
Abstract
Limited studies investigated the reasons for not adopting specific preparedness actions. This paper addresses this gap using national survey data from China. Seven disaster preparedness actions are used to measure preparedness behaviors, including “preparing food and water at home,” “paying attention to disaster-related information,” “making emergency plans,” “being aware of nearest shelters,” “being aware of building codes,” “participating in exercises or drills,” and “volunteering for emergencies.” The primary reasons for not adopting are “lack of awareness,” “not knowing where to buy or reach resources,” and “perceiving the action as unnecessary.” Other less chosen reasons ranking from high to low are the “financial cost,” “need for special knowledge,” “lack of time,” “need for collaboration with others,” “human energy consuming,” and “not feeling responsible.” Trust in government, relocation due to disasters, living in urban areas, and higher socioeconomic status are positively correlated with higher probabilities of adopting all seven preparedness activities. These findings emphasize the importance of community outreach by emergency management professionals to increase public awareness of disaster preparedness.
Similar content being viewed by others


Introduction
Natural-induced disasters claim hundreds of lives and millions of economic losses worldwide each year. According to reports from the United Nations Disaster Risk Reduction and the Davos World Risk Forum, there is an increasing trend of threats from various risks worldwide, especially in the context of climate change1,2. Pre-disaster mitigation and preparedness can reduce the impact of disasters. For example, calculations from the United States demonstrate that a one-dollar pre-disaster mitigation investment can reduce six dollars in losses from potential disasters3, while this investment and benefit ratio is about four in low- and middle-income countries4. Therefore, it is essential to discover the facilitators and barriers of pre-disaster mitigation and preparedness to reduce potential disaster losses in the uncertain world5.
There are two ways to conceptualize the contents of preparedness in current disaster research and practice. One way is to see preparedness as an overall conceptualization covering all mitigation, prevention, protection, response, and recovery activities, which is proposed as the Disaster Preparedness Framework by the Federal Emergency Management Agency of the United States6. Another traditional and widely accepted conceptualization of disaster preparedness involves the knowledge and capacities developed by all stakeholders within a community before a disaster occurs. Developing an emergency plan, learning about risk and protective actions, and participating in exercises or drills are commonly known activities7. Since disaster preparedness needs to engage all stakeholders within communities, households should be at the core of efforts to promote disaster preparedness activities.
Most current disaster preparedness studies at the household level follow the social-psychological paradigm, with surveys being the predominant method8,9,10,11,12. Examples of disaster preparedness activities within a household can be material preparedness, such as preparing emergency kits, food, or water; awareness preparedness, such as learning disaster-related knowledge; or behavioral preparedness, such as participating in drills or volunteering for a community emergency response team13,14,15. The Protective Action Decision Model (PADM), Health Belief Model (HBM), Social Cognitive Model (SCM), Theory of Planned Behavior (ToPB), and Protection Motivation Theory (PMT) are the widely used theoretical frameworks for investigating the determinants of household preparedness16,17,18. The cognitive processes, such as risk perception, responsibility attribution, trust in key stakeholders, and socioeconomic status differences, are the general influencing factors included in empirical studies19,20,21.
According to the theories mentioned earlier, the factors influencing individual and household preparedness behaviors can be categorized into four groups17,18,22,23,24. The first group of variables related to the socioeconomic and demographic characteristics of respondents and their households, such as income, education, gender differences, and having dependents like children or disabled family members25,26. For example, females usually have a higher risk perception but a relatively lower degree of preparedness than males27. The second cluster concerns hazards and contextual factors, such as environmental cues and related psychological feelings like place attachment and the disaster experience. The third cluster of influencing factors is the mental model or the psychological antecedents of behaviors12,18,28, which can determine an individual’s comprehension of potential hazards and then link these comprehensions to the decision-making process. These factors include risk perception, efficacy perception, trust, and responsibility attribution among stakeholders. The final group of factors are known as barriers and facilitators14,18, also referred to as obstacles29 or enablers30. These factors may prevent or encourage individuals to turn their decision-making about preparation into actual actions18,24, especially considering that socially vulnerable conditions can be the barriers to taking actual protective actions31. Practice-oriented or action researchers have investigated various ways of promoting public engagement in disaster preparedness activities24,32. Among these factors, the barriers between preparedness intentions and actual actions are the least investigated but crucial from an implementation or disaster justice perspective33.
Therefore, guided by the PADM and the literature review mentioned earlier, this analysis focuses on the barriers to adopting real actions, rather than just the willingness to act34. However, it does not consider detailed mental and decision-making processes such as risk comprehension35,36,37, risk perception20,38, efficacy perception17,39, or responsibility attribution21,40 (Fig. 1). We proposed nine potential reasons14,41 for not adopting a specific preparedness action if a respondent answered “not adopted” for one of the seven specific actions and conducted a national survey in China. We also include the basic individual characteristics, disaster experience, and trust in government in the modeling. This paper can answer the following questions, which have rarely been studied in previous literature:
-
(1)
What are the primary reasons for not adopting specific preparedness actions, such as preparing an emergency kit or volunteering for a community emergency response team?
-
(2)
Will trust in the government affect the adoption of preparedness actions?

Model of factors influencing actual preparedness behaviors.
Results
Descriptive analysis
We surveyed 6530 respondents from all 31 provinces in mainland China. As shown in Table 1, 59.95% of respondents were male, 40.03% were under 30, 59% were between 30 and 60, and only 0.96% were older than 60. A total of 7.14% were minorities, 79.10% were married, 20.47% had children at home, 24.61% had elders within the home, and 14.24% were from rural areas. Regarding educational attainment, 0.63% had primary school education or were illiterate, 3.86% had middle school education, 18.21% had high school education, 72.54% had college education, and 4.76% had post-graduate education degrees. The average self-reported socioeconomic status was 2.91, with a standard deviation of 0.77 and a range between 1 to 5. This means that the average self-reported socioeconomic ranking, from “Lowest (1)” to “Highest (5)”, was about three (Middle). Regarding disaster experience, 14.75% of participants had experienced natural disasters such as floods, earthquakes, or landslides; 7.12% had experienced H1N1 or H1N5 flu; and 14.75% had been relocated due to disasters. The overall degree of trust in government was 19.88, ranging between 5 and 25.
For the seven types of disaster preparedness activities, 90.84% of respondents said they would pay special attention to disaster-related information during regular days; 76.60% indicated they had prepared food and water that could last about 3 days at home; 72.22% said they had an emergency plan within their family; 75.53% knew the nearest emergency shelters; while 73.75% knew the building code requirements for potential earthquakes in their region; 66.26% had participated in a community exercise or drill; 54.10% reported volunteer experience.
Barriers of preparedness
We inquired about the reasons for not adopting a specific preparedness action when respondents chose “No” and proposed nine options with an additional open question for others. The primary reasons were “I am not aware (of doing this for potential disasters),” “I don’t know where to buy or to learn or to reach,” and “I don’t think it’s useful or necessary” (Fig. 2). For material preparedness and “paying attention to disaster-related information,” the top three reasons for not preparing were “not aware,” “not useful,” and “don’t know where to buy or to reach.” The top three reasons for “not making an emergency plan” were “not aware,” “don’t know where to learn,” and “not my responsibility.” For “knowing the building code,” the top three reasons for not adopting were “don’t know where to reach,” “not aware,” and “need too much technical knowledge,” while the top three reasons for not being aware of the shelter were “don’t know where to learn,” “not aware,” and “not useful.” For the two participation preparedness activities, in terms of volunteering and training, the primary reason for not adopting was “don’t know where to reach,” while “not aware,” “time-consuming,” “need collaboration efforts,” and “energy-consuming” had similar distributions.

Reasons for not prepared (percentage in tables).
We used the aggregation of the adoption of the seven disaster preparedness activities as the overall degree of disaster preparedness and a two-level multilevel linear regression model to estimate the effects of socioeconomic variables, disaster experience, and trust in government on overall preparedness. As shown in Fig. 3, being male, being a minority, being married, and having a higher degree of self-reported socioeconomic ranking were significantly associated with reporting a higher degree of disaster preparedness. Elders, families with elders living in rural areas, and those with natural disaster experiences were negatively and significantly correlated with disaster preparedness. However, those with experience of relocation due to disasters reported 1.189 higher degrees of preparedness than those without relocation experience. Moreover, with a higher degree of trust in government, a respondent would have a higher degree of preparedness. Educational attainment, having children at home, and experience of H1N1 were not significant predictors.

Multilevel regression on the overall disaster preparedness degrees.
We conducted seven logistic regressions to estimate the correlations between the abovementioned factors and the seven specific preparedness actions, with the results reported in Table 2. Overall, those with higher socioeconomic status, those with relocation or reconstruction experience due to disasters, those with a higher degree of confidence in the government’s capacity in disaster response, and those living in urban areas had a significantly higher likelihood of adopting all seven preparedness actions included in this study. Having children and pandemic experience were not significantly correlated with any of the seven actions. Gender, age, minority status, education, marriage, having elders in the family, and disaster experience had mixed correlations among these seven preparedness actions. The gender difference was not significant for “paying attention” and “knowing the community emergency plan.” Elders were less likely to have material supplies, “know the community plan,” “know emergency shelters,” “participate in drills,” or “be a volunteer.” With a higher degree of education, a respondent would be more likely to “pay attention,” “participate in drills,” or “be a volunteer,” but less likely to know community emergency plans. Married individuals were more likely to adopt all preparedness actions except for participating in drills. Families with elders were less likely to know the emergency plan, the shelter, the building code, participate in drills, and work as a volunteer. Interestingly, natural disaster experience was negatively correlated with knowing the emergency plan, knowing the nearest shelter building code, and volunteering.
Discussion
Disasters claim human lives and economic property each year. Pre-disaster mitigation and preparedness actions have proven useful in both developed and developing countries3,4. However, public preparedness is not satisfactory. Recent extreme weather and floods across Europe, Asia, America, and Oceania in the last several years have demonstrated that early warning information was delivered, but evacuation and other protective actions became the primary attribution of lives lost42,43,44,45. This paper can contribute to at least two aspects of current disaster and emergency management research.
First, to our knowledge, this is the only study investigating public preparedness in China using a national dataset. Most common preparedness activities are surveyed, including material preparedness, awareness preparedness, and participation preparedness. Most importantly, we investigated the primary reasons for not adopting these proposed preparedness activities. The top three reasons are lack of awareness, limited access to preparedness products or services, and low perceived response efficacy39 (not useful). This national survey highlights the importance and necessity of community outreach and public education from disaster and emergency management professionals. Also, providing channels for the public to become aware of and access either products or services or skills about disaster risk reduction is crucial.
Although Lindell has developed the Protective Action Decision Model for over 10 years18, which is more sophisticated and appropriate than other sociopsychological models such as the social cognitive model or the theory of planned behavior, the barriers and facilitators that influence the transition from protective action decision-making intention to actual behavior are still under-investigated. This is true for both normal preparedness behaviors and emergency situations such as warning and evacuation. Despite the functioning of risk monitoring and warning message dissemination in early warning systems46, there have been recent instances of inadequate evacuation or protective actions adopted by both individuals and governments during extreme weather and floods across the globe45,47. The United Nations has pledged to promote climate-related disaster early warning systems for “every single person on the planet” by the end of 202748, but the success of this ambition and its final results will depend on how people react to warnings during emergencies. Thus, following this study, we advocate for further investigation into the barriers to taking protective actions in different disaster scenarios and countries from a comparative perspective.
Second, trust in government, people living in rural areas, with lower socioeconomic status, and those with disaster experience but were not severely impacted have a lower probability of adopting all seven types of preparedness behaviors. As prior studies have revealed20,40,49, trust or confidence in government can play a dual role in disaster risk reduction. If a resident believes the government will come and is capable of saving his/her/them, they may rely more on the government and thus share less responsibility. Though a high level of trust in the government can be useful for the public to accept the government’s risk communication and protective action adoption suggestions, such as wearing masks during the Covid-19 pandemic. The findings about the role of disaster experience can remind researchers that we should carefully design our measures. Disaster experience has been found to have mixed or nonsignificant effects on adopting disaster risk reduction activities27. If a respondent was affected by a disaster but had no loss or minor loss, it is understandable that the respondent will not adopt disaster preparedness activities in the future. Thus, measurements of disaster experience in disaster studies should be carefully designed to capture the real impact.
This study has at least two limitations. First, the cross-sectional nature of this survey can only generate correlations instead of causal inference. Studies with experimental design or longitudinal design should be adopted to investigate the real causal relationship. Considering the potentially high cost for experimental studies with large samples and the appropriate to real-life situations, we recommend a survey-experiment research design that integrates experimental design into questionnaire surveys in future studies. Also, we propose to conduct deeper analysis on the reasons why different populations do not adopt a specific preparedness action. Second, we did not link the preparedness data from the survey to geodata. Therefore, we hope longitudinal research on disaster preparedness with geo-information can be conducted in the future.
Methods
Sampling and participants
We surveyed 6530 respondents from all 31 provinces in mainland China using a stratified sampling method. First, we selected the capital city of each province and another prefecture-level city in the province. For Yunnan and Jiangxi provinces, we selected two prefecture-level cities to compare the two provinces since Yunnan is earthquake-prone while Jiangxi has a lower earthquake risk. Within each city, 100 respondents were randomly selected using a quota sampling method with a 5% error. For the four megacities, Beijing, Shanghai, Chongqing, and Tianjin, we doubled the quotas to 200 respondents within each city.
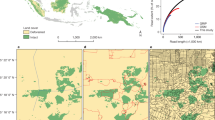
Data collection was implemented between August and September 2018 through an online survey platform. A written informed consent regarding the purpose of this study and voluntary participation was presented on the first page when a respondent chose to participate in the survey, and they can quit anytime during the survey. Of the 6611 questionnaires returned, 81 were dropped because they were either unfinished or the answering time was too short. Finally, 6530 respondents from 60 cities in 31 provinces were included in the analysis (Fig. 4).

The figure is created by the authors using data owned by the authors.
The study was performed in accordance with the Declaration of Helsinki. The survey was conducted through an online platform, and all participation was voluntary and anonymous. The study was approved by the ethical review committee of the Institute of Geophysics, China Earthquake Administration.
Measures of variables
Disaster preparedness: there are usually two ways of inquiring about an individual’s preparation for potential disasters. One is self-reported perception, where the question is framed like “How do you evaluate your preparation for XXX” and the answers are measured on a Likert scale49. An alternative way is to investigate actual preparation behavior, where the question is generally expressed as “Have you prepared a XXX?” and the answers are a checklist of actual preparedness actions14,15. Based on these studies that inquire about actual preparedness actions, we asked respondents’ adoption of seven preparedness actions in this survey: (1) preparing unique materials for emergencies, (2) paying attention to disaster-related information, (3) preparing a written family emergency plan, (4) being aware of nearest emergency shelters, (5) being aware of the building code for seismic risk of the region, (6) participating in emergency-related training or drills, and (7) being a volunteer for emergency-related activities. The first is a material preparedness action, the last two are community participation-related activities, and the rest are awareness preparedness actions. The answers to all seven questions were “yes (1)” or “no (0)”. The analysis used the aggregation of all seven preparedness actions to measure preparedness, with the preparedness indicator ranging from one to seven, with a mean value of 5.09 and a standard deviation of 2.23 (Table 1).
If a respondent chose “no,” we inquired about why they did not adopt that specific preparedness action in detail, based on previous studies. Lindell et al. conducted a study that included eight reasons for not adopting a disaster mitigation or preparedness action in a non-specific disaster context14. In contrast, Meyer et al. listed 15 barriers in a specific evacuation scenario, with examples such as “Cannot afford to leave” or “Do not want to leave pet”41. Since our study only inquired about general situations without specific disaster scenarios, we used the question, “Can you tell us the primary reason that you did not adopt this action, please?” and proposed nine potential reasons, with an additional option for others to allow respondents to fill in their own text. The ten proposed reasons were (1) too costly/have no money, (2) needs lots of knowledge or technology, (3) time-consuming, (4) cannot finish by oneself/need collaboration with others, (5) too human energy-consuming, (6) not aware, (7) the action has limited function/no necessity, (8) don’t know where to buy or prepare, (9) taking this action is not my responsibility, (10) others.
Controlled variables: based on prior studies on disaster preparedness15,50, we included the gender (male = 1), age group, ethnicity status (minority = 1), education attainment, marriage status (married = 1), whether there are children at home (yes = 1), whether there are elders at home (yes = 1), urban and rural differences (rural = 1), self-reported socioeconomic status, disaster experience, and trust in government as the controlled variables in this study. Disaster experience had three measures: experience of a natural-induced disaster, such as an earthquake, landslide, or flood; pandemic experience, such as H1N1, H1N5; and whether they had been relocated due to disasters. Trust in government captured the degrees of trust in five levels of government in China: central government, provincial government, county government, township government, and village/community self-governance committee. The question was “How do you trust the following institutions,” with answers for each ranging from 1 to 5, representing “not trust at all” to “trust very much.” The sum of trust degrees for all five levels of government was used as the degree of trust in government ranging from five to twenty-five with a Cronbach’s alpha test result of 0.8570, indicating good internal reliability. Self-reported socioeconomic status ranking from one to five was captured by the question, “How do you evaluate your socioeconomic ranking from the lowest to highest in the region where you live now?”
Data analysis strategy
We employed multilevel regressions for modeling in this analysis. We first reported the descriptive analysis of preparedness activities and influencing factors in Table 1, then reported the inquired reasons for not being prepared in Fig. 1. The overall preparedness degree was the aggregation of the adoption of the seven specific preparedness activities, so we employed a two-level linear regression model with control for province differences, with results reported in Fig. 2. For this specific model, we used the following syntax in Stata: mixed preparedness gender age minority education married economic family_with_baby family_with_elder rural experience_disaster experience_flu reconstruct trust_govment ||province. Moreover, we employed two-level logistic regressions to estimate the effects of predicting variables on the seven specific preparedness actions, respectively, with results reported in Table 2. For these multilevel logistic regression models, we used the “melogit” command and replaced the dependent variable with a specific action like “whether paid attention to disaster information” and kept all other influencing factors. All data analysis was implemented using statistical software Stata 16.0.
Data availability
The Disaster Preparedness Survey (2018) data used for the analysis and modeling in the study are available at Mendeley Data via doi: 10.17632/r5tfjc8j2m.1 with CC BY 4.0.
Code availability
The analysis code (Stata) for this paper is available upon request to the corresponding author.
References
UNDRR. United Nations Office for Disaster Risk Reduction Annual Report 2020. https://www.undrr.org/publication/undrr-annual-report-2020 (2020).
World Economic Forum. The Global Risks Report 2020. https://www3.weforum.org/docs/WEF_Global_Risk_Report_2020.pdf (2020).
Gall, M. & Friedland, C. J. If mitigation saves $6 per every $1 spent, then why are we not investing more? A Louisiana perspective on a national issue. Nat. Hazards Rev. 21, 04019013 (2020).
UNDRR. Benefits of Disaster Risk Reduction. https://www.preventionweb.net/understanding-disaster-risk/business-case-for-DRR (2021).
Joffe, H. et al. The fix-it face-to-face intervention increases multihazard household preparedness cross-culturally. Nat. Hum. Behav. 3, 453–461 (2019).
FEMA. National Preparedness Report (United States Department of Homeland Security, 2016).
UNDRR. Preparedness. https://www.undrr.org/terminology/preparedness (2020).
Bird, D. K. The use of questionnaires for acquiring information on public perception of natural hazards and risk mitigation—a review of current knowledge and practice. Nat. Hazards Earth Syst. Sci. 9, 1307–1325 (2009).
Paton, D. Disaster preparedness: a social‐cognitive perspective. Disaster Prev. Manag. 12, 210–216 (2003).
Paton, D. Disaster risk reduction: psychological perspectives on preparedness. Aust. J. Psychol. 71, 327–341 (2019).
Rostami-Moez, M., Rabiee-Yeganeh, M., Shokouhi, M., Dosti-Irani, A. & Rezapur-Shahkolai, F. Earthquake preparedness of households and its predictors based on health belief model. BMC Public Health 20, 646 (2020).
van Valkengoed, A. M. & Steg, L. Meta-analyses of factors motivating climate change adaptation behaviour. Nat. Clim. Change 9, 158–163 (2019).
Han, Z., Wang, H., Du, Q. & Zeng, Y. Natural hazards preparedness in Taiwan: a comparison between households with and without disabled members. Health Secur. 15, 575–581 (2017).
Lindell, M. K., Arlikatti, S. & Prater, C. S. Why people do what they do to protect against earthquake risk: perceptions of hazard adjustment attributes. Risk Anal. 29, 1072–1088 (2009).
Wu, G., Han, Z., Xu, W. & Gong, Y. Mapping individuals’ earthquake preparedness in China. Nat. Hazards Earth Syst. Sci. 18, 1315–1325 (2018).
Ejeta, L. T., Ardalan, A. & Paton, D. Application of behavioral theories to disaster and emergency health preparedness: a systematic review. PLoS Curr. https://doi.org/10.1371/currents.dis.31a8995ced321301466db400f1357829 (2015).
Kojan, L., Burbach, L., Ziefle, M. & Calero Valdez, A. Perceptions of behaviour efficacy, not perceptions of threat, are drivers of COVID-19 protective behaviour in Germany. Humanit. Soc. Sci. Commun. 9, 1–15 (2022).
Lindell, M. K. & Perry, R. W. The protective action decision model: theoretical modifications and additional evidence. Risk Anal. 32, 616–632 (2012).
Bubeck, P., Botzen, W. J. W. & Aerts, J. C. J. H. A review of risk perceptions and other factors that influence flood mitigation behavior: review of flood risk perceptions. Risk Anal. 32, 1481–1495 (2012).
Han, Z., Lu, X., Hörhager, E. I. & Yan, J. The effects of trust in government on earthquake survivors’ risk perception and preparedness in China. Nat. Hazards 86, 437–452 (2017).
Wehde, W. & Nowlin, M. C. Public attribution of responsibility for disaster preparedness across three levels of government and the public: lessons from a survey of residents of the U.S. South Atlantic and Gulf Coast. Publius 51, 212–237 (2021).
Kohn, S. et al. Personal disaster preparedness: an integrative review of the literature. Disaster Med. Public Health Prep. 6, 217–231 (2012).
Levac, J., Toal-Sullivan, D. & O’Sullivan, T. L. Household emergency preparedness: a literature review. J. Community Health 37, 725–733 (2012).
Ryan, B., Johnston, K. A., Taylor, M. & McAndrew, R. Community engagement for disaster preparedness: a systematic literature review. Int. J. Disaster Risk Reduct. 49, 101655 (2020).
Adams, R. M., Eisenman, D. P. & Glik, D. Community advantage and individual self-efficacy promote disaster preparedness: a multilevel model among persons with disabilities. IJERPH 16, 2779 (2019).
Eisenman, D. P. et al. Variations in disaster preparedness by mental health, perceived general health, and disability status. Disaster Med. Public Health Prep. 3, 33–41 (2009).
Wachinger, G., Renn, O., Begg, C. & Kuhlicke, C. The risk perception paradox—implications for governance and communication of natural hazards. Risk Anal. 33, 1049–1065 (2013).
Carman, J. P. & Zint, M. T. Defining and classifying personal and household climate change adaptation behaviors. Global Environ. Change 61, 102062 (2020).
Sadiq, A.-A. & Weible, C. Obstacles and disaster risk reduction: survey of memphis organizations. Nat. Hazards Rev. 11, 110–117 (2010).
Ramsbottom, A., O’Brien, E., Ciotti, L. & Takacs, J. Enablers and barriers to community engagement in public health emergency preparedness: a literature review. J. Community Health 43, 412–420 (2018).
Deng, H. et al. High-resolution human mobility data reveal race and wealth disparities in disaster evacuation patterns. Humanit. Soc. Sci. Commun. 8, 1–8 (2021).
Eisenman, D. P. et al. A program for local health departments to adapt and implement evidence-based emergency preparedness programs. Am. J. Public Health 108, S396–S398 (2018).
Lukasiewicz, A. The emerging imperative of disaster justice. in Natural Hazards and Disaster Justice: Challenges for Australia and Its Neighbours (eds Lukasiewicz, A. & Baldwin, C.) 3–23 (Springer, 2020).
Wang, T. et al. The determinants affecting the intention of urban residents to prepare for flood risk in China. Nat. Hazards Earth Syst. Sci. 22, 2185–2199 (2022).
Keselman, A., Slaughter, L. & Patel, V. L. Toward a framework for understanding lay public’s comprehension of disaster and bioterrorism information. J. Biomed. Inform. 38, 331–344 (2005).
Ripberger, J. T. et al. Measuring Tornado warning reception, comprehension, and response in the United States. Weather Clim. Soc. 11, 863–880 (2019).
Sugerman, D. E. et al. Emergency health risk communication during the 2007 San Diego Wildfires: comprehension, compliance, and recall. J. Health Commun. 17, 698–712 (2012).
Li, X. & Liu, T. Community participation effects on preparedness behaviour through risk perception: empirical data of hazardous chemicals from China. Int. J. Disaster Risk Reduct. 44, 101421 (2020).
Chen, Z. & Cong, Z. Response efficacy perception and taking action to prepare for disasters with different lead time. Nat. Hazards Rev. 23, 04021055 (2022).
Han, Z., Liu, J. & Wu, W.-N. Trust and confidence in authorities, responsibility attribution, and natural hazards risk perception. Risk Hazards Crisis Public Policy 13, 221–237 (2021).
Meyer, L., Vatcheva, K., Castellanos, S. & Reininger, B. Barriers to disaster preparedness among medical special needs populations. Front. Public Health 3, 205 (2015).
Kozlov, M. Hurricane ida forces researchers to rethink their future. Nature 597, 313–314 (2021).
Johnston, S. G. & Maher, D. T. Drought, megafires and flood-climate extreme impacts on catchment-scale river water quality on Australia’s east coast. Water Res. 218, 118510 (2022).
Hanchey, A. et al. Notes from the field: deaths related to Hurricane Ida reported by media—nine states, August 29–September 9, 2021. Morb. Mortal. Wkly. Rep. 70, 1385 (2021).
Han, Z., Shen, M., Liu, H. & Peng, Y. Topical and emotional expressions regarding extreme weather disasters on social media: a comparison of posts from official media and the public. Humanit. Soc. Sci. Commun. 9, 1–10 (2022).
Perera, D., Agnihotri, J., Seidou, O. & Djalante, R. Identifying societal challenges in flood early warning systems. Int. J. Disaster Risk Reduct. 51, 101794 (2020).
Thieken, A. H. et al. Performance of the flood warning system in Germany in July 2021–insights from affected residents. Nat. Hazards Earth Syst. Sci. 23, 973–990 (2023).
Gray, J. UN chief announces plan to get the whole world access to early weather warnings within 5 years. CNN https://www.cnn.com/2022/03/23/weather/worldwide-early-warning-systems-un-wmo/index.html (2022).
Han, Z., Wang, L. & Cui, K. Trust in stakeholders and social support: risk perception and preparedness by the Wenchuan earthquake survivors. Environ. Hazards 20, 132–145 (2021).
Lindell, M. K. & Perry, R. W. Household adjustment to earthquake hazard: a review of research. Environ. Behav. 32, 461–501 (2000).
Acknowledgements
We appreciate all the participants who participated in this survey. This study is supported by the Special Fund of the Institute of Geophysics, China Earthquake Administration (grant nos. DQJB22Z07 and DQJB23X12).
Author information
Authors and Affiliations
Contributions
Z.H. proposed the idea and drafted the paper, G.W. provided resource and data analysis. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Han, Z., Wu, G. Why do people not prepare for disasters? A national survey from China. npj Nat. Hazards 1, 1 (2024). https://doi.org/10.1038/s44304-024-00001-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s44304-024-00001-2
