
Abstract
The PI3K-AKT-mTOR pathway lies at the confluence of signaling pathways in which various components are subjected to activating genetic alterations in acute myeloid leukemia (AML), thus contributing to oncogenesis. Three AKT isoforms exist in humans. However, whether one isoform predominates in AML remains unknown. This study reveals that AKT3 behaves very distinctly than AKT1 or AKT2 in both normal myeloid differentiation and AML. During normal differentiation, AKT3 is preferentially expressed in hematopoietic stem cells whilst AKT1 becomes preferentially expressed as cells differentiate into granulocytes or monocytes. AKT2 expression remains unchanged. In AML, AKT3 expression varies widely among patient samples and is counterintuitively high in mature/monocytic leukemia. Furthermore, a low level of AKT3 expression is strongly correlated to genetic alterations associated with a better outcome (NPM1 mutations and RUNX1-RUNX1T1 translocation), while a high level is correlated to alterations associated to a bad outcome (RUNX1 mutations; and SRSF2, U2AF1, SF3B1, ASXL1 and BCOR mutations occurring frequently in MDS and MPN). Consistently, a high AKT3 expression level appears as a very strong predictor of poor survival. Curiously, although modestly varying among AML samples, a high AKT1 expression shows in contrast as a strong predictor of a better patient outcome. These data suggest that AKT3 and AKT1 expressions have strong, yet opposite, prognostic values.
Similar content being viewed by others


Introduction
Acute myeloid leukemia (AML) is a heterogeneous disease. It is characterized by a plethora of genetic alterations including various chromosomal translocations and/or a wide variety of mutations, whose nature allows a classification of patients according to their chances of survival. One classification that has been accepted for several years is that given by the European LeukemiaNet in 2017 (ELN-20171) and updated in 2022 (ELN-20222). Depending on the nature of the cytogenetic abnormalities and mutations detected at diagnosis, this classification divides patients into three groups: the adverse group with a risk of poor survival, the favorable group with an expected better prognosis, and an intermediate group. However, even if this scoring remains a good assessment, the survival of patients in each of these groups can be heterogeneous. The detection of genetic abnormalities at diagnosis can also assist clinicians in recommending targeted therapies, typically prescribed as a second-line treatment. Indeed, the majority of AML patients are first treated with intensive chemotherapy to harness the lethal acute phase. Although some patients are refractory, many go into remission after this induction chemotherapy. To reinforce the treatments and to delay the relapses, patients can then benefit from a milder protocol known as consolidation chemotherapy, and/or benefit from a targeted therapy. There are therapies specifically targeting genetic alterations, such as inhibitors of the mutated FLT3 kinase, inhibitors of the mutated IDH1 and IDH2 enzymes, or molecules targeting DNA methylation, as frequent mutations affect various genes (e.g. DNMT3A, TET2) whose protein products are involved in the regulation of DNA methylation. Targeted therapies include also BCL2 inhibitors, prescribed mainly to unfit patients who are not eligible for intensive chemotherapy. A wide range of molecules targeting less specific features has also been tested in pre-clinical settings as potential therapeutics against AML. These include molecules impinging upon major signaling pathways that are activated in leukemic cells but also in many other cancers. This is for instance the case for compounds inhibiting the AKT protein kinase.
AKT is a serine/threonine kinase playing major roles in intracellular signaling pathways. It is one key actor in the PI3K-AKT-mTOR pathway which senses environmental signals such as growth factors and nutrients availability, and converts these cues into survival, growth and/or proliferation capabilities. Of note, the PI3K-AKT-mTOR pathway controls the rate of protein synthesis and consequent cell growth3, a pre-requisite for entering the cell cycle. Given these critical properties, AKT has attracted much attention from the medico-scientific community, particularly in the cancer field, and AKT inhibitors have been designed for research purposes and for clinical perspectives4. Although AKT itself is rarely mutated in AML, the kinase lies at the confluence of several signaling pathways in which various components can themselves be activated by gene mutations (e.g. FLT3, KIT, NRAS, KRAS, PIK3CB…). However, the use of AKT inhibitors in pre-clinical settings has been disappointing, with an overall non-convincing benefit-to-risk ratio. After all, AKT also plays important physiological roles in healthy cells. Targeting AKT can therefore provoke significant adverse effects which limit the applicable doses. Yet, there are three distinct AKT genes in human, encoding three different proteins: AKT1, AKT2 and AKT3. These three AKT proteins show tissue-specific distributions5 and recent studies indicate that each may exhibit different affinities for various partners and may therefore touch more specifically one pathway than another6. Indeed, although the three human AKTs possess a relatively well conserved overall amino-acid sequence, they harbor some sequence divergences and distinct intracellular localizations. Both of these features might perhaps explain the fact that they can interact with and phosphorylate different partners. However, although some AKT1 versus AKT2 substrate specificities have been identified, much less is known about AKT3 specific targets6. In a more recent report, while AKT1 was described as preferentially located in close proximity of the plasma membrane, AKT2 appeared more cytosolic and AKT3 seemed anchored to the nuclear envelope, facing the cytosol7. In the same report, AKT3 has been suspected to be constitutively activated in a series of established cancer cells (no leukemic cells were included in this study), although the mechanism responsible for such a permanent activation remains unknown. This observation reinforced an earlier report saying that AKT3 is also constitutively activated in a glioma cell line8. Unfortunately, none of the AKT inhibitors available to date exhibit a sufficiently strong isoform specificity to selectively target AKT36. Thus, the development of inhibitors specific to each AKT isoform could be of clinical interest.
In this study, we examined the expression of the three AKT isoforms in a thousand of normal hematopoiesis and AML samples emanating from cohorts established in three different countries (France, USA, Canada). All the data clearly converge toward AKT3 as being the bad in AML.
Results
Expression of the three AKTs in normal myeloid differentiation
To generate a picture of how expression of each of the three AKT genes evolves in the course of differentiation of the myeloid lineages, analyses of healthy samples from the Bloodspot9 and Leucegene public datasets were performed.
We first looked at two independent microarray datasets from the BloodSpot repository (datasets #1 and #2), each containing peripheral blood or bone marrow cells sorted by cytometry with the help of specific markers distinguishing different steps of myeloid differentiation, staging from hematopoietic stem cells (HSCs) to granulocytes or monocytes. In both sets, the data revealed that AKT1 expression shows a bi-phasic but significant increase along granulo or monocytic differentiation, although at the end AKT1 expression appears higher in granulocytes than in monocytes. AKT2 expression remains constant. The expression of AKT3 in HSCs appears in both sets higher than those of AKT1 and AKT2 then decreases gradually but strongly as cells progress toward terminal granulocytes or monocytes, although the decrease is less marked in monocytes of the dataset #2 (Fig. 1A, top and bottom).

Expression of each AKT transcript in normal hematopoiesis. (A) Each dot in the curves shows micro-array normalized expression (log2) of each AKT transcript in cells sorted from individual healthy bone marrow donors of the BloodSpot #1 (top) or #2 (bottom) series of samples as described in the Method section. X axes: HSC = hematopoietic stem cell; HPC = hematopoietic progenitor cell; MPP = multipotent progenitor; CMP = common myeloid progenitor; GMP = granulocyte monocyte progenitor; PM = promyelocyte; MY = myelocyte; MM = metamyelocyte; BC = band cell; PMN = polymorphonuclear cell; Mono = monocyte. Array probes: 207163_s_at (AKT1), 225471_s_at (AKT2), 212609_s_at (AKT3) (top); 207163_s_at (AKT1), 225471_s_at (AKT2), 212607_at (AKT3) (bottom). Other probes gave similar tendencies. (B) Each dot shows RNA-seq normalized expression (log2 RPKM) of each AKT transcript in cells sorted from healthy donors of the Leucegene series as described in the Method section. X axis: CB CD34 + = cord blood CD34 + cells of individual donors; PB CD34 + = peripheral blood CD34 + cells pooled from 4 donors; Granulo = granulocytes; Mono = monocytes. (C) Each dot in the curves shows micro-array normalized expression of each AKT transcript in cells sorted from individual healthy bone marrow donors of the BloodSpot #3 series of samples as described in the Method section. X axis: HSC-1 = HSC CD133 + CD34dim; HSC-2 = HSC CD38- CD34 + ; MEP = megakaryocyte/erythrocyte progenitor; Mega-1 = CFU megakaryocyte; Mega-2 = megakaryocyte; Eryth-1 = eryth.CD34-CD71 + GlyA-; Eryth-2 = eryth.CD34-CD71 + GlyA + ; Eryth-3 = eryth.CD34-CD71loGlyA + ; Eryth-4 = eryth.CD34-CD71-GlyA + . Array probes: 207163_s_at (AKT1), 211453_s_at (AKT2), 212607_at (AKT3). Bars represent medians + /- 95% CI (confidence interval).
To verify these observations in samples from healthy donors where gene expression was measured by another technique, we looked at bulk RNA-seq data of the Leucegene project. This dataset contains sorted CD34+ HSC/progenitor samples from either cord of peripheral blood and granulocytes and monocytes from peripheral blood. As compared to the observations made in BloodSpot microarray datasets #1 and #2, a similar observation was made, with notably a significant lower expression of AKT3 in granulocytes and monocytes (although less marked in monocytes) than in CD34+ HSC/progenitors (Fig. 1B).
Expression of each the three AKTs was then monitored in samples of a third BloodSpot dataset (#3) which contains, among others, normal hematopoietic samples that were sorted with the help of antibodies specific to various stages of differentiation including HSCs, megakaryocytic/erythroid progenitors and intermediary and terminal megakaryocytes and erythrocytes. AKT1 expression goes down as cells differentiate into megakaryocytes, but does not change during erythroid differentiation. AKT2 expression remains always constant, while that of AKT3 diminishes gradually along differentiation into both terminal megakaryocytes and terminal erythrocytes (Fig. 1C).
Taken together, analyses of these four independent data sets converge toward a similar observation: AKT3 expression is elevated in HSCs but goes down as they differentiate into either one of the four branches (granulocytic, monocytic, megakaryocytic or erythroid) of myeloid differentiation.
Expression of the three AKTs in AML samples
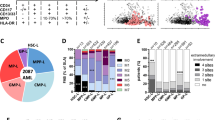
Global expression We first analyzed a bulk ribo-zero RNA-seq we have performed earlier on the blasts of 40 AML patients, a cohort hereafter named IUCT-AML, and in which all samples are with normal cytogenetics (CN-AML)10. The results indicate that expression of AKT3 in blasts is globally weaker than those of AKT1 and AKT2. However, the range of AKT3 expression shows a much wider spectrum among samples, with a roughly ~ 120-fold difference between the sample expressing the most and the one expressing the less AKT3. In the same samples, the variations in AKT1 and AKT2 expressions are very much less marked with an only ~ threefold amplitude for each isoform (Fig. 2A, left). To gain in significance, the expression of AKT was verified in 445 AML diagnosis samples from the Beat-AML public data set (including samples with either normal or abnormal cytogenetics)11 where gene expression was measured by poly(A) RNA-seq. Similar observations were made. Clearly, although globally weaker, AKT3 expression among AML samples is much more variable than those of AKT1 and AKT2 (Fig. 2A, right).

Expression of each AKT transcript in AML samples. (A) Each dot shows RNA-seq normalized expression (log2 RPKM) of each AKT in samples of the IUCT-AML (left, n = 40) or the Beat-AML (right, n = 445) datasets. (B) Each dot shows expression of each AKT in AML FAB categories of the IUCT-AML (left, n = 40) or of the Beat-AML (right, n = 445) cohort. X axes: M0 = undifferentiated; M1 = myeloblastic without maturation; M2 = myeloblastic with maturation; M3 = promyelocytic; M4 = myelomonocytic; M5 = monocytic; M6 = erythroleukemia; M7 = megakaryoblastic. (C) Each dot shows expression of each AKT in hierarchical clustering categories (left, n = 281) or as a function of the PC3-34 score (right, n = 445) of the Beat-AML series of samples. X axes: PRIM = primitive; INT = intermediary; GMP = granulo-monocyte progenitor; MAT = mature. Bars represent medians with 95% CI. Trend curves are shown as dotted lines + coefficients of linear regression (r2).
FAB. We then asked whether expression of each AKT in blasts shows a pattern similar to the one seen during normal differentiation, with notably a decreasing expression of AKT3 as cells progress toward differentiation. To obtain a first indication, we looked in AML samples categorized according to the French-American-British (FAB) classification. Such FAB classification is based on blast morphological aspects and groups AML samples into seven categories (M0-M7), from the less (M0) to the most (M5: monoblastic leukemia; M6: erythroleukemia; M7: megakaryocytic leukemia) differentiated stages. In our IUCT-AML series, which is devoid of M0, M3 and M7 samples, the M4 group contains samples with the highest level of AKT3 expression, although such a visible tendency is not statistically significant. No conclusion can be drawn from the M5 and M6 categories as they contain only 3 and 1 samples, respectively (Fig. 2B, left). However, among the bigger number of Beat-AML diagnosis samples for which the FAB is known (n = 275) and containing many samples in all FAB categories, a significantly higher expression of AKT3 in the M5 category appears, with a noticeable progressive increase in AKT3 expression from M1 to M5 groups. The M3 group, also called “acute promyelocytic leukemia”, and which represents a separate entity characterized by the PML-RARA chromosomal translocation, shows a homogenous pattern of AKT3 expression, and a significant ~ twofold increase in AKT2 expression. Another intriguing observation is that Beat-AML samples of the M0 and M1 (and to a lesser extent of the M2 and M4) categories seem to cluster into two AKT3high and AKT3low subgroups. No conclusion can be drawn from the M6 and M7 categories as they contain only 6 and 3 samples, respectively (Fig. 2B, right). Thus, AKT3 expression in AML samples is apparently following a counterintuitive pattern with the M4/M5 myelomonocytic/monocytic leukemia samples exhibiting the highest levels of AKT3 expression, as opposed to what happens in normal differentiation.
Hierarchical clustering and PC2-34 scoring. As the FAB classification is based only on morphological characteristics, it was important to explore the expression level of each AKT by another approach, especially for the counterintuitive high level of AKT3 expression seen in more mature M4/M5 samples. To do so, we performed new RNA-seq analyses in light of a recent publication which, based on gene expression deconvolution on bulk AML transcriptomes (from TCGA, Beat-AML and Leucegene projects) using single-cell reference profiles of distinct AML stem, progenitor and mature cell types, indicates that AML samples can be categorized into four hierarchical clusters of different degrees of maturation: primitive (shallow hierarchy, LSPC-enriched), GMP (dominated by GMP-like blasts), mature (steep hierarchy, enriched for mature Mono-like and cDC-like blasts) and intermediate (balanced distribution)12. Based on the combined and weighted expression of 34 genes, the authors also defined a score (called PC2-34) which can rank AML samples along the primitive-to-mature branch. First, thanks to the analysis performed earlier with 281 AML samples of the Beat-AML project12, we verified how AKT3 expression distributes in the four hierarchical clusters. As expected from the FAB data presented above, all Beat-AML samples belonging to the mature cluster express a higher level of AKT3 as compared to samples of the less mature GMP cluster. In the primitive and intermediary clusters, AML samples distribute into two sub-groups with different levels of AKT3 expression (Fig. 2C, left). We then looked at the expression of each AKT as a function of the PC2-34 score in the 445 AML samples collected at diagnosis. The data show that as the score increases, i.e. as samples become increasingly mature, the level of AKT3 expression augments globally except for a small subgroup of primitive samples where AKT3 expression is high. Expressions of AKT1 and AKT2 remain relatively constant (Fig. 2C, right).
Taken together, these data suggest that the regulatory mechanisms targeting expression of each AKT in leukemic blasts are distinct than those involved in normal myeloid differentiation, with notably an unexpected high level of AKT3 expression in mature/monocytic leukemia but a lower level in many immature samples.
Expression of the three AKTs and ELN-2017
As AKT3 expression is highly variable among AML samples, we thought it could be significantly correlated to some clinical parameters. We first looked at the expressions of each AKT as a function of the ELN-2017 score which distributes the patients into three groups of differently predicted outcomes: adverse, intermediate or favorable. Here again, AKT3 is clearly distinguishable from the other two AKTs. Unfortunately, in our IUCT-AML cohort encompassing 40 AML samples, no sample is categorized as adverse, but 8 are in the favorable group and 32 are considered as intermediate. Despite the lack of an ELN-2017 adverse group, a strong difference in AKT3 expression is visible between the intermediate and the favorable groups, a low expression of AKT3 being a clear mark of the favorable entity (Fig. 3, left). We then looked at the Beat-AML diagnosis samples for which the ELN-2017 is known (n = 429) and where there is a copious number of samples in each of the three ELN-2017 categories. Consistently with our cohort, samples of the favorable group are those expressing very significantly the less AKT3 as compared to samples of the adverse and intermediate groups (Fig. 3, right). In both cohorts, a slightly higher expression of AKT1 appears in contrast in the favorable group, although the differences are much less pronounced, likely because the expressions of both AKT1 and AKT2 are much less variable among samples than that of AKT3 (Fig. 3).

Expression of each AKT transcript as a function of ELN-2017 score. Each dot shows expression (log2 RPKM) of each AKT as a function of ELN-2017 score in samples of the IUCT-AML (left, n = 40) or of the Beat-AML (right, n = 429) cohort. X axes: Adv = adverse; Int = intermediary; Fav = favorable. Bars represent medians with 95% CI.
Expression of the three AKTs and genetic status
NPM1 mutations. Since the ELN-2017 score is based on the nature of the genetic alterations found in AML samples and because AKT3 expression is significantly higher in the adverse group than in the favorable and intermediate groups, it was probable that some of these genetic abnormalities could be either correlated or anti-correlated to the level of AKT3 expression. We therefore looked at the expressions of the three AKT isoforms as a function of the most frequent mutations in our IUCT-AML cohort. NPM1 is the most frequently mutated gene in AML (approximately 30% of patients). Mutations in NPM1 create a sequence frameshift converting the nuclear localization signal located in the carboxyl-terminus of the protein into a nuclear export signal. As a consequence, the mutant proteins are localized in the cytosol (and are called NPM1c), while the wild-type protein (NPM1wt) shuttles between the nucleus and the cytoplasm. Interestingly, a lower level of AKT3 expression is clearly visible in the 14 NPM1c AML samples as compared to the 26 NPM1wt samples (Fig. 4A, top left).

Expression of each AKT transcript as a function of NPM1 and/or FLT3 mutational status. (A) Each dot shows expression (log2 RPKM) of each AKT as a function of NPM1 mutational status in samples of the IUCT-AML (top left, NPM1c = 14/40) or of the Beat-AML (bottom left, NPM1c = 125/445). Expression of each AKT in the Beat-AML cohort (n = 445) as a function of NPM1 expression in NPM1wt (n = 320) or NPM1c (n = 125) genotype, samples being ranked for each genotype in ascending order of global NPM1 expression (right). (B) Each dot shows expression of AKT3 in 445 samples of the Beat-AML cohort as a function of FLT3-ITD alone (n = 48), FLT3-TKD alone (n = 20), NPM1c alone (n = 58), NPM1c + FLT3-ITD (n = 51) or NPM1c + FLT3-TKD (n = 16) genotype. “wt” means no FLT3 or NPM1 mutation. (C) Expression of AKT3 in 445 samples of the Beat-AML cohort as a function of the PC2-34 score in NPM1wt (n = 320) or NPM1c (n = 125) genotype, samples being ranked for each genotype in ascending order of PC2-34 score. PRIM = primitive; MAT = mature. Bars represent medians with 95% CI. Trend curves are shown as dotted lines + coefficients of linear regression (r2).
To confirm this observation in a bigger series of samples, we repeated this analysis in the Beat-AML cohort which contains 125 NPM1c samples out of 445 AML diagnosis samples for which both the NPM1 mutational status and the RNA-seq data are available. Consistently with our modest cohort, a strong correlation exists here between NPM1c and a low expression of AKT3 (Fig. 4A, bottom left). The expression level each AKT isoform was then plotted as a function of NPM1 expression in either NPM1wt or NPM1c samples. In NPM1wt samples, the expression of AKT3 seems modestly inversely correlated to that of NPM1 (r2 = 0.0182), while no correlation is detected with AKT1 or AKT2. In NPM1c samples such anti-correlation between AKT3 and NPM1 expressions is much more pronounced (r2 = 0.3648) (Fig. 4A, right).
A gene whose mutations are frequently concomitant to those of NPM1 is FLT3. FLT3 can carry two types of mutations: internal tandem repeats (FLT3-ITD) and point mutations in the catalytic tyrosine kinase domain (FLT3-TKD). Whether or not these mutations coexist with that of NPM1 is a parameter affecting patient outcome, especially the combination NPM1c + FLT3-ITD which is of intermediary prognosis, while NPM1c alone is of favorable prognosis. We have therefore checked whether the different combinations between NPM1c and/or FLT3-ITD or FLT3-TKD groups of patient samples can be distinguishable by different levels of AKT3 expression. The results show no significant impact of any of the two types of FLT3 mutations in NPM1wt as well as NMP1c backgrounds, (Fig. 4B). Thus, NPM1c remains the major event associated with a low level of AKT3 expression in AML.
It has been often suggested that the NPM1c mutations in AML is characterized by CD34 negativity and monocytic differentiation. Therefore, to verify whether or not the association between NPM1c and low AKT3 expression is more related to the maturation status than the presence of NPM1c, AKT3 expression levels were plotted as a function of the PC2-34 score in either NPM1wt or in NPM1c samples. While in NPM1wt samples a relative flat distribution (r2 = 0.0225) is observed, in NPM1c samples the level of AKT3 expression is nicely correlated to the PC2-34 score (r2 = 0.5573) (Fig. 4C). This indicates that even if AKT3 expression is globally low in the NPM1c AML entity, it strongly goes up as NPM1c samples loose in immaturity markers.
All together, these data clearly reveal two strong yet independent features associated with different levels of AKT3 expression in AML: (i) many of the samples expressing the less AKT3 are those carrying a mutated NPM1 gene and, (ii) the low level of AKT3 expression increases in NPM1c blasts as cells progress toward a mature phenotype (as opposed to what happens in normal hematopoietic differentiation).
RUNX1 mutations & RUNX1-RUNX1T1 translocation. No significant correlation between expression of each of the three AKTs and any other mutation could be detected in our IUCT-AML cohort. However, this lack of correlation might be explained by the fact that many mutations are much less frequent than the mutations of NPM1, and therefore do not permit statistical analyses within a series containing 40 samples. However, correlations between the expression level of AKT3 and the Runt-related transcription factor 1 (RUNX1) genetic alterations emerged in the 445 diagnosis samples of the Beat-AML cohort. Indeed, AKT3 expression appears very significantly higher in the 47 samples harboring mutations in RUNX1, and in contrast significantly lower in the 13 samples harboring the t(8;21) (RUNX1-RUNX1T1) chromosomal translocation (Fig. 5, left). We then plotted le level of expression of the three AKT isoforms as a function of RUNX1 expression in either RUNX1wt, RUNX1mut or RUNX1-RUNX1T1 samples. In RUNX1wt samples, the expression of AKT3 appears somehow inversely correlated to global expression of RUNX1 (r2 = 0.1722), while no correlation is detected with AKT1 or AKT2. In RUNX1mut and RUNX1-RUNX1T1 samples no correlation between any of the three AKTs and global expression of RUNX1 is visible (Fig. 5, right).

Expression of each AKT transcript as a function of RUNX1 genetic status. Each dot shows expression (log2 RPKM) of each AKT as a function of RUNX1 mutation (mut, n = 47) or RUNX1-RUNX1T1 translocation (t, n = 13) in the 445 samples of the Beat-AML cohort (“wt” (n = 385) means no RUNX1 mutation or translocation) (left). Expression of each AKT in the 445 samples of the Beat-AML cohort as a function of RUNX1 expression in RUNX1-wt (wt, n = 385), RUNX1-mut (mut, n = 47) or RUNX1-translocated (t, n = 13) genotype, samples being ranked for each genotype in ascending order of global RUNX1 expression (right). Bars represent medians with 95% CI. Trend curve is shown as dotted line + coefficient of linear regression (r2).
These data show a strong upregulation of AKT3 in AML samples carrying a mutated RUNX1 gene, but in contrast a downregulation in samples harboring the RUNX1-RUNX1T1 translocation. Furthermore, the level of AKT3 expression appears inversely proportional to that of RUNX1 in RUNX1wt samples, a tendency no longer visible in RUNX1 genetic variant samples.
SRSF2, U2AF1, SRSF3, ASXL1 and BCOR mutations, and relations with MDS and MPN. In the 445 diagnosis samples of the Beat-AML cohort, a correlation between high levels of AKT3 expression and mutations of SRSF2 (n = 46), U2AF1 (n = 24), SRSF3 (n = 17), ASXL1 (n = 43) or BCOR (n = 23) is also observed (Fig. 6, left). Mutations in these genes are very frequent in myelodysplastic syndromes (MDSs) and myeloproliferative neoplasms (MPNs). MDS and MPN are two hematological disorders at risk for the onset of AML, and mutations in the related genes are categorized in the ELN-2017 adverse group. It was therefore of interest to verify the level of expression of each AKT in AML samples that developed after a MDS or a MPN. Such analyses were performed in the Beat-AML cohort. The data obtained reveal that among the 445 samples collected at diagnosis, those from patients who developed a prior MDS or a prior MPN exhibit a higher level of AKT3 expression (although not significant for the “prior MPN” category likely due to an insufficient number of samples), but not of AKT1 or AKT2 (Fig. 6, right).

Expression of each AKT transcript as a function of SRF2, U2AF1, SF3B1, ASXL1 or BCOR mutations and of prior MDS or prior MPN hematological disorders. Each dot shows expression (log2 RPKM) of each AKT as a function of SRSF2 (n = 46), U2AF1 (n = 24), SF3B1 (n = 17), ASXL1 (n = 43) or BCOR (n = 23) mutations in 445 samples of the Beat-AML cohort (“wt” means no mutation in any of these 5 genes) (left), or in 445 samples but classified according to whether or not patients developed a MDS (n = 32), a MPN (n = 18) or a combination of both (n = 12) before the onset of leukemia (right). Bars represent medians with 95% CI. Student t tests were here calculated after having grouped mutant (left) or MDS + MPN + both (right) samples.
These data show an upregulation of AKT3 expression in AML samples carrying mutations in SRSF2, U2AF1, SRSF3, ASXL1 or BCOR, and consistently in samples of patients who developed a leukemia after a MDS or a MPN.
Expression of the three AKTs and overall survival
All the aforementioned observations argued in favor of a bad prognostic value for AKT3 expression. Indeed, samples of the ELN-2017 group express a higher amount of AKT3. Also, the level of AKT3 expression is lower in leukemic blasts harboring NPM1 mutations or the RUNX1-RUNX1T1 translocation which are both of better prognosis, but higher in samples harboring RUNX1, SRSF2, U2AF1, SF3B1, ASXL1, or BCOR mutations which are of bad prognosis. To assess the prognostic impact of each AKT, the patient overall survivals were first evaluated by Kaplan–Meier curves using the Beat-AML dataset. To avoid potential bias in data interpretation, we removed here the samples that were not collected at diagnosis but later after the first line of therapy, those presenting with no AML but with an MDS or a MPN, and the samples from patients who could benefit from a transplantation (either bone marrow or cord blood cells engraftment). The Kaplan–Meier curves were finally plotted for each AKT with such a homogeneous set of n = 239 patients (Fig. 7A). Once more, AKT3 behaved distinctly. Its expression level is highly correlated to a poor outcome (p = 0.0004), while AKT2 expression cannot distinguish two groups with a significant difference (p = 0.4550). The data obtained with AKT1 were very surprising. As opposed to AKT3, its expression level correlates significantly to a better survival (p = 0.0422).

Kaplan–Meier curves showing the overall survival of AML patients as a function of expression each AKT transcript. (A) Data obtained from the Beat-AML cohort (n = 239). (B) Data obtained from the Leucegene cohort (n = 373).
Given these strong, yet opposite, predictive values of AKT1 and AKT3 expression levels, it was important to verify whether similar counterintuitive observations could be made in another consistent cohort. We therefore looked at the Leucegene public dataset encompassing 373 AML samples. As no clinical information can be obtained with the Leucegene cohort, were here downloaded the Kaplan–Meier overall survival curves as they appear online. We could not select the samples to provide information on a homogeneously treated set of patients. Yet, the results were very similar to those obtained with the Beat-AML cohort. High AKT3 expression appears as a powerful predictor of poor survival (p = 0.0000), while in contrast AKT1 shows as a strong predictor of better survival (p = 0.0012), and no significant difference can be highlighted using AKT2 expression as a parameter (p = 0.1648) (Fig. 7B).
In each dataset, samples are split into 2 categories (AKThigh or AKTlow) based on median gene expression value.
Discussion
Prognostic values of AKT1 and AKT3 That a higher expression of AKT3 appears as a marker of bad prognosis is not surprising for a kinase lying in the PI3K-AKT-mTOR pathway so important for cancer cell growth and survival. What is quite counterintuitive, is the exact opposite prognostic value of AKT1 expression. Our search in the literature of which of the AKT1 versus AKT3 kinase specific substrate(s) could provide a probable explanation remained unsuccessful. The expanding list of such specific substrates will certainly help elucidating this mystery. Yet, this discrepancy highlights the need to search for specific inhibitors capable of discriminating each of the three AKT protein isoforms. Up to now, the vast majority of experimental works designed at describing the function of AKT in cancer cells was performed using panAKT inhibitors. If the three AKT kinases have distinct or even opposite effects on a biological function, as is the case for instance in vascular tumors where AKT1 and AKT3 kinases exhibit opposite effects on endothelial cell growth13, this may have generated biases in data interpretation.
What could be the advantage for HSCs or leukemic blasts to express AKT3? As said in the introduction, a recent report indicates that unlike AKT1 and AKT2, the AKT3 kinase locates at the nuclear envelope, facing the cytosol, and its protein serine/threonine kinase activity appears constitutively activated in a panel of established cancer cells6. As no leukemic cell lines were included in this earlier study, it would be interesting to check whether leukemic blasts express also a constitutive AKT3 kinase. Given the cellular functions of AKTs this would confer a serious survival/proliferation advantage, notably in mature/monocytic-like blasts expressing a higher than expected level of AKT3 expression.
Relationship between AKT3 and NPM1wt or NPM1c A recent report showed that NPM1wt and NPM1c proteins exhibit opposite effects on AKT kinase activation in leukemic blasts. Indeed, it was shown there that the NPM1c protein physically associates with AKT and antagonizes the inhibitory effect of NPM1wt on AKT phosphorylation. Interestingly, this leads to enhanced sensitivity of NPM1c leukemic blasts to AKT inhibitors14. However, in this report were used only anti-AKT and anti-phosphoAKT antibodies that cannot discriminate the three AKT protein isoforms (i.e. panAKT antibodies). Therefore, it is yet not known whether NPM1c interacts preferentially with one or another of the AKT kinases. This merits further investigations.
Relationship between AKT3 and RUNX1wt, RUNX1mut or RUNX1-RUNX1T1 Another striking observation in our study is the inverse correlations between elevated AKT3 expression and RUNX1mut in one hand, and diminished AKT3 expression and RUNX1-RUNX1T1 translocation in the other hand, as compared to RUNX1wt samples. Here again, whether and how molecularly the two mutated or translocated RUNX1 variants could control AKT3 transcript expression in opposite ways, or whether these events are solely correlated with no causal connection, remains unknown. This warrants further investigation to experimentally determine whether in the myeloid lineage the RUNX1 transcription factor or its mutant or translocated variants interact directly with the AKT3 gene locus. A recent report suggests that the RUNX1 transcription factor does indeed interact directly with the AKT3 locus, although this was shown in lung15. In a clinical perspective, the very low expression of AKT3 in RUNX1-RUNX1T1 AML suggests it would be preferable to target AKT1 or AKT2 kinase in this leukemic entity. This is consistent with an earlier report which indicated that RUNX1-RUNX1T1 blasts harbor an activated AKT1 kinase and are specifically sensitive to AKT1 inhibition both in vitro and in vivo settings16.
Relationship between AKT3 and mutations related to MDS or MPN hematological disorders The MDS- or MPN-related mutations affect genes involved in different molecular aspects of gene expression including RNA splicing (SRSF2, U2AF1 and SF3B1), chromatin remodeling (ASXL1) and gene transcription (BCOR). It is therefore hard to anticipate how mutations in these different sorts of genes could impact AKT3 expression. A quick glance at how AKT3 RNA-seq reads align to the AKT3 locus failed to reveal any change in the pattern of AKT3 mRNA splicing that might have been responsible for the higher AKT3 mRNA expression in splicing mutant samples (data not shown). In addition, as opposed to what was seen with NPM1 or RUNX1 genetic alterations, no correlation could be established between expression of ASXL1 or BCOR (either wild types or mutants) to that of AKT3 (data not shown), suggesting no direct link between the transcriptional activity of ASXL1 or BCOR and the expression of AKT3.
AKT3, genetic alterations and the degrees of blast maturation and aggressiveness Taken together these data indicate that AKT3 expression is highly variable among AML samples and that different kind of gene mutations/translocations are associated with either high or low AKT3 expression. One feature which is more globally and positively correlated to AKT3 expression is the degree of blast maturation (as opposed to healthy myeloid differentiation). We therefore favor a model whereby the causes of variable AKT3 expression in AML may be multiple, but ultimately the most aggressive leukemic blasts are characterized by a high level of AKT3.
Methods
Donors, patients and tumor samples
Normal hematopoiesis. For studying normal hematopoiesis, three different datasets of the BloodSpot repository available on-line (https://www.bloodspot.eu)9 were used: (i) the dataset in the “Normal human hematopoiesis (HemaExplorer)” tab (here called bloodSpot #1); the dataset in the “Normal hematopoiesis with AMLs” tab (here called BloodSpot #2); (iii) the dataset in the “Normal human hematopoiesis (DMAP)” tab (here called BloodSpot #3). They all contain normalized and quantified micro-array data (log2) from normal hematopoiesis samples. See the figure legends for details on the micro-array probes. Were also used data from the Leucegene project (GSE48846 and GSE51954) containing poly(A) RNA-seq of sorted CD34+ HSC/progenitor cells from either cord of peripheral blood and sorted granulocytes or monocytes from peripheral blood.
IUCT-AML cohort. AML patients were diagnosed, sampled and treated in our medical center and registered at the HIMIP (Hémopathies INSERM Midi-Pyrénées, France) collection. In this study, 40 cytogenetically normal AML (CN-AML) samples collected at diagnosis and for which the genetic status is known (including mutations and chromosomal translocations) were analyzed. Detailed clinical data related to these 40 patients have been published earlier9.
Ethics approval. In accordance with French law, each patient was informed and the HIMIP collection has been declared to the Ministry of Higher Education and Research (DC 2008–307) and a transfer agreement has been obtained (AC 2008–129) after approbation by the local ethical committee (“Comité de Protection des Personnes Sud-Ouest et Outremer II”). Clinical and biological annotations have also been declared to the CNIL (“Comité National Informatique et Libertés”). This study was conducted in accordance with the Declaration of Helsinki.
Beat-AML cohort
As a validation cohort for gene expression, were used the data of the Beat-AML project available on-line at http://vizome.org/aml2. This repository contains the genetic status (including mutations and chromosomal translocations) and quantified and normalized poly-(A) RNA-seq data of bone marrow or peripheral blood samples from healthy donors, and MDS, MPN and AML patients. In addition to sampling at diagnosis, a number of patient have also been collected at different times post-diagnosis. To explore a homogenous set of samples, the analyses in this study were performed only on AML samples that were collected at diagnosis and for which the genetic status and RNA-seq data are available, i.e. n = 445 AML samples.
Overall survival Kaplan–Meier curves
For calculating the probability of survival, data from the Beat-AML and from the Leucegene projects were used. The Beat-AML cohort (http://vizome.org/aml2) proposes for each patient quantified and normalized poly-(A) RNA-seq (expressed in log2 RPKM) and matched survival data. For Kaplan–Meier curves the cohort was split into 2 categories based on median expression value of each AKT gene (see the results section for precisions on the samples that were included in survival analyses). The Leucegene projects (https://data.leucegene.iric.ca/survival?lang=en) proposes directly the relationship between gene expression and clinical outcome in terms of survival. The cohort is also split into 2 categories based on median gene expression value. The survival cohort consists of 373 diagnostic AML samples (excluding acute promyelocytic leukemia). Gene expression was generated using STAR/RSEM and GRCh38 (Gencode32) and is expressed in TPM.
For each cohort, overall survival (OS) time was calculated from the date of diagnosis until death or last received news. Surviving patients were censored at the date of last follow-up.
RNA extraction, ribo-depletion and reverse transcription.
Total RNAs from the 40 CN-AML samples were extracted with the TRIzol reagent (Ambion, Austin, TX, USA). RNA integrity was evaluated using the RNA 6000 Nano Chip kit (Agilent Technologies, Massy, France). Only RNA extracts with RNA integrity values ≥ 7 underwent further reverse transcription. rRNA depletion was performed from total RNA with Ribo-Zero™ rRNA Removal Kits (Epicentre, Madison, WI, USA). All samples were reverse transcribed using the Superscript II reverse transcription kit (Invitrogen, Beijing, China), according to the manufacturer's protocol.
RNA-seq
RNA sequencing of the 40 CN-AML samples was performed at the BGI (Hong Kong). Paired-end, strand-specific reads of ~ 100 nucleotides were generated on an Illumina HiSeqTM2000. Alignment and mapping were performed using Tophat1 against the hg19 genome and the mapped reads were assembled by Cufflinks 2.0.22. The Cuffcompare program was used to merge the RefSeq, ENCODE and UCSC human known genes freeze January 2013 into one gene annotation set for comparison with the assembled transcripts17.
Statistical analyses
Unpaired Student t test (*: p < 0.05, **: p < 0.01, ***: p < 0.005, ****: p < 0.001) was used for sample inter-group significance. Linear regression (r2) was used for trend curves. Log-rank test was used for Kaplan–Meier curves.
Data availability
The raw and processed RNA-sequencing data generated in this study have been deposited at the National Center for Biotechnology Information Gene Expression Omnibus (repository number GSE62852).
References
Döhner, H. et al. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood. 129(4), 424–447 (2017).
Döhner, H. et al. Diagnosis and management of AML in adults: 2022 recommendations from an international expert panel on behalf of the ELN. Blood. 140(12), 1345–1377 (2022).
Faridi, J., Fawcett, J., Wang, L. & Roth, R. A. Akt promotes increased mammalian cell size by stimulating protein synthesis and inhibiting protein degradation. Am. J. Physiol. Endocrinol. Metab. 285(5), E964–E972 (2003).
Smit, D. J. & Jücker, M. AKT Isoforms as a Target in Cancer and Immunotherapy. Curr. Top. Microbiol. Immunol. 436, 409–436 (2022).
Masure, S. et al. Molecular cloning, expression and characterization of the human serine/threonine kinase Akt-3. Eur. J. Biochem. 265, 353–360 (1999).
Degan, S. E. & Gelman, I. H. Emerging roles for AKT isoform preference in cancer progression pathways. Mol. Cancer Res. 19(8), 1251–1257 (2021).
Wainstein, E., Maik-Rachline, G., Blenis, J. & Seger, R. AKTs do not translocate to the nucleus upon stimulation but AKT3 can constitutively signal from the nuclear envelope. Cell Rep. 41(10), 111733 (2022).
Mure, H. et al. Akt2 and Akt3 play a pivotal role in malignant gliomas. Neuro Oncol. 12(3), 221–232 (2010).
Bagger, F. O. et al. BloodSpot: a database of gene expression profiles and transcriptional programs for healthy and malignant haematopoiesis. Nucleic Acids Res. 44(D1), D917–D924 (2016).
De Clara, E. et al. Long non-coding RNA expression profile in cytogenetically normal acute myeloid leukemia identifies a distinct signature and a new biomarker in NPM1-mutated patients. Haematologica. 102(10), 1718–1726 (2017).
Tyner, J. W. et al. Functional genomic landscape of acute myeloid leukaemia. Nature. 562(7728), 526–531 (2018).
Zeng, A. G. X. et al. A cellular hierarchy framework for understanding heterogeneity and predicting drug response in acute myeloid leukemia. Nat. Med. 28(6), 1212–1223 (2022).
Phung, T. L. et al. Akt1 and akt3 exert opposing roles in the regulation of vascular tumor growth. Cancer Res. 75(1), 40–50 (2015).
Ren, Z. et al. Opposing effects of NPM1wt and NPM1c mutants on AKT signaling in AML. Leukemia. 34(4), 1172–1176 (2020).
Xiao, C. et al. RUNX1 targeting AKT3 promotes alveolar hypercoagulation and fibrinolytic inhibition in LPS induced ARDS. Respir. Res. 25(1), 54 (2024).
Wang, L. et al. Regulation of AKT signaling by Id1 controls t(8;21) leukemia initiation and progression. Blood. 126(5), 640–650 (2015).
Trapnell, C. et al. Differential gene and transcript expression analysis of RNA-seq experiments with TopHat and Cufflinks. Nat. Protoc. 7(3), 562–578 (2012).
Acknowledgements
Some of the results obtained in this publication are based upon data generated by the Leucegene group primarily located at IRIC in Montreal, Canada and supported by Genome Canada and Genome Québec. This data was made possible through human AML specimens provided by the BCLQ, Montreal, Canada.
Funding
The study was supported by the INSERM, Labex Toucan, Fondation Leucémie Espoir, Ligue Régionale Contre le Cancer, Fondation ARC, Association Laurette Fugain (ALF2018/03) and Cancéropôle Grand Sud-Ouest. E.C. was supported by Ligue Nationale Contre le Cancer, Société Française d’Hématologie and Labex Toucan. C.S. was supported by Fondation Toulouse Cancer Santé, Région Occitanie and Fondation pour la Recherche Médicale. R.P. was supported by Ministère de l’Enseignement Supérieur et de La Recherche. C.B. was supported by Fondation de France. S.D. was supported by a grant from the French Ministry of Health and the French National Cancer lnstitute (CircOma, PRT-K 2022-184).
Author information
Authors and Affiliations
Contributions
S.P. wrote the manuscript. C.R, M.B. and S.P. contributed to the study’s design, conception and analysis of the data. E.C, C.S., R.P, C.M., C.B. and M.B. prepared the material, collected and contributed to analyses. S.D. contributed to new analyses during manuscript revision. F.M and C.T. commented on and edited the manuscript.
Corresponding author
Ethics declarations
Competing interests
C.R. declares a consulting or advisory role with Abbvie, Amgen, Astellas, BMS, Boehringer, Jazz Pharmaceuticals and Servier, and received research funding from Abbvie, Amgen, Astellas, BMS, Iqvia and Jazz Pharmaceuticals. All other authors declare no conflict of interest.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Corre, E., Soum, C., Pfeifer, R. et al. Differential prognostic values of the three AKT isoforms in acute myeloid leukemia. Sci Rep 14, 7070 (2024). https://doi.org/10.1038/s41598-024-57578-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-57578-x
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
