
Abstract
Early-onset ischemic heart disease (IHD) is an emerging global health concern. Quantifying its burden and key risk factors is essential for effective prevention and control. This study utilizes the data from Global Burden of Disease Study 2021 to analyze the burden of IHD in young and middle-aged population (15–49 years old), including prevalence, incidence, deaths and disability-adjusted life years (DALYs) from 1990 to 2021. Attributable risk factors were assessed across different sex and region, and trends were analyzed using age-standardized rate (ASR) and average annual percentage change (AAPC). In 2021, the ASR of prevalence and incidence showed an increasing trend, with AAPCs of 0.26% (95% confidence interval [CI], 0.24% to 0.29%) and 0.23% (95%CI, 0.09% to 0.38%), respectively; the ASR of mortality and DALYs showed a decreasing trend, with AAPCs of -0.67 (95%CI, -0.91% to -0.44%) and − 0.64 (95%CI, -0.87% to -0.42%).The highest burden were observed in countries with low-middle socio-demographic index. Gender differences were observed, with men generally bearing a higher burden. Dietary risks were identified as the most significant risk factors. The burden of early-onset IHD remains a major health challenge, with significant region and gender disparities. The burden needs to be addressed through targeted public health policies.
Similar content being viewed by others
Introduction
Over the past few decades, cardiovascular diseases (CVD) have remained a leading cause of global mortality and a major consumer of healthcare resources1. Worldwide CVD deaths increased from 11 million in 1980 to 19.4 million in 2021, accounting for approximately 26.8% of all deaths2. Among CVDs, ischemic heart disease (IHD) is the primary cause of death, with disability-adjusted life years (DALYs) reaching 2275.9 per 100,000 population—substantially exceeding the burden of other cardiovascular conditions3. IHD is a condition characterized by restricted blood flow to the heart, primarily due to atherosclerosis coronary artery disease4. This narrowing of the coronary arteries reduces blood flow, leading to clinical manifestations such as angina, myocardial infarction (MI), and ischemic cardiomyopathy.
Traditionally viewed as a disease of older adults, IHD is increasingly reported in middle-aged and younger populations, who are often not regarded as high-risk and may therefore be overlooked in clinical practice5. Moreover, growing evidence indicates that early-onset IHD imposes substantial and multidimensional burdens on these populations: at the individual level, early-onset IHD is associated with prolonged morbidity and higher risks of recurrence and mortality6; at the family level, it imposes substantial emotional and financial strain7; at the workplace level, it reduces productivity through absenteeism and even unemployment8; and at the health-system level, it generates long-term demand for chronic care and repeated hospitalizations1,9. One study reported that, between 2004 and 2018, the cost of percutaneous coronary intervention (PCI) in young adults in the United States rose significantly—from $21,567 to $24,173—accompanied by increasing rates of mortality and clinical complications10. Moreover, rapid urbanization and socioeconomic transition have reshaped the risk profiles in younger adults11. Unhealthy dietary patterns, reduced physical activity, and the rising prevalence of obesity, hypertension, diabetes, and tobacco use have become particularly prominent in this age group—especially in low- and middle-income settings undergoing modernization—thereby accelerating cardiometabolic risk accumulation and shifting the onset of IHD earlier in life12,13,14,15. Importantly, many risk factors are modifiable, and younger patients who receive proactive prevention and management can achieve better clinical outcomes than older counterparts16,17. Therefore, addressing the healthcare burden of this premature IHD is of great significance for alleviating societal healthcare costs.
Systematic and up-to-date data are needed to assess the global burden of early-onset IHD. The Global Burden of Disease Study (GBD) 2021, an update of GBD 2019, incorporates improved methods and broader coverage, enhancing the reliability of its estimates. Existing studies using GBD data have analyzed the global, regional, and national IHD burden, often focusing on overall disease metrics, projected trends, or associated risk factors, whereas systematic evidence focusing specifically on younger and middle-aged populations remains scarce18,19,20. Most analyses have aggregated outcomes across entire population, emphasized older age groups, restricted attention to specific regions, or examined selected risk factors, thereby overlooking the unique epidemiological patterns and socioeconomic implications of early-onset IHD. In this study, we assessed the global, regional, and national disease burden of IHD among individuals aged 15–49 years—covering prevalence, incidence, mortality, and DALY rates—and analyze trends from 1990 to 2021. We also describe the distribution of attributable risk factors in this population.
Results
Global IHD burden among the young and middle-aged population
In 2021, among the young and middle-aged population aged 15–49 years the number of IHD prevalent, incident, death case and DALYs was substantial, with 22,580,203; 3,901,370; 609,809 and 30,443,373, respectively (Table 1). The age-standardized prevalence rate (ASPR) and age-standardized incidence rate (ASIR) per 100,000 population of IHD increased from 504.62 (95% confidence interval [CI], 504.33 to 504.92) and 88.91 (95% CI, 88.79 to 89.03) in 1990 to 546.36 (95% CI, 546.14 to 546.59) and 94.70 (95% CI, 94.61 to 94.80) in 2021, with average annual percentage changes (AAPC) of 0.26% (95% CI, 0.24% to 0.29%) and 0.23 (95% CI, 0.09, 0.38), respectively. The age-standardized mortality rate (ASMR) and age-standardized DALYs rate (ASDR) per 100,000 population decreased from 18.22 (95% CI, 18.17 to 18.28) and 904.39 (95% CI, 904.00 to 904.77) in 1990 to 14.86 (95% CI, 14.82 to 14.90) and 745.08 (95% CI, 744.82 to 745.35) in 2021, with AAPCs of −0.67% (95% CI, −0.91% to −0.44%) and − 0.64% (95% CI, −0.87% to −0.41%), respectively.
IHD burden among the young and middle-aged population in different SDI groups
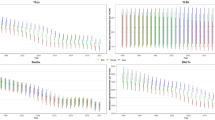
In terms of Socio-demographic Index (SDI) groups, the highest ASPR (629.99 [95% CI, 629.47 to 630.50]), ASIR (122.40 [95% CI, 122.17 to 122.62]), ASMR (22.30 [95% CI, 22.21 to 22.40]), and ASDR (1110.23 [95% CI, 1109.55 to 1110.90]) per 100,000 population of IHD among the young and middle-aged population were observed in countries with low-middle SDI (Fig. 1; Table S1). In contrast, countries with high SDI consistently had the lowest burden. The relationship between age-standardized rates (ASR) and SDI followed an inverse U-shaped curve (Fig. 2). Except for High SDI region, the AAPCs of ASPR and ASIR were − 0.18% (95%CI, −0.21% to −0.15%) and − 0.64% (95%CI, −0.81% to −0.47%), respectively, the ASPR and ASIR of other SDI groups have shown an upward trend in the past 30 years (Figs. 2 and 3; Table S1). In the past 30 years the ASMR and ASDR of each SDI group have decreased, with a faster decline rate observed in areas with higher SDI. In contrast, countries with middle, low-middle, and low SDI had slower decline rates.

Globally burden of IHD among the young and middle-aged population, by sex and SDI group from 1990 and 2021. IHD, ischemic heart disease; DALYs, disability adjusted life years.

Association between SDI and age-standardized prevalence (A), incidence (C), mortality (E) and DALYs (G) rates of IHD among the young and middle-aged population in 2021 and corresponding AAPC (B, D, F, H) from 1990 to 2021. Dotted lines refer to the global level of rates (A, C, E, G) and zero (B, D, F, H) respectively. IHD, ischemic heart disease; SDI, socio-demographic index; AAPC, average annual percentage change; DALYs, disability adjusted life years.

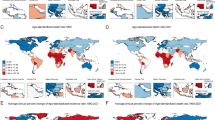
Age-standardized rate of prevalence (A), incidence (B), mortality (C) and DALYs (D) of IHD among the young and middle-aged population in 2021 and their AAPCs from 1990 to 2021. AAPC, average annual percentage change; DALYs, disability adjusted life years.
IHD burden among the young and middle-aged population in 21 GBD regions
Regarding geographical super-regions, the High-income Asia Pacific in 2021 was the region with the lowest IHD burden among the young and middle-aged population globally (Fig. 3; Table S1). North Africa and the Middle East, along with Eastern Europe, had the highest ASPR, each exceeding 900 per 100,000 population. The highest ASMR and ASDR were observed in Oceania. From 1990 to 2021, many regions, particularly East Asia, Andean Latin America, and South Asia, exhibited faster increases in prevalence than the global average. East Asia showed the fastest increase in ASIR globally, with an AAPC of 0.65% (95% CI, 0.55% to 0.74%). Over the past 30 years, the ASMR and ASDR IHD have decreased, with Western Europe, Central Europe, Australasia, and Southern Latin America showing the largest decreases, all with AAPCs below − 3%.
IHD burden among the young and middle-aged population in 204 countries and territories
At the country level, the lowest ASPR and ASIR were observed in the Republic of Korea (Fig. 4 and S1; Table S2;). In 2021, the ASPR per 100,000 population ranged from 151.67 (95% CI, 150.29 to 153.07) in the Republic of Korea to 1154.08 (95% CI, 1150.10 to 1158.07) in Saudi Arabia, while the ASIR ranged from 17.04 (95%CI, 16.57 to 17.51) in the Republic of Korea to 233.32 (95%CI, 230.50 to 236.18) in Afghanistan (Table S2). The top 10 countries with the highest ASPR and ASIR were all located in North Africa and the Middle East. Over the past 30 years, Saudi Arabia and Denmark experienced the fastest increases in IHD prevalence and incidence, respectively, with AAPCs of 0.80% (95% CI, 0.76% to 0.84%) and 1.42% (95% CI, 1.29% to 1.55%). The countries with the most significant declines in ASPR were Finland, the United States (US), New Zealand, and Germany, all with AAPCs below − 1%, the countries with the most significant declines in ASIR were Finland, the US Poland and Belgium, all with AAPCs below − 2%, and all of these countries are high SDI countries (Fig. 2).
Globally, Nauru had the highest ASMR and ASDR in 2021, with rates per 100,000 population of 117.53 (95% CI, 41.57 to 265.35) and 5710.28 (95% CI, 5059.62 to 6424.04), respectively (Table S2; Figure S1). Countries with high ASMR also tended to have high ASDR, with the top nine countries for both ASMR and ASDR located in Oceania (Figure S1). Despite the global decline in ASMR and ASDR over the past 30 years, many African countries have seen an upward trend, especially Lesotho, Zimbabwe, and Mozambique, where AAPCs have exceeded 2%.

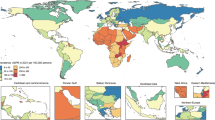
ASPR in 2021 and AAPC from 1990 to 2021of IHD among the young and middle-aged population by country and territory. (A) IHD, ischemic heart disease; ASPR, age-standardized prevalence rate; (B) AAPC, average annual percentage change. Map generated using R software (version 4.2.2; https://www.r-project.org/) with the ggplot2 and sf packages.
IHD burden among the young and middle-aged population by different genders and ages
Data from 1990 to 2021 show that men had a higher IHD burden in terms of ASPR, ASIR, ASMR and ASDR than women (Table 1; Fig. 5). In 2021, compared to women, men had higher ASPR (666.16 [95% CI, 665.81 to 666.51] vs. 424.98 [95% CI, 424.70 to 425.27]), ASIR (122.83 [95% CI, 122.68 to 122.98] vs. 66.19[95% CI, 66.08 to 66.30]), ASMR (21.15 [95% CI, 21.09 to 21.21] vs. 8.48 [95% CI, 8.44 to 8.52]), and ASDR (1053.89 [95% CI, 1053.44 to 1054.33] vs. 431.37 [95% CI, 431.08 to 431.65]). Additionally, the rising trend in prevalence and incidence over the past 30 years has been faster in women than in men (AAPC for prevalence: 0.33% [95% CI, 0.27% to 0.40%] vs. 0.22% [95% CI, 0.19% to 0.25%]; AAPC for ASIR, 0.40% [95% CI, 0.34% to 0.45%] vs. 0.17% [95% CI, −0.02% to 0.35%]).
When grouped by age (every 5 years), prevalence, incidence, mortality, and DALYs rate all increased with age, peaking in the 45–49 years age group (Fig. 5; Table S3). Gender differences in the burden of IHD also became more pronounced with age, with the largest differences observed in the 45–49 years age group. From 1990 to 2021, similar global trends were observed across age groups, with increasing prevalence and incidence and decreasing mortality and DALYs, especially in the older age groups, with the most notable trends observed in the 45–49 years age group. However, this trend was not the same among different SDI groups. In countries with middle or lower SDI, the mortality and DALYs of IHD in men had not significantly decreased over the past three decades. Especially in 40–44 years age groups, the rates had even increased.
Globally, the number of deaths of IHD among the young and middle-aged population increased with age (Figure S2A and S2B). Specifically, the increase in deaths mainly attributed to middle and low-middle SDI countries, particularly in the 40–45 and 45–49 years age groups, which together accounted for more than half of the total deaths. The most significant decrease of ASMR was observed in the 15–19 years and 45–49 years age groups and the decline has slowed down with the decline of SDI (Figure S2C).

Burden of IHD among the young and middle-aged population by sex, age group and SDI group in 1990 and 2021. (A) prevalence; (B)incidence; (C)mortality; (D) disability adjusted life years rate.
Attributable risk factors for dalys of IHD among the young and middle-aged population
In 2021, the top five attributable risk factors for DALYs of IHD among the young and middle-aged population globally were dietary risks, high LDL cholesterol, high systolic blood pressure, tobacco, and air pollution (Fig. 6). For both men and women across different regions, the most important risk factors were dietary risks and high LDL cholesterol. Among behavioral risks, men were more affected by tobacco than women (39.23% vs. 15.01%), while women were more affected by low physical activity, with a prevalence more than twice that of men (1.4% vs. 0.59%), though both were relatively low (Figure S3). Additionally, women were more affected by high body mass index than men (18.21% vs. 16.10%). From 1990 to 2021, globally, the proportion attributable to high LDL cholesterol remained stable, while the proportion attributable to other metabolic risks increased. Regarding SDI regions, although high SDI countries had a higher proportion of attributable DALYs from high LDL cholesterol, the proportion attributable to high systolic blood pressure (37.20% to 33.97%) and high LDL cholesterol (63.31% to 59.55%) decreased only in high SDI regions, with increases observed in other SDI regions. Furthermore, the proportion attributable to high body mass index increased with SDI, and it has risen across all SDI levels over the past 30 years. For environmental/occupational risks, the proportion attributable to air pollution increased as SDI decreased and the proportion attributable to tobacco decreased as SDI decreased. The proportion attributable to tobacco decreased across all SDI regions, with the most significant decrease observed in high SDI regions (54.79% to 41.55%). The proportion of risk factors in age groups after 25 was similar to that of the entire young and middle-aged population, with a significant increase in the proportion attributable to tobacco after 30 (Fig S4). The contribution of different risk factors did not vary with age, except for high systolic blood pressure, which showed an increasing trend.

DALYs of IHD among the young and middle-aged population attributable to risk factors by sex and SDI regions in 1990 and 2021.
Discussion
IHD is the leading cause of death among all types of CVD, responsible for the highest number of DALYs, reaching 2,275.9 per 100,000 population, and although it is often considered a condition affecting older adults, the early-onset burden has become increasingly significant. This study provides a comprehensive analysis of the disease burden of individuals aged 15–49 years. The results indicate that though the ASMR and ASDR of IHD among the young and middle-aged population have decreased since 1990, the number of IHD prevalent, incident, death case and DALYs still increasing, and ASPR and ASIR are also on the rise. Notably, this pattern contrasts with recent evidence from older adults (≥ 55 years), where IHD incidence has shown a declining trend underscoring the growing vulnerability of younger populations21. We also found that countries with low-middle SDI had the highest burden in 2021 and the burden of IHD is significantly higher in men than in women. Dietary risks, high LDL cholesterol, high systolic blood pressure, tobacco and air pollution were the most important risk factors for IHD globally. The burden of IHD in the 15–49 age group remains severe and should not be overlooked.
The burden of IHD among the young and middle-aged population shows striking variation across countries at different levels of socioeconomic development, with the highest burden observed in low-middle SDI countries. Health outcomes are closely linked to socioeconomic development, and low-middle SDI regions, which are undergoing modernization and urbanization, often face rapid changes in living environments and lifestyles, leading to increased exposure to health risks, such as sedentary lifestyles, poor dietary patterns, air pollution, obesity, hypertension, and high blood glucose, particularly for the young and middle-aged working population22,23. Consistent with this, the North Africa and Middle East region showed the highest age-standardized incidence and prevalence rates of early-onset IHD in our analysis, likely reflecting the rapid urbanization, dietary westernization, and limited access to preventive care across much of this region24,25. During this process, these countries also face issues arising from relatively underdeveloped healthcare systems, such as inadequate patient education, delayed diagnosis, and insufficient care and intensive care, which prevents them from balancing the growing burden of risk factors26,27. To address these challenges, targeted public health policies are urgently needed — for example, establishing community-based screening programs for hypertension and diabetes, implementing salt and trans-fat reduction policies, and improving access to affordable cardiovascular medications and acute care services. In contrast, high-SDI countries typically have high-quality healthcare systems. In Europe and the United States, cardiovascular disease and major risk factor screening systems have been developed early, allowing for the identification of high-risk populations and early intervention, which reduces the occurrence of acute IHD events28,29,30,31. Similarly, the High-income Asia Pacific region—where the early-onset IHD burden is the lowest globally—has also benefited from comprehensive preventive programs and healthier dietary patterns. In Japan, for instance, nationwide cardiovascular risk screening, along with long-term community-based surveillance, has contributed to sustained control of major risk factors32,33. The well-established emergency and intensive care systems in these regions also significantly reduce mortality from fatal MI34,35. For example, in Italy, despite IHD still being a leading cause of premature death, its mortality rate has steadily declined over the past decade36. Notably, countries with low SDI levels also appear to have a lower burden of early-onset IHD, contributing to the inverse U-shaped relationship observed between SDI and IHD rates. In low-SDI countries, the limited diagnostic capacity of health systems may lead to underdiagnosis, misclassification, or underreporting of IHD, contributing to an underestimation of its true burden37. Civil registration and vital statistics systems are often weak or incomplete, resulting in limited availability of reliable cause-of-death data for cardiovascular diseases38. Moreover, competing health risks such as infectious diseases, malnutrition, and injury-related mortality may mask the actual burden of cardiovascular disease in younger populations39. Strengthening disease surveillance systems, improving diagnostic accuracy, and integrating IHD monitoring into existing public health frameworks would be key steps to improve data quality and inform more effective interventions in these areas.
From 1990 to 2021, advancements in medical technology have significantly controlled the occurrence of fatal events associated with IHD. These improvements have led to better outcomes for high-risk acute events, particularly acute myocardial infarction (AMI). For instance, timely reperfusion therapies, such as primary PCI (PPCI), have become a standard of care for ST-segment elevation MI (STEMI). A study focusing on STEMI patients found that in 37 European Society of Cardiology countries, the number of PPCIs per 1 million population ranged between 400 and 600, with half of the countries showing substantial increases in PPCI utilization over the years40. As a result, age-standardized mortality rates for coronary artery disease have decreased by 30%–60% in high-income and many middle-income countries over the past decade41. These technological advances, particularly in acute care, have significantly reduced mortality from fatal MI. In recent years, the integration of digital innovations, especially the Internet of Things (IoT), has further expanded the scope of cardiovascular care42. IoT-based systems allow continuous patient monitoring, remote detection of arrhythmias, and real-time transmission of critical health data, which enhance early diagnosis, facilitate timely interventions, and may ultimately contribute to improved outcomes for IHD patients. Incorporating such digital health approaches may complement traditional strategies to further reduce the burden of early-onset IHD. In regions with lower SDI, the decline in IHD mortality and DALYs is less pronounced. Patients from these regions often face significant challenges in accessing effective treatment. These include lower healthcare expenditures, lack of insurance coverage, and limited access to life-saving interventions, such as coronary revascularization and heart surgery, which results in higher post-discharge mortality rates43. Strengthening universal health coverage, expanding essential cardiac care capacity, and establishing referral networks for acute coronary events could help narrow these disparities and improve survival in resource-limited settings. While mortality from IHD has been partially controlled globally, the incidence and prevalence continue to rise. In countries with high SDI, where cardiovascular risk factor monitoring and management systems were established earlier, both incidence and prevalence have been largely controlled44. In contrast, countries at other SDI levels are experiencing increases in both incidence and prevalence, which may be attributed to the widespread prevalence of risk factors such as hypertension, diabetes, obesity, and unhealthy lifestyles, underscoring the need to strengthen routine surveillance and early prevention programs targeting these modifiable risk factors45,46.
Gender and age differences play a critical and significant role in shaping the burden of early-onset IHD, with men consistently bearing a far greater burden than women across all regions, and the gap widening with age. In terms of gender differences, men have a much higher burden than women across all regions and age groups, regardless of the level of socio-economic development. Several factors, including genetics, lifestyle, social psychology, clinical manifestations, and healthcare, can help explain this gender difference47,48. Men have a higher proportion of tobacco-related DALYs than women, as they are more likely to be exposed to tobacco. Studies examining the gender-specific associations between risk factors and young people’s AMI have found that current smoking is associated with the highest odds of AMI in men49. Additionally, compared to older women, premenopausal women may benefit from significant protection from sex hormones, such as estrogen and ovarian hormones, which regulate oxidative stress and promote re-endothelialization, inhibiting the development of atherosclerosis50,51. Our results also show that the rising trend in the incidence and prevalence of early-onset IHD has been much faster in women than in men over the past 30 years. This could be attributed to the higher obesity rates in women, as high body mass index is a key contributing risk factor for early-onset IHD, with its proportion increasing significantly over the past 30 years46. Additionally, compared to older women, middle-aged and young women face pregnancy-related risk factors, such as oral contraceptive use, gestational hypertension, preeclampsia, and postpartum depression52,53,54,55. These women are often overlooked, leading to delayed diagnosis, and since women are less likely to experience chest pain and more likely to have symptoms masked by nausea or vomiting, the increasing awareness and improvement in screening systems have led to earlier diagnoses, contributing to the rise in incidence and prevalence, particularly among women56,57. These gender differences become more pronounced with age, peaking in the 45–49 age group, which reflects the cumulative effect of various risk factors over time. We also found that in countries with lower SDI, the control of IHD-related mortality in men is suboptimal. This may be due to lifestyle, working conditions, and cultural factors, with men in these countries facing more risk factors such as smoking, unhealthy diets, and air pollution58. At the same time, these high-risk groups often have limited access to healthcare services, which not only leads to delayed diagnosis but also causes them to miss the optimal treatment window for acute events59. Therefore, when making decisions about the prevention and management of early-onset IHD, it is crucial to consider both age and gender, particularly focusing on gender-specific risk factors and implementing differentiated management strategies. In countries with different levels of socio-economic development, policies should be tailored to local conditions, such as focusing on the female population in lower- and middle-income countries through improved screening for pregnancy-related cardiovascular risks, promoting tobacco cessation and weight management programs, and enhancing access to affordable primary and preventive care services.
Finally, this study identified several modifiable risk factors that significantly affect the burden of IHD among the young and middle-aged population, including tobacco use, unhealthy diet, hypertension, dyslipidemia, hyperglycemia, obesity, and insufficient physical activity. Notably, dyslipidemia and unhealthy diet ranked as the top two risk factors globally and in all SDI regions, which aligns with previous findings in younger populations, though hypertension has a higher population attributable fraction in those aged 55 and older21. This indicates that improving dietary habits and controlling blood lipids can yield significant preventive benefits in the middle-aged and young population and can also improve patient outcomes60,61. Overweight and obesity remain major health crises and are important risk factors for IHD. To date, no country has been able to curb the rising prevalence of overweight and obesity, particularly in adolescents and adults, leading to an ongoing increase in the IHD burden attributable to obesity46. In countries with higher socio-economic development, systems for identifying and treating major cardiovascular risk factors, especially hypertension, diabetes, and dyslipidemia, have been established44. Over the past 30 years, these countries have seen initial successes in controlling these risk factors through targeted primary, secondary, and tertiary prevention policies, though the burden of overweight and obesity continues to rise, requiring more effective prevention and management measures62. In contrast, in countries with lower socio-economic development, which are undergoing rapid transitions, air pollution control is suboptimal. Air pollution is a risk factor for many diseases and may increase the risk of IHD through mechanisms such as oxidative stress, endothelial dysfunction, and vascular dysfunction63,64.
Limitations
Despite this study providing a comprehensive assessment of the global, regional, and national burden and time trends of early-onset IHD among individuals aged 15–49 years, several limitations must be considered. First, the GBD 2021 database excludes data of poor quality or with significant flaws, and missing information from countries or regions is estimated through statistical modeling. Even where data exist, variations in case definitions, diagnostic criteria, and data collection methods across countries may introduce bias. Second, mortality and non-fatal outcomes in the GBD study rely on national vital registration systems, health surveys, and hospital records, which differ widely in completeness and accuracy. These disparities are particularly pronounced in low- and lower-middle-SDI regions, where limited diagnostic capacity, underdeveloped surveillance systems, and weak health infrastructure can lead to underreporting or misclassification of IHD cases. Finally, although the GBD framework uses advanced modeling techniques to reduce uncertainty, residual errors and wide uncertainty intervals remain inevitable, especially in regions with poor health infrastructure where primary data are limited or unreliable.
Conclusion
Early-onset IHD in individuals aged 15–49 years remains a significant global health challenge, with increasing rates of prevalence, incidence, and associated deaths and DALYs. Despite some regional improvements, the burden of early-onset IHD in individuals aged 15–49 years continues to rise, particularly in low-middle SDI countries undergoing rapid development. Gender differences significantly contribute to the disease burden, with men generally experiencing a higher burden than women. However, the rapid rise in incidence and prevalence among women over the past 30 years should not be overlooked. It is crucial to consider gender-specific risk factors in women for targeted control and prevention. Dietary risks and high LDL cholesterol are the leading attributable risk factors for early-onset IHD. Strengthening healthcare systems, improving risk factor management, and promoting public health policies focused on prevention are essential for reducing the global impact of early-onset IHD and addressing health inequities between regions.
Methods
Data source
The GBD is an ongoing large-scale study that provides reliable and timely assessments of the epidemiological profiles of diseases, injuries, and risk factors worldwide65. GBD 2021 is the most recent publicly available dataset, covering 204 countries and regions from 1990 to 202166. IHD was classified as a Level 3 cause in GBD 2021, comprising two major components: AMI and chronic IHD. For data modeling, GBD 2021 utilizes vital registration and verbal autopsy reports, with the Cause of Death Ensemble model (CODEm) integrating multiple data sources and covariates to estimate mortality in regions or years with sparse data. For non-fatal outcomes, including prevalence and incidence, the DisMod-MR 2.1 Bayesian meta-regression tool ensures internal consistency among epidemiological parameters and provides estimates for locations or time periods lacking direct observations. Missing or incomplete data in the GBD 2021 database are thus addressed through these standardized modeling frameworks.
This study was designed as a secondary data analysis of the Global Burden of Disease 2021 (GBD 2021) database. We extracted data of IHD prevalence, incidence, mortality, DALYs and 95% uncertainty interval (UI) for individuals aged 15–49 from 1990 to 2021, as well as age-specific rates and the attributable risk factors for IHD. The comprehensive data were publicly available in the Global Health Data Exchange GBD Results Tool (https://vizhub.healthdata.org/gbd-results/) and hence no ethical approval was necessary.
Attributable risk factors
In GBD 2021, risk factors are classified into a hierarchical structure with four levels, providing a comprehensive framework to assess the contribution of each factor to disease burden67. The burden attributable to each risk factor is estimated by calculating the population attributable fraction (PAF), which reflects the proportion of disease that would be avoided if exposure to a risk factor were reduced to an ideal level. The attributable DALYs are then derived by multiplying the PAF by the total DALYs from IHD. Globally, early-onset IHD-related deaths and DALYs can be attributed to 11 major risk factors, categorized into three broad groups: metabolic risks (kidney dysfunction, high low-density lipoprotein [LDL] cholesterol, high fasting plasma glucose, high systolic blood pressure, and high body mass index), environmental/occupational risks (air pollution, nonoptimal temperature, and other environmental exposures), and behavioral risks (low physical activity, tobacco use, and dietary risks). Given the ongoing debate surrounding the potentially protective effects of moderate alcohol consumption on IHD, alcohol use was excluded from the final analysis to avoid bias in interpretation68.
Subgroup analyses by sex and SDI
The SDI is a composite indicator developed by the Institute for Health Metrics and Evaluation to quantify the development level of countries or regions. The SDI ranges from 0 to 1, with higher values indicating greater socioeconomic development. In GBD 2021, the 204 countries and regions were categorized into five groups based on their SDI values: low, low-middle, middle, high-middle, and high SDI39. SDI is strongly correlated with health outcomes and serves as a framework to understand the relationship between socioeconomic development and health burdens.
In this study, subgroup analyses were conducted by sex and by SDI quintiles to explore disparities in IHD burden. These stratifications were selected because cardiovascular risk profiles differ substantially between men and women, and SDI reflects variations in healthcare access, economic status, and epidemiological transition across countries. Together, these subgroup analyses provide a more nuanced understanding of the heterogeneity in early-onset IHD burden across different demographic and developmental contexts.
Statistical analysis
We calculated ASR and corresponding 95% CI based on the world standard population reported in GBD 202169. To assess the magnitude and direction of temporal trends in early-onset IHD prevalence, incidence, mortality, and DALYs, we calculated the AAPC and its 95% CI using joinpoint regression. The Joinpoint software (version 4.9.1, National Cancer Institute, USA) was used to fit the simplest joinpoint model allowed by the data. Significance testing was performed using the Monte Carlo Permutation Test. If AAPC > 0 and P-value < 0.05, the ASR was considered to be increasing during the study period; if AAPC < 0 and P-value < 0.05, the ASR was decreasing; if P ≥ 0.05, the rate was considered stable. We applied least squares regression and generalized additive models to examine potential linear or nonlinear relationships between SDI and ASRs or AAPC. All statistical analyses were performed using R software (version 4.4.2). A P-value of < 0.05 was considered statistically significant.
Data availability
The data analyzed in this study were publicly available in the Global Health Data Exchange GBD Results Tool ([https://vizhub.healthdata.org/gbd-results/](https:/vizhub.healthdata.org/gbd-results)).
References
Rittiphairoj, T. et al. The economic burden of ischaemic heart diseases on health systems: a systematic review. BMJ Glob Health. 10, e015043 (2025).
Xia, X. et al. Global trends and regional differences in mortality of cardiovascular disease and its impact on longevity, 1980–2021: Age-period-cohort analyses and life expectancy decomposition based on the global burden of disease study 2021. Ageing Res. Rev. 103, 102597 (2025).
Mensah, G. A. et al. Global burden of cardiovascular diseases and Risks, 1990–2022. J. Am. Coll. Cardiol. 82, 2350–2473 (2023).
Młynarska, E. et al. From atherosclerotic plaque to myocardial Infarction—The leading cause of coronary artery occlusion. Int. J. Mol. Sci. 25, 7295 (2024).
Arora, S. et al. Twenty year trends and sex differences in young adults hospitalized with acute myocardial infarction. Circulation 139, 1047–1056 (2019).
Collet, J. P. et al. Long-Term evolution of premature coronary artery disease. JACC 74, 1868–1878 (2019).
Hagström, E. et al. Psychosocial stress and major cardiovascular events in patients with stable coronary heart disease. J. Intern. Med. 283, 83–92 (2018).
Smedegaard, L. et al. Return to work and risk of subsequent detachment from employment after myocardial infarction: insights from Danish nationwide registries. J. Am. Heart Association. 6, e006486 (2017).
Akhtar, K. H. et al. The spectrum of post-myocardial infarction care: from acute ischemia to heart failure. Prog. Cardiovasc. Dis. 82, 15–25 (2024).
Minhas, AMK. et al. Clinical and economic burden of percutaneous coronary intervention in hospitalized young adults in the united States, 2004–2018. Curr. Probl. Cardiol. 47, 101070 (2022).
Lear, S. A. et al. Social factors, health policy, and environment: implications for cardiovascular disease across the Globe. Eur. Heart J. 46, 2959–2973 (2025).
Neil, J. et al. Managing atherosclerotic cardiovascular risk in young adults: JACC State-of-the-Art review. J. Am. Coll. Cardiol. https://doi.org/10.1016/j.jacc.2021.12.016 (2022).
Odunaiya, N. A., Grimmer, K. & Louw, Q. A. High prevalence and clustering of modifiable CVD risk factors among rural adolescents in Southwest nigeria: implication for grass root prevention. BMC Public. Health. 15, 661 (2015).
Estebsari, F. et al. Risk factors of cardiovascular disease (CVD) in young adults: a community-based study of Iranian context. BMC Public. Health. 24, 2543 (2024).
Abbas, E. et al. Risk factors for the development of early onset diabetes in the population of Sindh Province, Pakistan. Biomedicines 13, 1107 (2025).
Pinxterhuis, T. H. et al. First myocardial infarction in patients with premature coronary artery disease: insights into patient characteristics and outcome after treatment with contemporary stents. Eur. Heart J. Acute Cardiovasc. Care. 12, 774–781 (2023).
Zeitouni, M. et al. Risk factor burden and Long-Term prognosis of patients with premature coronary artery disease. J. Am. Heart Association. https://doi.org/10.1161/JAHA.120.017712 (2020).
Tan, J. et al. Global, Regional, and National burden of ischemic heart disease attributable to 25 risk factors and their summary exposure value across 204 countries with different Socio-Demographic index Levels, 1990–2021: A systematic Fixed-Effects analysis and comparative study. Clin. Epidemiol. 17, 105–129 (2025).
An, J. Q. et al. Global burden, trends and inequalities for ischaemic heart disease attributable to high fasting plasma glucose, high low-density lipoprotein cholesterol and high systolic blood pressure, 1990–2021: an analysis of the global burden of disease study 2021. Diabetes Obes. Metabolism. https://doi.org/10.1111/dom.16199 (2025).
Shi, H. et al. Global burden of ischaemic heart disease from 2022 to 2050: projections of incidence, prevalence, deaths, and disability-adjusted life years. Eur. Heart J. - Qual. Care Clin. Outcomes qcae049, https://doi.org/10.1093/ehjqcco/qcae049 (2024).
Xue, P. et al. Global, regional, and National epidemiology of ischemic heart disease among individuals aged 55 and above from 1990 to 2021: a cross-sectional study. BMC Public. Health. 25, 1–16 (2025).
de Groot, R. et al. Urban-rural differences in the association between blood lipids and characteristics of the built environment: a systematic review and meta-analysis. BMJ Glob Health. 4, e001017 (2019).
Uthman, O. A. et al. Global prevalence and trends in hypertension and type 2 diabetes mellitus among slum residents: a systematic review and meta-analysis. BMJ Open. 12, e052393 (2022).
Aljefree, N. & Ahmed, F. Association between dietary pattern and risk of cardiovascular disease among adults in the Middle East and North Africa region: a systematic review. Food Nutr. Res. 59, https://doi.org/10.3402/fnr.v59.27486 (2015).
Ahmadi, M. et al. Burden of ischemic heart disease in the Middle East and North Africa (MENA) and attributable risk factors: an epidemiological analysis from 1990 to 2019. IJC Heart Vasculature. 50, 101316 (2024).
Nascimento, B. R., Brant, L. C. C., Marino, B. C. A., Passaglia, L. G. & Ribeiro, A. L. P. Implementing myocardial infarction systems of care in low/middle-income countries. Heart 105, 20–26 (2019).
Callender, T. et al. Heart failure care in Low- and Middle-Income countries: A systematic review and Meta-Analysis. PLoS Med. 11, e1001699 (2014).
Gandhi, S. et al. Ten-Year trends in patient Characteristics, Treatments, and outcomes in myocardial infarction from National cardiovascular data registry chest Pain-MI registry. Circ. Cardiovasc. Qual. Outcomes. 15, e008112 (2022).
Komajda, M. et al. EURObservational research programme: the chronic ischaemic cardiovascular disease registry: pilot phase (CICD-PILOT). Eur. Heart J. 37, 152–160 (2016).
Wilkinson, C. et al. Definitions of clinical study outcome measures for cardiovascular diseases: the European unified registries. Eur. Heart J. 46, 190–214 (2025).
Martin, S. S. et al. 2024 heart disease and stroke statistics: A report of US and global data from the American heart association. Circulation 149, e347–e913 (2024).
Hata, J. et al. Secular trends in cardiovascular disease and its risk factors in Japanese. Circulation 128, 1198–1205 (2013).
Tsushita, K. et al. Rationale and descriptive analysis of specific health guidance: the nationwide lifestyle intervention program targeting metabolic syndrome in Japan. J. Atheroscler Thromb. 25, 308–322 (2018).
Yoo, E. J., Edwards, J. D., Dean, M. L. & Dudley, R. A. Multidisciplinary critical care and intensivist staffing: results of a statewide survey and association with mortality. J. Intensive Care Med. 31, 325–332 (2016).
Mebazaa, A. et al. Management of cardiogenic shock complicating myocardial infarction. Intensive Care Med. 44, 760–773 (2018).
Zuin, M. et al. Declining trends of premature mortality from ischemic heart disease and regional differences in Italy from 2011 to 2017. Int. J. Cardiol. 383, 110–116 (2023).
Gupta, R. & Yusuf, S. Challenges in management and prevention of ischemic heart disease in low socioeconomic status people in LLMICs. BMC Med. 17, 209 (2019).
Adair, T., Firth, S., Phyo, T. P. P., Bo, K. S. & Lopez, A. D. Monitoring progress with National and subnational health goals by integrating verbal autopsy and medically certified cause of death data. BMJ Glob Health. 6, e005387 (2021).
GBD 2021 Diseases and Injuries Collaborators. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the global burden of disease study 2021. Lancet 403, 2133–2161 (2024).
Kristensen, S. D. et al. Reperfusion therapy for ST elevation acute myocardial infarction 2010/2011: current status in 37 ESC countries. Eur. Heart J. 35, 1957–1970 (2014).
Virani, S. S. et al. Heart disease and stroke Statistics—2020 update: A report from the American heart association. Circulation 141, e139–e596 (2020).
Mulita, F., Verras, G. I., Anagnostopoulos, C. N. & Kotis, K. A smarter health through the internet of surgical things. Sensors 22, 4577 (2022).
Tromp, J. et al. Global differences in burden and treatment of ischemic heart disease in acute heart failure. JACC: Heart Fail. 9, 349–359 (2021).
Mukonda, E. & Lesosky, M. A comparative analysis and review of how National guidelines for chronic disease monitoring are made in low- and middle-income compared to high-income countries. J. Glob Health. 11, 04055 (2021).
Sun, H. et al. IDF diabetes atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res. Clin. Practice 183, 109119 (2022).
Ng, M. et al. Global, regional, and National prevalence of adult overweight and obesity, 1990–2021, with forecasts to 2050: a forecasting study for the global burden of disease study 2021. Lancet 405, 813–838 (2025).
Lichtman, J. H. et al. Variation in recovery. Circulation: Cardiovasc. Qual. Outcomes. 3, 684–693 (2010).
Blum, A. Gender differences in vascular aging and in coronary artery disease pathophysiology. QJM: Int. J. Med. 116, 745–749 (2023).
Lu, Y. et al. Sex-Specific risk factors associated with first acute myocardial infarction in young adults. JAMA Netw. Open. 5, e229953 (2022).
Huang, A. & Kaley, G. Gender-Specific regulation of cardiovascular function: Estrogen as key player. Microcirculation 11, 9–38 (2004).
Mendelsohn, M. E. & Karas, R. H. Molecular and cellular basis of cardiovascular gender differences. Science 308, 1583–1587 (2005).
Marschner, S. et al. Prevention of cardiovascular disease in women with Pregnancy-Related risk factors: A prospective women’s heart clinic study. J. Am. Heart Assoc. 12, e030015 (2023).
van Roeters, J. E. et al. Women, lipids, and atherosclerotic cardiovascular disease: a call to action from the European atherosclerosis society. Eur. Heart J. 44, 4157–4173 (2023).
Crump C. et al. Pre-Term delivery and risk of ischemic heart disease in women. J Am. Coll. Cardiol. 76, 57–67 (2020).
O’Kelly, A. C. et al. Pregnancy and reproductive risk factors for cardiovascular disease in women. Circul. Res. 130, 652–672 (2022).
Meyer, M. R. et al. Gender differences in patient and system delay for primary percutaneous coronary intervention: current trends in a Swiss ST-segment elevation myocardial infarction population. Eur. Heart J. Acute Cardiovasc. Care. 8, 283–290 (2019).
Chen, W., Woods, S. L., Wilkie, D. J. & Puntillo, K. A. Gender differences in symptom experiences of patients with acute coronary syndromes. J. Pain Symptom Manag. 30, 553–562 (2005).
Isma’eel, H. A. et al. Worsening of the cardiovascular profile in a developing country: the greater Beirut area cardiovascular cohort. Global Heart. 13, 275–283 (2018).
Malamba-Lez, D., Ngoy-Nkulu, D., Steels, P., Tshala-Katumbay, D. & Mullens, W. Heart failure etiologies and challenges to care in the developing world: an observational study in the Democratic Republic of congo. J. Card Fail. 24, 854–859 (2018).
Winter, M. P. et al. Lipid profile and long-term outcome in premature myocardial infarction. Eur. J. Clin. Invest. 48, e13008 (2018).
Leistner, D. M. et al. Impact of elevated lipoprotein(a) on coronary artery disease phenotype and severity. Eur. J. Prev. Cardiol. 31, 856–865 (2024).
Adjei, N. K. et al. Ethnic differences in metabolic syndrome in high-income countries: A systematic review and meta-analysis. Rev. Endocr. Metab. Disord. 25, 727–750 (2024).
Münzel, T. et al. Effects of gaseous and solid constituents of air pollution on endothelial function. Eur. Heart J. 39, 3543–3550 (2018).
Chen, R. et al. Hourly air pollutants and acute coronary syndrome onset in 1.29 million patients. Circulation https://doi.org/10.1161/CIRCULATIONAHA.121.057179 (2022).
Murray, C. J. L. The global burden of disease study at 30 years. Nat. Med. 28, 2019–2026 (2022).
Murray, C. J. L. Findings from the global burden of disease study 2021. Lancet 403, 2259–2262 (2024).
Brauer, M. et al. Global burden and strength of evidence for 88 risk factors in 204 countries and 811 subnational locations, 1990–2021: a systematic analysis for the global burden of disease study 2021. Lancet 403, 2162–2203 (2024).
Millwood, I. Y. et al. Conventional and genetic evidence on alcohol and vascular disease aetiology: a prospective study of 500 000 men and women in China. Lancet 393, 1831–1842 (2019).
Schumacher, A. E. et al. Global age-sex-specific mortality, life expectancy, and population estimates in 204 countries and territories and 811 subnational locations, 1950–2021, and the impact of the COVID-19 pandemic: a comprehensive demographic analysis for the global burden of disease study 2021. Lancet 403, 1989–2056 (2024).
Acknowledgements
We extend our gratitude to the contributors of the Global Burden of Diseases, Injuries, and Risk Factors Study 2021 for their invaluable work (https://www.healthdata.org/research-analysis/gbd). We also express our sincere appreciation to the Institute for Health Metrics and Evaluation (IHME) for making the GBD data available for this research.
Funding
This research was funded by the National Natural Science Foundation of China (81973117).
Author information
Authors and Affiliations
Contributions
All authors have made substantial contributions to this study. Jiayi Song: Conceptualization, data curation, formal analysis, visualization, writing—original draft; Kun Yuan: Methodology, statistical analysis, validation; Yilin Huang: Data curation, validation; Zuo Chen, Xin Wang, Zengwu Wang: Data interpretation, resources; writing—review & editing; Linfeng Zhang: Conceptualization; project administration, funding acquisition, writing—review & editing. The final version of the manuscript was approved by all authors, who agreed to its submission.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Supplementary Information
Tables S1-3, and Figures S1-4.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Song, J., Yuan, K., Huang, Y. et al. Global, regional, and national burden of ischemic heart disease in young and middle-aged population from 1990 to 2021. Sci Rep 15, 41982 (2025). https://doi.org/10.1038/s41598-025-26248-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-26248-x
