
Abstract
Chiang Mai encounters severe pollution during the wildfire season. Wildland firefighters encounter various hazards while engaged in fire suppression operations, which encompass significant exposure to elevated concentrations of air pollutants resulting from combustion, especially particulate matter. The adverse effects of wildfire smoke on respiratory health are a significant concern. The objective of this study was to examine the potential adverse effects of PM2.5 exposure on the respiratory function and DNA damage of wildland firefighters. This prospective cohort study conducted in Chiang Mai from January to May 2022 planned to evaluate the health status of wildland firefighters during the pre-peak, peak, and post-peak ambient air pollution seasons. The measurement of PM2.5 was done at every forest fire station, as well as utilizing data from the Pollution Control Department. Participants received general health examinations, spirometry evaluations, and blood tests for DNA damage analysis. Pair t-tests and multiple regression models were used to examine the connection between pulmonary function parameters (FVC, FEV1) and PM2.5 concentration, with a significance level of P < 0.05. Thirty-three peak-season and twenty-one post-peak-season participants were enrolled. Four pre-peak-season wildland firefighters had FVC and FEV1 declines of > 15%. Multiple regression analysis showed a negative association between PM2.5 exposure and FVC% predicted (− 2.81%, 95% CI − 5.27 to − 0.34%, P = 0.027) and a marginally significant negative correlation with FVC (− 114.38 ml, 95% CI − 230.36 to 1.59 ml, P = 0.053). The remaining pulmonary measures showed a statistically insignificant decline. There were no significant changes in DNA damage detected. Wildland firefighters suffered a significant decline in pulmonary function associated with PM2.5 exposure. Spirometry is crucial for monitoring and promptly identifying respiratory issues that occur during wildfire seasons. Further research is recommended to explore DNA damage alterations and their potential association with PM2.5.
Similar content being viewed by others


Introduction
Ambient air pollution is a continually expanding global health concern. The World Health Organization (WHO) estimated that 99% of the global population breathes air that exceeds WHO guidelines, resulting in 4.2 million deaths each year due to ambient air pollution1. This issue has been significantly impacted by climate change and regionally distinct weather events2. Moreover, specific sources, such as smoke from wildfires, can contribute to ambient air pollution. In 2019, Global Forest Watch recorded more than 4.5 million fires worldwide, either directly or indirectly caused by climate change3. Wildland fire emissions contain a range of air pollutants, such as fine and coarse particulate matter (PM), gases, carbon monoxide (CO), methane, nitrous oxide (N2O), nitrogen oxides (NOx), volatile organic carbon (VOC), and many other air toxics. Therefore, it can lead to numerous adverse health consequences in various human systems4,5. There is evidence of a significant association between exposure to conflagration smoke or PM2.5 and all-cause mortality and respiratory morbidity6. Regarding the respiratory system, it was discovered that some lung function parameters declined due to wildfires5,7,8. In areas where wildfires have a greater impact, the issue of understanding the effects of wildfires is ongoing and must be addressed with greater awareness.
Firefighters are particularly at risk for wildfire hazards due to their exposure to extreme temperatures, hazardous chemicals and substances, shift work, and psychological stress in emergency fire suppression9. Although wildland firefighters (WLFF) are required to wear personal protective equipment (PPE), it is unlikely that they would use self-contained breathing apparatus (SCBA) like urban firefighters10,11. Due to the excessive weight and limited duration of use of SCBA, WLFF are at a higher risk of inhaling hazardous substances12. In addition to differences in working conditions, while few PM toxicity studies focus on wildfire sources, those that do suggest that finer particles are more adverse than coarser particles and that wildfire PM may be more toxic than urban PM13. One main system affected is the respiratory system. Changes in pulmonary function were reported regardless of smoking history14. Pulmonary inflammation is the established mechanism of change, leading to the formation of radicals15. Conducting research on either pulmonary function or DNA damage indicators would provide us with a comprehensive understanding.
Chiang Mai is one of the world's notable places with the most severe levels of ambient air pollution, surpassing the daily standard set by the air quality index. This is particularly evident during the peak of the annual wildfire season, which typically occurs from February to April. During the seasonal haze, PM2.5 levels in Chiang Mai exceeded the WHO annual air quality guideline value by four times or more. The previous study showed that one of the primary sources of ambient air pollution in Chiang Mai affects the biomass community with burning from forest fires and agricultural burning16. Forest fires in Chiang Mai doubled, increasing from 1537 occurrences in fiscal year 2022 to 3689 occurrences in fiscal year 202317. Currently, there is governmental involvement that wants to support and maintain wildland firefighters’ health but needs more information to assess fit-to-work and surveillance of wildland firefighters’ health, which might be established as a national standard. Our previous study revealed that WLFF in Thailand lacked sufficient medical surveillance and fitness-for-duty assessments18. Therefore, it was crucial to examine the negative health effects and implement a suitable occupational health and safety program for WLFF. To bridge this knowledge gap, we aimed to investigate the potential adverse effects of PM2.5 exposure on the respiratory function and DNA damage of WLFF during two phases: the pre-to-peak season and pre-to-post-peak season. Spirometry and DNA damage measures were utilized to describe both cell and clinical levels since research revealed that wildfire can induce deleterious effects from cell to clinical presentation.
Materials and methods
Study design and population
This prospective cohort study was conducted from January 2022 to May 2022, starting from a pre-peak season in January 2022 to a peak season of ambient air pollution in March 2022 and a post-peak season of ambient air pollution in May 2022. According to a previous study18 that recruited from all stations in Chiang Mai province administered by the Organization of Protected Areas, Regional Office 16, Department of National Parks, Wildlife, and Plant Conservation, Thailand, seven stations volunteered to participate in our study. The study's inclusion criteria required that participants had a minimum of 1 year of work experience and be at least 18 years of age. The study excluded participants who were no longer accessible for follow-up during the study period. A total of fifty-four wildland firefighters were recruited during the pre-peak season of ambient air pollution, which commenced in January 2022 and served as the baseline. In the final cohort observation, a total of thirty-two participants were observed during the peak season, while twenty participants were observed during the post-peak season of ambient air pollution. Figure 1 represented the study flow and timeline of participants’ surveillance during both periods.

The study flow diagram.
Data collection for working-area monitoring
The primary focus of participants' professional responsibilities revolved around the national park region. The likelihood of this region undergoing a transformation into large-scale wildfires was substantial. Their responsibility entailed being present at the station and constantly ready to participate in the suppression of wildfires in the event of any reported areas of high fire activity. Furthermore, their responsibilities encompassed the construction of firebreaks within the high-risk region of the hotspot during the pre-peak season. For the working area sampling, primary data from ambient work assessments was utilized at each forest fire station. Additionally, secondary data on the ambient air index was obtained from the Pollution Control Department, Ministry of Natural Resources and Environment, Thailand (PCD). The indoor PM2.5 assessment at the station was measured using the real-time optical scattering method by Dusttrak II Aerosol Monitors for an entire eight-hour workday. This method was recommended by the Thai regulations (announcement of the Department of Health on the monitoring of air quality in public buildings, B.E. 2565). The indoor PM2.5 concentration was presented as an eight-hour mean average. For ambient PM2.5 data, PCD continuously monitored it using beta-ray attenuation measurements. This information was computed and presented as a 3-day moving average.
Data collection for health assessments
The health assessments consisted of general health information, spirometry evaluations, and blood test for DNA damage analysis. Participants' general information includes their age, gender, body weight (kg), height (cm), waist circumference (cm), body mass index (BMI, kg/m2), smoking status, and vital signs. BMI was categorized into four groups by Asian BMI classification: underweight (< 18.5 kg/m2), normal weight (18.5–2.9 kg/m2), overweight (23–24.9 kg/m2), and obese (≥ 25 kg/m2)19. Participants' vital signs, including blood pressure and pulse rate, will be recorded to determine if they were able to do spirometry. Six milliliters of venous blood samples were collected twice from each subject.
Blood samples were transferred to be centrifuged at 3000 revolutions per minute (rpm) for fifteen minutes to enable the collection of plasma. DNA damage was measured using the alkali comet assay based on the method published by Singh et al.20 (Supplementary Information). Centrifugation was used to isolate lymphocytes, which were then prepared for electrophoresis and analyzed using a fluorescence microscope equipped with an imaging system and COMET Assay software. Tail length (the distance of DNA migration) and tail moment (the distance between the center of gravity of the head and the center of gravity of the tail) were the two main parameters measured. These values were measured and displayed in microns (μm).
The SpiroMaster PC-10 was used to evaluate the spirometry test. The procedures was conducted using recommendation standardization of spirometry from ATS/ERS21. Participants required to completed at least three acceptable graphs in accordance with ATS/ERS requirements21. Collecting parameters including FEV1, FCV, FEF50, and FEV1/FCV. The Thai Siriraj equation was used as a reference for predicting the value22. Interpretation of pulmonary function was calculated by using fixed ratio criteria to determine normal lung function, obstructive lung, restrictive lung, and mixed abnormal. The determination of abnormally reduced lung function was determined by using a 10% decline in FEV1 from baseline, and a significant reduction was considered when measured FEV1 declined by 15%23.
Statistical analysis
The mean of ambient PM2.5 concentration was calculated as the 3-day moving average 14 days before the test. The indoor PM2.5 was presented as mean average. In this study, paired t-test was used to compare changes in pulmonary function test and multiple regression statistical models was used to determine the correlation between lung function indices (FVC, FEV1) and PM2.5 concentration (0 day). Multiple imputation was used to assume the incomplete data for missing data in TL and TM before using multivariate regression based to compare difference of TL an TM between the two periods. Statistical analyzes were performed using STATA software (version 16.0) and statistical significance for P-values < 0.05 were considered.
Ethical considerations
This study and the protocol were approved by the Research Ethics Committee, Faculty of Medicine, Chiang Mai University, Thailand (Study code: COM-2564-08308).
Institutional review board statement
This study was conducted following the Declaration of Helsinki, and the protocol was approved by the Research Ethics Committee, Faculty of Medicine, Chiang Mai University, Thailand (Study code: COM-2564-08308).
Informed consent statement
Informed consent was obtained from all subjects involved in the study.
Results
Baseline characteristics of wildland firefighters and difference between two groups
All 54 participants actively participated in this study until its conclusion. Nevertheless, only 50 of the 54 wildland firefighters with completed spirometry data and 49 with completed DNA samples were available for analysis. Most of the participants were men, and their average age was 41.81 years. Following the phase of follow-up, we categorized all participants into two categories.
In the pre-to-peak season group, the mean age of participants was 41.59 + 10.19 years. In the pre-to-post-peak season group, the mean age of participants was 42 + 9.99 years. The majority of participants in both groups were male, engaged in smoking, and did not have any pre-existing medical conditions. There were no statistically significant differences observed in the characteristics of the two groups. Table 1 provided the pre-peak and pre-post-season groups' baseline characteristics.
Ambient and indoor PM2.5 concentration between pre-peak, peak, and post-peak season
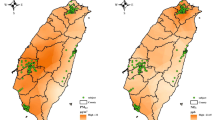
The ambient air monitoring was used to represent the average exposure of wildland firefighters operating at the scene during each period. Figure 2 showed the 3-day moving average of ambient PM2.5 prior to 14 days of data collection for each phase. In the pre-peak, peak, and post-peak seasons, ambient PM2.5 concentrations were 23.1 ± 3.2, 35.3 ± 7.4, and 13.1 ± 2.0 g/m3, respectively. The average concentration of indoor PM2.5 ranged between 17 and 24.44 g/m3 during the “pre-to-peak season” and between 10.78 and 85.95 g/m3 during the “pre-to-post-peak season.” Table 2 showed the “pre-peak season” and “post-peak season” mean indoor PM2.5 concentrations for each station. In every location, peak season PM2.5 concentrations were significantly higher than pre-peak season concentrations, and post-peak season PM2.5 concentrations were significantly lower than pre-peak season concentrations.

Comparison of the 3-day moving average concentration of ambient PM2.5 (14 days before the data collection date between the pre-peak season of ambient air pollution (January), the peak season of ambient air pollution (March), and post-peak season of ambient air pollution (May)).
Pulmonary function between two groups
This study found a significant difference in observed FVC, percent predicted FVC, observed FEV1, and percent predicted FEV1 among participants in the pre-to-peak season group (P < 0.05). The mean differences between observed FVC and observed FEV1 in pre-peak season were − 0.28 + 0.59 L (95% CI − 0.50 to − 0.06, P = 0.013) and − 0.21 + 0.49 L (95% CI − 0.39 to − 0.03, P = 0.025), respectively. For the pre-to-post-peak season, it was no significant difference in pulmonary function between the two periods. The overall details are shown in Table 3.
Out of the 30 individuals in the pre-to-peak group, seven of them, with six having normal lung function and one having obstructive lung function, experienced a significant decline in volume on the pulmonary function test. Four individuals observed a decrease in lung function exceeding 15%. In addition, the lung function of one participant shifted from normal to obstructive.
Among the group of 20 individuals observed during the pre-to-post-peak season, a significant decline in lung function was observed. Two individuals with abnormal lung function had a recovery to normal lung function, one due to obstruction and the other due to restriction. One participant underwent a shift from a normal lung to a restrictive lung without reporting a significant decrease in lung function.
The conclusion of pulmonary function and how it changes over each phase was described in Fig. 3.

Classification of pulmonary function and its changes between pre-to-peak to post-season periods.
Multiple regression analysis with adjustments for age, sex, smoking status, height, and weight in pre-peak group revealed a 10 g/m3 rise in PM2.5 had a negatively associated with the change in FVC% predicted (− 2.81%, 95% CI − 5.27 to − 0.34%, P = 0.027) and a marginally significant negative correlation with changing FVC (− 114.38 ml, 95% CI − 230.36 to 1.59 ml, P = 0.053). Other lung function parameters (FEV1, FEF50, and FEV1% predicted) showed negative direction without statistically significant. Change in pulmonary function with 10 µg/m3 increase in PM2.5 was showed in Fig. 4.

Multiple regression analysis of change in pulmonary function with 10 µg/m3 increase in PM2.5 adjusted by age, sex, smoking status, height, and weight. FVC Forced vital capacity, FEF50 Forced expiratory flow at 50% of the forced vital capacity, FEV1 Forced expiratory volume in 1 s, L liters.
DNA damage between two groups: tail length (TL) and tail moment (TM)
The mean change in the total case analysis (N = 49) was − 0.039 (95% CI − 0.230 to 0.152, P = 0.683) for TL and − 0.024 (95% CI − 0.010 to 0.051, P = 0.520) for TM. Multiple imputations of the average TL and TM changes were performed in 100 datasets using chained multivariate regression on an evaluation of the following baseline characteristics: age, gender, SBP, DBP, heart rate, BMI, TL, and TM. This method was applied to include an additional five right-censoring cases (10.2%) with presumed missing at random, as all missing participants came from a single forest fire control station. Results combined using Rubin’s rules were robust compared to the complete case analyses, with changes of − 0.037 (95% CI − 0.222 to 0.149, P = 0.691) for TL and − 0.023 (95% CI 0.097 to 0.05, P = 0.538) for TM. Table 4 presented the mean changes from the complete data analysis and multiple imputation analyses. TL and TM similarly showed no significant changes in the pre-to-peak and pre-to-post-peak season groups.
Discussion
Exposure to air pollution from wildfire smoke was a significant challenge for health among WLFF. This study highlighted the observed decline in pulmonary function during peak-pollution season among WLFF. The result found a 10 μg/m3 increase in PM2.5 was associated with declines in both the actual and predicted percentages of FVC and FEV1. However, it is worth noting that only the alteration in the predicted FVC percentage demonstrated statistical significance. The finding was reached along with the findings of several studies that demonstrated a decline in pulmonary function following exposure to wood and biomass combustion as PM2.57,8,24,25. Some of the previous studies have demonstrated a dose–response relationship, whereby an increase of 10 μg/m3 in short-term and long-term exposure to PM2.5 is associated with reductions in FEV1 and FVC24,26. We observed mean reductions of 52.64 ml in FEV1 and 114.38 ml in FVC. Nevertheless, the volume change observed in this study was greater than that found in the US WLFF study25. The meta-analysis conducted in occupational studies revealed that an increase of 10 µg/m3 in PM2.5 was associated with a reduction in FVC of 10.0 ml (95% CI − 18.62 to − 1.37 ml) and FEV1 of 7.63 ml (95% CI − 10.62 to − 4.63 ml) for a 10 µg/m3 increase PM2.524. In addition, the studies focused on WLFF showed the cross-shift changes in lung function, with a decline in FEV1 ranging from 30 to 50 ml7,25. Since previous studies primarily examined the immediate effects of occupational exposure after firefighting, it is plausible that repeated exposure could have a more significant impact on the number of declines observed during the study's pre-peak to peak season.
The pre-to-peak WLFF group exhibited a significant decline in FEV1 exceeding 10% from the baseline measurement, despite maintaining normal pulmonary function prior to and during exposure to air pollutants. Specifically, four out of six participants experienced a decline surpassing 15%. The outcome aligned with the conclusions presented by Gaughan DM. et al.7. The study involved US WLFF during the preseason, during-fire, and postseason of wildfires and revealed that 32.7% of US WLFF experienced a decline in FEV1 greater than 10% after a cross-shift, while only one participant demonstrated a decline in FEV1 exceeding 10% across the pre-to-post-peak season. Similar results were noted in studies involving firefighters and farmers exposed to wood and biomass burning7,8,27. These studies showed a decline in both FEV1 and FVC from the preseason to during-fire phase and an increase FEV1 and FVC from during-fire to postseason phase. However, even with the increase, the values remained lower than the baseline measurements. The timing of exposure, duration, lag time, and recovery time are also linked to the response of pulmonary functions. Short-term exposure can lead to cardiopulmonary effects with a lag time ranging from 0 to 7 days28,29. A washout period may play an essential role in the recovery of the pulmonary response to PM2.5. Observations indicate that cessation of exposure to high PM2.5 concentrations for 2–3 months improves pulmonary function7,8,27. In contrast, the study conducted by Jacquin et al. revealed a persistent reduction in FEV1 and FVC among WLFF even 3 months after end of fire season8. It is important to note that chronic exposure to particulate matter continues to have adverse effects on WLFF26. This suggests the potential lasting respiratory consequences can associated with the inhalation of forest fire smoke. Based on the evidence we have, we hypothesize that the WLFF in Chiang Mai was impacted on pulmonary function as a result of seasonal exposure to PM2.5 in the region. Even though ambient and indoor air pollution in this study did not differ significantly between pre-peak and peak seasons, there was still a trend of change in pulmonary function among WLFF without diagnosed abnormal spirometry. In addition, our findings suggested a partial improvement in the lung function with firefighting by the time we conducted our evaluation at the post-peak season. Therefore, further investigation on the recovery phase following the post-season to gather more informative data.
To gain further insight into the potential cause associated with the change in pulmonary function, we assessed the existence of DNA damage in WLFF. Several previous reviews indicate a negative association between particulate matter and DNA via mechanisms of inflammation and oxidative stress12,30,31. Surprisingly, this study found a non-statistical-significant change in DNA TL and DNA TM among pre-peak and pre-post-peak seasons. During the period of data collection, the concentrations of ambient and indoor particulate matter were observed to be lower compared to previous studies that reported significant changes in DNA damage markers32,33. Furthermore, several previous studies concentrated on short periods of exposure, in contrast to our extended monitoring duration34,35. This could be one of the causes of non-statistically significant changes and different DNA damage outcomes. Previously, there was a proposition suggesting that the comet assay might be useful as a suitable technique for monitoring occupational exposure. Nevertheless, the outcomes of its Evaluation of DNA-damaging Exposures in Occupational Environments were subject to controversy36. Comet assays might be more advantageous for assessing exposure than surveillance biomonitoring approaches37.
To our best knowledge, this study is a pioneering study trying to define the health outcomes for wildland firefighters in Thailand and find the tools to be used for proper surveillance. The study tries to assess more specific exposure assessment among WLFF in Thailand by simulating the daily activities of WLFF, including workplace indoor assessment, and comparing it with ambient air at the same time. It also tries to cover all periods of the annual season of pollution, including pre-peak and post-peak seasons. Nonetheless, this study had a few weaknesses that needed to be discussed. First, the duration of follow-up and assessment method may not represent the actual amount of exposure in cases of direct exposure after firefighting in expatriate areas. The event of a wildfire cannot be predicted, and we need to be concerned about interfering with WLFF during wildfire suppression. So, they were not available for us to follow them while wildfire events occurred due to our research team's safety. Second, the non-significant changes observed in certain pulmonary parameters and DNA damage during the peak season could potentially be attributed to the healthy worker effect and the limited sample size. WLFF requires a high level of physical exertion and optimal cardiopulmonary fitness to carry out strenuous job tasks, which may lead to increased physical training and self-care practices. The limited sample size might also have influenced the statistical power to detect significant differences in the measured parameters since a trend toward change in pulmonary parameters was observed.
The findings of this study indicate that Thai WLFF must establish a comprehensive medical surveillance system. We suggested implementing a spirometry pulmonary function test as an essential respiratory health monitoring tool for WLFF. In addition to interpreting spirometry results based on criteria for normal, obstructive, and restrictive abnormalities, it is essential to analyze a substantial decline of 10–15% in forced FEV1 compared with baseline spirometry measurements. It will be essential to implement this comprehensive approach is essential for early detection and optimal management strategies, which can be generalized to WLFF on a global scale. In addition, to reduce or minimize smoke exposure, it is recommended that WLFF implement a rotational work schedule involving the performance of other duties with lower levels of exposure. We also encourage the use of personal protective equipment to reduce smoke and PM2.5 exposure during fire suppression, evidence found that individuals who reported infrequent use of respiratory protection faced a greater risk of experiencing a faster decline in FEV1 compared to those who used it more frequently38. To strengthen the findings in future research, more participants are needed to increase the statistical power and result in more conclusive results. An accurate exposure assessment may be planned, and WLFF may be consulted to determine the proper approach for assessing actual exposure during the suppression of wildfires.
Conclusion
The findings of this study concluded that Thai WLFF had a crucial need to be concerned about their health, either in terms of their fitness for work or their work-related health effects. Pulmonary function deterioration can manifest rapidly, yet there is a lack of evidence regarding the possibility of recovery. Spirometry was essential for identifying early changes in the pulmonary status of WLFF due to their work, which could impact their ability to perform specific job duties. It serves as a valuable tool for health surveillance. Additional research is required to understand the alterations in DNA damage and their potential association with PM2.5 exposure. Real-time exposure evaluation during the process of wildfire suppression may be necessary to make adjustments to an existing exposure assessment methodology.
Data availability
The data presented in this study are available from the corresponding author upon request.
References
WHO. Ambient (outdoor) air pollution Geneva (2021) [updated 22 Sep 2021]. https://www.who.int/news-room/fact-sheets/detail/ambient-(outdoor)-air-quality-and-health
Kinney, P. L. Interactions of climate change, air pollution, and human health. Curr. Environ. Health Rep. 5(1), 179–186 (2018).
Mansoor, S. et al. Elevation in wildfire frequencies with respect to the climate change. J. Environ. Manag. 301, 113769 (2022).
Urbanski, S. P., Hao, W. M. & Baker, S. Chapter 4 Chemical composition of wildland fire emissions. In Developments in Environmental Science Vol. 8 (eds Bytnerowicz, A. et al.) 79–107 (Elsevier, 2008).
Reid, C. E. et al. Critical review of health impacts of wildfire smoke exposure. Environ. Health Perspect. 124(9), 1334–1343 (2016).
Cascio, W. E. Wildland fire smoke and human health. Sci. Total Environ. 624, 586–595 (2018).
Gaughan, D. M. et al. Acute upper and lower respiratory effects in wildland firefighters. J. Occup. Environ. Med. 50(9), 1019–1028 (2008).
Jacquin, L. et al. Short-term spirometric changes in wildland firefighters. Am. J. Ind. Med. 54(11), 819–825 (2011).
Soteriades, E. S., Smith, D. L., Tsismenakis, A. J., Baur, D. M. & Kales, S. N. Cardiovascular disease in US firefighters: A systematic review. Cardiol. Rev. 19(4), 202–215 (2011).
The Department of the Interior. Federal Interagency Wildland Firefighter Medical Standards (2009). https://www.nifc.gov/medical_standards
The Department of the Interior. The Essential Functions and Work Conditions of a Wildland Firefighter U.S. (2009) [updated 5 January 2023; cited 2023 5 January]. https://www.nifc.gov/medical_standards/index.html
Adetona, O. et al. Review of the health effects of wildland fire smoke on wildland firefighters and the public. Inhal. Toxicol. 28(3), 95–139 (2016).
Dong, T. T. T., Hinwood, A. L., Callan, A. C., Zosky, G. & Stock, W. D. In vitro assessment of the toxicity of bushfire emissions: A review. Sci. Total Environ. 603–604, 268–278 (2017).
Liu, D., Tager, I. B., Balmes, J. R. & Harrison, R. J. The effect of smoke inhalation on lung function and airway responsiveness in wildland fire fighters. Am. Rev. Respir. Dis. 146(6), 1469–1473 (1992).
Leonard, S. S. et al. Particle size-dependent radical generation from wildland fire smoke. Toxicology 236(1–2), 103–113 (2007).
Phairuang, W. et al. The influence of the open burning of agricultural biomass and forest fires in Thailand on the carbonaceous components in size-fractionated particles. Environ. Pollut. 247, 238–247 (2019).
Wildfire Statistics [Internet]. Forest Fire Control Office, Department of National Parks, Wildlife and Plant Conservation (2023) [cited 2 July 2023]. https://portal.dnp.go.th/
Panumasvivat, J., Sirikul, W., Surawattanasakul, V., Wangsan, K. & Assavanopakun, P. The urgent need for cardiopulmonary fitness evaluation among wildland firefighters in Thailand. Int. J. Environ. Res. Public Health 20(4), 3527 (2023).
Kanazawa, M. et al. Criteria and classification of obesity in Japan and Asia-Oceania. World Rev. Nutr. Diet. 94, 1–12 (2005).
Singh, N. P., McCoy, M. T., Tice, R. R. & Schneider, E. L. A simple technique for quantitation of low levels of DNA damage in individual cells. Exp. Cell Res. 175(1), 184–191 (1988).
Graham, B. L. et al. Standardization of spirometry 2019 update. An official American Thoracic Society and European Respiratory Society technical statement. Am. J. Respir. Crit. Care Med. 200(8), e70–e88 (2019).
Dejsomritrutai, W. et al. Reference spirometric values for healthy lifetime nonsmokers in Thailand. J. Med. Assoc. Thai 83(5), 457–466 (2000).
Redlich, C. A. et al. Official American Thoracic Society technical standards: Spirometry in the occupational setting. Am. J. Respir. Crit. Care Med. 189(8), 983–993 (2014).
da Silveira, F. A. et al. Environmental and occupational short-term exposure to airborne particles and FEV(1) and FVC in healthy adults: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 18(20), 10571 (2021).
Gaughan, D. M. et al. Exposures and cross-shift lung function declines in wildland firefighters. J. Occup. Environ. Hyg. 11(9), 591–603 (2014).
Edginton, S., O’Sullivan, D. E., King, W. & Lougheed, M. D. Effect of outdoor particulate air pollution on FEV(1) in healthy adults: A systematic review and meta-analysis. Occup. Environ. Med. 76(8), 583–591 (2019).
Agarwal, R., Awasthi, A., Singh, N., Gupta, P. K. & Mittal, S. K. Effects of exposure to rice-crop residue burning smoke on pulmonary functions and oxygen saturation level of human beings in Patiala (India). Sci. Total Environ. 429, 161–166 (2012).
Newell, K., Kartsonaki, C., Lam, K. B. H. & Kurmi, O. P. Cardiorespiratory health effects of particulate ambient air pollution exposure in low-income and middle-income countries: A systematic review and meta-analysis. Lancet Planet. Health 1(9), e368–e380 (2017).
Wong, C. M., Vichit-Vadakan, N., Kan, H. & Qian, Z. Public Health and Air Pollution in Asia (PAPA): A multicity study of short-term effects of air pollution on mortality. Environ. Health Perspect. 116(9), 1195–1202 (2008).
Risom, L., Moller, P. & Loft, S. Oxidative stress-induced DNA damage by particulate air pollution. Mutat. Res. 592(1–2), 119–137 (2005).
Moller, P. et al. Oxidative stress and inflammation generated DNA damage by exposure to air pollution particles. Mutat. Res. Rev. Mutat. Res. 762, 133–166 (2014).
Chu, M. et al. Personal exposure to PM2.5, genetic variants and DNA damage: A multi-center population-based study in Chinese. Toxicol. Lett. 235(3), 172–178 (2015).
Ma, M. et al. Characteristics and oxidative stress on rats and traffic policemen of ambient fine particulate matter from Shenyang. Sci. Total Environ. 526, 110–115 (2015).
Andersen, M. H. G. et al. Assessment of polycyclic aromatic hydrocarbon exposure, lung function, systemic inflammation, and genotoxicity in peripheral blood mononuclear cells from firefighters before and after a work shift. Environ. Mol. Mutagen. 59(6), 539–548 (2018).
Oliveira, M. et al. Firefighters exposure to fire emissions: Impact on levels of biomarkers of exposure to polycyclic aromatic hydrocarbons and genotoxic/oxidative-effects. J. Hazard. Mater. 383, 121179 (2020).
Møller, P., Knudsen, L. E., Loft, S. & Wallin, H. K. The comet assay as a rapid test in biomonitoring occupational exposure to DNA-damaging agents and effect of confounding factors. Cancer Epidemiol. Biomark. Prev. 9(10), 1005–1015 (2000).
Møller, P. The alkaline comet assay: Towards validation in biomonitoring of DNA damaging exposures. Basic Clin. Pharmacol. Toxicol. 98(4), 336–345 (2006).
Schermer, T. R. et al. Change in lung function over time in male metropolitan firefighters and general population controls: A 3-year follow-up study. J. Occup. Health 55(4), 267–275 (2013).
Acknowledgements
We would like to thank Peewara Kanta for assisting with the data collection for this study.
Funding
This research was supported by the Faculty of Medicine, Chiang Mai University, Grant no. 16-2565.
Author information
Authors and Affiliations
Contributions
Conceptualization, J.P., R.S., N.S., S.K.,W.K., W.S., W.I., and P.A.; methodology, J.P., R.S., and P.A.; software, W.K., W.S.; validation, J.P., W.S., and P.A.; formal analysis, R.S., W.K., W.S. and J.P.; investigation, J.P., N.S., S.K., and P.A.; resources, W.I., J.P. and P.A.; data curation, J.P., W.S., and P.A.; writing—original draft preparation, J.P., and P.A.; writing—review and editing, J.P., W.S., R.S., and P.A.; visualization, J.P., and P.A.; supervision, P.A.; project administration, P.A.; funding acquisition, P.A. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Panumasvivat, J., Sapbamrer, R., Sittitoon, N. et al. Exploring the adverse effect of fine particulate matter (PM2.5) on wildland firefighters’ pulmonary function and DNA damage. Sci Rep 14, 7932 (2024). https://doi.org/10.1038/s41598-024-58721-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-58721-4
Keywords
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
