
Abstract
This study aimed to establish sex- and age-specific reference values for motor performance (MP) in Hong Kong preschoolers aged 3–5 years old and examine the relationship between MP and BMI status. A cross-sectional study was conducted among 5579 preschoolers in Hong Kong. Three MP tests were administered, and height and weight information were collected. GAMLSS was used to compute the normative values of the motor tests. Boys outperformed girls in activities requiring muscle strength and power, while girls outperformed boys in activities requiring balance and coordination. The MP scores increased with age for both overarm beanbag throw and standing long jump for both sexes, while the one-leg balance scores showed larger differences between P50 and P95 in older preschoolers. Children with excessive weight performed worse in standing long jump and one-leg balance compared to their healthy weight peers. This study provides valuable information on the MP of preschoolers in Hong Kong, including sex- and age-specific reference values and the association between BMI status and MP scores. These findings can serve as a reference for future studies and clinical practice and highlight the importance of promoting motor skill development in preschoolers, particularly those who are overweight or obese.
Similar content being viewed by others


Introduction
Motor performance (MP) is the ability of a child to perform basic gross motor skills, which are movements used in daily life and physical activity1. Encouraging motor skills in early childhood may be a practical approach to maintaining engagement in physical activities throughout the stages of childhood and adolescence2,3. The preschool years are crucial for improving MP due to the "proficiency barrier," which prevents individuals with low motor skills from engaging in lifelong physical activity1,3,4. While physical fitness is regarded as a powerful health indicator in children5,6, MP is a component of physical fitness in preschool years that is linked to sports performance and motor skills7,8,9,10. During this time, children develop fundamental motor skills that they later apply to both organized and unorganized physical activity11. These skills are crucial for children to participate in sports as adults12,13.
Standardized measurements have been reported for schoolchildren above 6 years old from various populations14,15,16,17,18. However, literature addressing reference data of MP among preschoolers (3–5 years old) is rather scarce7,19,20,21. A set of tests for MP in Hong Kong preschoolers was developed 20 years ago9. The development of children’s motor skills and coordination in preschoolers has shown signs of a secular decline22,23. Recent research linking poor MP in typically-developing preschool children to low levels of physical activity highlights the importance of monitoring typically-developing children using standardized measurements24.
Childhood obesity is a significant public health concern as it increases the risk of chronic diseases such as hypertension, type 2 diabetes, stroke, cardiovascular disease, hyperlipidaemia, certain types of cancer, and decreased life expectancy25. The World Health Organization reported that approximately 39 million children under the age of 5 were overweight or obese in 2020, and children below 5 years old have shown a rapid increase in the development of obesity in recent years26. Previous studies have shown a negative association between school-aged childhood obesity and MP27,28,29. However, the relationship between obesity and MP in preschoolers is unclear30,31, and the available data is limited31,32,33,34. Most previous reports used body mass index (BMI) or percentage of body fat as continuous variables instead of categorical variables to determine the association with MP and coordination in young children, and their sample sizes were small31,34,35,36,37. Given the importance of obesity and fitness as predictors of health-related factors, it is essential to identify their relationship in preschool years. Additionally, improvements in fitness have been shown to reduce the risk of becoming overweight/obese during adolescence28,38,39 and BMI-related impairments in MP start to emerge in preschool age37,40,41,42.
Therefore, this study aimed to provide sex-and age-specific MP reference for preschoolers aged 3–5 years old in Hong Kong. This study also addressed sex-related differences across this age period, as well as the relationship between MP and BMI status in preschoolers.
Results
Descriptive characteristics
A total of 5579 preschoolers aged 3–5 years were enrolled in 63 kindergartens, comprising 2916 boys and 2663 girls. The mean age of the study population was 4.5 years. Descriptive characteristics of the participants are presented in Table 1. Boys were found to be taller than girls (105.2 cm vs 103.8 cm, p < 0.001), but there was no significant difference in weight by sex. BMI categories were utilized to classify BMI status, with the majority of children (88.0%) classified as having a healthy weight, 7.7% classified as having an excessive weight (overweight or obese), and 4.3% classified as underweight. BMI status classifications were similar between boys and girls (p = 0.072). The average results of the fitness tests for overarm beanbag throw, standing long jump, and one-leg balance were 299.1 cm, 74.1 cm, and 18.4 s, respectively. Significant sex differences were observed in all MP tests (all p values < 0.001), with boys performing better in overarm beanbag throw (313.6 cm vs 283.3 cm, p < 0.001) and standing long jump (75.7 cm vs 72.4 cm, p < 0.001), and girls performing better in one-leg balance (20.7 s vs 16.2 s, p < 0.001).
The fitted models
Table 2 presents a summary of the fitted models. The effective degrees of freedom (μ) for all models were found to be greater than 2, suggesting that there was no linear relationship between age and medians of fitness test scores for either boys or girls. Additionally, the majority of effective degrees of freedom (ν) were greater than 2, indicating that there was no linear relationship between age and skewness.
Normative values and centile curves of the MP scores
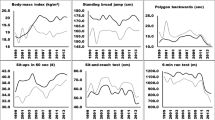
Table 3a–c provide the normative values of the MP tests presented as percentiles ranging from 5 to 95th Smoothed centile curves (P5, P10, P20, P30, P40, P50, P60, P70, P80, P90, and P95) relative to an age interval of 1 month for the MP scores by age and sex for children are presented in Fig. 1a–c. The tables and figures demonstrate that boys outperformed girls in the overarm beanbag throw and standing long jump, while girls outperformed boys in the one-leg balance. The MP scores for overarm beanbag throw and standing long jump increased steadily with age for both sexes. In the one-leg balance test, we observed larger differences between P50 and P95 in older preschoolers than in their younger counterparts (Fig. 1c). The skewness of one-leg balance time increased with age for both boys and girls. Our findings suggest that there are linear changes based on relative age in the various dimensions of tests studied in preschoolers.

Percentile curves for overarm beanbag throw, standing long jump and one-leg balance for boys and girls.
Association between BMI status and MP z-scores
Table 4 presents a comparison of the MP z-scores among BMI status groups. We observed significant differences in the z-scores of all tests among the groups. The mean test scores of children with excessive weight were found to be significantly lower than the other groups (p < 0.001) when compared to children with healthy weight, except for overarm beanbag throw. Children with excessive weight performed best in overarm beanbag throw (p < 0.001) but performed worse in standing long jump (p < 0.001). The one-leg balance score in children with healthy weight was better than those with excessive weight (− 0.196 vs 0.019, p < 0.001).
Discussion
This study established sex- and age-specific reference values for MP in Hong Kong preschoolers aged 3–5 years old and examined the relationship between MP and their BMI status. The findings of this study provide valuable information on the MP of preschoolers in Hong Kong, which can serve as a reference for future studies and clinical practice. The results showed that boys have better performance in activities requiring muscle strength and power, while girls have better performance in activities requiring balance and coordination. These findings are consistent with previous studies that have reported sex differences in MP7,8,9,43.
The MP scores increased steadily with age for both overarm beanbag throw and standing long jump for both sexes, which is consistent with previous studies7,9,30,44. In older preschool children, the difference in one-leg balance scores between the P50 and P95 was greater compared to younger preschool children. This finding is similar to the results of a 2019 study conducted on Spanish preschoolers7, indicating that children who have not developed good balance skills during their early years may struggle to catch up with their peers as they grow older. Our findings support that both age and sex significantly affect balance skill in preschoolers, as suggested by Franjoine et al. in 201045 and Latorre Roman et al. in 201746. This highlights the importance of early intervention to promote motor skill development in preschoolers.
The study revealed a significant correlation between BMI status and MP scores, indicating that children with excessive weight performed worse in standing long jump and one-leg balance compared to their healthy weight peers. These findings are consistent with previous studies that have reported a negative association between childhood obesity and MP in school children28,29,35,47 and suggest that MP is probably linked to the obesity and weakened musculoskeletal abilities of excessive weight children32. Additionally, this finding emphasizes the potential impact of muscular development in reducing the disparity in MP based on BMI status. The observed inconsistencies in our results, such as the lower mean test scores of children with excessive weight compared to those with healthy weight, except for overarm beanbag throw, can be explained by this finding. The ability to jump is a crucial skill that is often utilized in activities that require high energy expenditure. If obese children have limitations in this area, they may be less likely to participate in sports and physical activities that require jumping48,49. This reduced engagement in sports and physical activities that involve jumping may contribute to the continued presence of excessive body weight and additional fat accumulation50. Overall, the results of this study suggest that the negative association between obesity and MP may already be present in the preschool years.
To interpret the results of the MP assessment, it is necessary to compare the individual score with reference values for the general population, taking into account factors such as sex and age. Therefore, this research provides normative values of the general population, which allows for the assessment to compare the ability of Hong Kong children at defined ages. Physical fitness below P5 may be a sign of a potentially pathological condition, according to previous publications14,17. The lowest percentile can be used as a ''warning signal'' to perform additional tests to identify potential motor delays. Poor MP may motivate those who are directly responsible, such as parents, doctors, or the school community, to take action.
One limitation of this study is that it was cross-sectional, which limits the ability to establish causality between BMI status and MP scores. Future longitudinal studies are needed to examine the relationship between changes in BMI status and changes in MP scores over time. While BMI is a widely used measure for assessing health risk in preschoolers, it may not provide a complete picture of body composition. Markers of body fat, such as skinfold thickness or bioelectrical impedance, may offer a more accurate assessment of body composition. Nevertheless, the results of this study revealed a correlation between BMI status and MP scores, with overweight children exhibiting poorer performance in standing long jump and one-leg balance compared to healthy weight preschoolers. To determine the sequential relationship between BMI status and MP development, longitudinal studies are necessary. Another limitation is that the study sample was limited to kindergartens in Hong Kong, which may not be representative of the entire population of preschoolers in other regions. Although there is a lack of extensive research on the long-term effects of tested motor performance, the present study provides recommendations on the necessary tests to be conducted and how to obtain valuable reference values. However, further research is needed to fully understand the long-term implications.
Conclusion
In conclusion, this study provides valuable information on the MP of preschoolers in Hong Kong, including sex- and age-specific reference values and the association between BMI status and MP scores. These findings can serve as a reference for future studies and clinical practice and highlight the importance of promoting motor skill development in preschoolers, particularly those who are overweight or obese. MP is crucial for younger children due to global decline trends in physical activity22,23. It is important to prioritize MP at an early age to prevent future health issues and foster a lifelong habit of physical activity.
Methods
Participants and data collection
This cross-sectional study was conducted in kindergartens participating in the Hong Kong Growth Study and a contemporary community study, both of which aimed to collect updated data on growth parameters and support children's holistic development. To compile a sampling frame of all kindergartens in Hong Kong, a list of kindergartens from the "Profile of Kindergarten and Kindergarten-cum-child care centres, Education Bureau" was used for the Hong Kong Growth Study. Five kindergartens were randomly selected from each of the 5 major regions in Hong Kong-Hong Kong Island, New Territory East, New Territory West, Kowloon East, and Kowloon West-based on computer-generated random numbers according to the numbers of schools per region. If a selected school declines to participate in a study, the next school in the random selection process is invited to take its place. This ensures that the sample remains representative and helps maintain the integrity of the study.
In this study, all children who belong to the selected classrooms were invited to participate. Three MP tests including the one-leg balance (OB), standing long jump (SLJ) and beanbag throwing (BT) were administered to preschoolers to measure the students’ gross motor development and performance in static balance and muscle strength (both upper and lower limbs). These tests were adapted from the PREFIT fitness battery51 and Hong Kong Pre-school Motor Performance Award Scheme9. These tests were chosen because they were found to be reliable (r > 0.71) in preschoolers and could represent overall health among young children9,51. The study also incorporates data on height and weight. Data collection took place between December 2019 and August 2022. An informed consent form was voluntarily signed by parents allowing their children to take part in the study. The study was conducted in accordance with the Declaration of Helsinki, and approved by Ethics approval for HKGS was obtained from the Joint Chinese University of Hong Kong-New Territories East Cluster Clinical Research Ethics Committee (CREC ref. no. 2019.575), the University of Hong Kong-Hospital Authority Hong Kong West Cluster Joint Institutional Review Board (UW 18-593, UW 17-491) and the Ethics Committee of the Department of Health, Hong Kong SAR Government (LM 307/2018).
MP tests
Fundamental motor skills such as walking, running, skipping, and rolling play a crucial role in physical fitness, as they contribute to the development of strength, power, and endurance52. Seefeldt emphasized the importance of these basic motor skills in performing activities that promote structural and cardiovascular fitness in later years. Therefore, physical fitness tests for this age group should be closely related to and overlap with developmental assessment tests for gross motor skills. Based on a pilot study, the selected tests for this study met the following criteria:
-
1.
Appropriate for children aged 3–6 years.
-
2.
Activities that are simple to learn and safe to perform.
-
3.
Easily administered by a kindergarten teacher.
-
4.
Clearly defined and simple to score.
-
5.
Limited to the use of materials already available in Hong Kong kindergartens.
-
6.
Similar to motor performance tests for kindergarten children aged 3–6 years used in other parts of the world.
-
7.
Covering all aspects of motor performance, including static balance and muscle strength (both upper and lower limbs).
The preschoolers were given standard demonstrations and verbal cues to help them perform better during the actual tests. All tests were carried out in kindergartens and were supervised by a research team, with teachers also present, during playtime with each group of preschoolers. The participants completed all the tests in small groups, typically consisting of around 5 children for each task. Before the tests began, all participants completed a 5-min general and standardized warm-up. Investigators had previously been trained in administering all tests and following standard operating procedures, which included a proficient demonstration of each test technique, a verbal explanation, and motivational feedback.
One-leg balance
The participants began the test by standing on their dominant foot and placing their arms by their sides, not moving their feet or grabbing a support unless they needed to regain their balance. There were no restrictions on upper-limb movement as per the original protocol. When the participants moved from their stationary position or put the other leg down, the test was stopped. Recorded the best time covered for three trials in seconds for the foot used. The test was timed using a stopwatch. The timing with the stopwatch began when the heel was lifted off the floor. Each child was given 2 practice trials and 3 tests. After 3 tests, the best result was selected.
Standing long jump
This test entailed jumping forward as far as possible with feet separated at shoulder width and landing upright. A mattress with footprints was placed on the floor to direct participants to the jumping line. The participants were instructed to stand just behind the starting line. The distances between the starting line and the back heel of the participants were measured. Jumping with running was not counted. The participants took the test three times, resting in between each attempt. The best of three attempts was recorded in cm.
Overarm beanbag throwing
The participants were instructed to throw a standard beanbag (Leisure and Cultural Department reference code: LC/TQ/55/14(P)) with 140 g using their preferred hand as far they could with an overarm posture. A 1000 cm/30 feet long place was required for the testing and every 150 cm/5 feet marked on the ground to facilitate the recording. The throwing distances (not including the sliding distance) of three attempts were measured. The recorded measurement for the farthest distance achieved in throwing the beanbag was in cm (greater or equal to 15 cm/6 in. counted as for one additional 12 in.).
Anthropometric measurements
Participants' body weight and height were assessed using standard anthropometric techniques. Weight was measured with a portable digital scale (SECA 876, Hamburg, Germany) to the nearest 0.1 kg, while the participants were lightly dressed, wearing only a sport shirt. Height was measured to the nearest 0.1 cm while the children were standing upright in bare feet, using a portable stadiometer (SECA 217, Hamburg, Germany). The measurements were performed twice, and the average of the two measurements was recorded.
Statistics
All statistical analyses were performed using R Statistical Software version 3.6.3 (http://cran.us.r-project.org/). The statistical tests were all conducted with a significance level of 0.05. Potential outliers were examined and removed if the fitness scores were ≥ 4 interquartile ranges from the group median by age and sex for each test.
Body mass index (BMI) was calculated as the weight in kilograms (kg) divided by the square of height in meters (m2). Students were categorized into underweight, healthy weight, and excessive weight (overweight/obese) groups based on their BMI according to the International Obesity Task Force (IOTF) age- and sex-specific standards53. The underweight group was defined using the international cut-off point, which aligns with the World Health Organization (WHO) standard of thinness, passing through a BMI of 17 at age 18. The excess weight (overweight/obese) group was categorized using the cut-off point passing through a BMI of 25 at age 18, while the remaining individuals were considered to be in the healthy weight group.
Descriptive statistics were employed to analyse the characteristics of the participants, which included age, sex, weight, height, BMI status, and motor test scores. To compare the mean differences of continuous variables such as age, weight, height, BMI, and motor test scores between boys and girls, an independent t-test was used. Pearson’s Chi-square test was used to examine the distribution of BMI status between the two sexes. One-way ANOVA was then used to compare the difference of the MP z-scores among different BMI status. Tukey HSD was followed to test for pairwise comparisons. MP z-scores were extracted from the generalized additive model for location, scale and shape GAMLSS models.
GAMLSS54, an extension of the LMS method developed by Cole and Green, was used to compute the normative values of the motor tests. The GAMLSS model consists of three components which are represented by four parameters: (1) location (µ), median; (2) scale (variability σ); (3) shape (skewness ν and kurtosis τ). Distributions available include normal distribution (NO) with only location and scale; Box-Cox-Cole-Green (BCCG) distribution with location, scale and skewness, where ν is equivalent to Box-Cox power λ; Box-Cox-power-exponential (BCPE) distribution which is an extension of BCCG distribution including kurtosis18.
The finesses of the models constructed using the four distributions mentioned above were compared using the Generalized Akaike Information Criterion (GAIC). The models were selected automatically using the LMS function of the GAMLSS package, which is implemented in R version 3.6.3. More information about the GAMLSS package can be found at http://gamlss.org/. The smallest GAIC with a penalty tree (GAIC(3)), which favours smoother curves, was chosen to provide an optimal fit for model55. Q-Q plot of the normalized quantile residuals56, Q statistics57 and worm plots58 were used to test the goodness of fit. Sex-specific sensitivity analysis was carried out by comparing the 5th, 10th, 20th, 30th, 40th, 50th, 60th, 70th, 80th, 90th and 95th percentile curves for the motor tests18.
Informed consent
Informed consent was obtained from all subjects involved in the study.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- BMI:
-
Body mass index
- BT:
-
Beanbag throwing
- IOTF:
-
International Obesity Task Force
- WHO:
-
World Health Organization
- MP:
-
Motor performance
- OB:
-
One-leg balance
- SLJ:
-
Standing long jump
References
True, L. et al. Motor competence and characteristics within the preschool environment. J. Sci. Med. Sport 20, 751–755 (2017).
Milne, N., Leong, G. M. & Hing, W. The relationship between children’s motor proficiency and health-related fitness. J. Paediatr. Child Health 52, 825–831 (2016).
Stodden, D. F., True, L. K., Langendorfer, S. J. & Gao, Z. Associations among selected motor skills and health-related fitness: Indirect evidence for Seefeldt’s proficiency barrier in young adults?. Res. Q. Exerc. Sport 84, 397–403 (2013).
Brian, A., Getchell, N., True, L., De, M. A. & Stodden, D. F. Reconceptualizing and operationalizing Seefeldt’s proficiency barrier: Applications and future directions. Sports Med. 50, 1889–1900 (2020).
Ortega, F. B., Ruiz, J. R., Castillo, M. J. & Sjastram, M. Physical fitness in childhood and adolescence: A powerful marker of health. Int. J. Obes. (Lond.) 32, 1–11 (2008).
Smith, J. J. et al. The health benefits of muscular fitness for children and adolescents: A systematic review and meta-analysis. Sports Med. 44, 1209–1223 (2014).
Cadenas-Sanchez, C. et al. Physical fitness reference standards for preschool children: The PREFIT project. J. Sci. Med. Sport 22, 430–437 (2019).
Kit, B. K., Akinbami, L. J., Isfahani, N. S. & Ulrich, D. A. Gross motor development in children aged 3–5 years, United States 2012. Matern. Child Health J. 21, 1573–1580 (2017).
Lam, M. Y., Ip, M. H., Lui, P. K. & Koong, M. K. How teachers can assess kindergarten children’s motor performance In Hong Kong. Early Child Dev. Care 173, 109–118 (2003).
Silva-Santos, S., Santos, A., Vale, S. & Mota, J. Motor fitness and preschooler children obesity status. J. Sports Sci. 35, 1704–1708 (2017).
Gallahue, D. L., Ozmun, J. C. & Goodway, J. Understanding Motor Development: Infants, Children, Adolescents, Adults (Mcgraw-hill, 2006).
Malina, R. M. Physical activity and fitness: Pathways from childhood to adulthood. Am. J. Hum. Biol. 13, 162–172 (2001).
Stodden, D., Langendorfer, S. & Roberton, M. A. The association between motor skill competence and physical fitness in young adults. Res. Q. Exerc. Sport. 80, 223–229 (2009).
De Miguel-Etayo, P. et al. Physical fitness reference standards in European children: The IDEFICS study. Int. J. Obes. (Lond.) 38(Suppl 2), S57-66. https://doi.org/10.1038/ijo.2014.136.,S57-S66 (2014).
Vaccari, F. et al. Physical fitness reference standards in Italian children. Eur. J. Pediatr. 180, 1789–1798 (2021).
Ramos-Sepulveda, J. A., Ramirez-Velez, R., Correa-Bautista, J. E., Izquierdo, M. & Garcia-Hermoso, A. Physical fitness and anthropometric normative values among Colombian-Indian schoolchildren. BMC Public Health 16, 962–3652 (2016).
Tomkinson, G. R. et al. European normative values for physical fitness in children and adolescents aged 9–17 years: Results from 2 779 165 Eurofit performances representing 30 countries. Br. J. Sports Med. 52, 1445–14563 (2018).
Yip, K. M. et al. Age- and sex-specific physical fitness reference and association with body mass index in Hong Kong Chinese Schoolchildren. Int. J. Environ. Res. Public Health 19, 15346 (2022).
Diao, T. C., Dong, C. X. & Li, J. The Shanghai Norm of the test of gross motor development-3 in China. China Sport Sci. Technol. 54, 98–104 (2018).
Hoeboer, J. J. A. A. et al. The Athletic Skills Track: Age- and gender-related normative values of a motor skills test for 4- to 12-year-old children. J. Sci. Med. Sport 21, 975–979 (2018).
Rodrigues, L. P. et al. Normative values of the motor competence assessment (MCA) from 3 to 23 years of age. J. Sci. Med. Sport 22, 1038–1043 (2019).
Roth, K. et al. Is there a secular decline in motor skills in preschool children?. Scand. J. Med. Sci. Sports 20, 670–678 (2010).
Rao, N. et al. Early motor development in China: Secular trends among 4-year-olds. Early Child Dev. Care 193, 1–14 (2022).
King-Dowling, S., Rodriguez, C., Missiuna, C., Timmons, B. W. & Cairney, J. Health-related fitness in preschool children with and without motor delays. Med. Sci. Sports Exerc. 50, 1442–1448 (2018).
Farpour-Lambert, N. J. et al. Childhood obesity is a chronic disease demanding specific health care—a position statement from the childhood obesity task force (COTF) of the European Association for the Study of Obesity (EASO). Obes. Facts 8, 342–349 (2015).
WHO. Obesity and overweight. https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight. Accessed 14 8 Aug 2023 (WHO, 2021).
Barros, W. M. A. et al. Effects of overweight/obesity on motor performance in children: A systematic review. Front. Endocrinol. (Lausanne) 20, 759165 (2022).
Ho, F. K. et al. The reciprocal relationship between body mass index categories and physical fitness: A 4-year prospective cohort study of 20000 Chinese children. Pediatr. Obes. 15, e12646 (2020).
Hondt, D., Deforche, B., De, B. I. & Lenoir, M. Relationship between motor skill and body mass index in 5- to 10-year-old children. Adapt. Phys. Activ. Q. 26, 21–37 (2009).
Chow, B. C. & Can, L. Gross motor skills of Hong Kong Preschool children. Ajper 17, 71–77 (2011).
Wood, A. P., McMillan, A. G., Imai, S., Swift, D. & DuBose, K. D. Associations of percent body fat and motor skill development in preschool-aged children: National Youth fitness survey. Child. Obes. 18, 50–55 (2022).
Wearing, S. C., Hennig, E. M., Byrne, N. M., Steele, J. R. & Hills, A. P. The impact of childhood obesity on musculoskeletal form. Obes. Rev. 7, 209–218 (2006).
Zhang, X., Gu, X., Zhang, T., Caola, P. & Wang, J. Are movement behaviors and fundamental motor skills associated with fitness and fatness in early childhood? Findings from the 2012 NHANES National Youth Fitness Survey. Pediatr. Exerc. Sci. 32, 9–15 (2020).
Kakebeeke, T. H. et al. Association between body composition and motor performance in preschool children. Obes. Facts 10, 420–431 (2017).
Castetbon, K. & Andreyeva, T. Obesity and motor skills among 4 to 6-year-old children in the United States: Nationally-representative surveys. BMC Pediatr. 12, 25 (2012).
Katanic, B., Aleksic-Veljkovic, A., Prvulovic, N., Banjevic, B. & Tomic, I. Relationship between Fine motor skills and BMI of preschool children. J. Anthropol. Sport Phys. Educ. 6, 23–26 (2022).
Morano, M., Colella, D. & Caroli, M. Gross motor skill performance in a sample of overweight and non-overweight preschool children. Int. J. Pediatr. Obes. 6(Suppl 2), 42–46. https://doi.org/10.3109/17477166.2011.613665,42-46 (2011).
Haga, M. Physical fitness in children with high motor competence is different from that in children with low motor competence. Phys. Ther. 89, 1089–1097 (2009).
Moliner-Urdiales, D. et al. Associations of muscular and cardiorespiratory fitness with total and central body fat in adolescents: The HELENA study. Br. J. Sports Med. 45, 101–108 (2011).
Krombholz, H. The motor and cognitive development of overweight preschool children. Early Years 32, 61–70 (2012).
Logan, S. W., Scrabis-Fletcher, K., Modlesky, C. & Getchell, N. The relationship between motor skill proficiency and body mass index in preschool children. Res. Q. Exerc. Sports 82, 442–448 (2011).
Nervik, D., Martin, K., Rundquist, P. & Cleland, J. The relationship between body mass index and gross motor development in children aged 3 to 5 years. Pediatr. Phys. Ther. 23, 144–148 (2011).
Latorre Roman, P. A. et al. Physical fitness in preschool children: Association with sex, age and weight status. Child Care Health Dev. 43, 267–273 (2017).
Rodriguez-Ayllon, M. et al. Role of physical activity and sedentary behavior in the mental health of preschoolers, children and adolescents: A systematic review and meta-analysis. Sports Med. 49, 1383–1410 (2019).
Franjoine, M. R., Darr, N., Held, S. L., Kott, K. & Young, B. L. The performance of children developing typically on the pediatric balance scale. Pediatr. Phys. Ther. 22, 350–359 (2010).
Latorre Roman, P. A., Mora, L. D., Robles, F. A. & Garcia, P. F. Reference values of static balance in Spanish preschool children. Percept. Mot. Skills 124, 740–753 (2017).
Webster, E. K., Sur, I., Stevens, A. & Robinson, L. E. Associations between body composition and fundamental motor skill competency in children. BMC Pediatr. 21, 444–02912 (2021).
Riso, E. M., Kull, M., Mooses, K., Hannus, A. & Jurimae, J. Objectively measured physical activity levels and sedentary time in 7–9-year-old Estonian schoolchildren: Independent associations with body composition parameters. BMC Public Health 16, 346. https://doi.org/10.1186/s12889-016-3000-6 (2016).
Deforche, B., De, B. I., Dhondt, E. & Cardon, G. Objectively measured physical activity, physical activity related personality and body mass index in 6- to 10-yr-old children: A cross-sectional study. Int. J. Behav. Nutr. Phys. Act. 6, 25. https://doi.org/10.1186/1479-5868-6-25 (2009).
Parsons, T. J., Power, C., Logan, S. & Summerbell, C. D. Childhood predictors of adult obesity: A systematic review. Int. J. Obes. Relat. Metab. Disord. 23(Suppl 8), S1-107 (1999).
Ortega, F. B. et al. Systematic review and proposal of a field-based physical fitness-test battery in preschool children: The PREFIT battery. Sports Med. 45, 533–555 (2015).
Mrozkowiak, M. & Kaiser, A. Physical fitness in preschool children. J. Educ. Health Sport 11, 132–142 (2021).
Cole, T. J., Flegal, K. M., Nicholls, D. & Jackson, A. A. Body mass index cut offs to define thinness in children and adolescents: International survey. BMJ 335, 194 (2007).
Cole, T. J. et al. Age- and size-related reference ranges: A case study of spirometry through childhood and adulthood. Stat. Med. 28, 880–898 (2009).
Rigby, R. A. & Stasinopoulos, D. M. Smooth centile curves for skew and kurtotic data modelled using the Box-Cox power exponential distribution. Stat. Med. 23, 3053–3076 (2004).
Stasinopoulos, D. M. & Rigby, R. A. Generalized additive models for location scale and shape (GAMLSS) in R. J. Stat. Softw. 23(7), 1–46 (2007).
Royston, P. & Wright, E. M. Goodness-of-fit statistics for age-specific reference intervals. Stat. Med. 19, 2943–2962 (2000).
Van, B. S. & Fredriks, M. Worm plot: A simple diagnostic device for modelling growth reference curves. Stat. Med. 20, 1259–1277 (2001).
Acknowledgements
The authors would like to thank the Department of Health, the participating kindergartens and the support of all participants in this study.
Funding
This study was funded by the Health and Medical Research Fund (No. GC-CUHK) and the Collaborative Research Fund, University Grants Committee (No. C7149-20 GF).
Author information
Authors and Affiliations
Contributions
P.I. was involved in conceptualization, methodology, supervision, and writing—original draft (lead); K.Y. was involved in methodology, formal analysis, and writing— original draft; K.T.S.T., R.S.W., W.W.Y.T., I.C.K.W., J.C.Y., M.Y.W.K., L.H.T.L., A.L., L.L.H. and E.A.S.N. were involved in conceptualization, methodology, and writing—review and editing; H.S. and W.H.S.W. were involved in methodology, program administration, supervision, and writing—original draft. All authors approved the final manuscript as submitted and agreed to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Yip, KM., So, HK., Tung, K.T.S. et al. Normative values of motor performance and their relationship with BMI status in Hong Kong preschoolers. Sci Rep 14, 6567 (2024). https://doi.org/10.1038/s41598-024-57121-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-57121-y
Keywords
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
