
Abstract
Background
Lifestyle choices, metformin, and dietary supplements may prevent GDM, but the effect of intervention characteristics has not been identified. This review evaluated intervention characteristics to inform the implementation of GDM prevention interventions.
Methods
Ovid, MEDLINE/PubMed, and EMBASE databases were searched. The Template for Intervention Description and Replication (TIDieR) framework was used to examine intervention characteristics (who, what, when, where, and how). Subgroup analysis was performed by intervention characteristics.
Results
116 studies involving 40,940 participants are included. Group-based physical activity interventions (RR 0.66; 95% CI 0.46, 0.95) reduce the incidence of GDM compared with individual or mixed (individual and group) delivery format (subgroup p-value = 0.04). Physical activity interventions delivered at healthcare facilities reduce the risk of GDM (RR 0.59; 95% CI 0.49, 0.72) compared with home-based interventions (subgroup p-value = 0.03). No other intervention characteristics impact the effectiveness of all other interventions.
Conclusions
Dietary, physical activity, diet plus physical activity, metformin, and myoinositol interventions reduce the incidence of GDM compared with control interventions. Group and healthcare facility-based physical activity interventions show better effectiveness in preventing GDM than individual and community-based interventions. Other intervention characteristics (e.g. utilization of e-health) don’t impact the effectiveness of lifestyle interventions, and thus, interventions may require consideration of the local context.
Plain language summary
The effect of any given intervention to prevent gestational diabetes (high blood sugar levels that arise during pregnancy) may depend on the way it is delivered (how, when, what, etc). This study reviewed published literature to investigate if the effects of interventions (diet, exercise, metformin, probiotics, myoinositol) to prevent gestational diabetes differ according to the way it is being delivered (e.g., online vs in-person, by health professionals or others, etc.). Exercise delivered to group settings, or those delivered at a healthcare facility worked better to prevent gestational diabetes. Although we did not observe any differences with other delivery characteristics (e.g., online vs in-person), it does not mean they are always equally effective, it is important to consider individual situations when prescribing or developing interventions.
Similar content being viewed by others
Introduction
Gestational diabetes mellitus (GDM) is a metabolic disorder characterised by hyperglycemia, usually detected by screening in the late second or early third trimester of pregnancy1. In 2021, the International Diabetes Federation indicated that the global prevalence of GDM was 14%2. GDM poses several maternal health complications, including an increased risk of pre-eclampsia, caesarean delivery, and labor induction3. Offspring exposed to GDM in utero are more likely to be large-for-gestational-age4,5,6 and to develop impaired glucose metabolism and youth-onset type 2 diabetes7. Women with GDM have a risk of recurrent GDM in subsequent pregnancies8 and have an extremely elevated lifetime risk of developing type 2 diabetes mellitus9,10.
Although the etiology of GDM is idiopathic and multifactorial, it is presumed to be attributable to non-modifiable risk factors such as a previous history of GDM, advanced maternal age (>35 years), and family history of diabetes, and modifiable factors such as higher body weight11, metabolic syndrome12, and unhealthy lifestyle behaviors, including poor diet and lack of physical activity13.
Maintaining a normal body mass index (BMI) during preconception and interpregnancy periods, as well as limiting excessive gestational weight gain in early pregnancy, may help reduce the risk of developing GDM in some women. For women at higher risk of GDM, interventions with lifestyle modifications (diet and physical activity), medications(metformin), and dietary supplements (probiotics and inositol/myoinositol) that promote weight loss and/or improve insulin sensitivity could play a pivotal role in minimizing its development14,15,16. Previous studies on the effects of these interventions for reducing the risk of GDM, however, have reported inconsistent findings17,18,19,20,21,22,23,24,25,26,27,28,29. Taken together, these inconsistent findings could be due, in part, to the different intervention modalities that were delivered across trials.
According to the Consolidated Framework Implementation Research (CFIR), the implementation of a program requires the identification of core components that are essential to intervention efficacy, and peripheral components that can be adapted according to the context30. The Template for Intervention Description and Replication (TIDieR) checklist can be used to identify the core and peripheral components across intervention characteristics, such as who conducts the intervention and where the intervention delivery occurs31,32. Previous systematic reviews in the general population have found that intervention characteristics such as a greater number of sessions and interventions delivered by health professionals reduce the incidence of type 2 diabetes mellitus33 and promote weight loss in postpartum women34. Similarly, a meta-analysis35 and a randomized control trial36 demonstrated that other intervention characteristics, including lifestyle interventions assisted by technology and delivered at healthcare facilities, reduced the incidence of GDM. To date, there is no systematic review and meta-analysis that comprehensively evaluates the role of intervention type and characteristics on the effectiveness of lifestyle interventions, metformin, and dietary supplements in preventing GDM. A clear understanding of these moderating factors is essential to translate evidence from efficacy studies to implementation32,37,38,39,40,41,42.
This review is written on behalf of the American Diabetes Association (ADA)/European Association for the Study of Diabetes (EASD) precision Medicine in Diabetes Initiative (PMDI) as part of a comprehensive evidence evaluation in support of the 2nd International Consensus Report on Precision Diabetes Medicine43. This study therefore aimed to investigate the effect of intervention characteristics on GDM prevention using the TIDieR framework to inform the implementation of precision prevention in healthcare and community settings.
This study identifies that dietary, physical activity, diet plus physical activity, metformin, and myoinositol interventions reduce the incidence of GDM compared with control interventions. Group and healthcare facility-based physical activity interventions show better effectiveness in preventing GDM than individual and community-based interventions.
Methods
The Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) 2020 guideline was used to report this study44. The protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO: CRD42022320513).
Information sources and search strategy
Embase (Elsevier) and Ovid Medline/PubMed databases were searched to identify intervention studies published from inception through to May 24, 2022. Search strategies were built using several key terms and phrases by a professional medical librarian (AF) in consultation with the authors (SL, JJ, KV, and LR). The search was restricted to human studies and the English language. Search strategies for the respective databases are presented in Supplementary Data 1. A hand search was conducted on the reference lists of relevant reviews. All studies were exported to EndNote version 20 (Clarivate), and duplicates were identified and removed.
Study selection procedure and eligibility criteria
The retrieved articles from several databases were exported to Endnote Version 20 (Clarivate), and duplicates were removed. Hand searches, including the reference list of related reviews, were also assessed for additional eligible studies. Covidence (Veritas Health Innovation, Melbourne, Australia), an online software, was used for title/abstract screening and full-text reviews. Randomized Controlled Trials (RCTs) and Non-Randomised Controlled Trials (Non-RCTs) were included. Editorial letters, commentary articles, and conference abstracts were excluded. Interventions included lifestyle (diet and/or physical activity), metformin, and dietary supplements (myoinositol/inositol and probiotics). Control groups were usual care/placebo or minimal intervention (no more than one lifestyle session). The primary outcome was the development of GDM. The description of eligibility criteria on the population, intervention, control, outcome, and types of study are provided in Supplementary Table 1. Two reviewers from the reviewers’ team (WWT, SL, JG, MC, NH, GGU, GL, SJZ, RT, MP, KL, MB, and AQ) independently screened each record for eligibility, and disagreements were resolved by discussion with an arbiter (SL).
Assessment of risk of bias
The quality appraisal was performed using the Cochrane Risk of Bias tool for Randomized Trials (ROB 2.0)45 and the Risk of Bias in Non-randomized Studies of Interventions (ROBINS-I)46 for the study type, as their name suggests. The quality of cluster RCT studies was evaluated by the ROB 2.0 tool. The ROBINS-I tool was used to assess the quality of non-RCTs. The risk of bias was assessed independently by two reviewers, and discrepancies were resolved by consensus.
Assessment of evidence certainty
The certainty of the evidence was assessed using the Grading of Recommendations, Assessment, Development, and Evaluation method (GRADE)47. Five domains, namely the risk of bias (assessed using tools mentioned above), inconsistency, indirectness, imprecision, and publication bias, were used to evaluate the degree of certainty. The quality of evidence was ranked as high, moderate, low, or very low based on the GRADE guideline48.
Data extraction
The outcome variable (GDM incidence) was independently extracted by two reviewers. The study (authors name, study year, setting, design, and sample size) and intervention characteristics (e.g., type of intervention and intervention provider) were extracted using the TIDieR checklist49. The intervention characteristics include: (i) who (intervention providers/facilitators); (ii) tailoring (individualized plan); (iii) why (utilization of theoretical framework/model); (iv) how (application of technology and intervention modality); (v) what (intervention type e.g. diet, intervention material and procedure, control description); (vi) where (location of the intervention delivered; (vii) how much (duration and frequency of sessions), and (viii) how well was the intervention delivered (fidelity and attrition)49. Two authors (SL and WWT) independently coded the intervention characteristics, and disagreements were resolved by discussion. The detailed definition of each intervention characteristics (TIDieR constructs) is provided in Supplementary Data 2. Multiple reports from the same trial were considered as a single study.
Data synthesis and analysis
The outcome was GDM incidence. The data were analysed using STATA/SE TM Version 17. Risk ratios (RR) and 95% confidence intervals (CI) were pooled using the random-effects model by applying the DerSimonian and Laird estimator50.
Heterogeneity was examined by the I2 statistic51. Sensitivity analysis was carried out by excluding non-RCTs assuming the study design could impact the risk estimate due to lack of randomization52. Subgroup analysis by intervention characteristics was performed. A funnel plot and Egger’s test were used to examine publication bias. Asymmetry of the funnel plots and significant Egger’s test (p < 0.05) suggest publication bias.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Results
Study selection
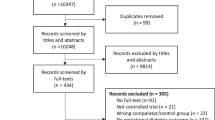
A total of 10,347 studies are retrieved, and 116 studies involving 40,940 participants are included. The PRISMA flow diagram is shown in Fig. 1.

The diagram illustrates the procedure followed to identify the eligible studies. Studies were excluded in each critical screening step based on the eligibility criteria.
Characteristics of the included studies
A description of the included studies is shown in Supplementary Data 3. Of those included, 102 (87.9%) were RCTs. A total of 92 (79.3%) studies involved lifestyle intervention, 13 (11.1%) metformin, and 12 (10.3%) examined the role of dietary supplements (myoinositol/inositol and probiotics) in preventing GDM. The criteria used for GDM diagnosis varied across the studies. The most commonly used diagnostic criterion (n = 37) is the International Association of the Diabetes and Pregnancy Study Groups (IADPSG). The 1999 World Health Organization (WHO) criterion (prior to WHO adopting those of the IADPSG) was reported in nine studies, Carpenter & Coustan in seven studies, and the National Diabetes Data Group in six studies. Of these, 70 (60.3%) studies were conducted in high-income countries (predominantly Europe), and 7 were conducted in low-middle-income settings.
Seven53,54,55,56,57,58 commenced the intervention during the preconception period, of which three were on lifestyle interventions, and the remaining were metformin interventions. The sample size ranged between 3159 and 4,63160 participants. The median age and BMI of participants at baseline were 30.3 years and 28.6 kg/m2, respectively.
Risk of bias and evidence quality assessment findings
Of the 102 RCTs, a high risk of bias was observed in 33 (32.4%), mainly owing to deviation from the intended intervention. Most studies (91.2%) had a low risk of bias in measuring the outcome domain. Generally, based on the overall quality judgment criterion, 33(32.4%) and 21(20.6%) of studies exhibited high and low risk of bias, respectively. In the non-RCTs, most had a low risk of bias due to the selection of study participants and reported results. A critical risk of bias due to confounding was observed in a third (33.3%) of studies. Overall, four non-RCTs were at critical risk of bias, according to the overall risk of judgment (Supplementary Data 4).
While the quality of evidence on diet-only and physical-only interventions was moderate, it was low for combined interventions (physical activity and diet). The quality of evidence for metformin, myoinositol/inositol, and probiotic interventions was very low. The most frequent reason to downgrade the level of certainty was a risk of bias and publication bias (Supplementary Data 5).
Effect of lifestyle intervention in reducing the incidence of GDM by intervention characteristics
Supplementary Data 6 shows the characteristics of the included studies by the TIDieR framework. Of the 92 included studies investigating lifestyle intervention, 59(64.1%) included combined physical activity and dietary interventions, 17(18.5%) were physical activity-only, and 16(17.4%) were diet-only interventions. Of the studies that included a dietary intervention, nine focused on specific dietary approaches, including the Mediterranean diet and low glycaemic index diet61,62,63,64,65,66, whilst the remaining provided general healthy dietary advice based on national dietary guidelines.
With regards to the delivery of the intervention, health professionals (e.g., dietitians, obstetricians, exercise physiologists, etc.) facilitated the intervention in 66 (71.7%). Twenty-two (23.9%) studies applied theoretical or behavioral change models, including social cognitive theory67,68,69,70,71,72,73,74. Except for three studies, a detailed description of the nature and procedure of the intervention delivered to the participants was reported. The care given to participants assigned to the control groups was described in 76 (82.6%) of studies. Most studies did not provide clear information on when the intervention commenced or ended for the participants63,75,76,77 nor the frequency of sessions.
E-health technologies (e.g. telephone calls, WeChat, and email) were used in 46 (50%) of studies to deliver the intervention. Four studies (4.3%) provided the intervention virtually, while 49 (53.3%) delivered face-to-face only. The intervention was delivered to individuals in 17 (18.5%) studies, in group format in nine (9.8%) studies, and in combined (group and individual) in 17(18.5%) studies, while there was no description format in the rest of the studies. Three studies (3.3%) initiated the intervention during the preconception period, whereas 28 (30.4%) were in the first trimester and 58 (63%) were during the second trimester. Seventy-four (80.4%) studies utilized interventions based on individualized plans. Forty (43.5%) studies applied intervention fidelity measures, such as a curriculum for lifestyle intervention. The attrition rate of the studies ranged between 0%78,79,80,81,82,83,84,85,86,87 and 49.3%88.
Meta-analysis of the effect of intervention characteristics on lifestyle interventions
A total of 92 studies involving 31,663 participants are included in the meta-analysis to examine the effect of lifestyle intervention on reducing GDM. Overall, lifestyle intervention reduced the incidence of GDM by 22% (RR 0.78; 95% CI 0.72, 0.85; I2 = 45%).
The difference between lifestyle intervention types was insignificant (subgroup p-value = 0.59) (Table 1).
Physical activity-only intervention
Physical activity-only interventions reduced GDM by 31% (RR 0.69; 95% CI 0.55, 0.85; I2 = 25.9%; moderate quality evidence) (Fig. 2) compared with control group. According to Egger’s test (p-value = 0.23) and funnel plot (Supplementary Fig. 1), publication bias was not observed. Group-based physical activity demonstrated the greatest reduction in risk of GDM (RR 0.66; 95% CI 0.46, 0.95; I2 = 28.3%) compared with combined (individual and group) (RR 0.79; 95% CI 0.47, 1.34; I2 = 0%) and individual (RR 1.03; 95% CI 0.72, 1.46; I2 = 0%) intervention modalities (subgroup p-value = 0.04). Physical activity interventions delivered in healthcare facilities reduced the risk of GDM by 41% (RR 0.59; 95% CI 0.49, 0.72; I2 = 33.8%) compared with home/community-based interventions (RR 1.05; 95% CI 0.73, 1.49; I2 = 58.8%), and combined settings (home plus and healthcare facility) (RR 1.21; 95% CI 0.67, 2.18) (subgroup p-value = 0.03) [Supplementary Data 7].

The estimates of 17 studies were pooled using the random-effects model to estimate the pooled effect of physical activity intervention on reducing the risk of GDM. The overall estimate represented in diamond shape shows the effect size (risk ratio with 95% confidence interval). The square shapes in individual study suggests the effect size estimate—the bigger the shape, the larger the effect size and the reverse is true.
Diet-only intervention
Dietary intervention reduced GDM by 27% (RR 0.73; 95% CI; 0.61, 0.86; I2 = 31.03%; moderate quality evidence) (Fig. 3). According to Egger’s test (p-value = 0.42) and funnel plot, (Supplementary Fig. 2), publication bias was not observed. Sensitivity analysis was done by excluding two non-RCT studies, and dietary intervention reduced the risk of GDM by 25% (RR 0.75; 95% CI; 0.64, 0.88; I2 = 23.1%). None of the intervention characteristics showed an effect on the effectiveness of dietary interventions in preventing GDM (Table 2).

The estimates of 16 studies were pooled using the random-effects model to estimate the pooled effect of dietary intervention on reducing the risk of GDM. The overall estimate represented in diamond shape shows the effect size (risk ratio with 95% confidence interval). The square shapes in individual studies suggest the effect size estimate—the bigger the shape, the larger the effect size, and the reverse is true.
Combined (diet and physical activity) intervention
The combined diet and physical activity intervention lowered the incidence of GDM by 18% (RR 0.82; 95% CI 0.74, 0.94; I2 = 46%; low-quality evidence). According to Egger’s test (p-value = 0.01) and funnel plot (Supplementary Fig. 3), publication bias was observed. After excluding six non-RCTs, combined lifestyle intervention reduced the risk of GDM by 17% (RR 0.83; 95% CI; 0.74, 0.93; I2 = 64.8%). Combined lifestyle interventions conducted in low-middle income countries (RR 0.51; 95% CI 0.32, 0.8; I2 = 17.3%) demonstrated a larger effect in reducing the risk for GDM than middle-income countries (RR 0.69; 95% CI 0.56, 0.83; I2 = 52.5%) and high-income countries (RR 0.93; 95% CI 0.84, 1.04; I2 = 52.5%) (subgroup p-value = 0.00) (Table 3). The incidence of GDM did not differ by any other intervention characteristic.
Effect of metformin on reducing the incidence of GDM by intervention characteristics
Thirteen studies were included. Nine studies described the intervention given to participants assigned to the placebo groups, two applied tailored interventions27,89,90, and one was technology-based (telephone)89. The range of daily dosage was 50089–3000 mg91. Eight studies monitored the adherence of participants to the medication through pill count. The attrition rate ranged from 0% to 42%92. The detailed intervention characteristics are presented in Supplementary Data 8.
On meta-analysis, metformin reduced the risk of developing GDM by 34% (RR 0.66; 95% CI 0.47, 0.93; I2 = 73.08%; very low-quality evidence) (Fig. 4). According to Egger’s test (p = 0.00) and funnel plot (Supplementary Fig. 4), publication bias was detected. Further subgroup analysis was not undertaken due to insufficient studies on each intervention characteristics group.

The estimates of 13 studies were pooled using the random-effect model to estimate the pooled effect of metformin intervention on reducing the risk of GDM. The overall estimate represented in diamond shape shows the effect size (risk ratio with 95% confidence interval). The square shapes in individual studies suggest the effect size estimate—the bigger the shape, the larger the effect size, and the reverse is true.
Effect of dietary Supplements on reducing the incidence of GDM by intervention characteristics
Probiotic supplementation
Five studies examined the relationship between probiotic supplements and the incidence of GDM. Three combined investigations of supplementation with a probiotic and another intervention (one co-administered a fish oil supplement)93, one applied an additional unspecified dietary intervention66, and one applied a technology via telephone94. Three (60%) studies monitored participants’ adherence to the intervention mainly through pill counts93,94,95. The attrition rate was 2.796–25.4%66. A detailed description is provided in Supplementary Data 9.
On meta-analysis, probiotics supplements did not reduce the risk of GDM (RR 0.88; 95% CI; 0.52, 1.47; I2 = 73.7%; very low-quality evidence). The Eggers test (p-value = 0.24) and funnel plot (Supplementary Fig. 5) reveal the absence of publication bias. By intervention type, probiotics co-administered with diet (RR 0.36; 95% CI; 0.18, 0.72), probiotics alone (RR 1.0; 95% CI 0.56, 1.81), and probiotics coupled with fish oil (RR 1.3; 95% CI 0.78, 2.15) reduced the risk of GDM (Fig. 5). Subgroup analysis by the intervention characteristics was not performed due to the limited number of studies in each subgroup.

The estimates of six studies were pooled using the random-effect model to estimate the effects of different categories of probiotics supplementation on reducing the risk of GDM. The red diamond shape shows the effect size (risk ratio) in each subgroup. The overall estimate represented in the green diamond at the bottom shows the overall effect size (risk ratio). The square shapes in individual studies suggest the effect size estimate ─the bigger the shape, the larger the effect size, and the reverse is true.
Myoinositol/inositol supplement
Seven studies96,97,98,99,100,101,102 examined the effect of myoinositol/inositol supplements in preventing GDM (Supplementary Data 4). On the meta-analysis, myoinositol/inositol supplement reduced the risk of GDM by 61% (RR 0.39; 95% CI 0.23, 0.66; I2 = 78.87%; very low-quality evidence) (Fig. 6). Egger’s test (p-value = 0.26) and funnel plot (Supplementary Fig. 6) exhibited that publication bias was not a concern.

The estimates of seven studies were pooled using the random-effects model to estimate the effects of different categories of myoinositol supplementation on reducing the risk of GDM. The overall estimate represented in the green diamond at the bottom of the figure shows the overall effect size (risk ratio with 95% confidence interval). The square shapes in individual studies suggest the effect size estimate—the bigger the shape, the larger the effect size, and the reverse is true.
Subgroup analysis by the intervention characteristics was not performed due to the limited number of studies in each subgroup.
Discussion
In this comprehensive systematic review and meta-analysis, interventions utilizing diet, physical activity, diet plus physical activity, metformin, and myoinositol reduced the incidence of GDM compared with control interventions. The findings are in line with the most recent findings from umbrella reviews103,104, implying the importance of incorporating these interventions in routine maternal care to prevent GDM. However, the primary analysis of this review has previously shown that not all interventions work equally for all participants105, and therefore, considering person-level characteristics (e.g., previous history of GDM) during implementation could be important to enhance the effectiveness of interventions. This secondary analysis shows the differences in the intervention effectiveness by intervention type and delivery. For physical activity interventions, those delivered in groups or in healthcare facilities resulted in a greater reduction in the risk of developing GDM compared with individual and combined (group and individual) formats and with community-home-based interventions. Diet-only interventions were similarly effective across all delivery contexts. Combined diet and physical activity interventions conducted in low-middle-income countries demonstrated a greater reduction in GDM than in upper-middle and high-income countries. Insufficient data were available for meta-analysis for metformin and dietary supplements.
This analysis found that group-based delivery was a more effective delivery format for physical activity interventions compared with individual-based or individual-plus group formats. This finding is in line with a systematic review demonstrating that group-based physical activity helps prevent GDM106. The greater effectiveness of group-based delivery for physical activity intervention may be due to a high number of studies (76.5%) within this category providing fully supervised sessions. The finding of this study is consistent with previous systematic reviews and meta-analyses in individuals with type 2 diabetes, where it has been reported that supervised physical activity intervention enhanced the effectiveness of blood glucose management in these individuals107,108. This may be because those studies utilized multiple behavior change techniques concurrently, including behavioral practice/rehearsal, demonstration of the behaviors, and feedback on behavior107. Group-based interventions may also be more beneficial in the prevention of GDM as they create the opportunity for women to engage with their peers. This occurs when individuals within a group share ideas and experiences, which could help enhance their commitment and motivation, ultimately motivating them to stay in the intervention program for the desired intervention period109. Greater effectiveness with group-based interventions has also been shown previously in diabetes and weight management interventions107,110,111,112. Peer support has been shown to predict physical activity behavior change in adolescents, serving as behavior change agents who provide support and role modelling to actively engage and maintain lifestyle interventions113.
In addition, group-based intervention is an acceptable delivery format by healthcare providers and by women. A systematic review among healthcare providers reported perceived positive experiences from group-based antenatal care, including richer use of their time and better value proposition in terms of provider investment and workload114. A recent systematic review of qualitative studies has also found that group-based physical activity was highly acceptable by women115. Given the observed effectiveness of group-based physical activity during pregnancy in reducing the risk of GDM and considerable acceptability by healthcare professionals and service users, it may be beneficial to utilize this format in a real-world setting.
Delivery settings could also affect the effectiveness of physical activity interventions in preventing GDM. Those initiated during pregnancy in health facilities reduced the incidence of GDM more than home/community-based interventions. This finding is supported by previous meta-analyses of RCTs of supervised physical activity interventions during pregnancy in preventing GDM35,116. In-facility interventions may provide opportunities for supervision and feedback from professionals, which likely enhance the adherence of participants and as a result, improve the intervention effectiveness117. However, as data on the level of adherence to physical activity interventions delivered in different settings were not reported, it is impossible to draw an inference that the better effectiveness of healthcare facility-based interventions are related to the better adherence of participants to the intervention. Future primary studies are recommended to examine the role of adherence in the effectiveness of physical activity interventions delivered in different settings.
Since all the physical activity intervention studies included in our review commenced during pregnancy, our findings may not be applicable to interventions started during the preconception or postpartum period, during which additional barriers to accessing interventions may exist. A systematic review of RCTs underscored that supervised physical activity intervention during the postpartum period leads to a high rate of refusal and withdrawal from the intervention118. This suggests the reproductive life stages of the participants are an important consideration in the choice of intervention setting. To foster better adherence of individuals to interventions throughout the inter-conception period, healthcare facilities need to be accessible to women and provide the necessary resources such as childcare119. Home-based interventions could be an alternative and preferred modality for reproductive-age women due to fewer barriers, such as parenting responsibilities and time constraints120,121. These factors must be considered when selecting the intervention setting. A flexible approach that considers home/community-based sessions supported by virtual or in-person supervision may provide equivalent benefits to healthcare facility-based interventions. Future trials are recommended to compare the role of different intervention settings across the reproductive life stages in preventing GDM and with an evaluation of adherence rate, consumer satisfaction, and resources required to generate user-informed and sustainable evidence-based practice in real-world settings.
Moreover, differences in the effectiveness of physical activity intervention across other intervention characteristics, including intensity and type of physical activity, were not observed. Similar to a recent umbrella review103, we found that physical activity interventions of light-moderate or moderate intensity effectively reduced the risk of GDM. However, the differences between subgroups by intensity were found to be insignificant (p-value = 0.18). It was evidenced that light to moderate or moderate intensity reduced the incidence of GDM compared with moderate to vigorous intensity103. Given the effectiveness of light-moderate activities, which are more achievable than higher-intensity training, especially during pregnancy, women at risk of GDM should be recommended to engage in moderate-intensity activities to reduce their GDM risk.
We observed that studies on combined lifestyle interventions conducted in low-middle-income countries demonstrated greater effectiveness in reducing the risk of GDM than in high- and upper-middle-income countries. Given the consistent evidence showing the effectiveness of lifestyle intervention in preventing GDM in low-middle income countries122, along with the growing diabetes burden in this region2,123, there is an urgent need for large-scale implementation of combined lifestyle intervention to curb the growing incidence of GDM in low-middle income countries. On the other hand, there is a paucity of studies in low-income countries, as evidenced by our study and a previous review122, which is an evidence gap hindering the reduction of global diabetes disparities in these regions. Thus, future studies are needed in low-middle-income countries to demonstrate the effectiveness of lifestyle interventions in GDM prevention and to identify effective intervention characteristics in these.
Diet-only interventions reduced the risk of GDM irrespective of the intervention characteristics (e.g., e-health and home-based) and setting (i.e. country). This suggests that dietary interventions could be delivered in any format according to contextual needs without compromising effectiveness in GDM prevention. However, comparison by intervention duration, frequency and dietary types were not performed due to poor reporting in the included studies, as reflected in a previous review124.
Future individual studies should improve the reporting on these characteristics to enable further elucidation of optimal duration, frequency, and dietary type of interventions in preventing GDM.
This is the first comprehensive review that investigated intervention characteristics of lifestyle, metformin, and dietary supplements in preventing GDM. The approach is underpinned by established frameworks such as CFIR for intervention implementation30 and TIDieR for the identification of intervention characteristics49. However, missingness in certain intervention characteristics (frequency of sessions and duration) was a major barrier in examining the effectiveness of these intervention characteristics. In addition, when interpreting and translating the evidence, it is important to note that substantial heterogeneity remained within subgroups, suggesting other sources of heterogeneity were present such as bias due to inclusion of non-RCTs52. However, the sensitivity analysis excluding non-RCTs did not alter the effect of interventions on reducing the incidence of GDM. Given the poor adherence of authors of individual studies to the evidence reporting checklist (TIDieR framework), coding was subject to interpretation. This was attempted to mitigate by having two trained reviewers (WWT and SL). Lastly, the certainty of quality of evidence for all interventions ranged from low to moderate, suggesting caution when applying the findings in real-world settings.
Conclusions
Dietary, physical activity, diet plus physical activity, metformin, and myoinositol interventions during pregnancy reduce the incidence of GDM compared with control interventions. Group and healthcare facility-based physical activity interventions during pregnancy reduce the risk of GDM compared with individual-based and home/community-based interventions, respectively. Dietary interventions could be implemented in any format with considerations of contextual factors. Researchers conducting intervention trials better follow TIDieR guidelines when reporting to enable the identification of key components for the implementation of interventions to prevent GDM.
Data availability
All data used to produce this study was gathered from published studies. The key terms and search strategies built to retrieve studies are available in Supplementary Table 1 of the Supplementary Information file. The list of included studies is available in Supplementary Data 1. All other relevant data that support the findings of the study are available from the corresponding author upon reasonable request.
References
American Diabetes Association. 2. Classification and diagnosis of diabetes: standards of medical care in diabetes—2019. Diabetes Care 42, S13–S28 (2019).
Wang, H. et al. IDF diabetes atlas: estimation of global and regional gestational diabetes mellitus prevalence for 2021 by International Association of Diabetes in Pregnancy Study Group’s Criteria. Diabetes Res. Clin. Pract. 183, 109050 (2022).
Malaza, N. et al. A Systematic Review to compare adverse pregnancy outcomes in women with pregestational diabetes and gestational diabetes. Int. J. Environ. Res. Public Health 19, 10846 (2022).
Wahabi, H. A., Esmaeil, S. A., Fayed, A. & Alzeidan, R. A. Gestational diabetes mellitus: maternal and perinatal outcomes in King Khalid University Hospital, Saudi Arabia. J. Egypt. Public Health Assoc. 88, 104–108 (2013).
Gasim, T. Gestational diabetes mellitus: maternal and perinatal outcomes in 220 Saudi women. Oman Med. J. 27, 140 (2012).
He, X.-J. et al. Is gestational diabetes mellitus an independent risk factor for macrosomia: a meta-analysis? Arch. Gynecol. Obstet. 291, 729–735 (2015).
Blotsky, A. L., Rahme, E., Dahhou, M., Nakhla, M. & Dasgupta, K. Gestational diabetes associated with incident diabetes in childhood and youth: a retrospective cohort study. CMAJ 191, E410–E417 (2019).
Schwartz, N., Nachum, Z. & Green, M. S. The prevalence of gestational diabetes mellitus recurrence—effect of ethnicity and parity: a metaanalysis. Am. J. Obstet. Gynecol. 213, 310–317 (2015).
Vounzoulaki, E. et al. Progression to type 2 diabetes in women with a known history of gestational diabetes: systematic review and meta-analysis. BMJ 369, m1361 (2020).
Saravanan, P. et al. Gestational diabetes: opportunities for improving maternal and child health. Lancet Diabetes Endocrinol. 8, 793–800 (2020).
Martínez‐Hortelano, J. A. et al. Interpregnancy weight change and gestational diabetes mellitus: a systematic review and meta‐analysis. Obesity 29, 454–464 (2021).
Habibi, N. et al. Maternal metabolic factors and the association with gestational diabetes: a systematic review and meta‐analysis. Diabetes/Metab. Res. Rev. 38, e3532 (2022).
Günther, J. et al. How does antenatal lifestyle affect the risk for gestational diabetes mellitus? A secondary cohort analysis from the GeliS trial. Eur. J. Clini. Nutr. 76, 150–158 (2022).
Thomas, T. & Pfeiffer, A. F. Foods for the prevention of diabetes: how do they work? Diabetes/Metab. Res. Rev. 28, 25–49 (2012).
Baker, C. & Brownell, K. Physical activity and maintenance of weight loss: Physiological and psychological mechanisms. Phys. Act. Obes. 311–328 (2000).
Miketinas, D. C. et al. Fiber intake predicts weight loss and dietary adherence in adults consuming calorie-restricted diets: the POUNDS lost (preventing overweight using novel dietary strategies) study. J. Nutr. 149, 1742–1748 (2019).
Song, C., Li, J., Leng, J., Ma, R. & Yang, X. Lifestyle intervention can reduce the risk of gestational diabetes: a meta‐analysis of randomized controlled trials. Obes. Rev. 17, 960–969 (2016).
Wu, S., Jin, J., Hu, K.-L., Wu, Y. & Zhang, D. Prevention of gestational diabetes mellitus and gestational weight gain restriction in overweight/obese pregnant women: a Systematic Review and Network Meta-Analysis. Nutrients 14, 2383 (2022).
Pascual-Morena, C. et al. Exercise versus metformin to improve pregnancy outcomes among overweight pregnant women: a systematic review and network meta-analysis. J. Clin. Med. 10, 3490 (2021).
Guo, X. Y. et al. Improving the effectiveness of lifestyle interventions for gestational diabetes prevention: a meta‐analysis and meta‐regression. BJOG 126, 311–320 (2019).
Bain, E. et al. Diet and exercise interventions for preventing gestational diabetes mellitus. Cochrane Database Syst. Rev. https://doi.org/10.1002/14651858.CD010443 (2015).
Han, S., Middleton, P. & Crowther, C. A. Exercise for pregnant women for preventing gestational diabetes mellitus. Cochrane Database Syst. Rev. https://doi.org/10.1002/14651858.CD009021 (2012).
Natali, A. & Ferrannini, E. Effects of metformin and thiazolidinediones on suppression of hepatic glucose production and stimulation of glucose uptake in type 2 diabetes: a systematic review. Diabetologia 49, 434–441 (2006).
Zhao, J., Liu, X. & Zhang, W. The effect of metformin therapy for preventing gestational diabetes mellitus in women with polycystic ovary syndrome: a meta-analysis. Exp. Clin. Endocrinol. Diabetes 128, 199–205 (2020).
Mahdizade Ari, M. et al. The effect of probiotics on gestational diabetes and its complications in pregnant mother and newborn: a systematic review and meta‐analysis during 2010–2020. J. Clin. Lab. Anal. 36, e24326 (2022).
Vitagliano, A. et al. Inositol for the prevention of gestational diabetes: a systematic review and meta-analysis of randomized controlled trials. Arch. Gynecol. Obstet. 299, 55–68 (2019).
Khattab, S. et al. Can metformin reduce the incidence of gestational diabetes mellitus in pregnant women with polycystic ovary syndrome? Prospective cohort study. Gynecol. Endocrinol. 27, 789–793 (2011).
Sales, W. B. et al. Effectiveness of metformin in the prevention of gestational diabetes mellitus in obese pregnant women. Rev. Bras. Ginecol. Obstet. 40, 180–187 (2018).
Barrett, H. L., Nitert, M. D., Conwell, L. S. & Callaway, L. K. Probiotics for preventing gestational diabetes. Cochrane Database Syst. Rev. 2014, Cd009951 (2014).
Damschroder, L. J. et al. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement. Sci. 4, 1–15 (2009).
Howick, J. et al. TIDieR-Placebo: a guide and checklist for reporting placebo and sham controls. PLoS Med. 17, e1003294 (2020).
Hoffmann, T. C., Erueti, C. & Glasziou, P. P. Poor description of non-pharmacological interventions: analysis of consecutive sample of randomised trials. BMJ 347, f3755 (2013).
Chen, M. et al. The effect of lifestyle intervention on diabetes prevention by ethnicity: a systematic review of intervention characteristics using the tidier framework. Nutrients 13, 4118 (2021).
Lim, S. et al. A systematic review and meta‐analysis of intervention characteristics in postpartum weight management using the TIDieR framework: a summary of evidence to inform implementation. Obes. Rev. 20, 1045–1056 (2019).
Doi, S. A. et al. Physical activity in pregnancy prevents gestational diabetes: a meta-analysis. Diabetes Res. Clin. Pract. 168, 108371 (2020).
Ding, B. et al. WeChat-assisted dietary and exercise intervention for prevention of gestational diabetes mellitus in overweight/obese pregnant women: a two-arm randomized clinical trial. Arch. Gynecol. Obstet. 304, 609–618 (2021).
Tang, Q. et al. Effectiveness of five interventions used for prevention of gestational diabetes: a network meta-analysis. Medicine 101, e29126 (2022).
Cleland, C. L., Tully, M. A., Kee, F. & Cupples, M. E. The effectiveness of physical activity interventions in socio-economically disadvantaged communities: a systematic review. Prev. Med. 54, 371–380 (2012).
Shepherd, E. et al. Combined diet and exercise interventions for preventing gestational diabetes mellitus. Cochrane Database of Syst. Rev. 11, Cd010443 (2017).
Singal, A. G., Higgins, P. D. & Waljee, A. K. A primer on effectiveness and efficacy trials. Clin. Transl. Gastroenterol. 5, e45 (2014).
Glasgow, R. E., Lichtenstein, E. & Marcus, A. C. Why don’t we see more translation of health promotion research to practice? Rethinking the efficacy-to-effectiveness transition. Am. J. Public Health 93, 1261–1267 (2003).
Cotterill, S. et al. Getting messier with TIDieR: embracing context and complexity in intervention reporting. BMC Med. Res. Methodol. 18, 1–10 (2018).
Tobias, D. K. et al. Second international consensus report on gaps and opportunities for the clinical translation of precision diabetes medicine. Nat. Med. 29, 2438–2457 (2023).
Page, M. J. et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst. Rev. 10, 1–11 (2021).
Sterne, J. A. et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ 366, l4898 (2019).
Sterne, J. A. et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ 355, i4919 (2016).
Guyatt, G. et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 336, 924–6(2008).
Grade Working Group. GRADEpro GDT: GRADEpro Guideline Development Tool [Software]. McMaster University (developed by Evidence Prime, Inc.) 2015. gradepro.org. Accessed 10 Mar 2020.
Hoffmann, T. C. et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ 348, g1687 (2014).
DerSimonian, R. & Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 7, 177–188 (1986).
Higgins, J. P. & Thompson, S. G. Quantifying heterogeneity in a meta‐analysis. Stat. Med. 21, 1539–1558 (2002).
Burns, P. B., Rohrich, R. J. & Chung, K. C. The levels of evidence and their role in evidence-based medicine. Plast. Reconstr. Surg. 128, 305 (2011).
Sahariah, S. A. et al. A daily snack containing leafy green vegetables, fruit, and milk before and during pregnancy prevents gestational diabetes in a randomized, controlled trial in Mumbai, India. J. Nutr. 146, 1453S–1460S (2016).
Sun, L. & Niu, Z. A mushroom diet reduced the risk of pregnancy-induced hypertension and macrosomia: a randomized clinical trial. Food Nutr. Res. 64, PMC7286351 (2020).
LeBlanc, E. S., Smith, N. X., Vesco, K. K., Paul, I. M. & Stevens, V. J. Weight loss prior to pregnancy and subsequent gestational weight gain. Am J Obstet Gynecol. 224, 99–99.e14 (2021).
LeBlanc, E. S., Smith, N. X., Vesco, K. K., Hillier, T. A. & Stevens, V. J. Weight loss prior to pregnancy and early gestational glycemia: prepare, a randomized clinical trial. J. Clin. Endocrinol. Metab. 106, e5001–e5010 (2021).
Ainuddin, J. A., Kazi, S., Aftab, S. & Kamran, A. Metformin for preventing gestational diabetes in women with polycystic ovarian syndrome. J. College Physicians Surg. Pakistan 25, 237–241 (2015).
Abd El Hameed, A. A., Shreif, H. E. & Mowafy, H. E. The role of continuing metformin therapy during pregnancy in the reduction of gestational diabetes and improving pregnancy outcomes in women with polycystic ovary syndrome. Middle East Fertil. Soc. J. 16, 204–208 (2011).
Trak-Fellermeier, M. A. et al. PEARLS randomized lifestyle trial in pregnant Hispanic women with overweight/obesity: gestational weight gain and offspring birthweight. Diabetes Metab. Syndr. Obesity 12, 225 (2019).
Garmendia, M. L. et al. Effectiveness of a normative nutrition intervention in Chilean pregnant women on maternal and neonatal outcomes: the CHiMINCs study. Am. J. Clin. Nutr. 112, 991–1001 (2020).
Al Wattar, B. H., Dodds, J., Hooper, R., Khan, K. & Thangaratinam, S. Effects of Mediterranean-style diet in pregnancies with metabolic risk factors (ESTEEM): a pragmatic multicentre randomized trial. BJOG 125, 108 (2018).
Alamolhoda, S. H., Simbar, M., Mirmiran, P. & Mirabi, P. The effectiveness of low trans-fatty acids dietary pattern in pregnancy and the risk of gestational diabetes mellitus. Casp. J. Intern. Med. 10, 197–204 (2019).
Assaf-Balut, C. et al. A Mediterranean diet with additional extra virgin olive oil and pistachios reduces the incidence of gestational diabetes mellitus (GDM): a randomized controlled trial: The St. Carlos GDM prevention study. PLoS ONE 12, e0185873 (2017).
Basu, A. et al. Dietary blueberry and soluble fiber improve serum antioxidant and adipokine biomarkers and lipid peroxidation in pregnant women with obesity and at risk for gestational diabetes. Antioxidants 10, 22 (2021).
Jovanovic-Peterson, L., Bevier, W. & Peterson, C. M. The Santa Barbara County Health Care Services program: birth weight change concomitant with screening for and treatment of glucose-intolerance of pregnancy: a potential cost-effective intervention? Am. J. Perinatol. 14, 221–228 (1997).
Luoto, R., Laitinen, K., Nermes, M. & Isolauri, E. Impact of maternal probiotic-supplemented dietary counselling on pregnancy outcome and prenatal and postnatal growth: a double-blind, placebo-controlled study. Br. J. Nutr. 103, 1792–1799 (2010).
Xu, M.-Y., Guo, Y.-J., Zhang, L.-J. & Lu, Q.-B. Effect of individualized weight management intervention on excessive gestational weight gain and perinatal outcomes: a randomized controlled trial. PeerJ 10, e13067 (2022).
Mills, H. L. et al. The effect of a lifestyle intervention in obese pregnant women on gestational metabolic profiles: findings from the UK Pregnancies Better Eating and Activity Trial (UPBEAT) randomised controlled trial. BMC Med. 17, 1–12 (2019).
Liu, J. et al. A behavioral lifestyle intervention to limit gestational weight gain in pregnant women with overweight and obesity. Obesity 29, 672–680 (2021).
Liu, J., Wilcox, S., Whitaker, K., Blake, C. & Addy, C. Preventing excessive weight gain during pregnancy and promoting postpartum weight loss: a pilot lifestyle intervention for overweight and obese African American women. Matern. Child Health J. 19, 840–849 (2015).
Kennelly, M. A. et al. Pregnancy exercise and nutrition with smartphone application support: a randomized controlled trial. Obstet. Gynecol. 131, 818–826 (2018).
Herring, S. J. et al. Preventing excessive gestational weight gain among African American women: a randomized clinical trial. Obesity 24, 30–36 (2016).
Harrison, C. L., Lombard, C. B., Strauss, B. J. & Teede, H. J. Optimizing healthy gestational weight gain in women at high risk of gestational diabetes: a randomized controlled trial. Obesity 21, 904–909 (2013).
Gonzalez-Plaza, E. et al. Effectiveness of a step counter smartband and midwife counseling intervention on gestational weight gain and physical activity in pregnant women with obesity (Pas and Pes Study): randomized controlled trial. JMIR mHealth uHealth 10, e28886 (2022).
Barakat, R., Cordero, Y., Coteron, J., Luaces, M. & Montejo, R. Exercise during pregnancy improves maternal glucose screen at 24–28 weeks: a randomised controlled trial. Br. J. Sports Med. 46, 656–661 (2012).
Barakat, R., Pelaez, M., Lopez, C., Lucia, A. & Ruiz, J. R. Exercise during pregnancy and gestational diabetes-related adverse effects: a randomised controlled trial. Br. J. Sports Med. 47, 630–636 (2013).
Cordero, Y., Mottola, M. F., Vargas, J., Blanco, M. & Barakat, R. Exercise is associated with a reduction in gestational diabetes mellitus. Med. Sci. Sports Exerc. 47, 1328 (2015).
Barakat, R., Refoyo, I., Coteron, J. & Franco, E. Exercise during pregnancy has a preventative effect on excessive maternal weight gain and gestational diabetes. A randomized controlled trial. Braz. J. Phys. Ther. 23, 148–155 (2019).
Buckingham-Schutt, L. M., Ellingson, L. D., Vazou, S. & Campbell, C. G. The Behavioral Wellness in Pregnancy study: a randomized controlled trial of a multi-component intervention to promote appropriate weight gain. Am. J. Clin. Nutr. 109, 1071–1079 (2019).
Chan, R. S. et al. Randomized trial examining effectiveness of lifestyle intervention in reducing gestational diabetes in high risk Chinese pregnant women in Hong Kong. Sci. Rep. 8, 13849 (2018).
Eslami, E., Mohammad Alizadeh Charandabi, S., Khalili, A. F., Jafarabadi, M. A. & Mirghafourvand, M. The effect of a lifestyle-based training package on weight gain and frequency of gestational diabetes in obese and overweight pregnant females. Iran. Red Crescent Med. J. 20, https://doi.org/10.5812/ircmj.62576 (2018).
Gregory, E. F., Goldshore, M. A., Henderson, J. L., Weatherford, R. D. & Showell, N. N. Infant growth following maternal participation in a gestational weight management intervention. Child Obes. 12, 219–225 (2016).
Harrison, C. L., Lombard, C. B., Strauss, B. J. & Teede, H. J. Optimizing healthy gestational weight gain in women at high risk of gestational diabetes: a randomized controlled trial. Obesity (Silver Spring) 21, 904–909 (2013).
Hui, A. L. et al. Effects of lifestyle intervention on dietary intake, physical activity level, and gestational weight gain in pregnant women with different pre-pregnancy Body Mass Index in a randomized control trial. BMC Pregnancy Childbirth 14, 331 (2014).
LeBlanc, E. S., Smith, N. X., Vesco, K. K., Paul, I. M. & Stevens, V. J. Weight loss prior to pregnancy and subsequent gestational weight gain: prepare, a randomized clinical trial. Am. J. Obstet. Gynecol. 224, 99.e91–99.e14 (2021).
Luoto, R. et al. Primary prevention of gestational diabetes mellitus and large-for-gestational-age newborns by lifestyle counseling: a cluster-randomized controlled trial. PLoS Med. 8, https://doi.org/10.1371/journal.pmed.1001036 (2011).
Simmons, D. et al. Effect of physical activity and/or healthy eating on GDM risk: the DALI Lifestyle study. J. Clin. Endocrinol. Metab. 102, 903–913 (2017).
Zhao, H. et al. Influence of gestational hypertension on cardiovascular health behaviors and factors. Comput. Intell. Neurosci. 2022, 1031418 (2022).
Dodd, J. M. et al. Effect of metformin in addition to dietary and lifestyle advice for pregnant women who are overweight or obese: the GRoW randomised, double-blind, placebo-controlled trial. Lancet Diabetes Endocrinol. 7, 15–24 (2019).
Løvvik, T. S. et al. Use of metformin to treat pregnant women with polycystic ovary syndrome (PregMet2): a randomised, double-blind, placebo-controlled trial. Lancet Diabetes Endocrinol. 7, 256–266 (2019).
Syngelaki, A. et al. Metformin versus placebo in obese pregnant women without diabetes mellitus. N. Engl. J. Med. 374, 434–443 (2016).
Chiswick, C. et al. Effect of metformin on maternal and fetal outcomes in obese pregnant women (EMPOWaR): a randomised, double-blind, placebo-controlled trial. Lancet Diabetes Endocrinol. 3, 778–786 (2015).
Pellonperä, O. et al. Efficacy of fish oil and/or probiotic intervention on the incidence of gestational diabetes mellitus in an at-risk group of overweight and obese women: a randomized, placebo-controlled, double-blind clinical trial. Diabetes Care 42, 1009–1017 (2019).
Lindsay, K. L. et al. Probiotics in obese pregnancy do not reduce maternal fasting glucose: a double-blind, placebo-controlled, randomized trial (Probiotics in Pregnancy Study). Am. J. Clin. Nutr. 99, 1432–1439 (2014).
Callaway, L. K. et al. Probiotics for the prevention of gestational diabetes mellitus in overweight and obese women: findings from the SPRING double-blind randomized controlled trial. Diabetes Care 42, 364–371 (2019).
D’Anna, R. et al. Myo-inositol supplementation for prevention of gestational diabetes in obese pregnant women: a randomized controlled trial. Obstet. Gynecol. 126, 310–315 (2015).
Celentano, C. et al. The influence of different inositol stereoisomers supplementation in pregnancy on maternal gestational diabetes mellitus and fetal outcomes in high-risk patients: a randomized controlled trial. J. Matern.–Fetal Neonatal Med. 33, 743–751 (2020).
D’Anna, R. et al. myo-Inositol supplementation and onset of gestational diabetes mellitus in pregnant women with a family history of type 2 diabetes: a prospective, randomized, placebo-controlled study. Diabetes Care 36, 854–857 (2013).
Farren, M. et al. The prevention of gestational diabetes mellitus with antenatal oral inositol supplementation: a randomized controlled trial. Diabetes Care 40, 759–763 (2017).
Matarrelli, B. et al. Effect of dietary myo-inositol supplementation in pregnancy on the incidence of maternal gestational diabetes mellitus and fetal outcomes: a randomized controlled trial. J. Matern.-Fetal Neonatal Med. 26, 967–972 (2013).
Santamaria, A. et al. Myo-inositol may prevent gestational diabetes onset in overweight women: a randomized, controlled trial. J. Matern.-Fetal Neonatal Med. 29, 3234–3237 (2016).
Wickens, K. L. et al. Early pregnancy probiotic supplementation with Lactobacillus rhamnosus HN001 may reduce the prevalence of gestational diabetes mellitus: a randomised controlled trial. Br. J. Nutr. 117, 804–813 (2017).
Martínez‐Vizcaíno, V. et al. Exercise during pregnancy for preventing gestational diabetes mellitus and hypertensive disorders: an umbrella review of randomised controlled trials and an updated meta‐analysis. BJOG 130, 264–275 (2023).
Griffith, R. J. et al. Interventions to prevent women from developing gestational diabetes mellitus: an overview of Cochrane Reviews. Cochrane Database Syst. Rev. 6, Cd012394(2020).
Lim, S. et al. Participant characteristics in the prevention of gestational diabetes as evidence for precision medicine: a systematic review and meta-analysis. Commun. Med. 3, 137 (2023).
de Castro, R., Antunes, R., Mendes, D., Szumilewicz, A. & Santos-Rocha, R. Can group exercise programs improve health outcomes in pregnant women? An updated systematic review. Int. J. Environ. Res. Public Health 19, 4875 (2022).
Cradock, K. A. et al. Behaviour change techniques targeting both diet and physical activity in type 2 diabetes: a systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 14, 1–17 (2017).
Nicolaï, S. et al. Supervised exercise versus non-supervised exercise for reducing weight in obese adults. J. Sports Med. Phys. Fit. 49, 85 (2009).
Payne, J. A. Group learning for adults with disabilities or chronic disease. Rehabil. Nurs. 20, 268–272 (1995).
Borek, A. J., Abraham, C., Greaves, C. J. & Tarrant, M. Group‐based diet and physical activity weight‐loss interventions: a systematic review and meta‐analysis of randomised controlled trials. Appl. Psychol.: Health Well‐Being 10, 62–86 (2018).
Befort, C. A., Donnelly, J. E., Sullivan, D. K., Ellerbeck, E. F. & Perri, M. G. Group versus individual phone-based obesity treatment for rural women. Eat. Behav. 11, 11–17 (2010).
Paul-Ebhohimhen, V. & Avenell, A. A systematic review of the effectiveness of group versus individual treatments for adult obesity. Obes. Facts 2, 17–24 (2009).
Lawler, M., Heary, C. & Nixon, E. Peer support and role modelling predict physical activity change among adolescents over twelve months. J. Youth Adolesc. 49, 1503–1516 (2020).
Lazar, J., Boned-Rico, L., Olander, E. K. & McCourt, C. A systematic review of providers’ experiences of facilitating group antenatal care. Reprod. Health 18, 1–21 (2021).
Plesh, C. R., Withers, R. A. & Skelton, D. A. Women’s perceptions or experiences of physical activity and exercise interventions to improve bone health: a systematic review. J. Frailty Sarcopenia Falls 8, 94–106 (2023).
Bennett, G., King, N., Redfern, K. & Breese, B. Supervised physical activity and the incidence of gestational diabetes mellitus: a systematic review and meta-analysis. J. Matern.-Fetal Neonatal Med. 36, 1–9 (2022).
Buffart, L. M. et al. Effects and moderators of exercise on quality of life and physical function in patients with cancer: an individual patient data meta-analysis of 34 RCTs. Cancer Treat. Rev. 52, 91–104 (2017).
Nascimento, S., Pudwell, J., Surita, F., Adamo, K. & Smith, G. The effect of physical exercise strategies on weight loss in postpartum women: a systematic review and meta-analysis. Int. J. Obes. 38, 626–635 (2014).
Rosas, L. G. et al. Preferences for technology-mediated behavioral lifestyle interventions with different levels of coach and peer support among Latino men: comparative study within one arm of a randomized controlled trial. JMIR Form. Res. 6, e29537 (2022).
Jones, E. J., Fraley, H. E. & Mazzawi, J. Appreciating recent motherhood and culture: a systematic review of multimodal postpartum lifestyle interventions to reduce diabetes risk in women with prior gestational diabetes. Matern. Child Health J. 21, 45–57 (2017).
Østbye, T. et al. Active Mothers Postpartum: a randomized controlled weight-loss intervention trial. Am. J. Prev. Med. 37, 173–180 (2009).
Sagastume, D. et al. The effectiveness of lifestyle interventions on type 2 diabetes and gestational diabetes incidence and cardiometabolic outcomes: a systematic review and meta-analysis of evidence from low-and middle-income countries. EClinicalMedicine 53, 101650 (2022).
International Diabetes Federation. IDF Diabetes Atlas 10th edn. 2021 (International Diabetes Federation, accessed 21 March 2023); https://diabetesatlas.org/data/en/.
Kocanda, L. et al. The effectiveness of randomized controlled trials to improve dietary intake in the context of cardiovascular disease prevention and management in rural communities: a systematic review. J. Acad. Nutr. Diet. 121, 2046–2070.e2041 (2021).
Acknowledgements
The ADA/EASD Precision Diabetes Medicine Initiative, within which this work was conducted, has received the following support: The Covidence license was funded by Lund University (Sweden), for which technical support was provided by Maria Björklund and Krister Aronsson (Faculty of Medicine Library, Lund University, Sweden). Administrative support was provided by Lund University (Malmö, Sweden), the University of Chicago (IL, USA), and the American Diabetes Association (Washington D.C., USA). The Novo Nordisk Foundation (Hellerup, Denmark) provided grant support for in-person writing group meetings (PI: L Phillipson, University of Chicago, IL) (NNF22SA0081670).SL is funded by the Australian National Health and Medical Research Council (NHMRC) Fellowship (APP1139481). JW is funded by the NHMRC Ideas Grant. WT, MC, and GU were funded by the Australian Government Research Training Program Scholarship. LR is funded by the National Institute of Health (5R01DK124806). We are highly indebted to extend our gratitude to the authors of primary studies for responding to our data enquiries. Finally, librarians from Monash University are also appreciated for their support during accessing freely available studies.
Author information
Authors and Affiliations
Consortia
Contributions
SL, JJ, LR, KV conceptualised the research question. AF contributed to the search of the articles. SL, MC, JG, NH, LR, JJ, KV, WWT, KL, GGU, SC screened the articles, JG, NH, WWT, GGU, GL, NH, JG, SJZ, RT, MP, KL, MB, EGM, AQ, WH extracted the data and appraised the studies. WWT and SL coded the intervention characteristics and analysed the data. WWT drafted the manuscript. All authors have revised and approved the final version of the manuscript and agreed to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Competing interest
The authors declare no competing interests.
Peer review
Peer review information
Communications Medicine thanks Shuyuan Huang and Jess Harding for their contribution to the peer review of this work. A peer review file is available
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Takele, W.W., Vesco, K.K., Josefson, J. et al. Effective interventions in preventing gestational diabetes mellitus: A systematic review and meta-analysis. Commun Med 4, 75 (2024). https://doi.org/10.1038/s43856-024-00491-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s43856-024-00491-1
