
Abstract
Objectives:
The aim of this study was to evaluate the effect of walking with isocentric reciprocating gait orthoses (IRGOs) utilizing two designs of ankle foot orthoses (AFOs) on specific outcome measures in people with spinal cord injury (SCI).
Methods:
Four volunteer SCI subjects participated in this study, and were fitted with an IRGO equipped with either solid or dorsiflexion-assisted AFOs in a randomized order. Subjects walked at their self-selected speed along a flat walkway to enable a comparison of walking speed, endurance and the resulting physiological cost index (PCI) to be performed.
Results:
Increased walking speed, increased distance walked and less PCI were demonstrated in walking with the IRGO incorporating dorsiflexion-assisted AFOs as compared to walking with an IRGO plus solid AFO as a control condition.
Conclusion:
This study demonstrated that people with SCI could walk at relatively higher speeds and with greater endurance and a reduced PCI when utilizing an IRGO with dorsiflexion-assisted AFO components compared to solid ones. It is therefore concluded that the IRGO incorporating dorsiflexion-assisted AFOs may be an effective alternative in helping to reduce the energy consumption experienced by people with SCI.
Similar content being viewed by others


Introduction
Various types of mechanical orthoses are available for orthotic gait training by spinal cord injury (SCI) patients. These include the advanced reciprocating gait orthosis (ARGO), the isocentric reciprocating gait orthosis (IRGO), the Louisiana State University reciprocating gait orthosis (LSU-RGO), and medial linkage orthosis designs such as the Walkabout and Primewalk orthoses. In addition, devices such as conventional hip knee ankle foot orthoses (HKAFOs) and the hip guidance orthosis are also available.1,2
The high rate of energy consumption experienced when ambulating has been reported as one limiting factor during gait training with such orthoses by people with SCI.3 Attempts have been made to solve this problem using powered gait orthosis and hybrid orthosis, but this has not yet been achieved,4 meaning orthotic use is often rejected—mainly due to exhaustion.5,6 The evidence available in the literature has demonstrated that energy consumption is reported to be less in IRGOs than when wearing HKAFOs or other types of reciprocating gait orthoses (RGOs); but RGOs, like other mechanical orthoses, cannot be a totally appropriate replacement for wheelchairs in people with SCI.1
The ankle joint plays a critical role in facilitating forward propulsion during walking by moving the center of mass forward during push-off, with the ankle plantarflexor muscles performing a pivotal role during this phase.7,8 The ankle dorsiflexors also decrease energy loss at heel strike by positioning the ankle effectively prior to ground contact.9,10,11 From a physiological viewpoint, the afferent feedback from the ankle joint has important effects on the control of walking and changes to the motor output of spinal motor neurons by rhythmic limb loading.12,13 As a result, provision of ankle motion during ambulation with RGOs in paraplegic patients may also be important.
IRGO was developed in 1992, by Motlock, by replacing the cable connecting the hip joints with a low-friction rocker bar link. The IRGO produced higher walking speeds and increased walking distance compared to other mechanical orthoses (for example, other types of RGO, the walkabout orthosis and hip-knee-ankle-foot-orthosis).1 IRGOs and ARGOs are two types of RGO designs that are used in orthotic gait training by SCI patients,14 but they routinely use solid ankle foot orthoses (AFOs) in their design, which means that the ankles are immobilized. When using a dorsiflexion-assisted AFO components within an ARGO, Bani et al.15 demonstrated that the mean walking speed, stride length, and ankle and hip joint ranges of motion were all significantly increased along with cadence by a group of paraplegic volunteers compared to when walking using an ARGO with solid AFOs. Genda et al.16 developed the hip ankle-linked orthosis and reported that step lengths and pelvic rotation were more normal when using hip ankle-linked orthosis compared to the prime walk orthosis in a single SCI subject. Kawashima et al.17 developed a new powered weight-bearing control orthosis for walking by SCI patients. The foot section of this orthosis provided powered foot clearance to facilitate ambulation. Analysis of this orthosis in paraplegic patients demonstrated increased speed of walking and less energy consumption compared to previous studies performed in this field.
Previous studies have therefore demonstrated that ankle joint mobility can have a positive effect on improving gait parameters when SCI patients walk with the aid of mechanical orthoses. The use of reciprocal gait orthoses (RGOs) when utilizing dorsiflexion-assisted AFOs to walk has a potential to decrease the energy consumption based on increased endurance compared with those with solid AFOs.18 However, the effect of ankle joint mobility on energy consumption is not clear in SCI patients. Based on the important role of the ankle joint during walking and improvement of walking parameters via movable ankle joints in using mechanical orthosis, we hypothesized that ankle joint mobility would have a positive effect on reducing energy consumption during walking with an IRGO. Therefore the aim of this study was to evaluate the effect of an IRGO utilizing bilateral solid AFOs versus the same orthosis fitted with AFOs offering a dorsiflexion- assist function on energy consumption in a group of people with SCI.
Materials and methods
Subjects
Four SCI patients participated in this study. All subjects had thoracic-level injury, either grade A or B, according to the American Spinal Injury Association Score.19 Table 1 shows the demographics of subjects who volunteered for this pilot study. Inclusion criteria included no evidence of cardiovascular problems, spasticity, contracture, obesity or asymmetry in hip joint positions in the sagittal plane and all participants were required to be at least 6 months post-injury to allow psychological improvement to occur prior to being enrolled in the study. Informed consent was obtained from volunteer patients prior to being included in the study, and the Human Ethics Committee of the University of Social Welfare and Rehabilitation Sciences gave approval to perform the study.
Orthotic intervention
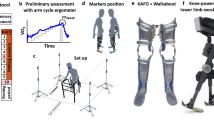
The IRGO consisted of two knee AFOs, which were connected together with a pelvic band and superstructure with bilateral hip joints connected together via a rocker-type reciprocal link. The function of the reciprocal link is to provide flexion of the orthotic hip joint on one side with simultaneous extension of the contralateral hip joint. In this study, the AFOs incorporated in the IRGO were custom molded using plaster of Paris casts of the lower limbs for each volunteer subject, and the superstructure adjusted and adapted to fit each patient. In the IRGO, as control orthosis the AFO section had solid ankle joint without movement. In the IRGO with a dorsiflexion-assisted AFO function, the AFOs incorporated dorsiflexion-assisted ankle joints.20 The overall view of the dorsifexion-assisted ankle joint is shown in Figure 1. When the ankle joint rotates into plantar flexion, a stirrup compresses the spring and the assist device generates the assist moment proportional to the plantar flexion angle. When the ankle joint rotates into dorsiflexion, it rotates freely because a spring in the ankle joint can move with little friction in dorsiflexion direction. Knee joints in two orthosis were of the drop locked type. All patients walked without shoes. A one- inch heel lift with a nonslip finish was added to the heel area of all the AFOs to replicate the pitch of a shoe with a 1-inch heel.

IRGO overall view and dorsiflexion-assisted ankle joints used in this study.
Orthotic gait training
Based on the level of injury all subjects received between 6 and 8 weeks of experience in gait training with two type of interventions prior to gait analysis. This comprised of five 2-h sessions per week with the orthosis. The orthotic gait training program consisted of donning and doffing of the orthoses, passive stretching of the lower extremities, upper-limb strengthening, balancing in a standing position and walking training on regular flat surfaces. All gait training was done by an expert physiotherapist experienced in training paraplegic patients in walking and standing. Orthotic gait training with the orthosis was completed prior to performing the trials for this study to ensure that each SCI subject could walk with the IRGO and the IRGO plus dorsiflexion-assisted AFO independently without falling when walking with the aid of a walking frame.
Experimental approach
To provide information to evaluate physiological cost index (PCI), a polar heart rate monitor was used.21,22 To calculate the PCI using this approach, the heart rate at steady-state walking and the heart rate at rest were measured. The following formula was used to measure the PCI:
To obtain a baseline level of PCI, subjects sat for 10 min prior to any measurement.23–25 The approach of PCI measurement consisted of 5 min complete rest in sitting position, 5 min in standing position, walking with the orthosis for 6 min at their self-selected walking speed and a final 2 min of rest in the seated position. During resting, standing and walking, the heart rate was calculated every 15 s. After 10 min of rest in the sitting position with the alternative test condition donned, the next evaluation and measurement was started. The mean heart rate during the final 2 min of rest in the sitting position was considered as heart rate at rest and average heart rate after 6 min of walking with the orthosis was considered as the heart rate at steady state.
Subjects were asked to walk using the two types of orthosis condition in a randomized order, along a pre-determined 40 m rectangular walkway at their self-selected speed. To calculate the velocity the interval between the starting and stopping time was used. Velocity (V) was calculated by dividing the walking distance (measured by Six-Minutes Walking Test (6MWT)) by time. Walking speed was measured via time by a stopwatch and distance walked was measured using a meter. The positive and negative accelerations at the start and finish plus that utilized during turns was not included. Three trials were used for each condition and subject. The two test conditions were randomly selected (A=wearing IRGO plus to solid AFO, B=wearing IRGO plus dorsiflexion-assisted AFO) to evaluate the effect of ankle joint mobility on speed, distance of walking and PCI when either walking with an IRGO with solid AFO as a control condition, or walking with IRGO with AFO-associated dorsiflexion assist. Figure 1 shows the IRGO and the AFO with dorsiflexion-assisted design used in this study.
Results
Table 2 demonstrates the mean±s.d. of PCI, speed of walking, distance walked, heart rate at steady speed and heart rate at rest during the two test conditions. Increased walking speed, increased distance walked and less PCI were demonstrated in walking with the IRGO incorporating dorsiflexion-assisted AFOs as compared to walking with an IRGO plus solid AFO as a control condition (Table 2).
Discussion
The aim of this present study was to evaluate ankle joint mobility on energy consumption during walking in people with SCI when using a mechanical orthosis. The results of this study demonstrated that using dorsiflexion-assisted AFOs in an IRGO increased the walking speed, walking distance and decreased PCI.
In this study, the results of the PCI measurement demonstrated that SCI patients walked faster and more efficiently using the IRGO with dorsiflexion-assisted AFOs compared to the IRGO with solid AFOs. In addition, the performance of these subjects may further improve when they have more orthotic gait training. The level of injury, duration of orthoses use, gait velocity and the type of orthosis used can affect energy consumption during orthotic walking in people with SCI.14 From an orthotic point of view, hybrid and powered orthosis designs could be an effective alternative in reducing energy consumption for people with SCI to help provide their optimum walking function. According to our knowledge, this study is the first one to analyze energy consumption in an IRGO when comparing two AFO designs.
Ankle joint ranges of motion are 10° of dorsiflexion during mid-stance and 20° of plantar flexion in the pre-swing phase during normal walking.26 Any condition that influences ankle joint ROM can cause a reduction of gait efficiency. The mean speed of walking in subjects with ankle arthrodesis has been reported as 1.12 m s−1 (67 m min−1), which is 84% of the normal walking speed.27 The average person with an ankle fusion uses a 3% greater rate of energy consumption than for a normal subject when walking at the same speed, and gait efficiency for such patients has been shown to average only 90%.28 Using a short leg walking cast and the prefabricated lower leg orthosis has been shown to require significantly more energy in comparison with normal walking in normal able-bodied subjects. Walking with these conditions also provided short step length and therefore reduction of speed of walking.29 Also, in using a AFO, Arazpour et al. demonstrated that using an ARGO with dorsiflexion-assisted AFOs increased the fear of falling, but did improve static postural stability and increased walking speed and endurance.18 Increase of temporal spatial parameters and improvement of hip joint kinematic was reported by Bani et al.15 via using an ARGO with dorsiflexion-assisted AFOs compared to ARGO with solid AFO.
The walking speed demonstrated by people with SCI when using mechanical orthoses is one-third of that demonstrated by able-bodied subjects during normal ambulation.1 Walking with dorsiflexion-assisted AFOs had a positive effect in improving this parameter compared to solid AFOs in walking with the IRGO in this study. The ankle joint plays an important role in providing propulsion. The provision of movable ankle joints within mechanical reciprocal orthoses appears to facilitate more efficient ambulation.
When using a powered foot section in the weight-bearing control orthosis, Kawashima et al.17 reported the mean of speed of walking was 19 m min−1. Genda et al.16 in the development of an orthosis using movable orthotic ankle joints and a hip and ankle linkage system when compared to the prime walk orthosis reported a mean walking speed of 36 m min−1 compared to walking with prime walk. When utilizing dorsiflexion-assisted AFOs within an ARGO compared to solid AFOs, Bani et al.15 demonstrated that using the movable ankle joints caused increased walking speed.
The small sample size is a limitation of this present study. Evaluation of IRGOs incorporating AFOs with a dorsiflexion-assisted function was done to determine the energy consumption in this study, but this study did not evaluate the alterations to compensatory motions or the loads applied to the upper limb joints; these also need to be evaluated in a future study. As powered orthosis have shown encouraging results in improving the rate of energy consumption compared to other mechanical orthoses (HKAFO and IRGO),22 a comparison between powered orthosis and the IRGO with dorsiflexion-assisted AFOs will be beneficial in this field. The use of orthotic devices mainly depended on their acceptance by the users, while the participants were not evaluated subjectively in walking with two types of orthoses. This point is another main limitation of this present study.
Conclusion
In this study, the PCI walking speed and distance walked were investigated during orthotic walking with an IRGO incorporating dorsiflexion-assisted AFOs, and it was demonstrated that people with SCI could walk at a relatively higher mean speed and less PCI compared with an IRGO with solid AFOs. It is therefore concluded that the IRGO incorporating dorsiflexion-assisted AFOs could be an effective alternative to help reduce energy consumption in people with SCI. In further analyses, both clinical and physiological evaluation will be required to clarify the influences of orthotic gait for people with SCI.
References
Arazpour M, Bani MA, Hutchins SW . Reciprocal gait orthoses and powered gait orthoses for walking by spinal cord injury patients. Prosthet Orthot Int 2013; 37: 14–21.
Ahmadi Bani M, Arazpour M, Farahmand F, Mousavi ME, Hutchins SW . The efficiency of mechanical orthoses in affecting parameters associated with daily living in spinal cord injury patients: a literature review. Disab Rehab Assist Technol 2015; 10: 183–190.
Arazpour M, Bani MA, Kashani RV, Ghomshe FT, Mousavi ME, Hutchins SW . Effect of powered gait orthosis on walking in individuals with paraplegia. Prosthet Orthot Int 2013; 37: 261–267.
Arazpour M, Chitsazan A, Hutchins SW, Ghomshe FT, Mousavi ME, Takamjani EE et al. Design and simulation of a new powered gait orthosis for paraplegic patients. Prosthet Orthot Int 2012; 36: 125–130.
Arazpour M, Chitsazan A, Hutchins SW, Ghomshe FT, Mousavi ME, Takamjani EE et al. Evaluation of a novel powered hip orthosis for walking by a spinal cord injury patient: a single case study. Prosthet Orthot Int 2012; 36: 105–112.
Arazpour M, Chitsazan A, Hutchins SW, Mousavi ME, Takamjani EE, Ghomshe FT et al. Evaluation of a novel powered gait orthosis for walking by a spinal cord injury patient. Prosthet Orthot Int 2012; 36: 239–246.
Meinders M, Gitter A, Czerniecki J . The role of ankle plantar flexor muscle work during walking. Scand J Rehab Med 1998; 30: 39–46.
Kuo AD, Donelan JM, Ruina A . Energetic consequences of walking like an inverted pendulum: step-to-step transitions. Exerc Sport Sci Rev 2005; 33: 88–97.
Neptune RR, Kautz S, Zajac F . Contributions of the individual ankle plantar flexors to support, forward progression and swing initiation during walking. J Biomech 2001; 34: 1387–1398.
Gottschall JS, Kram R . Energy cost and muscular activity required for propulsion during walking. J Appl Physiol 2003; 94: 1766–1772.
Donelan JM, Kram R, Kuo AD . Mechanical work for step-to-step transitions is a major determinant of the metabolic cost of human walking. J Exp Biol 2002; 205: 3717–3727.
Grey MJ, Mazzaro N, Nielsen JB, Sinkjær T . Ankle extensor proprioceptors contribute to the enhancement of the soleus EMG during the stance phase of human walking. Can J Physiol Pharmacol 2004; 82: 610–616.
Dietz V, Müller R, Colombo G . Locomotor activity in spinal man: significance of afferent input from joint and load receptors. Brain 2002; 125: 2626–2634.
Arazpour M, Samadian M, Bahramizadeh M, Joghtaei M, Maleki M, Bani MA et al. The efficiency of orthotic interventions on energy consumption in paraplegic patients: a literature review. Spinal Cord 2015; 53: 168–175.
Bani MA, Arazpour M, Ghomshe FT, Mousavi ME, Hutchins SW . Gait evaluation of the advanced reciprocating gait orthosis with solid versus dorsi flexion assist ankle foot orthoses in paraplegic patients. Prosthet Orthot Int 2013; 37: 161–167.
Genda E, Oota K, Suzuki Y, Koyama K, Kasahara T . A new walking orthosis for paraplegics: hip and ankle linkage system. Prosthet Orthot Int 2004; 28: 69–74.
Kawashima N, Sone Y, Nakazawa K, Akai M, Yano H . Energy expenditure during walking with weight-bearing control (WBC) orthosis in thoracic level of paraplegic patients. Spinal Cord 2003; 41: 506–510.
Arazpour M, Bani M, Hutchins S, Curran S, Javanshir M . The influence of ankle joint mobility when using an orthosis on stability in patients with spinal cord injury: a pilot study. Spinal Cord 2013; 51: 750–754.
Maynard FM, Bracken MB, Creasey G, Ditunno J, Donovan WH, Ducker TB et al. International standards for neurological and functional classification of spinal cord injury. Spinal Cord 1997; 35: 266–274.
Bani MA, Arazpour M, Ghomshe FT, Mousavi ME, Hutchins SW . Gait evaluation of the advanced reciprocating gait orthosis with solid versus dorsi flexion assist ankle foot orthoses in paraplegic patients. Prosthet Orthot Int 2012; 37: 161–167.
Leung A, Wong A, Wong E, Hutchins S . The physiological cost index of walking with an isocentric reciprocating gait orthosis among patients with T 12–L 1 spinal cord injury. Prosthet Orthot Int 2009; 33: 61–68.
Arazpour M, Bani M, Hutchins S, Jones R . The physiological cost index of walking with mechanical and powered gait orthosis in patients with spinal cord injury. Spinal Cord 2012; 51: 356–359.
Nene A, Jennings S . Physiological cost index of paraplegic locomotion using the ORLAU ParaWalker. Spinal Cord 1992; 30: 246–252.
Graham RC, Smith NM, White CM . The reliability and validity of the physiological cost index in healthy subjects while walking on 2 different tracks. Arch Phys Med Rehab 2005; 86: 2041–2046.
Bar-On Z, Nene A . Relationship between heart rate and oxygen uptake in thoracic level paraplegics. Spinal Cord 1990; 28: 87–95.
Inman VT, Ralston HJ, Todd F . Human Walking. Williams & Wilkins: Baltimore, MD, USA, 1981.
Waters R, Barnes G, Husserl T, Silver L, Liss R . Comparable energy expenditure after arthrodesis of the hip and ankle. J Bone Jt Surg 1988; 70: 1032–1037.
Waters RL, Mulroy S . The energy expenditure of normal and pathologic gait. Gait Posture 1999; 9: 207–231.
Fowler PT, Botte MJ, Mathewson JW, Speth SR, Byrne TP, Sutherland DH . Energy cost of ambulation with different methods of foot and ankle immobilization. J Orthopaed Res 1993; 11: 416–421.
Acknowledgements
We thank the Iranian National Science Foundation (INSF) for providing financial support (grant number 93002957) for this research.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Arazpour, M., Hojjati, M., Samadian, M. et al. The effect of ankle joint mobility when using an isocentric reciprocating gait orthosis (IRGO) on energy consumption in people with spinal cord injury: preliminary results. Spinal Cord Ser Cases 1, 15017 (2015). https://doi.org/10.1038/scsandc.2015.17
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/scsandc.2015.17
