
Abstract
The purpose of this study was to investigate the accuracy of double contrast-enhanced ultrasonography (DCEUS) for assessing the Borrmann classification of advanced gastric carcinoma (AGC) preoperatively. Three hundred twenty nine patients with proved AGC were enrolled. DCEUS (intravenous microbubbles combined with combined with oral contrast-enhanced ultrasound) was performed preoperatively. The diagnostic accuracy of DCEUS in determining Borrmann classification was compared with postoperative pathological findings. The reliability of DCEUS was analyzed. The accuracy of DCEUS in determining the Borrmann classification of AGC was 91.49%. The intra- and inter-observer reproducibility was both almost perfect for assessing the Borrmann classification of AGC by DCEUS. DCEUS could be considered as an accurate, non-invasive and reliable diagnostic method for preoperative Borrmann classification of advanced gastric carcinoma.
Similar content being viewed by others

Introduction
The classification of advanced gastric cancer (AGC), one of the crucial factors of therapeutic strategy, proposed by Borrmann in 1926 according to the macroscopic aspect1, is still widely used by surgeons, pathologists and endoscopists around the world2. Many modalities, such as computed tomography (CT) and endoscopy have been used for assessing the Borrmann classification of AGC. Particularly, multi-detector row CT (MDCT) with multi-planar reformatted views is a powerful test for non-invasive evaluation of gastric cancer3. However, it carries a burden on ionizing radiation which may be a disadvantage4.
Upper digestive tract endoscopy is the gold standard in the diagnosis of gastric tumors. With the advent of endoscopy, accuracy in the diagnosis of gastric carcinoma has undoubtedly improved5. When combined with biopsy and brush cytology, endoscopy has an overall sensitivity of 95%–98% in the detection of gastric cancer6,7.
Unfortunately, endoscopy has a wide range of accuracy according to the gross tumor growth pattern and anatomic tumor location8 and additionally which is rather invasive and traumatic. In patients with linitis plastica, endoscopy has been reported to have a sensitivity of only 33%–73%8,9. Endoscopists often have difficulty recognizing these lesions, as the tumors are located predominantly in the submucosa; therefore, the overlying mucosa appears normal. Furthermore, the tumor cells of scirrhous gastric carcinoma are often dispersed within a dense fibrous matrix and tend to be widely separated8,9,10.
There is an obvious tendency in modern medicine to identify widely accessible, well-tolerated, non invasive, precise diagnostic procedures. Our previous studies and other reports had shown that intravenous contrast-enhanced ultrasound combined with oral contrast-enhanced ultrasound (DCEUS) is an accurate, non-invasive and reliable diagnostic method for preoperative assessment and detection of AGC11,12,13,14,15,16. The aim of this study was to assess the accuracy of the Borrmann classification in patients with AGC compared with postoperative pathology, using ultrasonography with DCEUS, in which an oral ultrasonic contrast agent is combined with an intravenous contrast agent.
Results
Three hundred and twenty nine patients with AGC were enrolled in this study and treated with surgery. Among them, the pathological Borrmann classification in 23 cases (6.70%) was type I; in 69 cases (20.97%) was type II; in 161 cases (48.94%) was type III and in 76 cases (23.10%) was type IV. The overall accuracy of DCEUS in determining the Borrmann classification of AGC was 91.49%, the accuracy of DCEUS in determining Borrmann I, II, III and IV was 86.96%, 89.86%, 91.93% and 93.42% respectively. A total of 17 cases were overstaged (3 patients with Borrmann I were overstaged as II; 6 patients with II were overstaged as III; 8 patients with III were overstaged as IV) and 11 cases were understaged(1 patient with II was understaged as I; 5 patients with III were understaged as II; 5 patients with IV were understaged as III) (Table 1). The sensitivity, specificity, PPV and NPV of DCEUS in determining Borrmann classification were listed in Table 2.
The intra- and inter-observer reproducibilities were both almost perfect for assessing the Borrmann classification of AGC with a Kappa value of 0.880 (P < 0.001) for intra-observer (Table 3) and 0.834 (P < 0.001) for inter-observer (Table 4) by DCEUS.
Discussion
Conventionally, the role of transabdominal ultrasonography in the evaluation of gastric carcinoma has been to assess the presence of distant metastases, especially to regional nodes and the liver. However, it is difficult to visualize gastric cancers of small size and deep location because of interference by intragastric gas. Oral contrast enhanced ultrasound improves imaging by displacing the air in the stomach and by distending the gastric lumen, thus helping to display mucosal lesions20,21. Intravenous contrast imaging allows for assessment of blood perfusion of the lesions using an intravascular contrast agent. Thus, DCEUS is able to demonstrate both morphologic appearances and perfusion status of both normal and abnormal structures.
The intravenous contrast agent we used is SonoVue, a blood pool agent that does not cross into the interstitial space22,23. Because such microbubbles flow with red blood cells, the injected microbubbles act as markers for tissues that are densely vascularized. Modern multipulse imaging methods, such as the CPS we have used, effectively suppress tissue echoes, so that the microvasculature can be detected24,25.
Our data has similar prevalence rates to those reported by Maruyama and Baba26. Our study shows that DCEUS can be used to visualize the thickened gastric wall and to assess the Borrmann classification of AGC. The intra- and inter-observer reproducibilities were both almost perfect for assessing the Borrmann classification of AGC with a Kappa value of 0.88 (P = 0.000) for intra-observer and 0.83 (P = 0.000) for inter-observer of DCEUS, showing that the consistency was very good and that the criteria could be learned and applied easily.
Oral contrast enhancd ultrasound is restricted by many factors, such as the limit of resolution, the small difference of the acoustic impedance among different tissues (making for low contrast) and necrotic tissue persisting in the surface of gastric ulcer causing posterior acoustic attenuation. It is difficult to distinguish tumor infiltrate from inflammation adjacent to the lesion and from peritumoral fibrosis on B-mode, so that overestimation or underestimation of the Borrmann classification may occur when using oral contrast enhancd ultrasound27. A total of 27 (12.3%) of our patients were overestimated and 24 (30.2%) patients were underestimated using oral contrast enhancd ultrasound.
Angiogenesis is essential for the growth of solid tumors28. Intravenous contrast-enhanced ultrasonography (CEUS) is a useful modality to assess the angiogenesis of cancers29. In term of the difference from CT contrast agents such as lipiodol, microbubble-based contrast agent does not penetrate the vessel walls and so behaves as a blood pool agent. Its distribution in the lesion represents the distribution of the microvessels so the intensity of the enhancement represents the density of these vessels30,31,32. Microvascular assessment is more sensitive for the evaluation of tumor stage, lesion size and sonographic appearance33. Therefore, DCEUS can be used to evaluate the morphology of gastric lesions. In this study, the CEUS was performed with CPS mode, which uses phase and amplitude modulation to separate the microbubble signals the echoes from tissue and from the oral contrast agent within the gastric lumen, which does not appear on microbubble-specific images since it behaves like tissue with minimal non-linear properties. Because such microbubbles flow with red blood cells, the injected microbubbles act as markers for gastric cancers that are densely vascularized, thus complementing the improved visualization of the gastric wall provided by the oral contrast agent. Its advantage is the high-contrast resolution between tumors and normal tissues, making it sensitive for lesion detection, characterization and staging. More importantly, DCEUS can show the relationship of the lesion's vasculature and the gastric wall as well as their contours.
Because of the use of harmonic technologies at low emission frequencies, there is some loss of spatial resolution and overall image quality, typically resulting in a grainy appearance of the CEUS images. Moreover, the depth at which the lesion resides affects the detectability of vascularity as deep-seated lesions give poorer signals34. Furthermore, two-dimensional views of DCEUS do not provide the gross appearance of macroscopic morphology of AGC. A total of 17 cases (5.2%) of overestimation and 11 (3.3%) cases of underestimation of Borrmann classification occurred using DCEUS.
There were some limitations to this study. First, this study was retrospective and included only patients referred to our hospital for surgery. Although blinded to the endoscopic, surgical and histopathologic results, the observers were aware of the presence of a tumor. Second, DCEUS examinations was paired rather than randomized unpaired. Third, comparative studies between DCEUS, CT, MRI or EUS on preoperative Borrmann classification were not carried out in this study and this is the subject of ongoing research.
Conclusion
DCEUS shows promise as a new noninvasive, convenient and repeatable method for preoperative Borrmann classification of advanced gastric carcinoma, which has a high accuracy.
Methods
Patients
Between October 2006 and June 2012, 390 patients were examined using DCEUS preoperatively. The inclusion criteria were as follows:  adenocarcinoma of stomach proven by endoscopic biopsy;
adenocarcinoma of stomach proven by endoscopic biopsy;  not treated with nonsteroidal antiinflammatory drugs, chemotherapy, radiotherapy or immunotherapy previously. Surgical resections were performed within 1 week after the DCEUS examination. The exclusion criteria were as follows:
not treated with nonsteroidal antiinflammatory drugs, chemotherapy, radiotherapy or immunotherapy previously. Surgical resections were performed within 1 week after the DCEUS examination. The exclusion criteria were as follows:  elderly patient with comorbidities for surgery (15 cases);
elderly patient with comorbidities for surgery (15 cases);  unresectable lesions with metastasis detected on preoperative evaluation (21 cases);
unresectable lesions with metastasis detected on preoperative evaluation (21 cases);  early stage tumors on postoperative pathology (25 cases). Finally, the remaining 329 patients (203 male and 126 female; age range, 31 ~ 81 years; mean age 62.0 ± 10.5 years) were enrolled in the study. Informed consent was obtained from all patients before their examination and the local ethics committee and institutional review board approved this prospective study (Ethics No.2006-02).
early stage tumors on postoperative pathology (25 cases). Finally, the remaining 329 patients (203 male and 126 female; age range, 31 ~ 81 years; mean age 62.0 ± 10.5 years) were enrolled in the study. Informed consent was obtained from all patients before their examination and the local ethics committee and institutional review board approved this prospective study (Ethics No.2006-02).
Ultrasonography
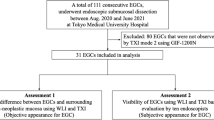
DCEUS of each case were performed after fasting for at least 6 hours; atropine sulfate (0.05 mg/kg) was administered via intramuscular injection 30 min before the examination to inhibit gastric peristalsis. The flowchart of DCEUS examination was shown in Figure 1. An Acuson Sequoia 512 system (Siemens, Mountain View, CA), equipped with a 4V1 vector™ transducer (frequency: 1.0–4.0 MHz) and the microbubble-specific contrast pulse sequencing (CPS) technology was used17. The linear signals from tissue are suppressed, leaving the non-linear microbubble signals that are used to form the microbubble-specific image in CPS mode. The oral contrast agent Xinzhang (Huqingyutang, HangZhou, China) was composed by a kind of soya derivative (48 grams per package); it was reconstituted by adding 500 mL of boiling water and gently stirring the water by hand to form a homogeneous suspension. After cooling to a comfortable temperature, the patient was asked to drink the palatable liquid as quickly as possible. It dilates the stomach and displaces the air within it so that the lumen appears as a homogenous mid-gray on B-mode imaging thus providing an acoustic window that lasts for around 60 min. It does not appear on microbubble-specific images since it behaves like tissue, with minimal non-linear properties.

Flowchart of DCEUS examination in patients with advanced gastric carcinoma.
The distal esophagus and the cardia of all patients were studied in real time B-mode using conventional tissue settings while the patients ingested the oral agent. Then the remaining parts of the stomach and the duodenal bulb were examined in turn, with the patient in the supine and both decubitus positions to facilitate complete filling and visualization of the lesion. The entire movie sequence of each case was stored on magnetic optical disks for analysis. When the lesion was displayed clearly, contrast-enhanced ultrasonography (CEUS) was performed using the contrast pulse sequencing (CPS) mode. The transmit frequency of 1.5 MHz and an acoustic power of −15 to −21 dB. This resulted in a low mechanical index (0.20), which minimized microbubble disruption. A cannula with 19-gauge was inserted into an antecubital fossa vein and 2.4 mL of SonoVue (Bracco, Milan Italy) was injected as a bolus followed by 10 mL of saline flush for each contrast study. A three-way tap was used so that the saline flush could be given immediately after the microbubble injection. A timer on the sonographic unit was activated at the beginning of the injection. The entire movie sequence (at least 5 minutes) was stored on magnetic optical disks for analysis. The i.v. contrast study could be repeated a second time if necessary.
Contraindications of DCEUS were defined for patients with pregnancy, breast-feeding and severe heart diseases, including instable coronary artery disease, frequent and/or repeated angina or chest pain in the past 7 days, acute cardiac failure, severe arrhythmic disorders, patients with right-to-left shunts, acute endocarditis, prosthetic valves, severe increase in pulmonary artery blood pressure, uncontrolled systemic hypertension and adult respiratory distress syndrome18.
Image analysis and Borrmann classification
The cine loops of DCEUS were reviewed by two radiologists (SL and PH, with 12 and 17 years of experience, respectively) in consensus without knowledge of the definitive diagnosis and other imaging information at the time of the analysis. Advanced carcinomas of the stomach were classified according to the Borrmann system, into four macroscopic tumor growth patterns types1 (Figure 2): Borrmann type I, nodular polypoid tumor without ulceration and usually with a broad base (Figure 3); type II, tumor is an ulcerative lesion but elevated and distinct borders(Figure 4); type III, an ulcerating tumor with a penetrating, infiltrating ulcer base (Figure 5); type IV, a diffuse thickening of the gastric wall, without a discretely marginated mass or ulceration (Figure 6).

Schematic diagram of Borrmann classification.

Oral contrast enhanced ultrasound(OCEUS) shows the thickened gastric wall with nodular polypoid appearance (arrow) (A), while DCEUS (B) shows that the lesion was enhanced with nodular aspect (arrow).
This case was classified as Borrmann I by OCEUS and DCEUS.

OCEUS (A) shows the thickened gastric wall with a penetrating, infiltrating ulcer base (calipers); while an ulcerative lesion with elevated and distinct borders (arrows) can be demonstrated by DCEUS (B).
This case was classified as Borrmann II by DCEUS.

An ulcerative lesion with larger ulcer can be shown using OCEUS (A) and the ulcerating tumor (arrow) with a penetrating, infiltrating ulcer base (large arrow) was demonstrated by DCEUS (B).
This case was classified as Borrmann III by DCEUS.

A diffuse thickening of the gastric wall (between the arrows), without a discretely marginated mass or ulceration can be seen on OCEUS (A) and DCEUS (B).
This case was classified as Borrmann IV by OCEUS and DCEUS. STO = distended lumen of stomach filled with oral contrast agent.
For the inter-observer reliability, the image data of DCEUS were analyzed again by another two ultrasound experts (MP and YZ, with 13 years of experience, respectively) in consensus and the results were compared with the previous findings (obtained by SL and PH) for calculating the inter-observer reliability. After three month, long enough for observer (SL) to forget his first responses, the analysis was repeated to evaluate the intra-observer reliability of DCEUS in assessing Borrmann classification of AGC. All these reviewers were blinded to the results of surgery and other reviewers' findings.
Immediately after surgery, the gastrectomy specimens were transferred to the department of pathology. The macroscopic types of the surgical specimens were classified according to Borrmann criteria1 by the pathologist (SW, with 6 years of experience), who was unaware of the ultrasound findings.
Statistical analysis
SPSS version 16.0 (SPSS Inc., Chicago, IL, USA) was used for the statistical analysis. The sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) were calculated for each macroscopic staging. Additionally, concordance of DCEUS within and between observers were assessed using Kappa analysis19 and a well reliability was set as Kappa value large than 0.75. For all analyses, P values less than 0.05 was considered statistically significant.
References
Borrmann, R. [Geschwulste des margens] Handbuch spez pathol anat und hist [Henke F. & Lubarsch O. (eds)][864–871] (Springer-Verlag, Berlin. 1926).
Borchard, F. Classification of gastric carcinoma. Hepatogastroenterology. 37, 223–232 (1990).
Lee, M. H., Choi, D., Park, M. J. & Lee, M. W. Gastric cancer: Imaging and staging with MDCT based on the 7th AJCC guidelines. Abdom Imaging. 37, 531–540 (2012).
Brenner, D. J. et al. Cancer risks attributable to low doses of ionizing radiation: assessing what we really know. Proc Natl Acad Sci USA. 100, 13761–13766 (2003).
Gore, R. M. Upper gastrointestinal tract tumours: diagnosis and staging strategies. Cancer Imaging. 5, 95–98 (2005).
Qizilbash, A. H., Castelli, M., Kowalski, M. A. & Churly, A. Endoscopic brush cytology and biopsy in the diagnosis of cancer of the upper gastrointestinal tract. Acta Cytol. 24, 313–318 (1980).
Llanos, O., Guzman, S. & Duarte, I. Accuracy of the first endoscopic procedure in the differential diagnosis of gastric lesions. Ann Surg. 195, 224–226 (1982).
Winawer, S. J. et al. Endoscopic diagnosis of advanced gastric cancer. Gastroenterology. 69, 1183–1187 (1975).
Levine, M. S., Kong, V., Rubesin, S. E., Laufer, I. & Herlinger, H. Scirrhous carcinoma of the stomach: radiologic and endoscopic diagnosis. Radiology. 175, 151–154 (1990).
Park, M. S. et al. Scirrhous gastric carcinoma: endoscopy versus upper gastrointestinal radiography. Radiology. 231, 421–426 (2004).
Huang, P. et al. Double contrast enhanced ultrasonography evaluation of preoperative Lauren classification of advanced gastric carcinoma. Arch Med Sci. 7, 287–293 (2011).
Xue, N. et al. Predicting lymph node status in patients with early gastric carcinoma using double contrast-enhanced ultrasonography. Arch Med Sci. 7, 457–464 (2011).
Zheng, Z. et al. Double contrast–enhanced ultrasonography for the preoperative evaluation of gastric cancer: a comparison to endoscopic ultrasonography with respect to histopathology. Am J Surg. 202, 605–611 (2011).
Li, S. et al. Preoperative T Staging of Advanced Gastric Cancer using Double Contrast-Enhanced Ultrasound. Ultraschall in Med. 33, E218–E224 (2012).
Badea, R. et al. The role of i.v. and oral contrast enhanced ultrasonography in the characterization of gastric tumors. A preliminary study. Med Ultrason. 14, 197–203 (2012).
Shi, H. et al. Double contrast-enhanced two-dimensional and three-dimensional ultrasonography for evaluation of gastric lesions. World J Gastroenterol. 18, 4136–4144 (2012).
Phillips, P. & Gardner, E. Contrast-agent detection and quantification. Eur Radiol. 14, 4–10 (2004).
Barnett, S. B., Duck, F. & Ziskin, M. Recommendations on the safe use of ultrasound contrast agents. Ultrasound Med Biol. 33, 173–174 (2007).
Landis, J. R. & Koch, G. G. An application of hierarchical kappa-type statistics in the assessment of majority agreement among multiple observers. Biometrics. 33, 363–374 (1977).
Harisinghani, M. G., Saini, S., Schima, W., McNicholas, M. & Mueller, P. R. Simethicone coated cellulose as an oral contrast agent for ultrasound of the upper abdomen. Clin Radiol. 52, 224–226 (1997).
Barr, R. G. Ultrasound contrast. Oral and i.v. agents amplify the image. Diagn Imaging (San Franc). 21, 56–61 (1999).
Schneider, M. et al. BR1: a new ultrasonographic contrast agent based on sulphur hexafluoride-filled microbubbles. Invest Radiol. 30, 451–457 (1995).
Schneider, M. SonoVue, a new ultrasound contrast agent. Eur Radiol. 9, S347–S348 (1999).
Brasch, R. C., Weinmann, H. J. & Wesbey, G. E. Contrast-enhanced NMR imaging: animal studies using gadolinium-DTPA complex. AJR. 142, 625–630 (1984).
Strich, G., Hagan, P. L., Gerber, K. H. & Slutsky, R. A. Tissue distribution and magnetic resonance spin lattice relaxation effects of gadolinium-DTPA. Radiology. 154, 723–726 (1985).
Maruyama, M. & Baba, Y. Gastric carcinoma. Radiol Clin North Am. 32, 1233–1252 (1994).
Ganpathi, I. S., So, J. B. & Ho, K. Y. Endoscopic ultrasonography for gastric cancer: does it influence treatment? Surg Endosc. 20, 559–562 (2006).
Folkman, J. Tumor angiogenesis: therapeutic implications. N Engl J Med. 285, 1182–1186 (1971).
Li, S. et al. The relationship between enhanced intensity and microvessel density of gastric carcinoma using double contrast-enhanced ultrasonography. Ultrasound Med Biol. 35, 1086–1091 (2009).
Lim, M., Cheshier, S. & Steinberg, G. K. New vessel formation in the central nervous system during tumor growth, vascular malformations and Moyamoya. Curr Neurovasc Res. 3, 237–245 (2006).
Des Guetz, G. et al. Microvessel density and VEGF expression are prognostic factors in colorectal cancer. Meta-analysis of the literature. Br J Cancer. 94, 1823–1832 (2006).
Zhao, H. et al. Microvessel density is a prognostic marker of human gastric cancer. World J Gastroenterol. 12, 7598–7603 (2006).
Lassau, N., Lamuraglia, M., Leclère, J. & Rouffiac, V. Functional and early evaluation of treatments in oncology: interest of ultrasonographic contrast agents. J Radiol. 85, 704–712 (2004).
Borzio, M. et al. Impact of large regenerative, low grade and high grade dysplastic nodules in hepatocellular carcinoma development. J Hepatol. 39, 208–214 (2003).
Acknowledgements
We thank Dr. David Cosgrove for his time spent in reviewing our manuscript. This study was supported by Health Bureau of Zhejiang Province (Project No. 2010KYB059), Wenzhou Science & Technology Bureau (Project No.H20060039), the National Natural Science Funds (Grant No. 81071164, 81271584) of China, the Key Specialty and Special Disease Foundation of Hangzhou Science and Technology Bureau (No. 20110733Q01) and the Main International Project of Zhejiang Province of China (No. 2009C14017), which is gratefully acknowledged and with no conflict of interest.
Author information
Authors and Affiliations
Contributions
P.H. designed this study. M.P. and Y.Z. acquired the data. P.H., S.L., S.W. and J.C. interpreted the data. P.H. and S.L. wrote the main manuscript text. All authors reviewed the manuscript.
Ethics declarations
Competing interests
On behalf of all authors of this paper, I declare that this study will not lead to any financial or other kinds of conflicts of interest.
Rights and permissions
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/3.0/
About this article
Cite this article
Pan, M., Huang, P., Li, S. et al. Double contrast-enhanced ultrasonography in preoperative Borrmann classification of advanced gastric carcinoma: comparison with histopathology. Sci Rep 3, 3338 (2013). https://doi.org/10.1038/srep03338
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep03338
This article is cited by
-
Double contrast-enhanced ultrasound for the preoperative gross classification of gastric cancer: a comparison with multidetector computed tomography
BMC Medical Imaging (2022)
-
Contrast-Enhanced Ultrasonography with Quantitative Analysis allows Differentiation of Renal Tumor Histotypes
Scientific Reports (2016)
-
Discriminative Learning for Automatic Staging of Placental Maturity via Multi-layer Fisher Vector
Scientific Reports (2015)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
