
Abstract
Use of alcohol and other substances remains a major health concern among higher learning institutions. This study aimed at assessing the prevalence of alcohol and other substance use among students at Busitema University in Eastern Uganda. A cross sectional survey was conducted among 658 undergraduate students using a questionnaire consisting of Alcohol, Smoking and Substance Involvement Screening Tool and participant sociodemographic and clinical factors. Logistic regression was used to explore the associations. Two hundred sixty-five (40.3%) students reported ever using alcohol and 158 (24.0%) had used in last 3 months. Seventy-four (11.2%) students reported ever use of other substances including tobacco, cannabis, cocaine, stimulants sedatives and hallucinogens and 36 (5.5%) had used within the recent 3 months. After controlling for potential confounders, recent alcohol use was associated with engaging in romantic relationship (odd ratio (OR) = 1.9, P value (P) = 0.045) while having chronic medical conditions was protective (OR = 0.3, P = 0.031). On the other hand, recent use of other substances was 7 times higher among males (OR = 7.0, P = 0.008) compared to females while fourth year of study was protective (OR = 0.05, P = 0.011). Although alcohol use is a worsening challenge among university students, use of other substances is also highly prevalent after COVID-19 lockdown. There is need for universities to identify students with above factors and design interventions to address them in order to prevent the likely undesirable outcomes of alcohol and substance use.
Similar content being viewed by others

Introduction
Globally, the burden of annual alcohol consumption per person aged 15 years and above is 6.5 L of pure alcohol. Additionally, 3.5–5.7% of the world’s population reported consuming at least one other psychoactive substances including cannabis, opioids, injection drugs, stimulants among other respectively1. In 2020, alcohol accounted for 1.78 million deaths globally and about 59% of people aged 15–39 years were engaging in harmful drinking2. In low and middle income countries the prevalence of these substances varies widely ranging from 5.8% for alcohol in Sub-Saharan Africa3, 5.2–13.5% for cannabis and 3.7% for injection drugs in West and Central Africa1.
In 2018, the per capita alcohol consumption in Uganda was 15.1 among persons aged 15 years and above3. A nation-wide survey indicated that alcohol is the commonest substance with current use among adult persons was 26.8% with 9.8% having an alcohol-use-related disorder and majority (76.9%) being aged between 18 and 49 years4. Other substances that also reported to be commonly used by young people at educational institutions in Uganda include tobacco, stimulants and opioids inhalants among others5. In Uganda, most students join University at the age of 18 years and above which is the age at highest risk of substance use6. Existing studies indicate that prevalence of substance use among university students varies widely ranging from 31% for alcohol7, cannabis at 8% and tobacco at 7%8.
Whereas substances other than alcohol are considered to be harmful and hence illegal in most countries, World Health Organisation also advises that no amount of alcohol is good for one’s health hence should be avoided9. However, there are various factors that influence substance use and they vary geographically due to the diverse sociocultural factors and also as per substance2,10,11. For instance in Egypt substance use was found to be significantly associated with being male and attending practical college12. In Yemen and Saudi Arabia, there was statistically significant difference in prevalence of use of substances like prescription drugs such as stimulants and sedatives and was found to be higher among males compared to females13.
Some studies have documented that alcohol and other substance use has been associated with having mental illness like depression and anxiety disorders14, excessive academic stress7 and type of residence at university8. Use of substances such as cannabis have been associated with academic difficulties among students characterized by skipping classes and poor academic performances15. In Kerala India, tobacco use among college students was mainly associated with male gender and comorbid use of alcohol16. Similarly hallucinogen use among university students has been associated with comorbid use of other substances like alcohol as well as have mental health problems, risky sexual behaviors, low self-esteem and impulsivity personality traits17. Among college students in the United States, engaging in romantic relationship was highly associated with binge alcohol drinking, marijuana and nicotine use but not prescription drugs18.
At a time when most countries including Uganda are recovering from COVID-19 pandemic and its related lockdown, substance use is likely to be on the rise as some people resorted to it as a coping mechanism. Hence, University students who underwent restrictions such as suspension of academic activities, transition to online versus physical studying and other psychosocial change were at higher risk of using substances to deal with depressive and anxiety symptoms19. These post-COVID effects come as additions to the already existing academic, social and financial challenges at University.
Unfortunately, literature regarding the status of alcohol and related substance use among university students after COVID-19 pandemic remains scanty. Whereas some studies have been conducted during and post-COVID-19 lockdown to assess substance use among students of higher institutions of learning and the finding vary geographically20,21,22,23. Hence this calls for context specific research to inform local policies and interventions. Therefore, this study aimed at determining the prevalence of alcohol and other related substance use among undergraduate students at Busitema University in rural Eastern Uganda. By understanding the burden and determinants of substance use, we can be able to design context specific intervention geared towards reduction of the burden of use and resultant complication for a more productive university population.
Methods and materials
Study design and site
This was a cross sectional survey conducted at Busitema University (BU) in Eastern Uganda. BU is a multi-campus public university having six campuses spread across 6 districts in this region with each offering different courses. This study was conducted at the main (Busitema) campus which is in Tororo district and Mbale campus which is in Mbale district. Busitema campus offers mainly engineering courses like civil and electrical engineering at certificate, diploma and bachelor’s degree levels while Mbale campus offers medical courses such as medicine and surgery, nursing, and anesthesia at bachelor’s degree level. The study was conducted at these two sites due to proximity and comparability since they all offer science related courses. Additionally, Busitema is the main campus for the University while most cases of mental illness had been reported at Mbale campus prior to conducting this study24,25. At the time of conducting the study, Busitema campus had approximately 700 students while Mbale campus had about 490 students.
Study population, sampling and recruitment
Eligible participants included any undergraduate students aged above 18 years attending any of the above two campuses who were available at the time of data collection. Students having any severe mental or physical illness that could make them unable to respond meaningfully to research questions were excluded. Participants were recruited at their respective campuses during their free time or at times when they had breaks from academic activities to minimize interference with academic work. These were approached by trained research assistants who would explain the purpose, benefits and risks of the study and hence obtain written informed consent prior to participation. Each participant was required to present a valid university identity card and would further be verified by checking on the respective student list obtained from university administration for each campus.
A total of 658 students (298 and 360 students at Mbale and Busitema campuses respectively) were recruited and this was estimated using Cochran (1977) formula26,27 considering two clusters (two campuses), Inter-Cluster Correlation of 0.5 between two campuses, design effect of 1.5, alpha of 0.05 and z value of 1.96 at 95% confidence level and 10% non-response rate. The prevalence of substance use disorders was considered to be 50% in order to achieve the maximum sample size. Sample sizes at each campus were based on the proportion of the respective total population of students. Stratified sampling was used based on the eligibility criteria in relation to both sites. At each site, proportions of students to be recruited were determined by the relative total number of students in each year of study. For each year of study, participants were recruited consecutively until the required sample sizes were achieved at both sites.
Data collection and management
Data was collected by well-trained research assistants using an electronic questionnaire installed on tablets designed using Google form software. The questionnaire consisted of mainly three sections: (1) sociodemographic characteristics, (2) social and clinical factors influencing substance use, and (3) Alcohol, Smoking and Substance Involvement Tool (ASSIST). ASSIST is used for screening alcohol and other psychoactive substances including tobacco products, cannabis, cocaine, amphetamine-type stimulants, sedatives and sleeping pills, hallucinogens, inhalants, opioids, injection drugs and others. It was developed by World Health Organisation for primary health care and community settings. It has eight items with question 1 and 8 assessing “ever use” while questions 2–7 assess substance use in the last 3 months. Each item is scored on a likert scale with responses such as “never” = 0, “once or twice” = 2, “monthly” = 3, “weekly” = 4, “daily/almost daily” = 6 (for question 2). However, these assigned numerical scores differ from question to question and the total risk score is calculated by adding score of questions 2 to 7 with the minimum being 0 and maximum is 39. The total score can be categorized into the ASSIST risk score whereby for alcohol, lower risk ranges from 0–10, moderate risk is from 11–26, and high risk = 27 and above while for other substances, lower risk ranges from 0–3, moderate risk is from 4–26 and high risk is 27 and above28. This tool has been validated and used in different settings including Uganda and has high reliability with sensitivity ranging from 65 to 75% and specificity of 69–80% respectively depending on the substance and ASSIST risk score29,30,31.
For this study, the main outcome variables were alcohol use and other substance use as assessed by ASSIST. The independent variables included sociodemographic and clinical factors influencing substance used as derived from existing literature like age, sex, socioeconomic status, academic-related stressors, personal and familial history of mental or physical illnesses, among others12,30 (see Appendix 1).
Each participant was assigned a unique identification number for this study and completed forms were submitted to an online server which was password protected and only accessible by or with authorization for principal investigator. The completed forms were downloaded in an excel format, checked for completeness, cleaned, and coded before analysis.
Data analysis
The final excel sheet was imported into STATA version 16 software for analysis. Summary statistics were calculated, whereby for dichotomous or categorical variables frequencies and percentages were reported while for continuous variables, means and corresponding standard deviations were reported. Prevalences of alcohol and other substance use were calculated as proportions of participants scoring above set cutoff points on ASSIST. Any student who responded “Yes” (score 3) for any specific substance as per question 1 was considered as having ever used that substance. Also, any student who scored 2 and above on question 2 was considered as having used that specific substance in the last 3 months. Factors associated with alcohol use and use of other substances were determined using bivariable and multivariate logistic regression. The measure of association was odds ratio considering 95% confidence interval and statistical significance of less than 5%. Variables with a P value of 0.2 at bivariable analysis were included in the multivariate logistic regression model.
Quality control
The study protocol was developed based on existing high quality scientific literature and was followed strictly and carefully throughout the study. The most senior team member was the quality control coordinator throughout the study. Research assistants completed a course in Good Clinical Practice and protection of human participants and were trained in the administration of data collection tools such as ASSIST. All study tools administered in English for uniformity by all research assistants. During data collection, the principal investigator would routinely sit in interview sessions by the different research assistants to assess their performance and provide feedback and guidance whenever necessary. Data collection software was designed with checks that minimized errors or missing data. Data collection tools were pilot tested among university students for standardization. Data analysis software will also be programmed to flag missing data, out of range or illogical values during analysis.
Ethical considerations
Ethical approval was sought from Busitema University Faculty of Health Sciences Research Ethics Committee (Number: BUFHS-2022-11) and Uganda National Council of Science and Technology (Number: HS2700ES). Permission to collect data at the respective study sites was sought from the University administration and each student provided written informed consent prior to participation in the study. All data collection, management and analysis procedures were conducted according to guidelines and regulations by the Uganda National Council of Science and Technology.
Results
Participant characteristics and prevalence of substance use
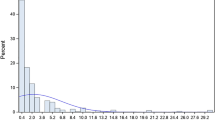
Majority of the participants were males (63.7%), born again Christians (44.5%) and single (83.4%). Over 67% of the students were privately sponsored, 54.3% were coming from semi-urban homes, and 62.2% were taking with maximum duration of 4 years. Tables 1 and 2 show the distribution of the various characteristics of the study participants that had either alcohol or other substance use within the last 3 months to the study. There proportion of students engaging in romantic relationships (P = 0.027) and having dependents (P = 0.038) who used alcohol in the last 3 months was significantly higher than those that did not. Also, there was a probable association between year of study (P = 0.019) and use of other substances in the last 3 months. Out of the 658 participants, 265 (40.3%) and 74 (11.2%) reported history of ever use of alcohol and other substances respectively (see Fig. 1).

Graph showing prevalence of common substances used by students.
Also, alcohol was the most prevalent substance used within the last 3 months at 24% while use of other substances was at 5.5% with tobacco being the most used at 3% (see Fig. 1). Notably, no student reported ever use of opioids or any other injection drugs at both campuses.
Considering participants who had ever used alcohol or any other substance, moderate to high-risk use was greater among participants using other substances (21.4%) compared to alcohol (12.9%). (see Table 3).
Bivariate and multivariate analysis using logistic regression showed that students with chronic medical conditions were less likely to use alcohol within last 3 months (odd ratio (OR) = 0.3, P value = 0.031). Conversely, students involved in a romantic relationship were almost twice more likely (OR = 1.9, P value = 0.045) to use alcohol within the last 3 months compared to those not involved in such relationship. (see Table 4).
Regarding use of other substances within the last 3 months, the odds were 7 times higher among males (OR = 7.0, P = 0.008) compared to females while for being in fourth year of study was protective (OR = 0.05, P value = 0.011) against use compared to other years (see Table 5).
Discussion
This study aimed at determining the prevalence and associated factors of alcohol and other substance use among undergraduate students at Busitema University. The findings indicated that prevalence of ever use and use within last 3 months of alcohol use was 40.3% and 24.0% while for other substances was 11.2% and 5.5% respectively. Risky use of alcohol and other substances was higher among male than female students. Current alcohol use among students was associated with being involved in a romantic relationship while having chronic medical conditions was protective while use of other substances was associated with being male while fourth year of study was protective.
These findings are in line with studies that have documented similar prevalence of alcohol use among university students. For example at Makerere University prevalence of alcohol use was 39% among social media users though this was in a 12-month period and use in last 3 months was never assessed32. However, our findings differed from what was reported among undergraduate students at Gulu University of 35%33 and 52.9% at Mbarara University34. This difference may be explained by differences in study tools used for example the former used Alcohol Use Disorder Identification Test which assesses alcohol use disorder33 while the latter34 used no standard tool for assessing alcohol use and none of these assessed ever use or use within last 3 months. Additionally, the differences in prevalences could be due to geographical variations whereby the above two institutions are in northern and southwestern regions respectively hence having students who predominantly come from those regions. This study was conducted at Busitema and Mbale campuses of Buistema University which mainly serves eastern Uganda. The geographical distribution of these Universities is associated with social cultural differences which greatly influence substance use behaviors among people in the specific regions.
However, a study conducted among undergraduate students in Kenya using ASSIST indicated that 21.9% of students ever used alcohol while only 16.9% had used within the recent 3 months8 which are markedly lower than our findings. Hence this indicates that the problem is higher in Eastern Uganda which may be one of the effects of COVID-19 since the Kenya study was conducted before COVID-19 pandemic.
Additionally, the prevalence of other substance use in this study was higher than what has been documented among the same Kenyan student population whereby prevalence of ever use of any other substance was 9.4% with cannabis being the commonest rather than tobacco as per our setting8.
Conversely, studies in other settings have reported varying prevalence of use of other substances among university students such as 8.9% for tobacco and 4.3% for sedatives in Egypt35, 41% for Khat (amphetamine), 22% for Cigarettes and 7.4% for illicit drugs in Ethiopia36 and 52% for cannabis, 25% for cocaine and 9% for amphetamines in Ireland37. These variations in prevalence of use of different substances are influenced by psychosocial and cultural factors within the different contexts hence suggesting need for context-specific studies and interventions.
Generally, there was a higher prevalence of alcohol use among university students compared to other substances. This could be because alcohol is legally available to all persons aged 18 years and above as per the current regulatory policies. It is also readily available and affordable on the market in various forms with some types being locally brewed in homes which exposes students to its use early in life. Additionally, most sociocultural groups in the eastern region consider alcohol use to be a culturally acceptable practice and some homes sell it as source of livelihood hence students from such backgrounds are prone to using it38. However, some are able to break the chain by cessation of drinking as they grow hence explaining the lower prevalence of current use compared to ever use.
Unlike alcohol, most of the other substances such as cannabis, cocaine and others are illegal and not readily available for sale on market which makes accessibility more difficult which possibly explains the lower prevalence of both ever and current use39. This is in line with finding from most of the existing literature which has documented alcohol to be the most commonly used substance among students40,41. Generally, more students had low risk use of alcohol and other substances which show the need to ensure that they keep abstaining or do not worsen their substance use habits to prevent progression to high-risk use. However, for those with moderate to high risk use (especially those using other substances), more intensive interventions to counteract their current drinking, smoking and other substance use habits42.
Recent alcohol use was found to be significantly associated with being involved in a romantic relationship which may be more of a poor coping mechanism used by students due to social pressures resulting from such relationships. Recent studies have indicated that Ugandan university students engage in sexual relationships referred to as “situationships” with different individuals including their peers, teachers and other people mainly to navigate socioeconomic challenges or for monetary purposes43. Hence, alcohol use may be related to students trying to boost their confidence to face challenges resulting from such relationships like rejection, separation, or any other form of disappointments. For other students especially the youth, this may be due to peer pressure or role modelling effect from their partners who use substances compelling them to start use in order to fit in the group44. Notably, partner influence has been found to be strongly associated with alcohol use with females having more influence than males45. Whereas this influence can be protective, sometimes in this case it may be responsible for the high rates of substance use among the couples. Hence this may mean that many students are currently using alcohol because of influence by their romantic relationship partners.
Conversely, students having chronic medical conditions were less likely to use alcohol which may be because of the fear of worsening their pre-existing medical illnesses. Also, by having chronic medical illnesses these students are more likely to receive medical education and counselling discouraging them from using alcohol in order not to exacerbate their illnesses. This is consistent with findings from primary healthcare settings in California where people with medical conditions were less likely to drink alcohol46. However, it is important to consider that chronic alcohol use has also been associated with many other chronic medical conditions such as hypertension, diabetes, liver disease and others, though these are less common in our study population47.
Unlike alcohol, use of other substances was associated with being male which could be explained by the aggressive nature of males compared to females which makes them able to search and obtain these illegal substances. This is in line with what was reported in other studies where males were more likely to use substances compared to females8,12,33. Commonly, males are more likely to have antisocial, extraversion and impulsive personality traits which are more associated with risky substance use and hence several studies have found higher prevalence of illicit drug use among them compared to females48,49,50,51.
On the other hand, fourth year of study was protective against use of other substances. Since this is the final year for most courses offered at both campuses, these students are usually more likely to be more hopeful in the life after school where they are expected to act professionally hence reducing their chances of substance use. Relative to other years of study, where there may be more stressor including some from teachers, final year students tend to be kindlier by their teachers who may become colleagues after their completion hence the protective effect towards substance use.
Implications of study findings
The findings indicate that whereas alcohol remains the commonest substance used by students at the university, other substances like tobacco, cannabis, cocaine, amphetamines, sedatives and hallucinogens are also in use. Hence interventions and education and health policies should broaden their scope to curb the use of all these substances. The factors associated with alcohol and other substance use are both non-modifiable indicating that intervention strategies should mainly aim at preventive measure involving screening for the above risk factors among students while reinforcing the protective ones.
Study limitations
The study was conducted at only two out of six campuses of Busitema University hence the findings may not perfectly reflect the exact situation at other campuses or even other universities. However, the findings shed light on what is going on at the university in relation to substance use among students and hence calling for possible interventions. Since the study investigated a sensitive social issue, there might have been response bias from some participants especially regarding use of illegal substances. This was minimized by using independent well trained research assistants within the age range of most students who were not university staffs to enhance freeness during interviews.
Conclusion and recommendations
Like findings from other universities in Uganda, use of alcohol and other substance remains a significant health challenge among undergraduate students at Busitema Universities especially at a time when the country is struggling with effects of COVID-19 pandemic. The factors associated with use of these substances occur both at individual and institutional level. This calls for interventions at national and institutional levels for-example ensuring health relationships among students or regulating the marketing and acquisition of some of the currently legal products such as alcohol and tobacco by students. Institutions may also need to put in place measures to monitor any involvement in transactions leading to acquisition or use of any substances in institutions. Finally, there is need for more research regarding measures or interventions to manage and rehabilitate students who may have any substance use disorders to ensure that they successfully study and complete their respective courses.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
References
World Health Organisation. Substance Abuse. WHO | Regional Office for Africa. https://www.afro.who.int/health-topics/substance-abuse (2023).
Bryazka, D. et al. Population-level risks of alcohol consumption by amount, geography, age, sex, and year: A systematic analysis for the Global Burden of Disease Study 2020. Lancet 400, 185–235 (2022).
World Bank. World Bank Open Data. World Bank Open Data. https://data.worldbank.org (2023).
Kabwama, S. N. et al. Alcohol use among adults in Uganda: Findings from the countrywide non-communicable diseases risk factor cross-sectional survey. Glob. Health Action https://doi.org/10.3402/gha.v9.31302 (2016).
Abbo, C., Okello, E. S., Muhwezi, W., Akello, G. & Ovuga, E. Alcohol, substance use and psychosocial competence of adolescents in selected secondary schools in Uganda: A cross sectional survey. Int. Neuropsychiatr. Dis. J. 7, 25387 (2016).
Vasilenko, S. A., Evans-Polce, R. J. & Lanza, S. T. Age trends in rates of substance use disorders across ages 18–90: Differences by gender and race/ethnicity. Drug Alcohol Depend. 180, 260–264 (2017).
Kamulegeya, L. H. et al. Prevalence and associated factors of alcohol use patterns among university students in Uganda. Pan Afr. Med. J. 37, 339 (2020).
Musyoka, C. M., Mbwayo, A., Donovan, D. & Mathai, M. Alcohol and substance use among first-year students at the University of Nairobi, Kenya: Prevalence and patterns. PLoS One 15, e0238170 (2020).
World Health Organisation. No level of alcohol consumption is safe for our health. https://www.who.int/europe/news/item/04-01-2023-no-level-of-alcohol-consumption-is-safe-for-our-health
Ayiga, N. Patterns of substance use and its predictors among North-West University students Mafikeng campus. Kabale University https://www.kab.ac.ug/publication/patterns-of-substance-use-and-its-predictors-among-north-west-university-students-mafikeng-campus/ (2017).
Kahsay, Z. H., Tesema, A. G. & Bazzano, A. N. A qualitative study of drivers of psychoactive substance use among Mekelle University students, Northern Ethiopia. Subst. Abuse Treat. Prev. Policy 14, 11 (2019).
Kabbash, I., Zidan, O. & Saied, S. Substance abuse among university students in Egypt: Prevalence and correlates. East. Mediterr. Health J. 28, 31–40 (2022).
Fadhel, F. Misuse of prescription drugs and other psychotropic substances among university students: A pilot study. East Mediterr. Health J. 28, 288–295 (2022).
Blows, S. & Isaacs, S. Prevalence and factors associated with substance use among university students in South Africa: Implications for prevention. BMC Psychol. 10, 309 (2022).
Arria, A. M., Caldeira, K. M., Bugbee, B. A., Vincent, K. B. & O’Grady, K. E. The academic consequences of marijuana use during college. Psychol. Addict. Behav. 29, 564–575 (2015).
Menon, P. G. et al. Tobacco use among college students across various disciplines in Kerala, India. Tob. Use Insights 13, 1179173X20938773 (2020).
Grant, J. E., Lust, K. & Chamberlain, S. R. Hallucinogen use is associated with mental health and addictive problems and impulsivity in university students. Addict. Behav. Rep. 10, 100228 (2019).
Blumenstock, S. M. & Papp, L. M. Substance use behaviors in the daily lives of U.S. college students reporting recent use: The varying roles of romantic relationships. Soc. Sci. Med. 279, 114021 (2021).
Maria Najjuka, S., Checkwech, G., Olum, R., Ashaba, S. & Mohan Kaggwa, M. Depression, anxiety, and stress among Ugandan university students during the COVID-19 lockdown: An online survey. Afr. Health Sci. 21, 1533–1543 (2020).
Roberts, A. et al. Alcohol and other substance use during the COVID-19 pandemic: A systematic review. Drug Alcohol Depend. 229, 109150 (2021).
Ghelbash, Z., Alavi, M., West, S., Lees, D. & Cleary, M. A post-pandemic reset: Reversing the COVID-19 increase in substance use by adolescents and young adults. Issues Ment. Health Nurs. 44, 576–579 (2023).
Bountress, K. E. et al. The COVID-19 pandemic impacts psychiatric outcomes and alcohol use among college students. Eur. J. Psychotraumatol. 13, 2022279 (2022).
Pfledderer, C. D., Bai, Y., Brusseau, T. A., Burns, R. D. & King Jensen, J. L. Changes in college students’ health behaviors and substance use after a brief wellness intervention during COVID-19. Prev. Med. Rep. 26, 101743 (2022).
About | Busitema University. https://busitema.ac.ug/about (2023).
Degrees and Programmes | Busitema University. https://busitema.ac.ug/degrees-and-programmes (2023).
Masrom, M. B. Cochran Formula to Calculate Sample Size (Cochran, 1977) | https://people.utm.my/maslin/cochran-formula-to-calculate-sample-size-cochran-1977/ (2023).
Charan, J. & Biswas, T. How to calculate sample size for different study designs in medical research?. Indian J. Psychol. Med. 35, 121–126 (2013).
World Health Organization. The Alcohol, Smoking and Substance Involvement Screening Test (ASSIST). https://www.who.int/publications-detail-redirect/978924159938-2 (2010).
Kane, J. C., Murray, L. K., Bass, J. K., Johnson, R. M. & Bolton, P. Validation of a substance and alcohol use assessment instrument among orphans and vulnerable children in Zambia using Audio Computer Assisted Self-Interviewing (ACASI). Drug Alcohol Depend. 166, 85–92 (2016).
Rebecca, S. Factors Influencing Substance Abuse Amongst Health Care Professionals in Kampala, Uganda (2022).
Kaswa, R. & de Villiers, M. Prevalence of substance use amongst people living with human immunodeficiency virus who attend primary healthcare services in Mthatha, South Africa. S. Afr. Fam. Pract. 62, 1–7 (2020).
Atusingwize, E. et al. Social media use and alcohol consumption among students in Uganda: A cross sectional study. Glob. Health Action 15, 2131213 (2022).
Otike, C. Prevalence and Factors Associated with Alcohol Use Among Undergraduate Students in Gulu University (Makerere University, 2021).
Choudhry, V., Agardh, A., Stafström, M. & Östergren, P.-O. Patterns of alcohol consumption and risky sexual behavior: A cross-sectional study among Ugandan university students. BMC Public Health 14, 128 (2014).
Kabbash, I., Zidan, O. & Saied, S. Substance abuse among university students in Egypt: Prevalence and correlates. East Mediterr. Health J. 28, 31–40 (2022).
Tesfaye, G., Derese, A. & Hambisa, M. T. Substance use and associated factors among university students in Ethiopia: A cross-sectional study. J. Addict. 2014, e969837 (2014).
Millar, S. Drug use among students in higher education in Ireland. Drugnet Ireland 81, 1–4 (2022).
Ssebunnya, J. et al. Social acceptance of alcohol use in Uganda. BMC Psychiatry 20, 52 (2020).
Narcotic Drugs and Psychotropic Substances (Control) Act, 2016 (Act 3 of 2016) | Ulii. https://ulii.org/akn/ug/act/2016/3/eng%402016-02-05 (2016).
Roba, H. S., Beyene, A. S., Irenso, A. A. & Gebremichael, B. Prevalence of lifetime substances use among students in Ethiopia: A systematic review and meta-analysis. Syst. Rev. 8, 326 (2019).
Sahu, A., Bhati, N. & Sarkar, S. A systematic review and meta-analysis of substance use among medical students in India. Indian J. Psychiatry 64, 225–239 (2022).
scheme=AGLSTERMS. AglsAgent; corporateName=Department for Health and Wellbeing; address=11 Hindmarsh Square, A. ASSIST (Alcohol, Smoking and Substance Involvement Screening Test). https://www.sahealth.sa.gov.au/wps/wcm/connect/Public+Content/SA+Health+Internet/Clinical+Resources/Clinical+Programs+and+Practice+Guidelines/Substance+misuse+and+dependence/Drug+and+alcohol+training+and+development/ASSIST+Alcohol+Smoking+and+Substance+Involvement+Screening+Test
Choudhry, V., Petterson, K. O., Emmelin, M., Muchunguzi, C. & Agardh, A. ‘Relationships on campus are situationships’: A grounded theory study of sexual relationships at a Ugandan university. PLoS One 17, e0271495 (2022).
High Risk Substance Use in Youth | Adolescent and School Health | CDC. https://www.cdc.gov/healthyyouth/substance-use/index.htm (2023).
Muyingo, L. et al. Relationships on the rocks: A meta-analysis of romantic partner effects on alcohol use. Psychol. Addict. Behav. 34, 629–640 (2020).
Sterling, S. A. et al. Associations between medical conditions and alcohol consumption levels in an adult primary care population. JAMA Netw. Open 3, e204687 (2020).
World Health Organisation. Harmful use of alcohol. World Health Organization—Regional Office for the Eastern Mediterranean. http://www.emro.who.int/noncommunicable-diseases/causes/harmful-use-of-alcohol.html (2014).
Martin, C. E., Ksinan, A. J., Moeller, F. G., Dick, D., Spit for Science Working Group. Sex-specific risk profiles for substance use among college students. Brain Behav. 11, e01959 (2021).
Mbuthia, G. W. Correlates of Substance Use, Risky Sexual Behaviour and Effectiveness of Awareness Campaigns against Alcohol and Drug Abuse among University Students in Coastal Region, Kenya (JKUAT COHES, 2016).
Hamdan-Mansour, A. M., Mahmoud, K. F., Al Shibi, A. N. & Arabiat, D. H. Impulsivity and sensation-seeking personality traits as predictors of substance use among university students. J Psychosoc. Nurs. Ment. Health Serv. 56, 57–63 (2018).
Kang, W. Big Five personality traits predict illegal drug use in young people. Acta Psychol. 231, 103794 (2022).
Acknowledgements
We appreciate the administration of Busitema University and government of Uganda for providing funds that enabled us to conduct this study as well as the deans and student leaders of Busitema and Mbale campuses who supported us throughout the data collection process.
Author information
Authors and Affiliations
Contributions
JK conceived the idea, wrote proposal, oversaw data collection, analysis and interpretation of results, drafted manuscript and proof read integrated all co-authors contributions. EKK and JM conceived the idea, wrote proposal, participated in data collection, analysis and interpretation of results, proof read all versions of the manuscript including the final one. CEA, KN, AO, RK, FK and JW supported proposal writing, data collection, analysis and interpretation of results and proof read all versions of manuscript whereas JW also provided additional technical support to the team. All authors have read and approved this manuscript prior to submission.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kirabira, J., Kagoya, E.K., Mpagi, J. et al. Burden of alcohol and other substance use and correlates among undergraduate students at Busitema University in rural Eastern Uganda after COVID-19 lockdown. Sci Rep 14, 6194 (2024). https://doi.org/10.1038/s41598-024-56861-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-56861-1
Keywords
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
