
Abstract
To investigate the association of red and processed meat intake with the risk of gestational diabetes (GDM) in Iranian mothers. A total of 635 pregnant mothers were included. Dietary intake was assessed by a 90-item food frequency questionnaire during the first trimester of pregnancy. Intakes of total red meat, unprocessed red meat, and processed meat were calculated and then, Cox proportional hazard model was used to calculate the hazard ratios (HR) and 95%CIs of GDM across tertiles of red meat intake while controlling for age, occupation, pre-pregnancy body mass index, physical activities, history of cardiovascular disease, hypertension, hypothyroidism, hyperthyroidism, and pregnancy hypertension, order of pregnancy, nausea during current pregnancy, multivitamin use during current pregnancy, weight gain during current pregnancy and total energy intake. The average age of the mothers was 28.80 ± 5.09 years, the average pre-pregnancy body mass index was 25.13 ± 4.43 kg/m2, and the average weight gain during pregnancy was 13.50 ± 5.03 kg. The multivariable-adjusted HRs of GDM for the third tertiles of red and processed meat, red meat, and processed meat intake were, respectively, 1.92 (95% CI 1.06, 3.49), 1.52 (95% CI 0.85, 2.72) and 1.31 (95% CI 0.73, 2.34) when compared to the first tertiles. Our prospective cohort study suggested that there was a positive association between the consumption of red and processed meat and with risk of GDM in a small sample of Iranian mothers with low red meat intake. More large-scale cohort studies in the Iranian population are needed to present more robust evidence in this regard.
Similar content being viewed by others


Introduction
Gestational diabetes mellitus (GDM), a common complication during pregnancy, is characterized by the initial manifestation or first appearance of impaired glucose tolerance during pregnancy1. Compared to the global standardized prevalence of GDM, which is 14%2, this rate ranges from 1.3 to 18.8% in Iranian pregnant women3. GDM is linked with unfavorable outcomes such as neonatal macrosomia and hypoglycemia4. The occurrence of Type 2 diabetes is more likely among women who have previously experienced GDM, thereby emphasizing the necessity of identifying modifiable risk factors to diminish the likelihood of developing GDM5.
Evidence points to a connection between eating choices before and during pregnancy and the risk of GDM6. A high intake of red and processed meat, along with increased adherence to a Western dietary pattern, may potentially be associated with an elevated susceptibility to developing GDM7. Unhealthy cooking methods such as frying in ketchup, cooking with fried vegetables, and grilling may increase the production of dangerous substances such as advanced glycation end products, polycyclic aromatic hydrocarbons (PAHs), and heterocyclic amines (HCAs)8. These products can interfere with insulin sensitivity and, thus, may be linked to a higher risk of type 2 diabetes9.
However, studies investigating the association of red meat with the risk of GDM are controversial. An increased intake of red meat was found to be positively associated with the risk of GDM in a prospective observational study conducted in India10. In contrast, a cohort study in Singapore that looked at the relationship between red meat protein consumption and the risk of GDM did not report any significant association11. Although there are several investigations on the association between dietary patterns and the risk of GDM in Iran12,13,14, studies of the association between the consumption of red and processed meat and the risk of GDM in the Iranian population are lacking. In general, Iranians consume less red and processed meat than those living in Western countries. Iranian traditional diet is rich in carbohydrates and refined grains. Considering the recent controversy on the link between the consumption of red and processed meat and multiple health outcomes15,16, it is uncertain whether the consumption of red and processed meat in a population with low red meat consumption is associated with the risk of developing GDM. Hence, the present prospective cohort study aimed to assess the association of the consumption of red and processed meat during early pregnancy with the risk of GDM in a sample of Iranian women.
Materials and methods
Participants
The present study was carried out within the framework of the Persian (Prospective Epidemiological Research Studies in IRAN) Birth Cohort17. The Persian Birth Cohort is an ongoing, national, prospective cohort research in five districts in Iran to advance knowledge and supply scientific proof for the creation of evidence-based national policies on various developmental causes of health and disease17. Pregnant women in Semnan, a city in central Iran, were chosen as participants. Pregnant women in Semnan who were referred to medical facilities between 2018 and 2020 were asked to take part in this prospective cohort research. Additionally, to entice women to join in this prospective cohort research, we distributed advertising through local and social media, as well as at medical clinics located around the city. Women of Iranian descent who are in their first trimester of pregnancy, regardless of gravidity, parity, or use of fertility therapy, who have lived in Semnan for at least a year, and who want to give birth in a hospital in Semnan met the inclusion criteria. Pregnancies that ended in a cesarean section or a normal vaginal birth were both included. Twin pregnancies, disorders connected to hormones, and hormone treatment were excluded criteria.
1024 women in total consented to take part in the study. For the present study, a total of 635 pregnant women were included after excluding certain groups of individuals. Including, mothers with insufficient information on dietary intake (n = 281), those who had incomplete information about study outcomes and did not continue until the end (n = 45), mothers with outlier energy intake (n = 18), those who smoked cigarettes (n = 10), and mothers with a previous history of GDM (n = 35) were excluded from the analyses. The study's procedure was described to each participant, who also completed an informed consent form. The ethics committee of the Semnan University of Medical Sciences (Ethic code: IR.SEMUMS.REC.1401.233) approved the study protocol.
Assessment of dietary intake
A food frequency questionnaire consisting of 90 items that were created and validated for use in this prospective cohort research was used to assess the individuals' dietary intake throughout the first trimester of pregnancy17. Dietary evaluations were carried out by professional interviewers conducting in-person interviews. We asked mothers to indicate how frequently they consumed the food items included in the food frequency questionnaire throughout their first trimester of pregnancy. There were nine multiple-choice options for frequency responses, ranging from "never or less than once a month" to "6 or more times per day" depending on the type of food item. Every stated consumption frequency was converted to grams per day using standard units. To determine the total calorie and nutrient intakes, Nutritionist IV software (version 7.0; N-Squared Computing, Salem, OR), customized for Iranian meals, was used.
Outcome assessment
We followed the American Diabetes Association criteria for diagnosis of GDM18. Accordingly, mothers who had at least two of the following criteria were considered as having GDM: fasting plasma glucose higher than 95 mg/dL, 1-h plasma glucose higher than 180 mg/dL, 2-h plasma glucose higher than 155 mg/dL, and 3-h plasma glucose greater than 140 mg/dL.
Assessment of other variables
Using organized, pre-tested questionnaires created for use in Persian Birth Cohorts, trained interviewers gathered information about the research participants' characteristics17. Interviewers with training took down details about the subjects' ages, medical histories, educational levels, occupations of their mothers and fathers, and family income. We employed the internationally accepted and verified International Physical Activity Questionnaire (IPAQ) to assess the levels of physical activity19. The participants were categorized into two groups based on their Metabolic Equivalent minutes per week (MET-min/week) values, i.e., no or low physical activity (< 3000 MET-minute/week) and moderate and high physical activity (> 3000 MET-minute/week)20. An experienced interviewer took measurements of weight and height. Weight was assessed at the study's baseline using a digital scale, with light clothing and no shoes, to the closest 0.5 kg. In the second and third trimesters, weight measurements were repeated. Before birth, the mothers' final weights were assessed in the hospital using the same methodology. The difference between the first and last weights was used to compute weight gain. The participants were asked to stand without shoes with their shoulders touching the wall while having their height measured with a tab that was measured to the closest 0.5 cm. Based on the division of the weight in kilograms by the square of the height in meters, the body mass index (BMI) was derived.
Plant or plant material
Our prospective cohort study was observational and we did not use any plant or plant material in this research.
Statistical analyses
We first classified red and processed meat consumption into tertiles and then grouped study participants by tertiles of red and processed meat intake. Second, an analysis was conducted to compare participants' characteristics across tertiles of red and processed meat intake. We compared values of continuous and categorical variables between categories of red and processed meat intake using ANOVA and chi-squared tests, respectively. We calculated the hazard ratio (HR) and 95% confidence interval (CI) of GDM across categories of red and processed meat intake using the Cox proportional hazard model. Age, having a job with income, pre-pregnancy BMI, history of cardiovascular disease (yes/no), weight gain during current pregnancy (kg), history of hypertension, hypothyroidism, and pregnancy hypertension (yes/no), nausea during current pregnancy (yes/no), use of multivitamins during current pregnancy (yes/no), order of pregnancy, physical activities (no or low/moderate to high), and total energy intake were all taken into consideration for multivariable-adjusted analyses. SPSS (SPSS Inc., version 22) was used for all statistical analyses. P-values less than 0.05 were regarded as significant.
Ethics approval and consent to participate
This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving research study participants were approved by the ethics committee of Semnan University of Medical Sciences. Written informed consent was obtained from all subjects/patients.
Results
The characteristics of the study participants (n = 635) for each category of red and processed meat intake are displayed in Table 1. The average age of the mothers was 28.80 ± 5.09 years. The average pre-pregnancy BMI was 25.13 ± 4.43 kg/m2, and the average weight gain during pregnancy was 13.50 ± 5.03 kg.
Mothers who ate more red and processed meat were more likely to be university graduates and less likely to have nausea during current pregnancy. Moreover, mothers with the highest tertile of red and processed meat intake used more multivitamins during their current pregnancy. Other characteristics of the mothers did not differ significantly across tertiles of red and processed meat intake.
Intake of micro- and macronutrients and food groups across tertiles of red and processed meat intake are described in Table 2. In our study population, a higher intake of red and processed meat was accompanied by higher intakes of energy, carbohydrate, total fat, total protein, saturated fat, monounsaturated fatty acids, dietary fiber, magnesium, and calcium. In addition, Table 2 presents food group intakes based on tertiles of red and processed meat intake, where a higher intake of red and processed was related to a higher intake of fruit, beans and nuts, sweets, poultry, and egg.
Table 3 indicates the HR and 95% CI of GDM (n = 80 cases) across tertiles of red and processed meat intake. In the multi-variable adjusted model, participants in the third tertile of red and processed meat intake had a higher risk of GDM compared to those in the first tertile (HR 1.92, 95% CI 1.06, 3.49). There was no association between red or processed meat intake and risk of GDM.
Discussion
In this study, we looked into the relationship between a sample of Iranian women's risk of GDM and their consumption of red and processed meat during the early stages of pregnancy. Our prospective birth cohort study demonstrated that there was a positive link between the risk of GDM and the consumption of red and processed meat.
Evidence on the association of red and processed meat with the risk of GDM is conflicting. In accordance with our study, a prospective evaluation in the Nurses' Health Study II, which included 21,457 mothers with singleton pregnancies, found that mothers in the highest quintile of total red meat consumption had twice the risk of GDM than mothers in the lowest quintile21. Higher consumption of animal-based proteins, especially those from red meat, in the second trimester of pregnancy was highly related to the risk of developing GDM, according to a prospective cohort study of 452 pregnant women in Malaysia22. Furthermore, more red meat consumption during the second trimester of pregnancy was linked to an increased risk of GDM, according to a Chinese cohort study; however, there was no link between red meat consumption during the first trimester and that risk23.
In contrast to our results, there was no correlation between the consumption of red and processed meat and other animal-based dietary protein sources and the probability of GDM, according to a small hospital-based case–control research in Iran24. Another cohort study of 980 mothers with singleton pregnancies in Singapore suggested no connection between the consumption of red meat proteins and the risk of developing GDM11. A prospective cohort study on 1178 newly diagnosed cases of type 2 diabetes in Japan concluded that there was no significant relationship between the consumption of red and processed meat and the risk of type 2 diabetes in women25. The analysis of 1733 participants in Eastern Massachusetts in a prospective cohort study found no evidence that red or processed meats are associated with the risk of developing impaired glucose tolerance or GDM26.
The modulation of skeletal muscle glucose uptake and glycogen synthesis, hepatic glucose production, and insulin secretion provide evidence for the importance of amino acids in glucose homeostasis27. An observational study found that eating a high-protein diet for 6 months increased the amount of insulin released when glucose levels reached a certain level. This was because the endocrine -cells' glucose threshold was lowered, endogenous glucose output and plasma glucagon levels were increased, and gluconeogenesis was boosted28. Additionally, studies have shown that roasting or grilling red meat at high temperatures over an open flame can result in the production of various hazardous compounds, including heteroaromatic amines and PAHs29. Research have shown correlations between urine PAH biomarkers and inflammatory indicators such as 1- and 2-hydroxynaptol and 2-hydroxyphenanthrene, as well as a higher prevalence of type 2 diabetes30,31. Additionally, mounting evidence indicates that cooking beef at high temperatures may cause the development of advanced glycation end products, which have been related in both animal and human studies to oxidative stress, inflammation, and insulin resistance32,33.
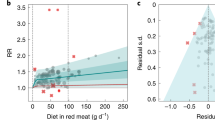
In general, the average intake of red meat in Iranian population is lower than those living in Western countries. For instance, the Nurse's Health Study found that daily intake of total red meat varied from 20 to 150 g21, compared to 0 to 90 g/d in the present study. Our findings suggest that higher intake of red and processed meat, even in a population with such a low intake, may be positively associated with the risk of GDM. The average intake of red and processed meat in our study (12.90 g/day) was comparable to the previous hospital-based case–control study in Iran in 2019 (13.17 g/day)24. The inconsistency in the findings between our study and those found in the previous study in Iran may be due to a difference in study design (prospective cohort versus hospital-based case–control) and their small sample size (n = 320)24. In a previous publication from the Persian Birth Cohort, we found that greater adherence to the Mediterranean diet during early pregnancy was associated with a lower risk of GDM in Iranian mothers34. Evidence from previous research suggests that individual components of the Mediterranean dietary pattern are not equal in relation to prevention of cardiovascular disease35 and, thus, more research is needed to examine the effect of specific food groups included in the Mediterranean diet score. Our findings in the present study suggest that higher intake of red and processed meat, even in a population with such a low red meat intake, may be associated with a higher risk of GDM. A recent evaluation within the EPIC-InterAct Study indicated that replacement of red and processed meat with other dietary protein sources including cheese, yogurt, nuts, and cereals was associated with a lower risk of type 2 diabetes36. An evaluation within the Nurse’s Health Study indicated that substitution of red meat with poultry, fish, nuts or legumes was associated with a lower risk of GDM in the US mothers with very higher red meat intake in comparison to the Iranian mothers21. Therefore, further research using innovative statistical methodologies such as substitution analysis are warranted to determine whether replacement of red and processed meat with other plant- and animal-based dietary protein sources is associated with a lower risk of GDM in Iranian pregnant women.
The interpretation of our findings has to take into account a number of limitations. Since our investigation was observational, residual confounding by unmeasured or unrecorded variables might skew the results. Second, the self-administered FFQ used to measure food intakes has the potential to misclassify research participants. Finally, because only the first trimester of pregnancy was included for our nutritional evaluation, any prospective changes in dietary intakes during pregnancy were not taken into account.
Conclusion
This prospective birth cohort study indicated that consumption of red and processed meat during first trimester of pregnancy may be positively associated with the risk of GDM in a small sample of Iranian mothers, suggesting that intake of red and processed meat is associated with the risk of GDM, as found in Western countries, in a population with such a low red meat intake. Future cohort studies with larger sample sizes and more accurate dietary evaluations during pregnancy are warranted to examine this association, and to determine whether replacement of red and processed meat with other dietary protein sources is associated with a lower risk of GDM in Iranian pregnant mothers.
Data availability
The datasets used and/or analyzed during the current study will be available from the corresponding author on reasonable request.
References
Metzger, B. E. et al. Summary and recommendations of the fifth international workshop-conference on gestational diabetes mellitus. Diabetes Care 30(Supplement_2), S251–S260 (2007).
Wang, H. et al. IDF diabetes atlas: Estimation of global and regional gestational diabetes mellitus prevalence for 2021 by International Association of Diabetes in Pregnancy Study group’s criteria. Diabetes Res. Clin. Pract. 183, 109050 (2022).
Jafari-Shobeiri, M. et al. Prevalence and risk factors of gestational diabetes in Iran: A systematic review and meta-analysis. Iran J. Public Health 44(8), 1036–1044 (2015).
Ferrara, A., Hedderson, M. M., Quesenberry, C. P. & Selby, J. V. Prevalence of gestational diabetes mellitus detected by the national diabetes data group or the carpenter and coustan plasma glucose thresholds. Diabetes Care 25(9), 1625–1630 (2002).
Noctor, E. & Dunne, F. P. Type 2 diabetes after gestational diabetes: The influence of changing diagnostic criteria. World J. Diabetes 6(2), 234 (2015).
Zhang, C. & Ning, Y. Effect of dietary and lifestyle factors on the risk of gestational diabetes: Review of epidemiologic evidence. Am J. Clin. Nutr. 94(suppl_6), 1975S-1979S (2011).
Zhang, C., Schulze, M. B., Solomon, C. G. & Hu, F. B. A prospective study of dietary patterns, meat intake and the risk of gestational diabetes mellitus. Diabetologia 49(11), 2604–2613 (2006).
Neuhouser, M. L. Red and processed meat: more with less?. Am. J. Clin. Nutr. 111(2), 252–255 (2020).
Liu, G. et al. Cooking methods for red meats and risk of type 2 diabetes: A prospective study of U.S. women. Diabetes Care 40(8), 1041–1049 (2006).
Deepa, R., Lewis, M. G., Van Schayck, O. C. P. & Babu, G. R. Food habits in pregnancy and its association with gestational diabetes mellitus: results from a prospective cohort study in public hospitals of urban India. BMC Nutr. 6(1), 63 (2020).
Pang, W. W. et al. Higher maternal dietary protein intake is associated with a higher risk of gestational diabetes mellitus in a multiethnic Asian cohort. J. Nutr. 147(4), 653–660 (2017).
Roustazadeh, A. et al. A dietary pattern rich in fruits and dairy products is inversely associated to gestational diabetes: A case-control study in Iran. BMC Endocr. Disord. 21(1), 1–9 (2021).
Zamani, B. et al. Association of a plant-based dietary pattern in relation to gestational diabetes mellitus. Nutr. Diet. 76(5), 589–596 (2019).
Zareei, S. et al. Dietary pattern in pregnancy and risk of gestational diabetes mellitus (GDM). Diabetes Metab. Syndr. 12(3), 399–404 (2018).
Johnston, B. C. et al. Unprocessed red meat and processed meat consumption: dietary guideline recommendations from the Nutritional Recommendations (NutriRECS) Consortium. Ann. Intern. Med. 171(10), 756–764 (2019).
Qian, F., Riddle, M. C., Wylie-Rosett, J. & Hu, F. B. Red and processed meats and health risks: How strong is the evidence?. Diabetes Care 43(2), 265–271 (2020).
Zare Sakhvidi, M. J. et al. The prospective epidemiological research studies in IrAN (PERSIAN) birth cohort protocol: Rationale, design and methodology. Longitud. Life Course Stud. 12(2), 241–262 (2021).
Association, A. D. Classification and diagnosis of diabetes. Diabetes Care. 38(Supplement 1), S8–S16 (2015).
Craig, C. L. et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 35(8), 1381–1395 (2003).
Ainsworth, B. E. et al. 2011 Compendium of physical activities: A second update of codes and MET values. Med. Sci. Sports Exerc. 43(8), 1575–1581 (2011).
Bao, W., Bowers, K., Tobias, D. K., Hu, F. B. & Zhang, C. Prepregnancy dietary protein intake, major dietary protein sources, and the risk of gestational diabetes mellitus: A prospective cohort study. Diabetes Care 36(7), 2001–2008 (2013).
Yong, H. Y. et al. Higher animal protein intake during the second trimester of pregnancy is associated with risk of GDM. Front. Nutr. 8, 718792 (2021).
Bai, D. et al. Prospective study of red meat intake in the first and second trimesters and the risk of gestational diabetes mellitus in Chengdu in 2017. Wei Sheng Yan Jiu. 50(1), 63–68 (2021).
Hezaveh, Z. S. et al. The association between maternal dietary protein intake and risk of gestational diabetes mellitus. Int. J. Prev. Med. 10, 197 (2019).
Kurotani, K. et al. Red meat consumption is associated with the risk of type 2 diabetes in men but not in women: A Japan Public Health Center-based Prospective Study. Br. J. Nutr. 110(10), 1910–1918 (2013).
Radesky, J. S. et al. Diet during early pregnancy and development of gestational diabetes. Paediatr. Perinatal Epidemiol. 22(1), 47–59 (2008).
Tremblay, F., Lavigne, C., Jacques, H. & Marette, A. Role of dietary proteins and amino acids in the pathogenesis of insulin resistance. Annu. Rev. Nutr. 27, 293–310 (2007).
Linn, T. et al. Effect of long-term dietary protein intake on glucose metabolism in humans. Diabetologia 43(10), 1257–1265 (2000).
Anderson, K. E. et al. Meat intake and cooking techniques: Associations with pancreatic cancer. Mutat. Res. 506–507, 225–231 (2002).
Everett, C. J. et al. Association of urinary polycyclic aromatic hydrocarbons and serum C-reactive protein. Environ. Res. 110(1), 79–82 (2010).
Alshaarawy, O., Zhu, M., Ducatman, A., Conway, B. & Andrew, M. E. Polycyclic aromatic hydrocarbon biomarkers and serum markers of inflammation. A positive association that is more evident in men. Environ. Res. 126, 98–104 (2013).
Uribarri, J. et al. Advanced glycation end products in foods and a practical guide to their reduction in the diet. J. Am. Diet. Assoc. 110(6), 911–16.e12 (2010).
Vlassara, H. et al. Oral AGE restriction ameliorates insulin resistance in obese individuals with the metabolic syndrome: A randomised controlled trial. Diabetologia 59(10), 2181–2192 (2016).
Mohtashaminia, F. et al. Adherence to the Mediterranean diet and risk of gestational diabetes: a prospective cohort study. BMC Pregnancy Childbirth 23(1), 647 (2023).
Grosso, G. et al. A comprehensive meta-analysis on evidence of Mediterranean diet and cardiovascular disease: Are individual components equal?. Crit. Rev. Food Sci. Nutr. 57(15), 3218–3232 (2017).
Ibsen, D. B. et al. Replacement of red and processed meat with other food sources of protein and the risk of type 2 diabetes in european populations: The EPIC-InterAct study. Diabetes Care 43(11), 2660–2667 (2020).
Funding
This study was supported by Semnan University of Medical Sciences (Grant number: 3278).
Author information
Authors and Affiliations
Contributions
A.J., S.S.-B., and M.M.K. conceived and designed the study, R.N., A.J., S.A., and A.E. contributed to the data gathering, R.N. and A.J. analyzed the data, R.N., A.J., S.A., and A.E. wrote the first draft of the manuscript, S.S.-B. and M.M.K. critically revised the manuscript. All authors have read and approved the final manuscript. S.S.-B. had primary responsibility for final content.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Norouziasl, R., Jayedi, A., Mirmohammadkhani, M. et al. Consumption of red and processed meat during early pregnancy and risk of gestational diabetes: a prospective birth cohort study. Sci Rep 14, 5209 (2024). https://doi.org/10.1038/s41598-024-55739-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-55739-6
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
