
Key Points
-
Investigates the current level of dental implant education in relation to General Dental Council and Association of Dental Education Europe requirements.
-
Reports some interesting opinions relating to the current implant education.
-
Identifies the barriers in the provision of dental implants in general dental practice.
-
Makes recommendations for the implementation of a holistic approach in undergraduate dental implant education.
Abstract
Objective The aim of this study was to understand the opinion of general dental practitioners about the current level of implant education at both undergraduate and postgraduate levels.
Materials and methods A questionnaire was sent to the general dental practitioners working in a group of practices in the West Midlands, UK. The completed responses were analysed.
Results Ninety-one out of 101 dentists responded to the questionnaires (95.6%). Sixty-seven (77%) dentists stated that they learnt only theoretical aspects of dental implants during their undergraduate training. The majority of them stated that the training they received was not adequate. In addition, few barriers in dental implant provision by general dentists were also identified in the survey. The main barriers were risk of failures (56.3%), to avoid complications (65.5%) and the cost of learning (51.7%). The results were correlated to the implant competences set by the regulatory organisations such as General Dental Council and Association of Dental Education Europe.
Conclusion The present study confirmed that the current implant education at both undergraduate and postgraduate levels in the UK does not instil confidence to the GDPs to provide and maintain dental implants.
Similar content being viewed by others

Introduction
The adult dental health survey 2009, reported a 6% decrease in the average number of edentate adults in England compared to the previous surveys.1,2,3 Similar statistics of increased tooth retention have been reported in other Western countries.4,5 In addition, patient expectations have also increased with respect to aesthetics and function. Therefore, advanced treatment planning including implants has become inevitable in modern dentistry.6 Such treatment planning challenges the general dental practitioner who has not necessarily received specialist training to deal with implant restored mouths. The need to maintain or intervene in the maintenance of implants is increasing even if the practitioner does not place or restore implants themselves. Hence, implant education that is tailored to the range of cases that a non-specialist is likely to encounter is required at both undergraduate and postgraduate levels.
The General Dental Council's (GDC) document Preparing for practice – dental team learning outcomes for registration expects the registered dentist to recognise and explain to patients the range of implant treatment options, their impact outcomes, limitations and risks. It also mandates the dentist to describe the risks related to dental implant therapy and manage the health of peri-implant tissues.7 However, the GDC limits the UK qualified dentist from practicing implant dentistry without undertaking structured postgraduate training and assessment of competence, which relates to the Training standards in implant dentistry published by the Faculty of General Dental Practitioners.8,9
The Association of Dental Education in Europe (ADEE) is an independent European organisation, which contributes to implant education by organising periodic the European Consensus workshops. The outcomes of the workshop in 2008 were the Profile and competences statement for the European Dentist and the Competencies and learning outcome in implant education documents. The first document recommends a competent dentist to be familiar with the diagnosis for potential implant patients, communicating to patients about the risks, benefits and long term consequences of using implants within an overall treatment concept, and the principles and techniques involved.10 The second set of documents set out the competences and learning outcomes for teaching in implant dentistry in undergraduate, postgraduate and CPD courses.11,12
The 2nd consensus workshop report confirmed the integration of implant dentistry in undergraduate education in European institutions.13 However, the education delivery is variable in terms of the amount of information provided, the level of training and whether the course is purely theory or contains any hands on clinical component.14 The report also identified the challenges in developing strategies and in implementing the existing competence profiles. It also considered the challenge of how much should be delivered at undergraduate level. Whilst at the post graduate level, there are many implant training courses available, there is once again a great variation in the quality of training and duration of these courses as they may range from one day workshops to degree level qualifications.15,16
Surveys on dental implant education are limited and those published have focused on specific areas. For example, two surveys recorded the responses from dentists who attended the continuing dental education in dental implants.17,18 In these surveys, the respondents were mainly established private practitioners. They considered that attending those courses made them aware of their own limitations and the majority of them thought there should be a dental implantology speciality.
The present literature and guidelines indicate that more information is required on how general dentists encounter implants in their everyday practice to assess whether they are meeting the learning outcomes or competencies highlighted in the previous documents.
Aims
The aim of this study is to evaluate the current level of implant experience; barriers in implant provision and opinion of general dental practitioners working predominantly within the NHS in the UK.
Materials and methods
A structured paper based questionnaire was developed to collect information about the participant's background, implant education and experience including their opinion about current implant education. The questionnaire included closed and open ended questions to facilitate quicker response and to allow comments and reflections at strategic points respectively. The survey was refined after a pilot response to the questionnaire from five dentists. The study was conducted complying with the University of Birmingham Ethics committee guidelines. The questionnaire was distributed to general dental practitioners working within a representative group of practices in the West Midlands, UK. The chosen group of practices have spread all over the west midlands with a mixture of dentists from different Institutional backgrounds. The dentists who participated in the study were 26 local graduates, 11 from the London area, and at least two were representing each university in the UK. This formed the majority of the study group. The remaining were from European countries such as Portugal, Germany, and non-EU countries such as India and Pakistan. The response to the questionnaire was maximised by delivering to the practitioners in a range of formats including email, regular post, internal post arrangement within the group of practices and a few were hand delivered where necessary. The dentists were encouraged to provide responses using different modes such as regular post, email attachments, 'whatsapp' and multimedia messages. This was to facilitate the response rate. The digital data transmission, especially through whatsapp, has been reported and recommended in the medical field.19
Results
The questionnaire was initially emailed to 101 clinicians. Nine of the respondents were found to be hygienists or therapists and were excluded for the purposes of this study. One dentist had left the practice group at the time when the questionnaire was sent. This reduced the number of dentists to 91. Out of this, 87 dentists responded to the questionnaire. This gave a response rate of 95.6%.
The age categorisation and year of graduation are shown in Tables 1 and 2 respectively. The majority of the respondents were aged 40 and under (79.3%), and over half of them graduated after 1990 (66.7%).
Seventy-six (87.4%) of the total respondents were predominantly NHS practitioners (Table 3), and nearly 90% of them did not provide implant treatment (Table 4). Nine percent of the dentists limited themselves to simple implant treatments such as single implants or small bridges.
Sixty-seven (77%) stated that they learnt about the theoretical concepts of fixed implants and implant supported overdentures during their undergraduate training (Table 5). However, they stated that there was no practical or clinical component provided.
Further training
The group consisted of general dentists of varied experience, including two dentists enrolled on a university-based MSc in implant dentistry, three orthodontists, two dentists holding qualifications in periodontics and two in prosthodontics. In addition, two dentists had completed a one-year certificate in implant dentistry.
Forty two (48.3%) dentists did not have any postgraduate training in dental implants (Table 6). The remaining 52.7% underwent postgraduate dental implant training through CPD courses including section 63 courses and vocational training study days; commercial courses within the UK or overseas courses. An example of the overseas country providing implant courses was Egypt. These trainings ranged from a one day workshop to a ten day course. The certificate courses extended up to 12 months, some including treatment of candidates' own patients in the training clinic at a subsidised cost. The treatment cost was in turn added to the dentist's course fee.
Recall and maintenance protocol
Those dentists who provided implants reported on a range of recall intervals including monthly, three monthly, six monthly and annually. However, there was no strict protocol mentioned for the care of implant restorations. The dentists who provide implants reported that they regularly maintain their patients. Two dentists who do not provide implants suggested the recall and maintenance should be undertaken by hygienists. Only two of the respondents considered that it was the responsibility of the referring dentist to maintain implant restored mouths, if the patient had originally been sent to a specialist for implant provision.
Barriers in provision of implants
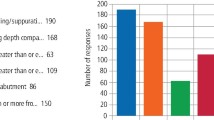
The main barriers reported to their own personal clinical placement of implants were risk of failures (56.3%), to avoid complications (65.5%) and the cost of learning (51.7%). The next level was the cost of treatment (36.8%). The maintenance aspect was not considered a major issue (15%) (Table 7).
The other barriers mentioned by the respondents were; the indemnity to cover dental implant treatment which is higher than their regular fee, with chances of increase in cost and conditions if a situation of compensation arises;20 interest in the other fields of dentistry; and family commitments.
Opinion about current undergraduate implant training
The general opinion was that the level of current undergraduate dental implant training is poor or inadequate. It was stated that further training is expensive and not available to everyone. Therefore the dentists who completed the questionnaire suggested that implant training should be part of the undergraduate curriculum and that it should be substantial to include a practical/hands-on aspect. At least one dentist has recommended shortening the teaching of other aspects to include implants in the curriculum. Two of the senior dentists recommended that dentists should only perform such treatment by following recognised specialist training.
Discussion
The study group involved dentists working in a large independent group of practices in the West Midlands. This is not a corporate chain and do not operate in the same way as a corporate. They have standard policies for the group, such as infection control and radiation protection. However, the policies related to specific treatments such as implants are tailored to the individual practice depending on how the dentists wish to work. Therefore, the results of the study are the opinion of the dentists, which is not influenced by the employment situation.
The majority of the dentists were associates, aged less than 40 years and graduated after 1990 providing predominantly NHS dentistry. The number of dentists involved in the survey may appear small; however, it does provide us with an insight into the opinions of younger general dental practitioners whose postgraduate training will influence the future of dentistry provision in the UK.
Only a few dentists in the group provided implant treatment. In contrast to the results of a previous survey conducted in 2006,18 the majority of the GDPs did learn implantology as an undergraduate. However, the education received was mainly theoretical teaching and learning which reveals the relative shortcomings in implant education. Many have had some form of postgraduate training through section 63, CPD courses which has raised their interest in learning about the use of dental implants.
With respect to implant dentistry in the UK, the General Dental Council recommends the dentist to communicate the risks and benefits of implants to the patients and to manage the health of peri-implant tissues.7 The number of patients presenting with peri-implant disease is also increasing.21,22 This can be a major factor in NHS that will take up the specialist time and funding. This will in turn limit the number of new implant placements.23 Therefore, the responsibility for the subsequent care and maintenance of the implant patient should be clearly defined and shared between the operator who places the implant and the clinician who maintains the overall dental health of the patient. However, in the current study, the majority considered that maintenance was the responsibility of the specialist dentist who provided the implant restoration.
In addition, there is no published guidance on how dental implant recalls should be structured. This is an area which needs further exploration.
As per the GDC and ADEE recommendations, the majority of the dentists are aware of their responsibility in educating patients and providing options of implants to patients. The opinion of the dentists participated in the survey has confirmed that the current implant training is deficient. Therefore, it is doubtful that they will be able to address the implant need for the appropriate patient, referral at a suitable stage and provide ongoing maintenance. The response about the current barriers indicates that their present implant education does not instil confidence in them. However, a direct question regarding the confidence in providing dental implant treatment was avoided to eliminate the Dunning–Kruger effect. This is a cognitive bias wherein the unskilled people mistakenly assess their ability to be much higher than is accurate.24 The dentists may assume that they are confident, but they may not be competent. The majority of the GDPs considered medical litigation as a major barrier in providing implants. This may also be related to their reluctance to be involved with the maintenance of the implants. The next major barrier was the cost of learning. Dental implant training is expensive as it involves high consumables and surgical costs. This may be a factor to consider, especially in the UK undergraduate programmes as they are state funded. This may not affect the other countries as the system is not common across the whole EU.
Investigation of implant education in Europe, five years after the first implant competency document was published showed that the volume of teaching implants is expanding, in line with the demand and regulations.25 The response to the present questionnaire also reflected this view. The majority stated that implant treatment can be provided in general practice with appropriate training. This was in contrast to the 2006 survey,18 where the majority of the respondents recommended a speciality pathway for dental implantology.
Current implant education and clinical training should be aligned to the competences and learning outcomes published by the GDC and ADEE. However the future provision of implant education at the undergraduate level requires much thought. The main problem addressed at the first ADEE consensus was to find a space in the already crowded curriculum. Several European Institutions have managed to overcome this issue which is partly related to other factors including different remuneration systems.22 In the UK, it may be the time to consider a holistic approach. This will make dental implant education a shared responsibility between prosthodontic, surgical and periodontic disciplines. However, more research may be needed to identify the amount and nature of information and training to be provided to the undergraduate student.
Conclusion
General dental practitioners in the UK and Europe are expected to attain specific competencies and fulfil learning outcomes in relation to dental implants. However, the results of the present study confirmed that the current implant education in the UK does not instil confidence to the GDPs to provide and maintain dental implants. Few barriers in implant provision have also been identified. Further research may be needed to explore the needs in relation to dental implant education.
References
Patel P, Lynch C D, Sloan A J, Gilmour A S M . Treatment planning for replacing missing teeth in UK general dental practice: current trends. J Oral Rehabil 2010; 37: 509–517.
Fuller E, Steele J, Watt R, Nuttall N . Oral health and function – a report from the Adult Dental Health Survey 2009. 2011. Online information available at http://www.dhsspsni.gov.uk/theme1_oralhealthandfunction.pdf (accessed June 2015).
Steele J, Treasure E, L F, Morgan M . Complexity and maintenance - a report from the Adult Dental Health Survey 2009. 2011. Online information available at http://www.hscic.gov.uk/catalogue/PUB01086/adul-dent-heal-surv-summ-them-the4-2009-rep6.pdf (accessed June 2015).
Whelton H, Crowley E, O'Mullane D, Woods N, McGrath C, Kelleher V . Oral Health of Irish Adults 2000–2002. Dublin: Department of Health and Children, 2007. Online information available at http://health.gov.ie/wp-content/uploads/2014/03/oral_health02.pdf (accessed June 2015).
Douglass C W, Jette A M, Fox C H et al. Oral health status of the elderly in New England. J Gerontol 1993; 48: M39–46.
Lang N P, DeBruyn H . The rationale for the introduction of implant dentistry into the dental curriculum. Eur J Dent Educ 2009; 13: 19–23.
General Dental Council. Preparing for practice - dental team learning outcomes for registration. 2012. Online information available at http://www.gdc-uk.org/Newsandpublications/Publications/Publications/GDC%20Learning%20Outcomes.pdf (accessed June 2015).
General Dental Council. Implantology - policy statement. Online information available at http://www.gdc-uk.org/Dentalprofessionals/Standards/Pages/Implantology.aspx (accessed June 2015).
Faculty of General Dental Practice. Training standards in implant dentistry. 2012. Online information available at http://www.fgdp.org.uk/_assets/pdf/publications/policy%20documents/implant%20training%20stds%20jun%2012.pdf (accessed June 2015).
Cowpe J, Plasschaert A, Harzer W, Vinkka-Puhakka H, Walmsley A D . Profile and competences for the graduating European dentist - update 2009. Eur J Dent Educ 2010; 14: 193–202.
Sanz M, Saphira L . Competencies in implant therapy for the dental graduate: appropriate educational methods. Eur J Dent Educ 2009; 13(Suppl 1): 37–43.
Donos N, Mardas N, Buser D . An outline of competencies and the appropriate postgraduate educational pathways in implant dentistry. Eur J Dent Educ 2009; 13(Suppl 1): 45–54.
Koole S, H D. Contemporary undergraduate implant dentistry education: a systematic review. Eur J Dent Educ 2014; 18(Suppl 1): 11–23.
Blum I R, O'Sullivan D J, Jagger D . A survey of undergraduate education in dental implantology in UK dental schools. Eur J Dent Educ 2008; 12: 204–207.
Addy L D, Lynch C D, Locke M, Watts A, Gilmour A S . The teaching of implant dentistry in undergraduate dental schools in the United Kingdom and Ireland. Br Dent J 2008; 205: 609–614.
Ivanovski S, Mattheos N, Scholz S, Heitz-Mayfield L . University postgraduate training in implant dentistry for the general dental practitioner. Aust Dent J 2010; 55: 339–345.
Brandt R L, Fitzpatrick B J, Moloney F B, Bartold P . Continuing dental education in osseointegrated implants. A survey. Aust Dent J 2000; 45: 285–288.
Gibson R L, Barclay C . Dental implantology education: a survey of opinion and experience of 106 general dental practitioners. Br Dent J 2006; 201: 367–370.
Giordano V, Koch H A, Mendes C H, Bergamin A, de Souza FS, do Amaral NP . WhatsApp messenger is useful and reproducible in the assessment of tibial plateau fractures: Interand intra-observer agreement study. Int J Med Inform 2015; 84: 141–148.
Young M, Carter D, Sloan P, Quayle A A . Oral implantology teaching: a survey of oral implantology teaching in the university dental hospitals and schools of the United Kingdom and Eire. Br Dent J 1999; 187: 671–676.
Lindhe J, Meyle J, Group D of European Workshop on Periodontology. Peri-implant diseases: consensus report of the sixth European workshop on periodontology. J Clin Periodontol 2008; 35: 282–285.
Lang N P, Berglundh T, Working Group 4 of the Seventh European Workshop on Periodontology. Peri-implant diseases: where are we now? Consensus of the Seventh European Workshop on Periodontology. J Clin Periodontol 2011; 38: 178–181.
Butterworth C, Baxter A, Shaw M, Bradnock G . Implants: the provision of dental implants in the National Health Service hospital dental services - a national questionnaire. Br Dent J 2001; 190: 93–96.
Kruger J, Dunning D . Unskilled and unaware of it: how difficulties in recognising one's own incompetence lead to inflated self-assessments. J Pers Soc Psychol 1999; 77: 1121–1134.
Koole S, De Bruyn H, Vandeweghe S, Mattheos N . Implant dentistry education in Europe: 5 years after the Association for Dental Education in Europe consensus report. Eur J Dent Educ 2014; 18: 43–51.
Acknowledgements
The authors would like to thank the managers of Bhandal Dental Practices for their assistance in distributing questionnaires and collecting responses.
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed Paper
Rights and permissions
About this article

Cite this article
Jayachandran, S., Bhandal, B., Hill, K. et al. Maintaining dental implants – do general dental practitioners have the necessary knowledge?. Br Dent J 219, 25–28 (2015). https://doi.org/10.1038/sj.bdj.2015.528
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.2015.528
This article is cited by
-
The referral pattern and treatment modality for peri-implant disease between periodontists and non-periodontist dentists
BMC Oral Health (2023)
-
What every dental practitioner should know about how to examine patients with dental implants
British Dental Journal (2023)
