
Abstract
A variety of stimuli including neurological insult may provoke primitive mesenchymal cells to differentiate into bone forming cells. Such a sequel following spinal cord injury can delay rehabilitation, enhance the spasticity and reduce the range of movement in the affected joint. It is characterised by an initial inflammatory phase followed by heterotopic bone formation. The early inflammatory lesion clinically mimics deep vein thrombosis, a developing pressure sore, infection, and tumour. An early diagnosis at a time of clinical uncertainty, before the plain radiographic features develop, has distinct advantages and therapeutic implications.
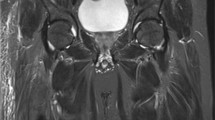
The unique pathological evolution and maturation of the lesion is clearly demonstrated by sequential sonographic (ultrasonic) assessment with depiction of the 'zone phenomena' seen on histology. Sonographic scans in 7 spinal injury patients proved diagnostic, before there was radiographic evidence of bone formation, and confidently excluded HBF in a further 18 patients without any false negative results.
Similar content being viewed by others

Article PDF
References
Riedel B (1883) Demonstration eines durch achttagiges Umhergehen total destruirten kniegelenkes von einem Patienten mit Stichverletzung des Ruckens. Verhandlungen der Deutschen Gesellschoft fur Chirurgie 12: 93.
Hardy A G, Dickson J W (1963) Pathological ossification in traumatic paraplegia. J Bone Joint Surg 45B: 76–87.
Ackerman L V (1958) Extra-osseous localized non-neoplastic bone and cartilage formation. (So-called myositis ossifications). J Bone Joint Surg 40A: 279–298.
Johnson L C (1948) Histogenesis of myositis ossificans. Am J Pathol 24: 681–682.
Buring K (1975) On the origin of cells in heterotopic bone formation. Clin Orthopaed 110: 293–302.
Stover S L, Niemann K M W, Miller J M (1976) Disodium etidronate in the prevention of post-operative recurrence of heterotopic ossification in spinal cord injury patients. J Bone J Surg 58A: 683–688.
Silver J R (1969) Heterotopic ossification. A clinical study of its possible relationship to trauma. Paraplegia 7: 220–230.
Wharton G W, Morgan T H (1970) Ankylosis in the paralyzed patient. J Bone Joint Surg 52A: 105–112.
Orzell J, Rudd T (1985) Heterotopic bone formation: Clinical, laboratory and imaging correlation. J Nucl Med 26: 125–132.
Mirra J M (1989) Bone Tumours. Vol 2. Lea & Febiger, Philadelphia: 1549–1586.
Gilmer W Anderson L (1959) Reactions of soft somatic tissue which may progress to bone formation: Circumscribed (traumatic) myositis ossificans. South Med J 52: 1432–1448.
Lagier R, Cox J N (1975) Pseudomalignant myositis ossificans. A pathological study of eight cases. Hum Pathol 6(6): 653–656.
Angervall L, Stener B, Stener I (1969) Pseudomalignant osseous tumour of soft tissue. A clinical, radiological and pathological study of five cases. J Bone Joint Surg 51B(4): 654–663.
Thomas E A, Cassar-Pullicino V N, McCall I W (1991) The role of ultrasound in the early diagnosis and management of heterotopic bone formation. Clin Radiol 43: 190–196.
Norman A, Dorfman H D (1970) Juxta-cortical circumscribed myositis ossificans: Evolution and radiographic features. Radiology 96: 301–306.
Goldman A B (1976) Myositis ossificans circumscripta: A benign lesion with a malignant differential diagnosis. Am J Radiol 126: 32–40.
Amendola M A, Glazer G, Agha F P, Francis I, Weatherbee L, Martel W (1983) Myositis ossificans circumscripta: computed tomographic diagnosis. Radiology 149: 775–779.
Freed H H, Dreisbach J N, Hahn H, Enneking W F, Springfield DS Andrew E R et al (1981) The use of the three phase bone scan in the early diagnosis of heterotopic ossification (HO) and in the evaluation of Didronel therapy. Proceedings of the Seventh Annual Scientific Meeting of the American Spinal Injury Association. March 26-30 1981, New Orleans: 63–64.
Suzuki Y, Hisada K, Takeda M (1974) Demonstration of myositis ossificans by 99mTC pyrophosphate bone scanning. Radiology 111: 663–664.
Venier L H, Ditunno J F Jr (1971) Heterotopic ossification in the paraplegic patient. Arch Phys Med Rehabil 52(10): 475–479.
Furman R, Nicholas J J, Jivoff L (1970) Elevation of the serum alkaline phosphatase coincident with ectopic-bone formation in paraplegic patients. J Bone Joint Surg 52A: 1131–1137.
Nicholas J J (1973) Ectopic bone formation in patients with spinal cord injury. Arch Phys Med 54: 354–359.
Finerman G A M, Stover S L (1981) Heterotopic ossification following hip replacement or spinal cord injury. Two clinical studies with EHDP. Metab Bone Dis Rel Res 4(5): 337–342.
Kramer K, Kurtz A, Rubin C, Goldberg B A (1979) Ultrasound appearance of myositis ossificans. Skel Radiol 4: 19–20.
Peck R J, Metreweli C (1988) Early myositis ossificans: A new echographic sign. Clin Radiol 39: 586–588.
Kirkpatrick J S, Koman L A, Rouere G D (1987) The role of ultrasound in the early diagnosis of myositis ossificans. Am J Sports Med 15: 179–181.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Cassar-Pullicino, V., McClelland, M., Badwan, D. et al. Sonographic diagnosis of heterotopic bone formation in spinal injury patients. Spinal Cord 31, 40–50 (1993). https://doi.org/10.1038/sc.1993.7
Issue Date:
DOI: https://doi.org/10.1038/sc.1993.7
Keywords
This article is cited by
-
Pre-surgical CT-assessment of neurogenic myositis ossificans of the hip and risk factors of recurrence: a series of 101 consecutive patients
BMC Musculoskeletal Disorders (2016)
-
Erhalt von Beweglichkeit
Trauma und Berufskrankheit (2013)
-
Rhabdomyolysis after heterotopic ossification: an unusual complication in a spinal cord injured patient
European Spine Journal (2012)
-
Magnetic resonance signal alterations in the acute onset of heterotopic ossification in patients with spinal cord injury
European Radiology (2005)
-
Nodular osteochondrogenic activity in soft tissue surrounding osteoma in neurogenic para osteo-arthropathy: morphological and immunohistochemical study
BMC Musculoskeletal Disorders (2004)
