
Abstract
Vitamin C played pleiotropic roles in critical illness and vitamin C insufficiency was predictive of the development of multiple organ failure. Currently, the prevalence of vitamin C insufficiency in Chinese critically ill patients is rarely determined and there are no established bedside tools to predict hypovitaminosis C. To develop a nomogram to identify patients with high risk of hypovitaminosis C, we performed a bi-center prospective cohort study at two ICUs of the first and sixth medical center in PLA General Hospital, Beijing, China from May 6th to July 31st, 2021 We identified 322 eligible patients. 62.4% patients were hypovitaminosis C. 7 features, including source of infection, the level of serum albumin, age, male gender, sepsis, vascular disease, and wasting of vitamin C by the kidney, were selected using LASSO algorithm and therefore included in the nomogram. In the testing set, our model showed moderate discrimination ability with areas under the curve of 0.75 [0.64–0.84]. Variable importance evaluated by SHAP value highlighted two novel important predictors, i.e., abdominal infection and the level of serum albumin. In conclusion, we first reported a high burden of vitamin C insufficiency in Chinese adult patient in the ICU. We also constructed a prediction model to timely identify patients with high risk of hypovitaminosis C, which allows the clinicians to choose appropriate candidates for Vitamin C repletion in clinical practice or clinical trials.
Similar content being viewed by others


Introduction
Vitamin C is an essential nutrient which cannot be synthesized or stored in humans1. It played pleiotropic roles in critical illness in terms of anti-oxidative injury, anti-inflammation, and synthesis of endogenous catecholamine, etc.1. Vitamin C insufficiency [including hypovitaminosis C (i.e., plasma vitamin C < 23 μmol/L) and vitamin C deficiency (i.e., plasma vitamin C < 11 μmol/L)] is commonly seen in critically ill patients, and measurements seem to be much lower in patients with sepsis2.
Low plasma concentration of vitamin C was predictive of the development of multiple organ failure3. Given scientific rationale of vitamin C treatment in sepsis, interest in supplementation of vitamin C has rapidly increased. However, from the inception of the “cocktail therapy (i.e., hydrocortisone, ascorbic acid [vitamin C], and thiamine, HAT)” strategy generated in a cohort study4, most of the subsequent randomized clinical trials (RCTs), including ACTS5, ORANGES6, HYVCTTSSS7, VITAMINS8, and VICTAS9, failed to meet the pre-defined primary endpoints, such as 28d or 30d mortality, or length of ICU stay, etc. Moreover, vitamin C using as monotherapy in sepsis also confirmed the aformentioned findings. In CITRIS-ALI study conducted among patients with sepsis and ARDS, vitamin C did not significantly improve organ dysfunction scores or alter markers of inflammation and vascular injury10. LOVIT study11 and its secondary analysis12 again proved invalidity of vitamin C in sepsis. Why effect of vitamin C on sepsis or septic shock among studies was so conflict? As an adjunctive therapy, it is reasonable to assume that only patients with vitamin C insufficiency could benefit from intravenous administration. However, none of the aforementioned RCTs have listed vitamin C insufficiency as the inclusion criteria since timely measurement of plasma vitamin C before randomization is not available. Hence, bedside screening for patients with high risk of vitamin C insufficiency is warranted.
In our prospective cohort study, we sought to describe the prevalence of vitamin C insufficiency in Chinese adult patients in the intensive care units (ICU), and establish a nomogram for clinicians to identify patients with high risk of hypovitaminosis C at ICU admission.
Methods
Study design and general information
The study was a bi-center, prospective cohort study conducted at two ICUs of the first and sixth medical center in PLA General Hospital, Beijing, China from May 6th to July 31st, 2021 (Registered on http://www.chictr.org.cn, ChiCTR2100043451 on 3rd June, 2021). Approval for the study was granted by the Ethics Committee of PLA General Hospital. Written informed consent forms were obtained by the patients or their legal proxies when patient consent was not available due to critical illness within 24 h after admission. These patients were followed up until death, discharge from the ICUs, or till 7 days, whichever applied to the patient. All methods were performed in accordance with the Declaration of Helsinki. In performing this study, we followed the recommendations established in the Transparency Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD) initiative13.
Inclusion criteria
All patients over 18 years old admitted to the ICUs of the first and sixth medical center in PLA general hospital.
Exclusion criteria
-
1.
Being pregnant or postpartum;
-
2.
Prior administration of intravenous Vitamin C within 1 week;
-
3.
3.Post-cardiopulmonary resuscitation;
-
4.
Discharged or having incomplete data within 24 h of admission;
-
5.
Consent forms cannot be obtained.
If patients were admitted to the ICUs for multiple times, only data from the first admission was recorded during the study period.
Outcome measures
The primary outcome was hypovitaminosis C, and the secondary outcome was vitamin C deficiency2. Blood samples were harvested immediately after the written consent forms were signed. Plasma Vitamin C were measured via Qlife Lab 9000 HPLC system (Qlife, Nanjing, China) for research purpose14.
Predictors
A list of candidate predictors with a known association with hypovitaminosis C were determined a priori, including age15, gender, obesity16, smoking17, and infectious disease18. In addition, comorbidities such as chronic respiratory diseases19, diabetes20, hypertension21, moderate to severe heart failure22, cancer with chemotherapy23, disorders of the gastrointestinal tract24 and liver cirrhosis25, and factors which lead to wasting of vitamin C by the kidneys24 were also included. Since vitamin C is actively accumulated in human granulocytes26 and vitamin C might be depleted in acute phase response due to oxidative stress, we assumed that biomarkers such as neutrophil lymphocyte ratio (NLR), C-reactive protein (CRP), and procalcitonin (PCT) might also be promising predictors. As vascular disease was associated with low vitamin C intake and high plasma fibrinogen concentration27, primary diagnosis of vascular disease and biomarkers including fibrinogen, D-dimer and prothrombin time (PT) were also collected as eligible predictors. In addition, serum lactate level was included for proper diagnosis of septic shock28. Sepsis and septic shock were established according to Sepsis 3.0 definition28 by a senior clinician unaware of the research purpose.
In general, our study encompasses demographics, Sequential organ function assessment (SOFA) score, comorbidities and presumed risk factors of vitamin C insufficiency, laboratory tests (determined by the primary investigators), and source of infection (if applicable). The clinical events during 7 days follow-up were also documented only to fully describe characteristics of enrolled patients. The details of included variables were presented in Supplemental Table S1.
Sample size calculation
The sample size was calculated to ensure that there were enough records for the development of the model. In terms of binary outcome, events per variable of 5 is needed29. With a presumed prevalence of hypovitaminosis C around 60% in adult patients17,30,31 in the ICU and 27 variables as potential risk factors, at least (27 × 5/0.6) = 225 samples are needed for the training dataset.
Statistical analysis
A statistical analysis protocol was prepared prior to data collection. Only participants with available measurements of plasma vitamin C were included in the final analysis. With regard to missing data, the “missing at random” assumption was applied. Missing data of continuous variables other than levels of plasma vitamin C were imputed with the median value of the entire feature column, and variables with a missing rate more than 5% were excluded.
The included patients were randomly divided into a training set and a testing set at a ratio of 7:3. For comparison of variables between groups, continuous data were presented as median with interquartile range (IQR, 25–75th percentiles) and compared with Mann–Whitney U test, while categorical variables were presented as frequencies and compared with a chi-square test. All analyses were two-sided, and a p value of less than 0.05 was considered statistically significant.
Prediction models were developed using logistic regression. Univariable models were fit for each predictor to assess individual associations. Restricted cubic spline (RCS) with three knots was used to account for potential non-linearity in the association between continuous predictors and the outcome. When evidence of a non-linear relationship was found, RCS was further used to model the effects of those predictors in multivariable model.
In the training set, variable selection was performed using a least absolute shrinkage and selection operator (LASSO) approach, where data values are shrunk towards a central point as the mean, i.e., forcing the β-coefficients of each factor to be zero32. All the listed eligible variables assessed in the univariable analyses were included in the LASSO algorithm. The predictors selected by LASSO algorithm were finally included in a logistic regression model.
Model performance was assessed as follows. The area under the receiver-operating-characteristics curve (AUROC) was deployed to evaluate the model discrimination. Bootstrapping based methods with 1000 resamples were applied to adjust for the overfitting33. Resampling model calibration through calibration curve was conducted to evaluate the model calibration. F1 score34, accuracy 35, sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were also calculated. Decision curve analysis (DCA) was implemented to assess the applicability of the prediction model36. We reported the above measurements of model performance both in training and testing dataset.
For better interpretation of the prediction model, a nomogram was established based on a logistic regression with variables selected by LASSO algorithm. The Shapley additive explanation (SHAP) was also applied to test how individual factors in this analysis contributed to hypovitaminosis C.
We also developed a prediction model for vitamin C deficiency. To meet the thumb rule of events per variable29, the model was derived from the complete cohort and the performances was adjusted with 1,000-fold bootstrapping.
Statistical analyses were conducted using R version 3.5.3 (R Core Team, R Foundation for Statistical Computing, Vienna, Austria) with relevant packages (tableone, rms, ROCR, glmnet, pROC, plyr, Hmisc, magrittr, rpart). Data pre-processing, model development and validation, and visualization of results are implemented using Python version 3.9 with related packages (pandas, numpy, scikit-learn, matplotlib).
Results
Patient characteristics
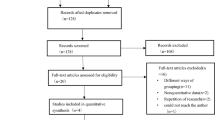
A total of 322 patients with available measurements of plasma vitamin C were eligible for the present study, who were divided into a training dataset with 225 patients and a testing dataset with 97 patients. Supplemental Fig. S1 shows the flowchart of the study. Overall, the median age was 68.00 [58.00, 79.00] years old, and 64.9% were male. 75.5% patients received mechanical ventilation. 13.7% developed acute kidney injury and 8.1% received renal replacement therapy within 7 days. 4% died within 7 follow-up days. 62.4% patients were hypovitaminosis C and 34.2% patients were vitamin C deficiency. Among all the candidate predictors, only CRP had missing values and therefore was imputed with the median of overall population.
Table 1 showed twenty-seven candidate variables differentiating between the training and testing sets, as well as the clinical events. The only significant difference found in the validation set was a higher serum level of D-dimer, which was negligible.
Comparison of patient characteristic grouped by hypovitaminosis C or vitamin C deficiency was demonstrated in Supplemental Tables S2 and S3. Patients with hypovitaminosis C or vitamin C deficiency were more likely to have older age, higher prevalence of vascular diseases, sepsis or septic shock, abdominal sepsis, higher SOFA score, higher levels of CRP, PCT, D-dimer, NT-pro brain natriuretic peptide (NT-pro BNP), creatinine, and prolonged PT but lower levels of albumin. Moreover, substantial differences in 7 days mortality and prolonged duration of mechanical ventilation were observed between the two groups. Additionally, patients with vitamin C deficiency were more likely to have lower BMI.
Development of a prediction model in training set
In the training set, 144 (62.2%) patients were hypovitaminosis C. In the univariable logistic regression analyses, age, levels of albumin, CRP, PT, NT-pro BNP, D-dimer, PCT, sepsis, SOFA score, source of infection, and vascular disease were found to be associated with hypovitaminosis C. The ORs with 95% CI are shown in Table 2. It is noted that NT-pro BNP, CRP, D-dimer, PCT, PT, SOFA score showed non-linear relationship with hypovitaminosis C (data not shown).
All 27 variables were included in the LASSO algorithm to perform feature selection to find a balance between model simplicity and accuracy in the training set. When the adjustment parameter was lambda.min (λ = 0.033), 7 features with nonzero coefficients were selected as important indices for the prediction of hypovitaminosis C (Supplemental Fig. S2), including source of infection, sepsis, serum albumin, age,male gender, wasting vitamin C by kidney, and vascular disease. The 7 features were included in the final logistic regression model. Notably, age (OR 1.02; 95% CI 1.01–1.04; p = 0.010), vascular disease (OR 9.28; 95% CI 2.04–42.20; p = 0.004), infection originated from abdomen (OR 2.31; 95% CI 1.02–5.22; p = 0.044), and level of albumin (OR 0.89; 95% CI 0.84–0.94; p = 0.000) were shown to be associated with hypovitaminosis C (Table 2).
To better interpretate the prediction, a nomogram was constructed, as described in Fig. 1a. Each predictor was corresponded to a single score shown on the top line of the nomogram. The total score of each patient is the summation of each single score. On the bottom line of the nomogram, the probabilities of hypovitaminosis C in ICU patients were predicted in terms of total score.

The nomogram for hypovitaminosis C (a) and Vitamin C deficiency (b).
To evaluate the contribution of any particular feature to the difference between actual and mean predictions, the SHAP values of 7 selected features in the predictive model were reported in Fig. 2a. It was noted that source of infection and levels of serum albumin were shown to be the most important predictors of hypovitaminosis C. Patients who had infection originated from abdomen were more likely to have hypovitaminosis C. Moreover, lower albumin level was a significant factor in the model against hypovitaminosis C. We further developed a WeChat based mini program named “HYPOVC” for bedside application (Supplemental Fig. S4).

Contributions of input features to prediction. This importance matrix plot depicts the importance of each feature in the development of the final predictive model. The higher the SHAP value of a feature, the higher the probability of hypovitaminosis C (a) or vitamin C deficiency (b).
Given the thumb rule of events per variable29, prediction model against Vitamin C deficiency was developed in the complete cohort. The ORs with 95% CI in the univariable and multivariable analyses were shown in Supplemental Table S4. All 27 variables were included in the LASSO algorithm to perform feature selection. When the adjustment parameter was lambda.min (λ = 0.034), 6 predictors were selected (Supplemental Fig. S5) and therefore included in the final model, which were source of infection, sepsis, serum albumin, age, wasting vitamin C by kidney, and vascular disease . Age (OR 1.02; 95% CI 1.00–1.04; p = 0.016), vascular disease (OR 4.50; 95% CI 1.84–11.02; p = 0.001), and septic shock (OR 2.68; 95% CI 1.01–7.15; p = 0.048) were shown to be independently associated with vitamin C deficiency. The nomogram of vitamin C deficiency and SHAP values were presented in Figs. 1b, and 2b, respectively.
Evaluation and validation of prediction model
Performances of the prediction model against hypovitaminosis C were presented in Table 3. The bootstrap-adjusted C index was 0.76 [0.69–0.83] and 0.75 [0.64–0.84] in the training and testing set, respectively. The ROC curve was shown in Supplemental Fig. S3a and b. In Supplemental Fig. S3c and d, the calibration curves indicated that there was good consistency between the predicted values and the actual observed values. As shown in Supplemental Fig. S3e and f, DCA demonstrated that the nomogram had good overall net benefits.
The aforementioned model performances were also evaluated in prediction model against vitamin C deficiency and adjusted with 1000-fold bootstrapping, as shown in Supplemental Table S5 and Supplemental Fig. S6. The bootstrap-adjusted C index was 0.72 [0.66–0.77].
Discussion
In this study of 322 Chinese adult patients in the ICU, nearly two thirds of them were hypovitaminosis C and one third of them were vitamin C deficiency. To our knowledge, this is the first study that constructed a bedside tool to identify patients with high risk of hypovitaminosis C with data available at admission to the ICU, which allows clinicians to screen eligible patients who might be benefit from vitamin C supplementation. Our study also highlighted infection originated from abdomen and serum albumin as novel predictors of hypovitaminosis C.
The epidemiology of vitamin C insufficiency was fully determined in lots of countries other than China. Our study reported a high burden of vitamin C insufficiency in Chinese ICU patients, which was in consistent with data from a cohort of 44 critical ill patients in New Zealand2. It is worth mentioning that abdominal surgeries were performed in 39.1% of patients in our cohort, indicating antecedent malabsorption of vitamin C. Since vitamin C cannot be synthesized by humans but only absorbed via enteral or parenteral nutrition1, the prevalence of vitamin C insufficiency still needs to be further determined in medical ICUs.
Aside from advanced age15, male gender16, sepsis or septic shock18, vascular disease27, and factors which leads to wasting of vitamin C by the kidneys24, our study also identified two novel important predictors of hypovitaminosis C, i.e. abdominal sepsis and serum albumin, using variable importance analysis based on SHAP value (the change in the prediction when the feature is added compared with the baseline for a given prediction37). Infection originated from abdomen implied malabsorption of vitamin C, and thereby was related with vitamin C insufficiency. Moreover, hypoalbuminemia was considered as a severity marker of underlying pulmonary capillary leakage in patients with COVID-1938, while administration of vitamin C could protect against vascular leakage in murine abdominal sepsis39, indicating underlying association between hypoalbuminemia and vitamin C insufficiency.
From the inception of the index cohort study4, in which administration of HAT remarkably reduced mortality of sepsis, the effect of vitamin C on sepsis or septic shock has generated deeply debate since plenty of subsequent RCTs using either HAT therapy5,6,8,9, or monotherapy of vitamin C11,40 failed to verify the improvement of survival. The common perspective, as a recent meta-analysis indicated, is that vitamin C might be able to improve delta SOFA score and reduce the duration of vasopressor use, but is not associated with reduction in short-term mortality41. In our opinion, the aforementioned controversy could be prominently attributed to discrepant timing42, duration43,44, dose45 of vitamin C administration, and more importantly, the inclusion criteria during patient recruitment.
Candidates in the current clinical trials were consist of plenty patients with pulmonary infection5,6,8,9,11,40. However, a recent animal study demonstrated that vitamin C therapy only worked in intra-abdominal sepsis other than pneumonia due to different inflammatory responses to infection34, indicating that pulmonary sepsis should be excluded in the future study. Therefore, in CITRIS-ALI study10 conducted only in patients with sepsis and ARDS, a 96-h infusion of vitamin C did not significantly improve organ dysfunction or vascular injury. It was further confirmed by our study since only intra-abdominal infection was associated with hypovitaminosis C rather than other resources. More importantly, patients in those trials5,6,8,9,11,40 were not all vitamin C insufficiency, and therefore would not benefit from vitamin C administration. Only two studies measured the baseline levels of vitamin C after patient recruitment. In ORANGES6, half of the enrolled patients were hypovitaminosis C, and the average levels of plasma vitamin C was higher in the treatment group (29.6 ± 56.8 μmol/L vs. 27.3 ± 22.7 μmol/L), albeit no statistical difference. The same story repeated in LOVIT study (20.6 ± 70.6 vs. 19.1 ± 39.7 μmol/L)11. It is noted that levels of plasma vitamin C were 14.1 ± 11.8 μmol/L in the treatment group in the index study4. Our study further elucidated that critical ill patient with hypovitaminosis C had higher 7 days mortality and prolonged duration of mechanical ventilation. Therefore, we speculated that the efficacy of vitamin C supplementation can only be observed among patients with vitamin C insufficiency, and that’s why identification of those patients before randomization is warranted.
Measurement of plasma vitamin C levels involves cumbersome techniques (direct measurement by HPLC or indirect measurement by RedoxSYS System46) that are impossibly to be available in all hospital laboratories and unlikely to provide a rapid turnaround time. Our study makes it possible to identify patients with high risk of hypovitaminosis C at admission to the ICU, and thus chose appropriate candidates for clinical trials before randomization. For better understanding and general application in the clinical settings, we chose LASSO algorithm with logistic regression in the model development process and further described it in a nomogram. The included predictors were all available at admission. Our Model achieved moderate discrimination and calibration both in the training and testing sets. However, given the small sample size of our cohort, we were not able to validate the model against vitamin C deficiency. In general, we believe that this study developed a promising predictive model of hypovitaminosis C at ICU admission.
Our study has several limitations. First, the enrolled candidates came from two ICUs in which most of the patients were originated from department of general surgery. The prevalence of vitamin C insufficiency might be overestimated due to malabsorption. Therefore, external validation to determine generalizability of our model is warranted, especially among patients from medical ICU. Second, the number of events per variable of vitamin C deficiency is relatively small. The performance of the model was only adjusted with bootstrapping-based method in the derivation cohort per se, and thus overfitting could not be overlooked.
Conclusions
In our prospective cohort study, we reported a high burden of hypovitaminosis C and vitamin C deficiency in Chinese adult critical ill patients. We for the first-time developed a predictive model and constructed a nomogram to predict the risk of hypovitaminosis C using variables that are commonly available at ICU admission.
Data availability
The data are available for other investigators’ use under reasonable request. Please contact the corresponding author for access requests.
References
Marik, P. E. Vitamin C for the treatment of sepsis: The scientific rationale. Pharmacol. Ther. 189, 63–70. https://doi.org/10.1016/j.pharmthera.2018.04.007 (2018).
Carr, A. C. et al. Hypovitaminosis C and vitamin C deficiency in critically ill patients despite recommended enteral and parenteral intakes. Crit. Care (Lond. Engl.) 21, 300. https://doi.org/10.1186/s13054-017-1891-y (2017).
Borrelli, E. et al. Plasma concentrations of cytokines, their soluble receptors, and antioxidant vitamins can predict the development of multiple organ failure in patients at risk. Crit. Care Med. 24, 392–397. https://doi.org/10.1097/00003246-199603000-00006 (1996).
Marik, P. E., Khangoora, V., Rivera, R., Hooper, M. H. & Catravas, J. Hydrocortisone, vitamin C, and thiamine for the treatment of severe sepsis and septic shock: A retrospective before-after study. Chest 151, 1229–1238. https://doi.org/10.1016/j.chest.2016.11.036 (2017).
Moskowitz, A. et al. Effect of ascorbic acid, corticosteroids, and thiamine on organ injury in septic shock: The ACTS randomized clinical trial. JAMA 324, 642–650. https://doi.org/10.1001/jama.2020.11946 (2020).
Iglesias, J. et al. Outcomes of metabolic resuscitation using ascorbic acid, thiamine, and glucocorticoids in the early treatment of sepsis: The ORANGES trial. Chest 158, 164–173. https://doi.org/10.1016/j.chest.2020.02.049 (2020).
Chang, P. et al. Combined treatment with hydrocortisone, vitamin C, and thiamine for sepsis and septic shock: A randomized controlled trial. Chest 158, 174–182. https://doi.org/10.1016/j.chest.2020.02.065 (2020).
Fujii, T. et al. Effect of vitamin C, hydrocortisone, and thiamine vs hydrocortisone alone on time alive and free of vasopressor support among patients with septic shock: The VITAMINS randomized clinical trial. JAMA 323, 423–431. https://doi.org/10.1001/jama.2019.22176 (2020).
Sevransky, J. E. et al. Effect of vitamin C, thiamine, and hydrocortisone on ventilator- and vasopressor-free days in patients with sepsis: The VICTAS randomized clinical trial. JAMA 325, 742–750. https://doi.org/10.1001/jama.2020.24505 (2021).
Fowler, A. A. 3rd. et al. Effect of vitamin C infusion on organ failure and biomarkers of inflammation and vascular injury in patients with sepsis and severe acute respiratory failure: The CITRIS-ALI randomized clinical trial. JAMA 322, 1261–1270. https://doi.org/10.1001/jama.2019.11825 (2019).
Lamontagne, F. et al. Intravenous vitamin C in adults with sepsis in the intensive care unit. N. Engl. J. Med. 386, 2387–2398. https://doi.org/10.1056/NEJMoa2200644 (2022).
Hemilä, H. & Chalker, E. Abrupt termination of vitamin C from ICU patients may increase mortality: Secondary analysis of the LOVIT trial. Eur. J. Clin. Nutr. 77, 490–494. https://doi.org/10.1038/s41430-022-01254-8 (2023).
Collins, G. S., Reitsma, J. B., Altman, D. G. & Moons, K. G. Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD): The TRIPOD statement. BMJ 350, g7594. https://doi.org/10.1136/bmj.g7594 (2015).
Rozemeijer, S., van der Horst, F. A. L. & de Man, A. M. E. Measuring vitamin C in critically ill patients: Clinical importance and practical difficulties-Is it time for a surrogate marker?. Crit. Care 25, 310. https://doi.org/10.1186/s13054-021-03670-x (2021).
Teixeira, A., Carrié, A. S., Généreau, T., Herson, S. & Cherin, P. Vitamin C deficiency in elderly hospitalized patients. Am. J. Med. 111, 502. https://doi.org/10.1016/s0002-9343(01)00893-2 (2001).
Via, M. The malnutrition of obesity: Micronutrient deficiencies that promote diabetes. ISRN Endocrinol. 2012, 103472. https://doi.org/10.5402/2012/103472 (2012).
Crook, J., Horgas, A., Yoon, S. J., Grundmann, O. & Johnson-Mallard, V. Insufficient vitamin C levels among adults in the United States: Results from the NHANES surveys, 2003–2006. Nutrients 13, 3910. https://doi.org/10.3390/nu13113910 (2021).
Fain, O. et al. Hypovitaminosis C in hospitalized patients. Eur. J. Intern. Med. 14, 419–425. https://doi.org/10.1016/j.ejim.2003.08.006 (2003).
Abuhajar, S. M., Taleb, M. H. & Ellulu, M. S. Vitamin C deficiency and risk of metabolic complications among adults with chronic respiratory diseases: A case-control study. Clin. Nutr. ESPEN 43, 448–455. https://doi.org/10.1016/j.clnesp.2021.03.007 (2021).
Christie-David, D. J. & Gunton, J. E. Vitamin C deficiency and diabetes mellitus—Easily missed?. Diabet. Med. 34, 294–296. https://doi.org/10.1111/dme.13287 (2017).
Morelli, M. B., Gambardella, J., Castellanos, V., Trimarco, V. & Santulli, G. Vitamin C and cardiovascular disease: An update. Antioxidants (Basel) 9, 1227. https://doi.org/10.3390/antiox9121227 (2020).
Song, E. K. & Kang, S. M. Vitamin C deficiency, high-sensitivity C-reactive protein, and cardiac event-free survival in patients with heart failure. J. Cardiovasc. Nurs. 33, 6–12. https://doi.org/10.1097/jcn.0000000000000389 (2018).
Mayland, C. R., Bennett, M. I. & Allan, K. Vitamin C deficiency in cancer patients. Palliat. Med. 19, 17–20. https://doi.org/10.1191/0269216305pm970oa (2005).
Maxfield, L. & Crane, J. S. in StatPearls (StatPearls Publishing Copyright © 2022, StatPearls Publishing LLC., 2022).
Coelho, J. M. et al. Association between serum and dietary antioxidant micronutrients and advanced liver fibrosis in non-alcoholic fatty liver disease: An observational study. PeerJ 8, e9838. https://doi.org/10.7717/peerj.9838 (2020).
Moser, U. & Weber, F. Uptake of ascorbic acid by human granulocytes. Int. J. Vitam. Nutr. Res. 54, 47–53 (1984).
Bulpitt, C. J. Vitamin C and vascular disease. BMJ 310, 1548–1549. https://doi.org/10.1136/bmj.310.6994.1548 (1995).
Singer, M. et al. The third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA 315, 801–810. https://doi.org/10.1001/jama.2016.0287 (2016).
Vittinghoff, E. & McCulloch, C. E. Relaxing the rule of ten events per variable in logistic and Cox regression. Am. J. Epidemiol. 165, 710–718. https://doi.org/10.1093/aje/kwk052 (2007).
Sharma, Y., Popescu, A., Horwood, C., Hakendorf, P. & Thompson, C. Prevalence of hypovitaminosis C and its relationship with frailty in older hospitalised patients: A cross-sectional study. Nutrients 13, 2117. https://doi.org/10.3390/nu13062117 (2021).
Tomasa-Irriguible, T. M. & Bielsa-Berrocal, L. COVID-19: Up to 82% critically ill patients had low Vitamin C values. Nutr. J. 20, 66. https://doi.org/10.1186/s12937-021-00727-z (2021).
Hutmacher, M. M. & Kowalski, K. G. Covariate selection in pharmacometric analyses: A review of methods. Br. J. Clin. Pharmacol. 79, 132–147. https://doi.org/10.1111/bcp.12451 (2015).
Smith, G. C., Seaman, S. R., Wood, A. M., Royston, P. & White, I. R. Correcting for optimistic prediction in small data sets. Am. J. Epidemiol. 180, 318–324. https://doi.org/10.1093/aje/kwu140 (2014).
Gabriel, R. A. et al. Machine learning-based models predicting outpatient surgery end time and recovery room discharge at an ambulatory surgery center. Anesth. Analg. 135, 159–169. https://doi.org/10.1213/ane.0000000000006015 (2022).
Schemper, M. Predictive accuracy and explained variation. Stat. Med. 22, 2299–2308. https://doi.org/10.1002/sim.1486 (2003).
Vickers, A. J. & Elkin, E. B. Decision curve analysis: a novel method for evaluating prediction models. Med. Decis. Mak. 26, 565–574. https://doi.org/10.1177/0272989x06295361 (2006).
Mahajan, A. et al. Development and validation of a machine learning model to identify patients before surgery at high risk for postoperative adverse events. JAMA Netw. Open 6, e2322285. https://doi.org/10.1001/jamanetworkopen.2023.22285 (2023).
Wu, M. A. et al. Hypoalbuminemia in COVID-19: Assessing the hypothesis for underlying pulmonary capillary leakage. J. Intern. Med. 289, 861–872. https://doi.org/10.1111/joim.13208 (2021).
Zhou, G., Kamenos, G., Pendem, S., Wilson, J. X. & Wu, F. Ascorbate protects against vascular leakage in cecal ligation and puncture-induced septic peritonitis. Am. J. Physiol. Regul. Integr. Comp. Physiol. 302, R409-416. https://doi.org/10.1152/ajpregu.00153.2011 (2012).
Wacker, D. A. et al. Evaluating vitamin C in septic shock: A randomized controlled trial of vitamin C monotherapy. Crit. Care Med. 50, e458–e467. https://doi.org/10.1097/ccm.0000000000005427 (2022).
Liang, B., Su, J., Shao, H., Chen, H. & Xie, B. The outcome of IV vitamin C therapy in patients with sepsis or septic shock: A meta-analysis of randomized controlled trials. Crit. Care 27, 109. https://doi.org/10.1186/s13054-023-04392-y (2023).
Long, M. T. et al. Early hydrocortisone, ascorbate and thiamine therapy for severe septic shock. Crit. Care Shock 23, 23–34 (2020).
Carr, A. C. Duration of intravenous vitamin C therapy is a critical consideration. Crit. Care Resusc. 21, 220–221 (2019).
Jung, S. Y., Lee, M. T., Baek, M. S. & Kim, W. Y. Vitamin C for ≥ 5 days is associated with decreased hospital mortality in sepsis subgroups: A nationwide cohort study. Crit. Care 26, 3. https://doi.org/10.1186/s13054-021-03872-3 (2022).
Zhang, J. et al. Pilot trial of high-dose vitamin C in critically ill COVID-19 patients. Ann. Intensive Care 11, 5. https://doi.org/10.1186/s13613-020-00792-3 (2021).
Rozemeijer, S. et al. Rapid screening of critically ill patients for low plasma vitamin C concentrations using a point-of-care oxidation-reduction potential measurement. Intensive Care Med. Exp. 9, 40. https://doi.org/10.1186/s40635-021-00403-w (2021).
Funding
This work was supported by grants from the “Field Internal Science” Army Key Discipline Construction. The results and conclusions reported in this paper are independent from the funding sources.
Author information
Authors and Affiliations
Contributions
J.H. and F.H.Z. conceived the study idea and designed the study. Q.L., X.H., W.W.W., and J.G.S. collected the data. J.W.Z. processed the corrected data. D.W. analyzed the data. J.H. wrote the initial draft of the manuscript. All authors revised the manuscript for intellectual content and approved the final version of the manuscript. The corresponding author attests that all listed authors meet the authorship criteria and that no others meeting the criteria have been omitted.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hu, J., Zhang, J., Li, D. et al. Predicting hypovitaminosis C with LASSO algorithm in adult critically ill patients in surgical intensive care units: a bi-center prospective cohort study. Sci Rep 14, 5073 (2024). https://doi.org/10.1038/s41598-024-54826-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-54826-y
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
