
Abstract
The COVID-19 pandemic has highlighted the urgent need to address vaccine coverage inequality. Despite calls from scientists and national organizations, progress in ensuring equitable access to vaccines has been slow. This study aims to reveal the COVID-19 vaccine coverage inequality and investigate the predictive effect of attitudes toward science and religion on real-word vaccination uptake. We draw on three high-quality, large-scale databases to unveil real-world vaccine coverage, which stood at an average of 53% of the population by mid-2022. The vaccination rate varies based on a country’s income, with higher-income nations having higher vaccination rates and faster vaccination speed. Regression models and a multiverse analysis reveal that both country-level attitudes towards science and religion, as well as religious faith, are linked to vaccination rate at the country level. Countries where a higher proportion of the population prioritize religious beliefs over scientific evidence when the two come into conflict tend to have lower vaccination coverage rates and slower vaccination speeds. These findings suggest that scientists and policymakers must take into account social and cultural characteristics of populations when addressing vaccine inequality.
Similar content being viewed by others

Introduction
Vaccinations play a crucial role in combating the coronavirus disease, i.e., the COVID-19 (Chen et al. 2022; Price et al. 2022; Watson et al. 2022). It is a crucial tool to minimize the magnitude of negative effects caused by the pandemic. Yet, COVID-19 vaccine allocation and uptake around the world is notably unequal, in that high-income countries gain remarkably more vaccine doses than low-income countries (Asundi et al. 2021; Burki 2021). Vaccine coverage is predominantly constrained by vaccine supply and allocation, with substantial efforts focused on augmenting vaccine availability in low-income countries (World Health Organization 2023). Conversely, certain social-cultural factors, such as societal norms, beliefs, and religious influences related to vaccination, are frequently underemphasized in addressing the vaccine inequality challenge. However, these factors consistently wield a significant influence on vaccine uptake. In a representative-sample survey study in 2020, for example, researchers found that nearly one-third of the population of Ireland and the UK were hesitant or resistant to accept a vaccine (Murphy et al. 2021). In the current study, we focus on people’s attitudes toward science and religion. They serve as fundamental principles that guide individuals in their vaccination decisions, yet they are frequently overlooked as contributors to variations in vaccine coverage across different countries.
Evidence has shown that trust or distrust of science is associated with hesitancy and uptake of a vaccine. A study using survey data from 2017 and 2019, which involved thousands of participants in Italy, revealed that people with stronger trust in the science community would evaluate a vaccine more positively (Cadeddu et al. 2021). Another recent study conducted in New Zealand, which included over 1,300 community participants, found that distrust of science could predict lower vaccine intention, and moreover, could exacerbate the negative effect of political beliefs on vaccine uptake (Winter et al. 2022). Some large-sample survey studies involving multiple-country data collection have also shown a consistently predictive effect of trust in science on vaccine hesitancy (e.g., Lazarus et al. 2022; Sturgis et al. 2021). Indeed, looking at the history of anti-vaccine movements and some worrisome casesof vaccine hesitancy, distrust in science and denial of mainstream scientific evidence about vaccines constitute one of the most important motivations for refusing vaccination (Kabat, 2017; Larson et al. 2022; Pertwee et al. 2022; Rutjens et al. 2021). Nevertheless, it remains unknown whether differences in science trust across countries could explain the differences in vaccination rates at the country level.
On the other hand, stronger religious faith is related to lower vaccination uptake. Firstly, due to the psychological benefits of religion and spiritual beliefs (Weber & Pargament 2014), it is not surprising that religious people often turned to their beliefs instead of scientific measures for psychological relief during the pandemic crisis. Secondly, sometimes people deny the scientific evidence of vaccines and refuse or delay vaccination because they think vaccination violates the teaching of their religion and challenges the will of God (Galang 2021; Garcia & Yap 2021; Hatala et al. 2022). In a qualitative case study conducted in 2018, participants from a church community said the HIV vaccine for adolescents could destroy the abstinence norm, and thus deviated from their religious teachings (Lahijani et al. 2021). Another survey study, which recruited nearly 2,000 American participants in 2021, found that Christian nationalism (the degree to which participants think the US should be declared a Christian nation) was the most important predictor of COVID-19 vaccine hesitancy (Corcoran et al. 2021). This is similar to a more recent study that showed people with stronger belief in God held more mistrust of the COVID-19 vaccine (Upenieks et al. 2022).
Although science and religion are not always opposed (e.g., Eriksson & Vartanova 2022), tension between them under the vaccination challenge is clear. Importantly, we argue that trust in science versus in religious faith could explain vaccination inequality across countries, not only because they could predict vaccine attitudes and decisions at individual level, but also because countries are different in terms of science trust and religious faith. According to a recent world survey, for example, only 14% of participants in China said they belonged to some religious denomination, while this number rose to 55.8% in the US and 98.8% in Turkey (EVS/WVS 2021).
In the current study, we used data from several high-quality public datasets to describe the remarkable fact of global vaccine coverage inequality and examine whether trust in science, religious faith and science-religion choice are associated with it. The term “science-religion choice” used in this study refers to the preference individuals have for either science or religion when the two are in conflict (see the “Method” section for the original measure question), and it serves as a pivotal gauge of an individual’s stance on the relationship between science and religion.
The data of vaccine coverage are from Our World in Data, the OWID (Mathieu et al. 2021). OWID COVID-19 database tracks daily vaccination information based on official, verifiable public sources from over 200 countries. It records the number of people vaccinated per hundred of the population (i.e., people who received at least one vaccine dose) and people fully vaccinated per hundred of the population (i.e., people who received all vaccine doses) by area during the last two years, which allows us to capture the pattern. We chose data recorded before 1 July 2022 to represent the COVID-19 vaccine uptake status until the middle of 2022, the time set for achieving the World Health Organization’s goal of a 70% vaccination rate (World Health Organization 2021). On the other hand, data on science trust and science-religion choice was obtained from the 2018 Wellcome Global Monitor (WGM 2018; Wellcome Trust, The Gallup Organization Ltd, 2019) and 2017–2022 World Values Survey Wave 7 (WVS Wave 7; Haerpfer et al. 2022). These two large-scale programs surveyed science and religion attitude among people around the world in recent years.
For the daily-updated OWID database, we chosen data up to 1 July 2022 and depicted the patterns of people vaccinated per hundred and people fully vaccinated per hundred. Specifically, the maximum values in different areas on these two variables, normally the exact values at 1July 2022 or very close to the day, were selected as a representation of the latest COVID-19 vaccine uptake status in the middle of 2022.
In addition, to facilitate understanding of vaccination coverage inequality between countries with different levels of income, we adopted the latest country classification from the World Bank database (World Bank 2022), in which countries were categorized into four types based on income. Countries within the OWID database but outside the World Bank country classification were excluded, which left 214 countries covering 99% of the world population for further analyses.
Results
Global vaccination rate and coverage inequality
The global average of people fully vaccinated per hundred in over 200 countries is 52.60 (SD = 26.42), which indicates that, at country level, nearly half of the population had still not been proactively immunized against SARS-CoV-2 by mid-2022. Nevertheless, at population level, 61.21% of the global population had been fully vaccinated. However, this is still much lower than the WHO’s objective: 70% by the middle of 2022 (World Health Organization 2021). The global average of people who had received at least one vaccine dose per hundred is 57.42 (SD = 26.49) at country level and 66.75% at population level.
Vaccine coverage varied a lot across countries, as shown in Fig. 1. Most countries in West and South Asia, Eastern Europe, Central America, and especially Africa (areas where low-income countries are usually aggregated) were notably lower on vaccination coverage than other countries. In addition, low-income countries had been much slower on vaccine uptake practices during 2020–2022. Figure 2 provides a rough estimate for the time series trend of vaccine uptake in terms of country income. As we can see, high-income countries have an earlier start in vaccine practice and vaccinate people drastically faster than low-income countries, and the gap continues to magnify over time.

Dark blue countries represent a higher percentage of fully vaccinated people per hundred of the population, while black areas indicate regions with no available data.

The values were calculated as the daily average of the number of people vaccinated per hundred (on the left) and the number of people fully vaccinated per hundred (on the right) for countries of different income categories.
We arranged all the countries by their vaccination coverage and showed the top and last 20 countries in Fig. 3. Top 20 countries such as Singapore (91.61%), China (88.40%), and Spain (85.42%) have already exceeded 80% an vaccination coverage rate, while the last 20 countries, such as Sudan (9.94%), Haiti (1.37%), and Burundi (0.12%) progressed slowly.

The blue and khaki bars represent number of people vaccinated per hundred in each country, while the black bars inside them indicate the number of people fully vaccinated per hundred in each country. The red line represents the global average of people fully vaccinated per hundred at the country level.
It is reasonable to suspect that the tremendous inequality of vaccination coverage may have been caused by the diversity in early vaccine supply ability, when some countries lagged in the initial promotion of vaccines. These may have risen rapidly after the supply problem had been solved. Given this, we calculated the daily growth of people fully vaccinated per hundred in these countries as an index of vaccination coverage speed. We found that top 50 countries were larger than the last 50 countries on vaccination coverage speed, Mtop50 = 0.19 (SD = 0.14), Mlast50 = 0.04 (SD = 0.02), Welch’t (51.51) = 7.80, p < 0.001; Cohen’d = 2.17, 95%CI = (1.48, 2.85); BF10 = 20.66. This suggests significantly faster vaccination progress in the top 50 countries than in the last 50 countries, beyond the huge gap in current vaccination coverage rate. Moreover, the difference was still large when we compared the last 50 countries at their speeds in 2022 (M = 0.04, SD = 0.03) with the top 50 countries at the initial speed before July 2021 (M = 0.24, SD = 0.19), Welch’t (46.14) = 6.82, p < 0.001; Cohen’d = 2.01, 95%CI = (1.29, 2.71); BF10 = 16.24. For people vaccinated per hundred, the results are similar. This simply implies that after broad endeavors on breaking the vaccine supply barrier (World Health Organization 2023), countries currently at low levels of vaccination coverage are still left far behind, even at the speed of recent vaccination progress, compared to the initial speed of current high-coverage countries. These results, combined with information from the trend line in Fig. 2, reveal a unique type of vaccine inequality that researchers tend to neglect. Apparently, income or vaccine-supply capacity is not the only factor in vaccine coverage inequality.
Prediction of vaccine inequality using science-religion choice
WGM 2018 collected data from 144 countries, including variables of science trust and science-religion choice, while another data set, WVS wave 7, surveyed people from 57 countries about religious faith and science-religion choice. We first ran regression models based on the common part of these two data sets, science-religion choice, and discussed science trust and religious faith later.
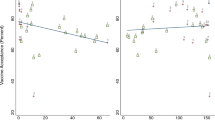
Figure 4 displays four scatter plots that demonstrate a negative association between science-religion choice and vaccination coverage. To simplify it, we recoded World Bank country income classification into two types: high or upper middle income and low or lower middle income. No matter their income types, countries with more people who choose religion when science conflicts with it are lower on vaccination coverage and slower on vaccination speed.

Subgraphs A and B use science-religion choice data from WGM 2018 dataset, while C and D utilize the same variable from WVS Wave 7 dataset. Each data point represents a country.
Next, standardized variables were entered into several ordinary least square regression (OLS) models. (See Table 1). Given the similarity and high correlation between people vaccinated per hundred and people fully vaccinated per hundred, we focused on the latter one as our dependent variable of vaccination coverage. Vaccination speed was also included as an outcome.
The result of model 1a reveals that science-religion choice (from WGM 2018) can predict vaccination coverage, β = −0.526, p < 0.001, suggesting that countries with more people choosing religion rather than science are lower on amount of people fully vaccinated. However, the relationship is not significant after covariables are considered, β = −0.085, p = 0.444. Model 1c and 1d continue the same pattern for vaccination speed, where science-religion choice predicts vaccination speed, β = −0.417, p < 0.001, and fails the prediction with covariables, β = −0.077, p = 0.565.
By contrast, with science-religion choice data obtained from WVS wave 7, more people choosing religion is always associated with both lower vaccination coverage and lower vaccination speed at country level, whether covariables are in the regression models or not (see Table 1).
To reduce the impact of variable-selection processes on statistical conclusion, we subsequently conducted a multiverse analysis and plotted a specification curve for all analytic decisions (Simonsohn et al. 2020; Steegen et al. 2016). One of the advantages of multiverse analysis is that researchers can present all results based on different analytic decisions. In our statistical model, numerous factors can be taken into consideration, including the number of covariates, the choice of the statistical model, the database from which the predictor variables are sourced, and the index of dependent variable. Any changes in these factors can potentially yield different results. Multiverse analysis allows us to avoid selective reporting and present the results of all plausible models.
We identified four major data analytic decisions, including which index to use as outcome (i.e., vaccination coverage or vaccination speed, two options), which predictor to be included (i.e., science-religion choice from WGM 2018 or WVS wave 7, two options), what regression model to run (i.e., robust regression or OLS, two options), and how many as well as which of the seven covariables should be considered (including no covariable, one hundred twenty-eight options).
In total, we obtained 1,024 ( = 2*2*2*128) plausible model specifications in the multiverse analysis. We focused on the regression coefficient of the predictor on outcome in each specification. Of all specifications, 77.44% obtained a coefficient significantly lower than zero. The median coefficient is β = −0.458. Figure 5 displays the details of the results from the specification curve analysis (Simonsohn et al. 2020), produced by R package “specr” (Masur and Scharkow 2020).

In subgraph A, the red section of the curve, represents significant specifications, consisting of point estimates of the standardized coefficients of the focal predictor in different specifications, enclosed by 95% confidence intervals (shown as the gray ribbon). The red dotted line signifies the median of the estimates. In subgraph B, we have displayed only the predictors, outcomes and regression models, omitting the combinations of covariables due to potential length constraints in the plot. Robust regression was performed using M-type estimator from an R package “robustbase” (Maechler et al. 2021). Subgraph C illustrates the sample size corresponding to each specification.
These results provide confidence for the robustness of our statistical conclusion. Overall, we found that science-religion choice is negatively linked with two different vaccination inequality indices. Countries with more people choosing religion rather than science are lower on vaccination coverage and vaccination speed.
Analysis of science trust and religious faith
Another two science-religion related variables, science trust from WGM 2018 and religious faith from WVS wave 7, were treated as additional focal predictors. Table 2 displays the regression model results. Science trust could predict vaccination coverage and vaccination speed only if covariables were excluded. By comparison, religious faith could always show predictive effect.
Although science trust is not a stable predictor of vaccination inequality, the information in Table 2 is still apparent: to some extent, the more trust a country puts in science, the higher coverage and speed of vaccination present, while the stronger religious faith is, the lower coverage and speed of vaccination appear. This is conceptually compatible with what we have found from models with science-religion choice as the predictor.
Discussion
Vaccine inequality is a widespread reality that could hinder the world’s full recovery from the impact of COVID-19. It poses the ongoing risk of viral mutations and multiple infections in the global population, worsens economic inequality, and further imperils vulnerable groups, including women and children (Asundi et al. 2021). Because of many international efforts to promote vaccine cooperation and increasing vaccine supply in low-income countries, the supply problem could be removed from the main factors affecting vaccination coverage. By contrast, social-cultural characteristics, which were proved to have powerful influence on personnel attitude and behavior towards vaccination (Browne et al. 2015; de Figueiredo et al. 2020; Murphy et al. 2021), could dominate when accounting for vaccine inequality. It is time to consider why people are unwilling to get vaccinated rather than how to promote vaccine supply. In the current study, we showed that country-level science-religion-related variables, including science trust, religious faith, and science-religion choice, are closely linked with real-world vaccination coverage.
Specifically, countries with higher scores of aggregated science trust are also higher on COVID-19 vaccine coverage, although the relationship between them does not seem as robust as expected. Yet, at individual level, trust in science was shown to to have a positive effect on vaccination behaviors, such as vaccine confidence and vaccination intention (Sturgis et al. 2021; Winter et al. 2022). The incompatibility between evidence showed here and in previous studies may indicate that a macro level of real-world vaccine uptake could be more complicated and determined by various factors associated with science other than country-level science trust; these are still ambiguous and call for more future research.
On the contrary, science-religion choice and religious faith are more robustly linked with vaccine uptake. Whether other variables being controlled or not, and no matter which database, science-religion choice and religious faith are always a successful predictor of current global vaccination coverage and its speed. However, it is worth noting that even if religious faith was thought to increase vaccine hesitancy (Lahijani et al. 2021), religious effects could be complex because teachings of religion vary by denominations (Alhawari et al. 2020; Morrison et al. 2015). For example, studies have found that people from different religious denominations were inconsistent on vaccine uptake (Trepanowski & Drążkowski, 2022), and the relationship between religious faith and vaccination intention might exhibit an inverted U-shaped pattern in some countries(Lahav et al. 2022). Hence, the impact of religious faith on vaccination uptake warrants further rigorous examination. For the issue of science-religion tension, we believe science-religion choice could be a better indicator:countries with more people who trust religion when science conflicts with it are lower on vaccination coverage and slower on vaccination speed.
While in general, religious beliefs are predictive of lower vaccination rates, the support for vaccines within religious faiths may mitigate this effect. For example, Christian and Islamic leaders have publicly supported the COVID-19 vaccine, viewing vaccine uptake as a way to align with their religious doctrines (Hsu, 2021; Mardian et al. 2021). As a result, endorsements from religious authorities can enhance vaccination intentions(Chu et al. 2021). Therefore, it is worth to note that the relationship between religious faith, trust in science, and vaccination uptake is intricate. While we can derive a rough predictive coefficient, the interplay of these three, both on an individual level and a national level, along with numerous other social-cultural characteristics, suggests that their true dynamics transcend the simple linear models described in this paper. Instead, they exist within the domain of higher-order interactions, where their intricate interdependence eludes simple explanation. Future research may employ innovative methods to elucidate the more precise dynamics governing these relationships (e.g., Battiston et al. 2020; Nie et al. 2022).
Overall, global vaccine inequality is was still severe as of mid-2022. We argue that more attention needs to be paid to countries’ social-cultural characteristics that may influence vaccine uptake, and more factors that are feasible for forming an intervention must be identified. In our study, science-religion-related variables could explain part of the inequality. This could provide valuable insights in the battle against COVID-19. For instance, in countries with a stronger religious faith, the acceptance of vaccines might rely on the notion that vaccination aligns with religious beliefs, and religious authorities could play a role in explaining how vaccination aligns with religious doctrine. In the future, further investment in scientific education should be considered if it is shown to enhance the likelihood of choosing science in the face of potential conflicts between science and religion. Vaccination rates are important for ending the pandemic, and now we need move forwards.
Materials and Methods
Globle vaccination data are from Our World in Data (OWID; Mathieu et al. 2021). Vaccination coverage was defined by the recorded maximum of people fully vaccinated per hundred in every country. Daily growth of vaccination coverage, or the index of vaccination speed, was calculated as the difference between the maximum and minimum divided by their day interval. For example, if people fully vaccinated per hundred of “A” country is 1,5,8 and 13 for Days 2, 7, 20, and 50, the current vaccination coverage of “A” country is 13 (the maximum value) and the vaccination speed is (13-1)/(50-2) = 0.25. Only values larger than zero involved calculation, as they are valid records of vaccination progress. The records in Gibraltar, the United Arab Emirates, Samoa and Tonga that exceed 100 were recoded as 100.
According to World Bank (World Bank, 2022), the latest income type of country is determined by their GNI per capita in 2021, “$1,805 or less” for low-income economies, “between $1,086 and $4,255” for lower middle-income economies, “between $4,256 and $13,205” for upper middle-income economies and “$13,205 or more” for high-income economies. Countries within the OWID database but outside the World Bank country classification were excluded.
The data on science trust, religious faith and science-religion choice was obtained from the 2018 Wellcome Global Monitor (WGM 2018; Wellcome Trust, The Gallup Organization Ltd 2019) and 2017–2022 World Values Survey Wave 7 (WVS Wave 7; EVS/WVS 2021). WGM 2018 surveyed science trust with the item, “In general, would you say that you trust science a lot, some, not much, or not at all?” and the science-religion choice with the item, “Generally speaking, when science disagrees with the teachings of your religion, what do you believe? Science or the teachings of your religion?” Responses were averaged after excluding other options (such as “don’t know” and “refused”) at the country level; therefore, we were able to obtain the science trust and science-religion choice for every country. In addition, WVS wave 7 provides two measures about religious faith and science-religion choice. Religious faith was determined by four items: people’s beliefs in God, life after death, hell, and heaven. These items, with Cronbach’s α = 0.868 and McDonald’s ω = 0.881, were first summed at individual level and then averaged at country level. Science-religion choice was based on a single question, “Please tell us if you strongly agree, agree, disagree, or strongly disagree with the following statements: Whenever science and religion conflict, religion is always right.” In summary, higher country-level score means stronger science trust, strong religious faith and more tendency toward religious choice. The idea here is simple: if a country has more people evaluating science to be more trustworthy, the country should be more pro-science; or if it has more people who select religion rather than science, or has more people holding stronger religious faith, it should be more pro-religion.
In addition, some country characteristics were included as covariables in our regression models. The policy stringency index (“stringency index”) was derived by OWID from the Oxford COVID-19 Government Response Tracker, which involves indicators such as travel bans and workplace closures. We used the mean stringency index of all records to represent the evaluation of a country’s average pandemic policy stringency. Poverty data was from the OWID database, which represents the share of the population living in extreme poverty. GDP was also was provided by OWID. Please note that data for both Poverty and GDP are constant values in every country each day. Government trust and vaccine trust are present within WGM 2018. Government trust was defined by asking, “How much do you trust the national government in this country?” Vaccine trust was measured by two items: people’s evaluation of the statements, “Vaccines are safe” and “Vaccines are effective”. The correlation of the two items is r = 0.58, p < 0.001, 95%CI = (0.58, 0.59). They were first combined at individual level and second at country level. Data on aging and population density, both from OWID, indicate the proportion of people older than 65 and the number of people divided by land area.
To organize data from the different databases, WGM 2018 and WVS wave 7 were respectively combined with OWID data by matching country names or ISO country code. There are some cases in which different names for a country were used in the three databases, such as “Palestine” in OWID as opposed to “Palestinian Territories” in WGM 2018, and “MOR” in WVS wave 7 as opposed to “MAR” in OWID (both refer to Morocco). We tried our best to deal with such impediments, see our analytic codes for details. For China, the mainland, Hong Kong, Macao, and Taiwan were calculated separately. The name “China” used in this study denotes the mainland China.
Data availability
All data and codes are available at: https://osf.io/e5vp2.
References
Alhawari Y, Verhoff MA, Ackermann H, Parzeller M (2020) Religious denomination influencing attitudes towards brain death, organ transplantation and autopsy—A survey among people of different religions. Int J Leg Med 134(3):1203–1212. https://doi.org/10.1007/s00414-019-02130-0
Asundi A, O’Leary C, Bhadelia N (2021) Global COVID-19 vaccine inequity: The scope, the impact, and the challenges. Cell Host Microbe 29(7):1036–1039. https://doi.org/10.1016/j.chom.2021.06.007
Battiston F, Cencetti G, Iacopini I, Latora V, Lucas M, Patania A, Young J-G, Petri G (2020) Networks beyond pairwise interactions: Structure and dynamics. Phys Rep. 874:1–92. https://doi.org/10.1016/j.physrep.2020.05.004
Browne M, Thomson P, Rockloff MJ, Pennycook G (2015) Going against the Herd: Psychological and Cultural Factors Underlying the ‘Vaccination Confidence Gap. PLoS ONE 10(9):e0132562. https://doi.org/10.1371/journal.pone.0132562
Burki T (2021) Global COVID-19 vaccine inequity. Lancet Infect Dis 21(7):922–923
Cadeddu C, Sapienza M, Castagna C, Regazzi L, Paladini A, Ricciardi W, Rosano A (2021) Vaccine Hesitancy and Trust in the Scientific Community in Italy: Comparative Analysis from Two Recent Surveys. Vaccines 9(10):1206. https://doi.org/10.3390/vaccines9101206
Chen X, Huang H, Ju J, Sun R, Zhang J (2022) Impact of vaccination on the COVID-19 pandemic in U.S. states. Sci Rep. 12(1):1. https://doi.org/10.1038/s41598-022-05498-z. Article
Chu J, Pink SL, Willer R (2021) Religious identity cues increase vaccination intentions and trust in medical experts among American Christians. Proc Natl Acad Sci 118(49):e2106481118. https://doi.org/10.1073/pnas.2106481118
Corcoran KE, Scheitle CP, DiGregorio BD (2021) Christian Nationalism and COVID-19 Vaccine Hesitancy and Uptake. Vaccine. https://doi.org/10.1016/j.vaccine.2021.09.074
de Figueiredo A, Simas C, Karafillakis E, Paterson P, Larson HJ (2020) Mapping global trends in vaccine confidence and investigating barriers to vaccine uptake: A large-scale retrospective temporal modelling study. Lancet 396(10255):898–908. https://doi.org/10.1016/S0140-6736(20)31558-0
Eriksson K, Vartanova I (2022) Vaccine confidence is higher in more religious countries. Hum Vaccines Immunotherapeutics 18(1):1–3. https://doi.org/10.1080/21645515.2021.1883389
EVS/WVS (2021) European Values Study and World Values Survey: Joint EVS/WVS 2017-2021 Dataset—Variable Report (Documentation/Tables). Version: July 2021 (v.2). GESIS Data Archive, Cologne and JD Systems Institute, Madrid
Galang JRF (2021) Science and religion for COVID-19 vaccine promotion. J Public Health, fdab128. https://doi.org/10.1093/pubmed/fdab128
Garcia LL, Yap JFC (2021) The role of religiosity in COVID-19 vaccine hesitancy. J Public Health, fdab192. https://doi.org/10.1093/pubmed/fdab192
Haerpfer C, Inglehart R, Moreno A, Welzel C, Kizilova K, Diez-Medrano J, Lagos M, Lagos M, Ponarin E, Puranen B (eds) (2022) World Values Survey: Round Seven – Country-Pooled Datafile Version 3.0. Madrid, Spain & Vienna, Austria: JD Systems Institute & WVSA Secretariat. https://doi.org/10.14281/18241.16
Hatala A, Pervaiz MC, Handley R, Vijayan T (2022) Faith based dialogue can tackle vaccine hesitancy and build trust. BMJ 376:o823. https://doi.org/10.1136/bmj.o823
Hsu T (2021) Pope Francis Encourages Covid Vaccines in Media Campaign. The New York Times. https://www.nytimes.com/2021/08/17/business/media/pope-covid-vaccine-ad.html
Kabat GC (2017) Taking distrust of science seriously. EMBO Rep. 18(7):1052–1055. https://doi.org/10.15252/embr.201744294
Lahav E, Shahrabani S, Rosenboim M, Tsutsui Y (2022) Is stronger religious faith associated with a greater willingness to take the COVID-19 vaccine? Evidence from Israel and Japan. Eur J Health Econ 23(4):687–703. https://doi.org/10.1007/s10198-021-01389-8
Lahijani AY, King AR, Gullatte MM, Hennink M, Bednarczyk RA (2021) HPV Vaccine Promotion: The church as an agent of change. Soc Sci Med 268:113375. https://doi.org/10.1016/j.socscimed.2020.113375
Larson HJ, Gakidou E, Murray CJL (2022) The Vaccine-Hesitant Moment. N Engl J Med 387(1):58–65. https://doi.org/10.1056/NEJMra2106441
Lazarus JV, Wyka K, White TM, Picchio CA, Rabin K, Ratzan SC, Parsons Leigh J, Hu J, El-Mohandes A (2022) Revisiting COVID-19 vaccine hesitancy around the world using data from 23 countries in 2021. Nat Commun 13(1):1. https://doi.org/10.1038/s41467-022-31441-x
Maechler M, Rousseeuw P, Croux C, Todorov V, Ruckstuhl A, Salibian-Barrera M, Verbeke T, Koller M, Conceicao EL, Anna di Palma M (2022) robustbase: Basic Robust Statistics (0.95-0) [Computer software]. https://robustbase.r-forge.r-project.org/
Mardian Y, Shaw-Shaliba K, Karyana M, Lau C-Y (2021) Sharia (Islamic Law) Perspectives of COVID-19 Vaccines. Front Tropical Dis, 2. https://www.frontiersin.org/articles/10.3389/fitd.2021.788188
Masur PK, Scharkow M (2020) specr: Conducting and Visualizing Specification Curve Analyses (0.2.1) [Computer software]. https://CRAN.R-project.org/package=specr
Mathieu E, Ritchie H, Ortiz-Ospina E, Roser M, Hasell J, Appel C, Giattino C, Rodes-Guirao L (2021) A global database of COVID-19 vaccinations. Nat Hum Behav 5(7):947–953. https://doi.org/10.1038/s41562-021-01122-8
Morrison M, Duncan R, Parton K (2015) Religion Does Matter for Climate Change Attitudes and Behavior. PLoS ONE 10(8):e0134868. https://doi.org/10.1371/journal.pone.0134868
Murphy J, Vallières F, Bentall RP, Shevlin M, McBride O, Hartman TK, McKay R, Bennett K, Mason L, Gibson-Miller J, Levita L, Martinez AP, Stocks TVA, Karatzias T, Hyland P (2021) Psychological characteristics associated with COVID-19 vaccine hesitancy and resistance in Ireland and the United Kingdom. Nat Commun 12(1):1. https://doi.org/10.1038/s41467-020-20226-9
Nie Y, Zhong X, Lin T, Wang W (2022) Homophily in competing behavior spreading among the heterogeneous population with higher-order interactions. Appl Math Comput 432:127380. https://doi.org/10.1016/j.amc.2022.127380
Pertwee E, Simas C, Larson HJ (2022) An epidemic of uncertainty: Rumors, conspiracy theories and vaccine hesitancy. Nat Med 28(3):456–459. https://doi.org/10.1038/s41591-022-01728-z
Price AM, Olson SM, Newhams MM, Halasa NB, Boom JA, Sahni LC, Pannaraj PS, Irby K, Bline KE, Maddux AB, Nofziger RA, Cameron MA, Walker TC, Schwartz SP, Mack EH, Smallcomb L, Schuster JE, Hobbs CV, Kamidani S, Randolph AG (2022) BNT162b2 Protection against the Omicron Variant in Children and Adolescents. N. Engl J Med 386(20):1899–1909. https://doi.org/10.1056/NEJMoa2202826
Rutjens BT, van der Linden S, van der Lee R (2021) Science skepticism in times of COVID-19. Group Process Intergroup Relat 24(2):276–283. https://doi.org/10.1177/1368430220981415
Simonsohn U, Simmons JP, Nelson LD (2020) Specification curve analysis. Nat Hum Behav 4(11):11. https://doi.org/10.1038/s41562-020-0912-z
Steegen S, Tuerlinckx F, Gelman A, Vanpaemel W (2016) Increasing Transparency Through a Multiverse Analysis. Perspect Psychological Sci 11(5):702–712. https://doi.org/10.1177/1745691616658637
Sturgis P, Brunton-Smith I, Jackson J (2021) Trust in science, social consensus and vaccine confidence. Nat Hum Behav, https://doi.org/10.1038/s41562-021-01115-7
Trepanowski R, Drążkowski D (2022) Cross-National Comparison of Religion as a Predictor of COVID-19 Vaccination Rates. J Relig Health 61(3):2198–2211. https://doi.org/10.1007/s10943-022-01569-7
Upenieks L, Ford-Robertson J, Robertson JE (2022) Trust in God and/or Science? Sociodemographic Differences in the Effects of Beliefs in an Engaged God and Mistrust of the COVID-19 Vaccine. J Relig Health 61(1):657–686. https://doi.org/10.1007/s10943-021-01466-5
Watson OJ, Barnsley G, Toor J, Hogan AB, Winskill P, Ghani AC (2022) Global impact of the first year of COVID-19 vaccination: A mathematical modelling study. Lancet Infect Dis, 0(0), https://doi.org/10.1016/S1473-3099(22)00320-6
Weber SR, Pargament KI (2014) The role of religion and spirituality in mental health. Curr Opin Psychiatry 27(5):358. https://doi.org/10.1097/YCO.0000000000000080
Wellcome Trust, The Gallup Organization Ltd. (2019) Wellcome Global Monitor, 2018 (2nd ed.) [Data collection]. UK Data Service. https://doi.org/10.5255/UKDA-SN-8466-2
Winter T, Riordan BC, Scarf D, Jose PE (2022) Conspiracy beliefs and distrust of science predicts reluctance of vaccine uptake of politically right-wing citizens. Vaccine 40(12):1896–1903. https://doi.org/10.1016/j.vaccine.2022.01.039
World Bank (2022) World Bank Country Classification, https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups
World Health Organization (2021) Achieving 70% COVID-19 Immunization Coverage by Mid-2022, https://www.who.int/news/item/23-12-2021-achieving-70-covid-19-immunization-coverage-by-mid-2022
World Health Organization (2023) Vaccine Equity, https://www.who.int/campaigns/vaccine-equity
Acknowledgements
This study was supported by the Youth Project of the National Natural Science Foundation of China 71101145 (JZ) and grant BOF/STA/202202/004 of Ghent University.
Author information
Authors and Affiliations
Contributions
Conceptualization: Z-FM, Q-WL, Y-MW, JZ; Methodology: Z-FM, Q-WL, Y-MW, JZ; Investigation: Z-FM; Visualization: Z-FM; Supervision: Z-FM, Q-WL, Y-MW, JZ; Writing—original draft: Z-FM; Writing—review & editing: Q-WL, Y-MW, JZ; Funding: JZ.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
This study was approved by Ethics Subcommittee of Institute of Psychology, Chinese Academy of Sciences (H19050), and was performed in accordance with relevant guidelines/regulations.
Informed consent
The data in this research were obtained from several global public datasets. No identifying information is involved in this research.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Mao, ZF., Li, QW., Wang, YM. et al. Pro-religion attitude predicts lower vaccination coverage at country level. Humanit Soc Sci Commun 11, 64 (2024). https://doi.org/10.1057/s41599-023-02598-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1057/s41599-023-02598-7
