPC compared with PSA nadir. On the basis of these findings, we speculate that PCa cells may hijack the androgen-independent AR-V7 to escape hormonal therapy and that aberrant expression of constitutively active AR-V7 may be a novel mechanism underlying the development of CRPC during PCa progression. Recently, Cao et al.21 observed that AR-V7 could activate the full-length AR in mediating resistance to androgen-directed therapy by both facilitating full-length AR nuclear localization in the absence of androgen and mitigating the ability of the anti-androgen enzalutamide to inhibit full-length AR nuclear trafficking.
Currently, limited molecular markers are available to predict CRPC patient outcomes. In a recent study, Hörnberg et al. found that the number of AR-V7 transcripts is increased in CRPC compared with hormone-sensitive bone metastases and is associated with a poor prognosis (p = 0.018)17. Accordingly, our study confirmed that expression of AR-V7 in primary tumors from CRPC patients was significantly associated with shorter survival, with median cancer-specific survival after TURP for patients with and without AR-V7 expression were 14 months and 21 months, respectively (p = 0.003). Poor prognosis of CRPC patients with AR-V7 expression is probably related to the postulated constitutive activity of AR-V7, which contains the nucleus localization sequence in its cryptic exon14. Unlike AR, which is activated after androgen binding, conformational changes and entering into the nucleus, the ligand-independent AR-V7 mediates genomic functions despite the absence of androgens or the presence of anti-androgens22. Results from published studies reveal that AR-V7 can translocate into the nucleus, bind AR responsive elements and regulate gene transcription in vitro without the need for ligand binding7,11,14,23.
We also noted that the expression of AR-V7 in both newly diagnosed metastatic PCa (p = 0.014) and CRPC patients (p = 0.045) was inversely correlated with the serum PSA level, which is in accordance with previous research16. Similarly, another study by Hornberg et al.17 found that human PCa metastases with higher AR-V7 expression showed significantly lower PSA expression. One possible explanation for this is that expression of AR-V7 and PSA are differentially regulated by androgen; that is, the expression of AR-V7 is increased by androgen deprivation and decreased upon androgen restoration11,24, while PSA is induced by androgen and repressed by androgen deprivation7,25.
The strengths of this study include it being the first report with regard to AR-V7 and PCa in a Chinese, or even an Asian, cohort. Second, the study was carried out at a single center with no discontinuity in recruitment and all surgical procedures, specimen evaluations, therapeutic schemes and follow-up examinations were performed using a consistent method. Third, we employed immunohistochemistry, which is feasible and routinely used in clinical diagnosis, combined with an AR-V7 specific antibody, instead of traditional anti-AR antibodies used in a previous study26, to detect the expression of AR-V7.
Despite its strengths, the present study has some limitations. For instance, we assessed the expression and predictive effect of AR-V7 without considering the expression of full-length AR and other AR splice variants, such as AR-V1 and ARv567es and the controversial interplay between them11,15,21. Another limitation was that we can't provide information from an independent patient cohort although the single institution nature of this study guarantee the uniform management throughout the study. Notwithstanding these limitations, our findings underscore that a further understanding of biological processes deregulated in cases with high expression of constitutively active AR-V7 may offer opportunities for rational development of approaches to predict, monitor, or prevent PCa progression in a castration setting.
In summary, constitutively active AR-V7 were more frequently expressed in CRPC compared with hormone sensitive PCa. Moreover, higher expression of AR-V7 in primary tumors was associated with CRPC development and predicted poor prognosis within the CRPC cohort. Our findings suggest that therapy targeting AR-V7 may help prevent PCa progression and improve the prognosis of CRPC patients.
Methods
Patients, tissue samples and variables
We enrolled 100 clinically localized PCa patients (cohort 1, treated from June 2008 to January 2010), 104 newly diagnosed metastatic PCa patients (cohort 2, treated from January 2002 to January 2008) and 46 CRPC patients (cohort 3, treated from January 2002 to June 2010), who were treated at Fudan University Shanghai Cancer Center. Cancer tissues were obtained from radical prostatectomy (cohort 1), prostate biopsy (cohort 2), or TURP (cohort 3) under an institutional review board-approved protocol. Haematoxylin and eosin sections were reviewed by the study pathologists to determine the presence of representative areas of the original samples and to confirm tumor histology and grade according to the Gleason system. The study was carried out in accordance with the ethical standards of the Helsinki Declaration II and approved by the Institution Review Board of Fudan University Shanghai Cancer Center. Written informed consent was obtained from each patient before any study-specific investigation was performed.
Patient characteristics, such as age, serum PSA level, Gleason score and metastatic sites were collected. The PSA nadir was the minimal serum PSA achieved during the first hormonal therapy. Time to PSA nadir was defined as the time interval between initial PSA and PSA nadir. PSAHL was defined as the time required for the PSA concentration to decline by exactly one-half during the first hormonal therapy and was calculated according to the formula:

where PSAnadir and PSAinitial are the PSA nadir and initial PSA during the first hormonal therapy, respectively, T is the time interval between these values and log refers to the natural logarithm. If the PSA nadir value was zero or undetected, the nearest measurement of a non-zero value before the nadir was used27. PSADT (PSA doubling time) was defined as the time required for the PSA level to double and was calculated according to the formula:

where PSA2 is the PSA defining CRPC and PSA1 is the next most recent PSA level, respectively, T is the time between PSA measurements and ln is the natural logarithm. All patients were followed up via medical records or telephone. The time to CRPC was calculated from the time of diagnosis until CRPC confirmation in cohort 2. For cohort 3, cancer-specific survival after TURP was calculated as the interval between the TURP date (at castration-resistant stage) and the date of death or the last follow-up visit for censored patients.
Immunohistochemistry staining
Immunostaining of AR-V7 was performed using a mouse monoclonal anti-AR-V7 antibody (A&G Pharmaceutical, Columbia, MD, USA) and the Envision detection kit (Dako, Carpinteria, CA, USA). The 4-μm-thick sections from the formalin-fixed paraffin-embedded representative PCa tissue blocks were deparaffinized in a series of xylene and hydrated in a graded series of ethanol solutions. Antigen retrieval was performed with 10 mM citrate buffer solution (pH 6.0) in a pressure cooker (20 psi for 10 min). Endogenous peroxidase was quenched in 3% hydrogen peroxide for 15 min at 37°C and nonspecific binding was blocked with 10% normal goat serum for 1 h at room temperature. Sections were then incubated with the primary antibody (1:200 dilution in Dako antibody diluent) at 4°C overnight. Chromogenic detection was carried out using a peroxidase-conjugated secondary antibody (30 min) and DAB reagents (5 min) provided in the Envision detection kit (Dako). Tissue sections were counterstained with Meyer's Haematoxylin (Thermo Fisher Scientific, Waltham, MA, USA). Omission of the primary antibody with phosphate-buffered saline served as a negative control.
All slides were examined and scored by two experienced pathologists, who were blinded to all clinical data, in an open discussion. Considering the heterogeneity of prostate cancer, we selected the tumor area where the AR-V7 expression was relatively stronger to evaluate each tissue sample. The nuclear AR-V7 immunostaining was measured based on the quantity of immunoreactive cells (quantity score) and the intensity of immune staining (intensity score), as previously reported28,29. The percent positivity was scored as 0, <1%; 1, 1%–10%; 2, 11%–50%; 3, 51%–80% and 4, >81%. The staining intensity was scored as 0, negative staining; 1, weak equivocal staining; 2, unequivocal moderate staining; 3, strong staining. The final value of the analysis of each tissue sample was then expressed as an absolute value obtained by multiplying quantity score and intensity score. Cores with an immunostaining score of 0 or 1 were considered negative and those with an immunostaining score of ≥2 were considered positive.
Statistical analysis
Continuous data are presented as median (range) and categorical data are presented as number (proportion). Patient clinical and pathological characteristics according to AR-V7 expression were compared using the Student's t-test for continuous variables and the Chi-square test for categorical variables. Univariate and multivariate Cox regression models were used to evaluate the predictive role of all covariates for the development of CRPC in cohort 2 and for cancer-specific survival in cohort 3. Time to CRPC and cancer-specific survival after TURP curves were estimated using the Kaplan-Meier method and compared by the log-rank test. For all statistical tests, a two-sided p value of less than 0.05 was considered statistically significant. All statistical analyses were performed using SPSS software version 16.0 (SPSS Inc., Chicago, IL, USA).
References
Ferlay, J. et al. Estimates of the cancer incidence and mortality in Europe in 2006. Ann Oncol 18, 581–592, 10.1093/annonc/mdl498 (2007).
Dai, B., Ye, D. W., Kong, Y. Y., Shen, Y. J. & Wang, B. H. Individualized prostate biopsy strategy for Chinese patients with different prostate-specific antigen levels. Asian J Androl 10, 325–331, 10.1111/j.1745-7262.2008.00345.x (2008).
Qu, Y. Y. et al. Prognostic factors in Chinese patients with metastatic castration-resistant prostate cancer treated with docetaxel-based chemotherapy. Asian J Androl 15, 110–115, 10.1038/aja.2012.110 (2013).
Gelmann, E. P. Molecular biology of the androgen receptor. J Clin Oncol 20, 3001–3015 (2002).
Dehm, S. M. & Tindall, D. J. Alternatively spliced androgen receptor variants. Endocr-Relat Cancer 18, R183–196, 10.1530/ERC-11-0141 (2011).
Libertini, S. J. et al. Evidence for calpain-mediated androgen receptor cleavage as a mechanism for androgen independence. Cancer Res 67, 9001–9005, 10.1158/0008-5472.can-07-1072 (2007).
Sun, S. et al. Castration resistance in human prostate cancer is conferred by a frequently occurring androgen receptor splice variant. J Clin Invest 120, 2715–2730, 10.1172/JCI41824 (2010).
Chan, S. C., Li, Y. & Dehm, S. M. Androgen receptor splice variants activate androgen receptor target genes and support aberrant prostate cancer cell growth independent of canonical androgen receptor nuclear localization signal. J Biol Chem 287, 19736–19749, 10.1074/jbc.M112.352930 (2012).
Lamont, K. R. & Tindall, D. J. Minireview: Alternative activation pathways for the androgen receptor in prostate cancer. Mol Endocrinol 25, 897–907, 10.1210/me.2010-0469 (2011).
Guo, Z. & Qiu, Y. A new trick of an old molecule: androgen receptor splice variants taking the stage. Int J Biol sci 7, 815–822 (2011).
Watson, P. A. et al. Constitutively active androgen receptor splice variants expressed in castration-resistant prostate cancer require full-length androgen receptor. P Natl Acad Sci USA 107, 16759–16765, 10.1073/pnas.1012443107 (2010).
Dehm, S. M., Schmidt, L. J., Heemers, H. V., Vessella, R. L. & Tindall, D. J. Splicing of a novel androgen receptor exon generates a constitutively active androgen receptor that mediates prostate cancer therapy resistance. Cancer Res 68, 5469–5477, 10.1158/0008-5472.can-08-0594 (2008).
Guo, Z. et al. A novel androgen receptor splice variant is up-regulated during prostate cancer progression and promotes androgen depletion-resistant growth. Cancer Res 69, 2305–2313, 10.1158/0008-5472.CAN-08-3795 (2009).
Hu, R. et al. Ligand-independent androgen receptor variants derived from splicing of cryptic exons signify hormone-refractory prostate cancer. Cancer Res 69, 16–22, 10.1158/0008-5472.CAN-08-2764 (2009).
Hu, R., Isaacs, W. B. & Luo, J. A snapshot of the expression signature of androgen receptor splicing variants and their distinctive transcriptional activities. Prostate 71, 1656–1667, 10.1002/pros.21382 (2011).
Zhao, H. et al. Transcript levels of androgen receptor variant AR-V1 or AR-V7 do not predict recurrence in patients with prostate cancer at indeterminate risk for progression. J Urology 188, 2158–2164, 10.1016/j.juro.2012.08.014 (2012).
Hornberg, E. et al. Expression of androgen receptor splice variants in prostate cancer bone metastases is associated with castration-resistance and short survival. PloS one 6, e19059, 10.1371/journal.pone.0019059 (2011).
Morote, J., Trilla, E., Esquena, S., Abascal, J. M. & Reventos, J. Nadir prostate-specific antigen best predicts the progression to androgen-independent prostate cancer. Int J Cancer 108, 877–881, 10.1002/ijc.11639 (2004).
Crawford, E. D., Bennett, C. L., Andriole, G. L., Garnick, M. B. & Petrylak, D. P. The utility of prostate-specific antigen in the management of advanced prostate cancer. BJU Int 112, 548–560, 10.1111/bju.12061 (2013).
Hyun Park, Y. et al. PSA half life and PSA doubling time as a predictor of response to androgen deprivation therapy for metastatic prostate cancer. J Urology 179, 185 (2008).
Cao, B. et al. Androgen receptor splice variants activating the full-length receptor in mediating resistance to androgen-directed therapy. Oncotarget 5, 1646–1656 (2014).
Hu, R., Denmeade, S. R. & Luo, J. Molecular processes leading to aberrant androgen receptor signaling and castration resistance in prostate cancer. Expert Rev Endocrinol Metab 5, 753–764, 10.1586/eem.10.49 (2010).
Sun, F. et al. Androgen receptor splice variant AR3 promotes prostate cancer via modulating expression of autocrine/paracrine factors. J Biol Chem 289, 1529–1539, 10.1074/jbc.M113.492140 (2014).
Yu, Z. et al. Rapid induction of androgen receptor splice variants by androgen deprivation in prostate cancer. Clin Cancer Res 20, 1590–1600, 10.1158/1078-0432.CCR-13-1863 (2014).
Liu, X., Choi, R. Y., Jawad, S. M. & Arnold, J. T. Androgen-induced PSA expression requires not only activation of AR but also endogenous IGF-I or IGF-I/PI3K/Akt signaling in human prostate cancer epithelial cells. Prostate 71, 766–777, 10.1002/pros.21293 (2011).
Zhang, X. et al. Androgen receptor variants occur frequently in castration resistant prostate cancer metastases. PloS one 6, e27970, 10.1371/journal.pone.0027970 (2011).
Lin, G. W. et al. Prostate-specific antigen half-life: a new predictor of progression-free survival and overall survival in Chinese prostate cancer patients. Asian J Androl 11, 443–450, 10.1038/aja.2008.36 (2009).
Mir, C. et al. Loss of androgen receptor expression is not associated with pathological stage, grade, gender or outcome in bladder cancer: a large multi-institutional study. BJU Int 108, 24–30, 10.1111/j.1464-410X.2010.09834.x (2011).
Nuzzo, P. V. et al. Prognostic value of stromal and epithelial periostin expression in human prostate cancer: correlation with clinical pathological features and the risk of biochemical relapse or death. BMC cancer 12, 625, 10.1186/1471-2407-12-625 (2012).
Acknowledgements
This study was supported in part by Grants from Guide Project of Science and Technology Commission of Shanghai Municipality (No. 124119a7300), Grants from International Cooperation and Exchange of Science and Technology Commission of Shanghai Municipality (No. 12410709300), Project of the National Natural Science Foundation of China (Grant No. 81272837) and a grant from the Outstanding Young Talent Training Plan of Shanghai Municipal Commission of Health and Family Planning (No. XYQ2013102).
Author information
Authors and Affiliations
Contributions
Y.Q. acquired, analyzed and interpreted the data and drafted the manuscript, B.D. and D.Y. designed and supervised the study. Y.K. and X.Y. reviewed Haematoxylin and eosin sections to determine the presence of representative areas of the original samples and to confirm tumor histology and grade, K.C. and Z.J. prepared all figures, H.Z., Y.Z. and G.S. edited all tables. All authors reviewed and approved the manuscript.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Rights and permissions
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International License. The images or other third party material in this article are included in the article's Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder in order to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
About this article

Cite this article
Qu, Y., Dai, B., Ye, D. et al. Constitutively Active AR-V7 Plays an Essential Role in the Development and Progression of Castration-Resistant Prostate Cancer. Sci Rep 5, 7654 (2015). https://doi.org/10.1038/srep07654
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep07654
This article is cited by
-
Proteogenomics of clear cell renal cell carcinoma response to tyrosine kinase inhibitor
Nature Communications (2023)
-
RNF8 up-regulates AR/ARV7 action to contribute to advanced prostate cancer progression
Cell Death & Disease (2022)
-
Proteogenomic characterization of MiT family translocation renal cell carcinoma
Nature Communications (2022)
-
The androgen receptor is a therapeutic target in desmoplastic small round cell sarcoma
Nature Communications (2022)
-
A proteogenomic analysis of clear cell renal cell carcinoma in a Chinese population
Nature Communications (2022)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
