
Key Points
-
The largest study to date of the prevalence of advertising for foods and beverages potentially detrimental to dental health on UK television watched by children.
-
Awareness of the high proportion of advertisements that children are exposed to for items that are potentially detrimental to dental health should inform policy in this area.
-
Particular questions arising from these findings relate to how policymakers should handle foods that are classified as healthy from an obesity perspective but are detrimental to dental health.
Abstract
Objective To quantify the prevalence of advertising for foods and beverages potentially detrimental to dental health on UK television watched by children.
Design Content analysis of pre-recorded television advertisements (adverts).
Materials and methods Three hundred and fifty-two hours of television were recorded (one weekday and one weekend day, 6 am – 10 pm) from the main commercial channel (ITV1). All adverts were coded using pre-defined criteria.
Setting UK television recorded between January and December 2012.
Results Of 9,151 adverts, foods and beverages were the second most commonly advertised products (16.7%; n = 1,532). Nearly two-thirds of food adverts were for items that are potentially harmful to dental health (61%; n = 934). Of these, 96.6% were cariogenic and 11% were acidogenic foods. During peak children's viewing hours, the proportion of foods that are potentially harmful to dental health was significantly higher than for non-harmful foods (65.9% vs. 34.1%; p = 0.011). Adverts for foods potentially harmful to dental health were rare around children's programmes, but significantly more frequent during other programmes watched by children (p <0.001).
Conclusion UK children are exposed to a particularly high proportion of advertisements for foods that are potentially detrimental to their dental health during their peak viewing hours and around the programmes they watch the most.
Similar content being viewed by others

Introduction
Several systematic reviews of the literature have concluded that television food advertisements (adverts) can have a direct effect on children's dietary choices, behaviour, and attitudes.1,2,3 A recent meta-analysis has demonstrated equivocally that children significantly increase their food consumption following exposure to unhealthy food advertising.4
Children in the UK are exposed to far higher levels of unhealthy than healthy food advertising around the television programmes they watch.5 Specifically, many food and drink products being promoted on television are potentially harmful to children's dental health.6,7 Rodd and Patel6 examined 41 hours of children's television (ITV recorded during the after school period and on Saturday mornings) shown during summer 2003 and found that food and drink adverts accounted for 34.8% of all adverts (n = 342), and 95.3% (n = 326) of foods appearing were potentially damaging to dental health as they contained high levels of sugar and/or acid. In another study, Morgan et al.8 studied 503 hours of children's television (across four channels: ITV, CITV, Nick Junior and Nickelodeon with recordings covering at least 9.5 hours per test day) broadcast during late 2006 and early 2007, and found that adverts for food products made up 16.4% of all advertising time, and 38.4% of this time was devoted to potentially cariogenic products (high sugar foods). However, these data reflect small sample sizes and do not take seasonal differences into account – the latter has been shown to be an important source of variation in television food advertising.5
Evidence also shows that children who spend more time watching television are at a greater risk of developing caries.9 In 2013, close to a half (46%) of 15-year-olds and over a third (34%) of 12-year-olds in the UK had 'obvious decay experience' in their permanent teeth, with almost a third (31%) of 5-year-olds and nearly a half (46%) of 8-year-olds having a similar problem with their primary teeth.10 Dental caries is a significant public health problem in the UK11 and worldwide,12 and has been strongly linked to an increase in the consumption of food with high sugar levels.13 In one study, a significant association was found between a high intake of acidic soft drinks, fruit juices, diet drinks, and sports drinks and dental erosion in children/adolescents.14 The recent report of the UK Scientific Advisory Committee on Nutrition (SACN) also concluded that high levels of sugar consumption are associated with a greater risk of tooth decay (with consumption of high-sugar beverages being also linked to weight gain and risk of developing type 2 diabetes), and recommended that intake of 'free sugars' (such as is found in unsweetened fruit juices) should be restricted.15 However, it is notable that the hydration recommendations within the 'Eatwell Guide' from Public Health England (a tool intended to support individuals to 'have a well-balanced and healthy diet') focus only on reducing sugar intake (it suggests swapping sugary soft-drinks for 'diet, sugar-free or no added sugar varieties'), suggesting that reducing the nation's intake of potentially erosive sugar-free drinks is not a public health priority.16 However, it is also important to note that the experience of caries from the consumption of fermentable carbohydrates is not just dependent upon the level of sugar in the food or beverage, but also on patterns of sugar intake including type and frequency of consumption17.
Oral health problems are significant issues because not only do these have a negative impact on children's dental health (for example, tooth loss), but also consequences can extend to affect their psychosocial well-being, which may include dental pain,18 dental anxiety19 and missed school days.20 Moreover, the effect of such problems can go beyond affecting individuals to affect families (for example, stress) and there are implications for the health care resources used to provide treatment.20
Concerns over health problems, such as an increase in the prevalence of childhood obesity and ill-health due to poor food selection behaviours, led the Office of Communications (Ofcom), the UK broadcast media regulator, to introduce new regulations for television advertising of food and drink products to children in three phases from 2007, with the aim of reducing children's exposure to such advertisements.21 Ofcom's own analysis showed that there was a reduction of about a third in high fat, sugar and/or salt (HFSS) food advertising to children aged 415-years-old in 2007/8 compared to 2005.22 However, a 2009 systematic review of evidence on food advertising to children confirmed the persistence of the issue as the authors noted that foods with low nutrition were still being heavily promoted, with the regulations having shown little progress towards achieving the policy aims.23
To our knowledge, no study has been conducted after the full implementation of Ofcom's food advertising regulations to examine whether or not advertising for food and beverage products potentially detrimental to children's dental health are still being promoted around the programming children watch. Therefore, the current study aimed to examine the prevalence of advertising of foods and beverages that are potentially harmful to dental health on the UK television watched by children in 2012. Our objectives were to examine the extent of advertising of different types of cariogenic (those producing or promoting the development of tooth decay) and acidogenic (those for which consumption leads to acid production) foods and beverages, to look at the variations in their advertising patterns around various programme types, during the day, and across the year in order to better understand likely differences in children's exposure.
Methods
Ethics statement
Ethical approval was not required for this study because it did not involve human participants.
Television sampling
The sample included 384 hours of television recorded from the ITV1 channel between January and December of 2012. One weekday and one weekend-day every month were recorded. Weekday recordings were limited to either Tuesdays or Thursdays of each month to reduce the potential impact of variation in advertising across days of the week. For weekend-days, recordings were made on either Saturdays or Sundays. Sixteen hours were recorded on each day, from 6 am to 10 pm.
Television broadcasts from ITV1 were studied to be consistent with previous research in this area,6,8 and because this channel is considered the biggest commercial television network in the UK (with digital terrestrial platforms still the most popular method of viewing TV, despite rises in satellite and cable access24). According to the Broadcasters Audience Research Bureau, ITV is watched by up to 10 million people in a typical week.25 Although it is not clear from those data how many children are in the audience, their programmes made up five of the top ten most popular with children of all ages (415 years) in 201126 and as a majority of children's viewing time is outside of dedicated children's airtime,27 this was deemed an appropriate channel to study.
Out of the 384 recorded hours, 32 hours were missing due to recording errors.
Coding
Recorded television hours were scanned for both food and beverage (hereafter referred to collectively as 'food') adverts and non-food adverts. All adverts were coded according to a scheme previously used by Boyland et al.,5 adapted from Kelly et al.28 and Gantz et al.29 Some additions to this coding were made for the current study, where foods were further classified based on their effect on dental health (details below). Because of the variable nature of programme sponsorship, in line with Boyland et al.,5 these segments were excluded and not coded as adverts.
Coding scheme
Coding of food and non-food adverts
The coding categories for both food and non-food adverts were the day of the week, the date, the programme name and type of programme in which the advertisement was shown (for example, comedy, music, news, entertainment, games or children's). Children's programmes were defined as any show designed for children under the age of 12.29 The type of product in every advertisement was coded (for example, food/drink/supermarkets advertising for food/non-food products, motoring, and toys).
Children's television viewing periods were classified into peak and non-peak. Peak viewing hours, when more than a quarter of the potential child audience are expected to be watching, were between 17:30 and 22:00 hours on weekdays, and between 19:00 and 21:00 hours on weekend days. All other viewing hours were considered non-peak30.
Coding of food adverts
Food adverts were coded based on the promoted food's effect on dental health into foods potentially harmful (acidogenic and/or cariogenic), and potentially non-harmful to dental health.
Adverts for foods/products considered potentially non-harmful to dental health were further subdivided into the following groups: adverts for non-cariogenic and non-erosive foods (for example, fish), adverts for supermarkets promoting non-food products (for example, washing powder) or dental healthcare products, and adverts for food with possible anti-cariogenic and/or anti-erosive effects. If more than one food product was promoted in the advertisement, the most dominant one was coded. If equal attention was given to different food products, the first shown item was coded.21
Cariogenic foods
Foods with the potential to cause dental caries (all foods and beverages with the exception of those defined above as being potentially non-harmful to dental health) were classified based on their sugar content using the values underpinning the traffic light labelling scheme.31 Specifically with regard to sugar levels, items were categorised as zero sugar level, low (0.1 ≤1.8 g/100 g or 100 ml), medium (1.9–9.0 g/100 g or 100 ml), high (9.1–32.5 g/100 g or 100 ml), or very high sugar level (≥32.6 g/100 g or 100 ml).32 The foods containing very high sugar levels were classified based on the Nizel and Papas system into liquid, slowly dissolving food, solid, and sticky foods.33
Acidogenic foods
Acidogenic items were considered to be those with erosive potential, such as soft drinks, fresh fruit juices and fruit juice drinks.14
Coding procedure
All coding was performed by a single researcher (MA). Recordings were copied from a hard disk drive onto DVD discs for coding. Coding was logged on a pre-prepared Microsoft Excel 2010 spreadsheet in accordance with the pre-defined criteria.
Statistical analysis
The final Microsoft Excel 2010 spreadsheet was imported into a Statistical Package for the Social Sciences software file (SPSS version 21.0, IBM Corporation, Armonk: NY), which was used for the data analysis. Descriptive statistics including frequencies, percentages (%), confidence intervals (CI), and cross tabulation were used. Binary logistic regression analysis was used to ascertain the odds ratio (OR) that helps in identifying any relationship between adverts for potentially harmful foods to dental health and other factors such as children's programmes, and children's peak and non-peak viewing hours. Pearson's chi-squared test was used to assess the association between adverts for foods that are potentially harmful to dental health and the other independent variables, which included peak and non-peak children's viewing hours, advertising pattern across the year, and programme category. Statistical significance was regarded as a p value (2-sided) ≤0.05.
Results
The overall recorded sample of 352 hours included 9,151 adverts for different product types.
The extent of advertising of foods potentially harmful to dental health
Food adverts (a term used here to refer to both food and beverage adverts) made up 16.7% of all adverts in this sample (n = 1532) and a majority (61%; n = 934) were classified as potentially harmful to dental health.
Of the products potentially harmful to dental health, 89% were cariogenic, with a further 7.6% both cariogenic and acidogenic, and 3.4% were common (to the diet) acidogenic foods.
Advertising of cariogenic foods
Adverts for foods with high or very high sugar levels accounted for almost 45% of all cariogenic food adverts. Of those with very high sugar levels, almost 50% were sticky foods. Foods with a low sugar level (0.1–1.8 g/100 g or 100 ml) were the least commonly advertised products in this category, comprising only 14.7% of all cariogenic food adverts (Fig. 1).

Number of adverts for each type of cariogenic food
Advertising of acidogenic foods
Of the 1,532 food adverts coded, 103 adverts were for acidogenic items. Soft drinks dominated, representing 52.4% of all acidogenic product adverts, followed by fruit juices (37.9%).
The extent of advertising food potentially harmful and potentially non-harmful to dental health during peak and non-peak children's viewing times
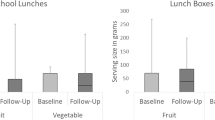
During both peak and non-peak viewing times, the majority of food advertisements depicted foods potentially harmful to dental health. During peak times, nearly two thirds (65.9%, n = 294) of all food advertisements shown were for foods potentially harmful to dental health. During non-peak times, 58.9% of food adverts (n = 640) depicted foods potentially harmful to dental health. The odds of a food advertisement being for food potentially harmful to dental health were significantly higher in peak children's viewing times than in non-peak times (odds ratio = 1.35, 95%CI; 1.07–1.70, p = 0.011) (Fig. 2).

Of all food adverts during peak viewing times, percentage of adverts for food potentially harmful and non-harmful to dental health
The extent of advertising of food potentially harmful to dental health around different programme categories
The extent of advertising food potentially harmful to dental health shown during different programme categories displayed considerable variations (Fig. 3). Although the number of adverts for food potentially harmful to dental health was less than 1% around dedicated children's programmes, those adverts were shown more during other programmes watched by greater numbers of children and young people. More than one third (42.7%) of all adverts for food potentially harmful to dental health were promoted in or around entertainment programmes (25.9%) and game shows (16.8%), which carried a significantly larger number of adverts for food potentially harmful to dental health than all other programme types (p <0.001).

Number of adverts for food potentially harmful and non-harmful to dental health during peak and non-peak children's viewing times
Variations in the food advertising patterns across the year
The monthly variations of advertising patterns for food potentially harmful to dental health across the year were found to be significant (p <0.001) (Table 1). When comparing the extent of advertising for foods potentially harmful to dental health for each month across the year, the highest percentage for such advertising was in March (70.7% of all food adverts shown in March), whereas the lowest was seen in December (42.8%). December was also the only month in which the proportion of adverts for food potentially harmful to dental health was less than the extent of adverts for foods/products potentially non-harmful to dental health.
Discussion
The results of this study showed that on the main commercial channel in the UK in 2012, almost two thirds of food adverts depicted food items that were potentially harmful to dental health, with a majority of these being cariogenic foods. Of the cariogenic food adverts, 43% were for foods/drinks containing high and very high sugar levels (>9 or 32.6 g/100 g or 100 ml). In the present study, food and drink products represented the second highest commonly advertised product, accounting for 16.7% of all adverts. This is consistent with the findings of previous studies.8,23 During peak children's viewing times, the prevalence of advertising for food potentially harmful to dental health (65.9%) was significantly higher than that for foods non-harmful to dental health (34.1%). Similar trends were found in a previous study.5
Furthermore, although the percentage of adverts for food potentially harmful to oral health was less than 1% in and around programmes specifically aimed at children, the food advertising in and around entertainment programmes and game shows had higher proportions of such items (25.9% and 16.8% respectively). This is consistent with previous studies which have shown greater prevalence of food advertising per se around these types of programmes. For example, Boyland et al.5 found that there were a significantly greater proportion of food advertisements in and around entertainment programmes (19.7%) as compared with children's programmes (4.5%) and Kelly et al.28 found that entertainment programmes were among the five programme categories with the highest proportion of food advertisements.21
It is apparent that, despite good adherence to the regulations,34 food marketers are still targeting children via television by promoting a significantly higher proportion of adverts for food potentially harmful to dental health during children's peak viewing times and around programmes that attract children and young teens, such as entertainment and games shows. The current findings are of particular concern given that children and adolescents spend the majority of their television viewing time outside of children's programmes.22
Some seasonal variation in food advertising patterns for items potentially harmful to dental health was observed. This is again consistent with previous research.5 The highest proportion of advertising of foods potentially harmful to dental health was found in March, and this is likely to reflect increased advertising of products associated with Easter (for example, chocolate eggs). Relative to other months, a reduction in the proportion of food adverts depicting items potentially harmful to dental health was seen in December. This is also consistent with Boyland et al.5 and, as in that study, is likely to result from increased miscellaneous supermarket advertising (that is, brand advertising or those promotions depicting a range of products that cannot be easily classified as healthy or unhealthy) over the pre-Christmas period. These differences emphasise the importance of analysing more than a single 'snapshot' of television in order to gain a clearer understanding of children's typical likely exposure, a strength of the current study.
This study also has some limitations. Analysis focused only on a single terrestrial channel, so the generalisability of the findings to other channels may be limited. The extensive availability of channels and changes in children's viewing habits (for example, the use of subscription channels like Netflix, and delayed viewing by 'catch up' services and YouTube) should be taken into account when evaluating children's exposure to food advertisements. A future study that includes a greater number of channels and viewing platforms would provide a more comprehensive assessment of children's exposure to food advertisements that promote foods potentially damaging to their dental health. In addition, it is a limitation of this study that it did not further consider which adverts were for foods that contain higher levels of sugar and are likely to be consumed frequently. It may be useful for future studies exploring this type of food advertising data to also incorporate coding to account for the foods and beverages most likely to be consumed frequently, in order to account for consumption patterns in relation to risk of dental problems.
However, the current study provides a retrospective insight into the extent of food advertising to children on UK television in 2012 with particular focus on post-regulation advertising of foods potentially damaging to dental health. The main area of concern is that children are exposed to a particularly high proportion of advertisements for foods potentially detrimental to oral health during peak children's viewing hours and also around other programmes watched by young people in large numbers. This suggests the need to apply a stricter restriction to meet the aim of the Ofcom regulations in significantly reducing children's exposure to unhealthy food advertisements.
Consideration should be given to the classification of foods as healthy (and therefore suitable to be advertised to children) when those products are detrimental to dental health (for example, zero calorie, sugar free carbonated soft drinks). Worrying numbers of children in the UK have dental health problems10 so arguably there is a need to take dental health, as well as obesity, into account when offering government-led consumer advice on hydration16 and when designing policies around food marketing to children.
References
Cairns G, Angus K, Hastings G . The extent, nature and effects of food promotion to children: A review of the evidence to December 2008. Prepared for the World Health Organization. Institute for Social Marketing, University of Stirling & the Open University. Geneva, Switzerland: WHO Press, 2009.
Institute of Medicine. Food marketing to children and youth: threat or opportunity? Washington DC: The National Academies Press, 2006.
Kunkel D, Wilcox B L, Cantor J, Palmer E, Linn S, Dowrick P . Report of the APA task force on advertising and children. 2004.
Boyland E J, Nolan S, Kelly B et al. Advertising as a cue to consume: a systematic review and meta-analysis of the effects of acute exposure to unhealthy food and nonalcoholic beverage advertising on intake in children and adults. Am J Clin Nutr 2016; 103: 519–533.
Boyland E J, Harrold J A, Kirkham T C, Halford J C G . The extent of food advertising to children on UK television in 2008. Int J Pediatr Obes 2011; 6: 455–461.
Rodd H D, Patel V . Content analysis of children's television advertising in relation to dental health. Br Dent J 2005; 199: 710–713.
Ghimire N, Rao A . Comparative evaluation of the influence of television advertisements on children and caries prevalence. Glob Health Action 2013; 6: 20066.
Morgan M, Fairchild R, Phillips A, Stewart K, Hunter L . A content analysis of children's television advertising: focus on food and oral health. Public Health Nutr 2009; 12: 748–755.
Locker D . Deprivation and oral health: a review. Community Dent Oral Epidemiol 2000; 28: 161–169.
The Health and Social Care Information Centre. The Children's Dental Health (CDH) Survey 2013, England, Wales and Northern Ireland. Available at: http://content.digital.nhs.uk/catalogue/PUB17137 (accessed January 2017).
Pitts N, Harker R . Obvious decay experience: Children's Dental Health in the United Kingdom 2003. London: Office for National Statistics, 2005.
Bagramian R A, Garcia-Godoy F, Volpe A R . The global increase in dental caries. A pending public health crisis. Am J Dent 2009; 22: 3–8.
Duggal M S, van Loveren C . Dental considerations for dietary counselling. Int Dent J 2001; 51: 408–412.
Moynihan P J . Dietary advice in dental practice. Br Dent J 2002; 193: 563–568.
Public Health England. SACN Carbohydrates and Health. 2015. Available at https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/445503/SACN_Carbohydrates_and_Health.pdf (accessed January 2017).
Public Health England. The Eatwell Guide: Helping you eat a healthy, balanced diet. 2016. Available at: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/551502/Eatwell_Guide_booklet.pdf (accessed January 2017).
Anderson C A, Curzon M E, Van Loveren C, Tatsi C, Duggal M S . Sucrose and dental caries: a review of the evidence. Obes Rev 2009; 10 Suppl 1: 41–54.
Tickle M, Blinkhorn A S, Milsom K M . The occurrence of dental pain and extractions over a 3year period in a cohort of children aged 3–6 years. J Public Health Dent 2008; 68: 63–69.
Kanaffa-Kilijanska U, Kaczmarek U, Kilijanska B, Frydecka D . Oral health condition and hygiene habits among adult patients with respect to their level of dental anxiety. Oral Health Prev Dent 2014; 12: 233–239.
Casamassimo P S, Thikkurissy S, Edelstein B L, Maiorini E . Beyond the dmft: the human and economic cost of early childhood caries. J Am Dent Assoc 2009; 140: 650–657.
Ofcom. Television advertising of food and drink products to children: Final statement. 22 February 2007. Available at: http://stakeholders.ofcom.org.uk/consultations/foodads_new/statement 2007 (accessed January 2017).
Ofcom. Changes in the nature and balance of television food advertising to children: A review of HFSS advertising restrictions. 17 December 2008. Available at: https://www.ofcom.org.uk/__data/assets/pdf_file/0028/23977/hfssdec08.pdf (accessed January 2017).
Adams J, Tyrrell R, Adamson A J, White M . Effect of restrictions on television food advertising to children on exposure to advertisements for 'less healthy' foods: Repeat cross-sectional study. PLoS One 2012; 7: e31578.
Ofcom. The communications market 2015: Television and audio-visual. 2015. Available at: https://www.ofcom.org.uk/__data/assets/pdf_file/0024/13974/uk_2.pdf (accessed January 2017).
Broadcasters Audience Research Bureau. Available from: http://www.barb.co.uk/whats-new/weeklytop30.
Ofcom. Children and parents: Media use and attitudes report 2012. 5 February 2015. Available at: https://www.ofcom.org.uk/research-and-data/media-literacy-research/children/october-2012 (accessed January 2017).
Ofcom (2012). Children's TV viewing: BARB analysis.
Kelly B, Halford J C G, Boyland E J et al. Television food advertising to children: a global perspective. Am J Public Health 2010; 100: 1730–1736.
Gantz W, Schwartz N, Angelini J R, Rideout V . Food for thought: Television food advertising to children in the United States: The Kaiser Family Foundation, 2007.
Ofcom. Childhood obesity: Food advertising in context. https://www.ofcom.org.uk/research-and-data/tv-radio-and-on-demand/tv-research/food-ads (accessed January 2017).
Department of Health. Guide to creating a front of pack (FoP) nutritional label for pre-packed products sold through retail outlets. 2013. Available at https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/566251/FoP_Nutrition_labelling_UK_guidance.pdf (accessed January 2017).
Hieke S, Wilczynski P . Colour Me In-an empirical study on consumer responses to the traffic light signposting system in nutrition labelling. Public Health Nutr 2012; 15: 773–782.
Nizel E, Papas S . Nutrition in clinical dentistry. 3rd ed. Philadelphia: WB Saunders Company, 1989.
Advertising Standards Authority. Compliance report: Food and soft drink advertising survey 2011.
Acknowledgements
This study formed part of Mrs Muneera Al-Mazyad's DDSc dissertation at the University of Liverpool, Orthodontic Department, who hereby acknowledge the support of the Ministry of Health in Kuwait.
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed Paper
Rights and permissions
About this article

Cite this article
Al-Mazyad, M., Flannigan, N., Burnside, G. et al. Food advertisements on UK television popular with children: a content analysis in relation to dental health. Br Dent J 222, 171–176 (2017). https://doi.org/10.1038/sj.bdj.2017.120
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.2017.120
This article is cited by
-
Impact of soft drinks to health and economy: a critical review
European Archives of Paediatric Dentistry (2020)
-
A content analysis of Australian television advertising: focus on child and adolescent oral health
BMC Pediatrics (2018)
-
Child dental health: Bombarded children
British Dental Journal (2017)
-
Are children's eyes bigger than their stomachs?
British Dental Journal (2017)
