
Abstract
The ketogenic diet (KD) has been shown to be effective in refractory epilepsy after long-term administration. However, its interference with short-term brain metabolism and its involvement in the early process leading to epilepsy remain poorly understood. This study aimed to assess the effect of a short-term ketogenic diet on cerebral glucose metabolic changes, before and after status epilepticus (SE) in rats, by using [18F]-FDG PET. Thirty-nine rats were subjected to a one-week KD (KD-rats, n = 24) or to a standard diet (SD-rats, n = 15) before the induction of a status epilepticus (SE) by lithium-pilocarpine administrations. Brain [18F]-FDG PET scans were performed before and 4 h after this induction. Morphological MRIs were acquired and used to spatially normalize the PET images which were then analyzed voxel-wisely using a statistical parametric-based method. Twenty-six rats were analyzed (KD-rats, n = 15; SD-rats, n = 11). The 7 days of the KD were associated with significant increases in the plasma β-hydroxybutyrate level, but with an unchanged glycemia. The PET images, recorded after the KD and before SE induction, showed an increased metabolism within sites involved in the appetitive behaviors: hypothalamic areas and periaqueductal gray, whereas no area of decreased metabolism was observed. At the 4th hour following the SE induction, large metabolism increases were observed in the KD- and SD-rats in areas known to be involved in the epileptogenesis process late—i.e., the hippocampus, parahippocampic, thalamic and hypothalamic areas, the periaqueductal gray, and the limbic structures (and in the motor cortex for the KD-rats only). However, no statistically significant difference was observed when comparing SD and KD groups at the 4th hour following the SE induction. A one-week ketogenic diet does not prevent the status epilepticus (SE) and associated metabolic brain abnormalities in the lithium-pilocarpine rat model. Further explorations are needed to determine whether a significant prevention could be achieved by more prolonged ketogenic diets and by testing this diet in less severe experimental models, and moreover, to analyze the diet effects on the later and chronic stages leading to epileptogenesis.
Similar content being viewed by others

Introduction
The temporal lobe epilepsy (TLE) is the most common form of focal epilepsy in humans, usually characterized by recurrent localized seizures in specific regions of the cerebral cortex, coupled with hippocampal atrophy and sclerosis1,2,3,4,5,6. Overall, it is reported that more than 30% of epileptic patients have drug-resistant seizures4,7.
The ketogenic diet (KD) is a high-fat, low-carbohydrate diet already used, for decades, as an alternative therapy in refractory TLE8,9. In clinical trials, it has been proven to be effective in reducing seizures by 50% after 3 months of administration compared to the control groups, with response maintained for up to one year. Therefore, KD remains an attractive option especially, in children and adolescents with refractory epilepsy for whom surgery was ruled out9,10,11. Recently, international experts recommend the initiation of the KD within the first week after the diagnosis during the acute phase, with the need to be continued for up to 3 months (post-acute phase) if proven to be effective12.
In animal studies, the effect of ketogenic diet on epilepsy treatment has been already studied, often involving its administration before inducing a status epilepticus13,14,15,16,17. Neurons and astrocytes exhibit the capacity to absorb and catabolize β-hydroxybutyrate and acetoacetate, using ketone bodies in mitochondria for energy production and amino acid synthesis18,19,20.
In vivo imaging techniques, such as [18F]-fluorodeoxyglucose positron emission tomography ([18F]-FDG PET) and magnetic resonance imaging (MRI) can be used as two complementary noninvasive imaging techniques to evaluate brain metabolic changes, particularly the glucose metabolism, at an early stage of epilepsy4,21. Their combination provides functional information from molecular PET imaging and morphological information from the MRI. Their coupling with quantitative analyses brings new diagnostic solutions by giving complementary elements on the detection of small brain abnormalities and on the characterization of the seizure location4,21,22,23. In a previous study from our team, the changes in the brain glycolytic metabolism have been characterized and quantified using [18F]-fluorodeoxyglucose positron emission tomography (PET) imaging in a lithium-pilocarpine epilepsy model, displaying an early hypermetabolism on site known to be involved in the epileptogenesis process (piriform and entorhinal cortex, hippocampus)21.
One of the most recognized method for semi-quantitative analysis of neuroimaging data is Statistical Parametric Mapping (SPM), widely used in preclinical studies21,24. SPM also tends to improve the visual assessment in various clinical studies25,26,27,28. It improves reproducibility and is a time saver compared to visual analyses.
By using [18F]-FDG PET and a dedicated voxel-based quantification pipeline, the present study aimed to assess the effect of a short-term ketogenic diet (7 days) on cerebral metabolic changes, before and after the status epilepticus (SE) and especially within the brain areas known to be involved in the later stages of epiletogenesis development.
Results
Ketogenic diet before SE
For the 15 KD-rats at D-1, the 7-days of the KD were associated with significant increases of the body weight (321 ± 25 vs. 256 ± 23 g, p < 0.05) and of the plasma β-hydroxybutyrate (1.67 ± 0.37 vs.1.16 ± 0.36 mmol/L, p < 0.05), but with a stable glycemia (6.11 ± 0.85 vs. 6.59 ± 1.11 mmol/L, NS) (Table 1).
The paired comparisons of the PET images before (D-8) and after (D-1) the KD showed areas of significant enhanced glycolytic brain metabolism at D-1, mainly within the hypothalamus (increased metabolism volume = 21.54 mm3T-voxel max at 5.21) and the periaqueductal grey matter (9.88 mm3, T-voxel max at 5.76) In contrast, no hypometabolic areas at D-1 were observed. The details are reported in Fig. 1 and Table 2.

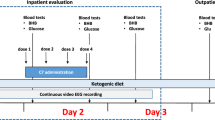
Study design. D-8 and D-1 are defined as eight and one day before status epilepticus (SE) respectively, H+4 is defined as four hours after SE.
SE after the ketogenic or standard diets
On the day of the SE induction, the level of plasma β-hydroxybutyrate was higher for the KD-rats than for the SD-rats (1.67 ± 0.37 vs. 1.08 ± 0.3 mmol/L, p < 0.05), but there was no significant difference between these 2 groups, neither for the body weight (321 ± 25 vs. 358 ± 31 g, NS), nor for the glycemia (6.59 ± 1.11 vs. 6.72 ± 0.25 mmol/L, NS) (Table 3).
All pilocarpine-treated rats entered convulsive SE of which 4 SD rats died during or after 4 h of convulsive SE.
The characteristics of the lithium pilocarpine-induced SE state were not influenced by the ketogenic diet. In each group, the event characteristics were like those previously documented in this model29,30,31.The rats of all groups exhibited the same behavioral features after the lithium-pilocarpine administration. Within 5 min after the pilocarpine injection, the rats developed diarrhea, piloerection, and other signs of cholinergic stimulation. During the following 10–20 min, the rats exhibited head bobbing, scratching, chewing, and exploratory behavior. Recurrent seizures started after pilocarpine administration with associated episodes of head and bilateral forelimb myoclonus with the animals rearing up on their hind legs and falling. They progressed to SE around 30–40 min after the pilocarpine injection.
The recurrent seizure thresholds seemed to appear faster in KD rats compared to SD rats (12–30 min after the pilocarpine injection vs. 18 to 32 min, in the KD and SD rats respectively, p < 0.05). The SE severity, however, was similar between the two groups.
The results of the paired comparisons of PET images recorded before the SE (D-8) and at the 4th hour following the SE induction (H+4), are detailed in Fig. 2 for both groups and in Tables 4, 5 and Tables 6, 7 for the SD- and KD-rats’ groups, respectively. Both groups exhibited equivalent increases of the brain metabolism and within the same brain areas (Tables 4 and 6)., i.e., hippocampus (KD-rats: 71.83 mm3, T-voxel max at 15.52 vs. SD-rats: 68.77 mm3, 15.48), parahippocampic areas (83.20 mm3, 8.10 vs. 45.29 mm3, 11.05), thalamic and hypothalamic areas (20.77 mm3, 5.37 vs. 50.22 mm3, 11.62), periaqueductal gray (4.10 mm3, 5.62 vs. 17.85 mm3, 10.12), limbic structures (33.48 mm3, 8.10 vs. 4.26 mm3, 5.53). An increase of the brain metabolism was observed on the motor cortex for KD-rats (32.57 mm3, 8.23). Hypometabolic areas were also observed in some areas as in the corpus callosum or in the cingular cortex (Table 5 and 7).

Representation of the spatial normalization pipeline. The PET images are normalized using non-linear transformations estimated between the SIGMA MRI (used to create the Atlas) and the individual MRI of each rat. PET images were previously registered to their individual MRI.
No significant differences were observed for the unpaired comparisons between the [18F]-FDG PET images from SD- and KD-rats at the 4th hour following SE induction.
Discussion
After status epilepticus (SE), a dynamic process start, leading to an abnormal brain network reorganization32, metabolic changes and neurodegeneration, contributing to the establishment of the chronic disease. On the rat lithium-pilocarpine model, a brain glycolytic hypermetabolism occurring 1 to 4 h after SE, has already been documented in the areas known to be involved in the subsequent epileptogenesis process (mostly in the regions related to SE propagation as piriform cortex, amygdala, CA1 of the hippocampus, and the hilus of dentate gyrus (DG))21,29,30.
Therefore, by using [18F]-FDG-PET and a dedicated voxel-based quantification pipeline, we attempted to investigate the impact of a short-term ketogenic diet (7 days) on the brain glycolytic metabolism, in a well-known and validated model of TLE, the rat lithium-pilocarpine model, with a special focus on the metabolism of the brain areas known to be involved in the subsequent epileptogenesis process.
To reduce the variation in glucose metabolism caused by a KD, we tested the effects of this diet on the brain metabolism in healthy rats. The diet was well tolerated, with the animals considerably gaining weight within one week. The blood level of the ketone bodies was also significantly increased, confirming previous works reporting a drastic carbohydrate reduction during 3 to 5 days, can induce a ketosis15,33. However, we noted that glycemia remained unchanged despite the 7-day low-carbohydrate diet in accordance with results from previously published studies34,35,36.
We used a voxel-based method for the PET images analysis (SPM), which provides an objective semi-quantification of the brain metabolic changes. We specifically designed a dedicated SPM pipeline for this study. The spatial normalization step using anatomical MRI images guarantees the best localization and ensures a total independence of the normalization and statistical analyses37. It is not the case when the voxel information from the PET scans is used in the two steps. Actually, it might lead to a loss of spatial accuracy and to a dispersion of the voxel values and then, to a loss of power of the statistical analysis38,39. This statement is particularly relevant in our study for H+4 acquired images. In fact, the important hypermetabolism during SE is responsible for large differences between the to-be-normalized images and the PET template. The intensity normalization is also a crucial step in [18F]-FDG semi-quantitative studies. The concentration reaching the brain is subject-dependent because of different physiological factors, such as, among others, the blood glucose level, medications, and age40. The proportional scaling is widely used but was not adapted for our study. In fact, a significantly higher global intensity at H+4 (in comparison with D-8) can lead to an attenuation of the hypermetabolism areas and create an artificial hypometabolism in normal areas on H+4 normalized images. In previous studies on the lithium-pilocarpine rodent model21,41,42, the pons was recommended as the reference region for the intensity normalization, but we did not use it in our study in order to take in consideration the metabolism variations within the pons due to the ketogenic diet. Opposed to the anatomical reference region methods, the histogram-based method used in this paper is data-driven and efficient to detect abnormal patterns without requiring previous knowledge about the analyzed model or disease43. This method has already been used in other preclinical studies44 and also proved its efficiency in a clinical context40. Indeed, although they are present, the artificial hypometabolic areas at H+4 (vs D-8) are limited and considered as false positive because no metabolism decrease during SE is reported in the literature.
This pipeline was firstly applied to the [18F]-FDG PET images recorded in healthy rats before (D-8) and after a 7-days (D-1) ketogenic diet (KD) before the induction of the epilepsy. Paired analyses gave clear evidence of a KD-related hypermetabolism in periaqueductal gray (PAG) and hypothalamic areas. In the brain, these structures are activated through the food intake and reward processes and have extensive connections mediating the appetitive and the consummatory behaviors45. The periaqueductal gray matter has long been known as a region modulating fear and anxiety-related reactions46,47,48,49. More recently, its role in regulating and driving appetitive behaviors and its connections to the central feeding network of the brain, such as the hypothalamus, have been explored48,50. Likewise, previous study has also shown that the inactivation of PAG in rats alters the hypothalamic signaling and the food consumption45. Our data provide new evidence that hypothalamic areas and PAG may play a major role in appetitive behaviors and that 7 days of ketogenic diet can induce brain metabolic changes in normal rats. In contrast, we observed no decrease in brain metabolism after a 7-day KD, showing a physiological consumption of glucose in other areas of the brain. This is in accordance with the observation of an unchanged plasma glucose in our KD rats. It must be kept in mind that complex metabolic adaptations may influence glucose regulation during short KD periods. More precisely, it is likely that certain enzymes of glucose metabolism have not yet been significantly downregulated after a 7-day period (i.e., metabolic adjustments could take a longer time to stabilize)51. In addition, it has been postulated that the control of metabolic enzymes and transporters could vary between different brain areas52. Finally, as suggested by Stincone et al., the acute use of ketone bodies during KD could lead to a paradoxical increase in the glucose release within blood, in order to maintain important functions such as the cytoplasmic antioxidant defense51,52.
After the SE induction, the SPM analysis showed a comparable increased metabolism within the primary sites that are subsequently implicated in the epileptogenesis process (hippocampic and parahippocampic areas, entorhinal and piriform cortices and thalamic and hypothalamic areas)15,21,30 in the KD group and in the SD group at H+4 compared to D-8. We observed slightly more pronounced hypermetabolic volumes in the KD group compared to the SD group. Several hypermetabolism areas, were also detected in the KD but not in the SD group, such as motor cortex (Tables 4 and 5). However, the inter-group comparisons do not show a significant difference in brain [18F]-FDG uptake, at H+4 of the SE, between the KD and SD rats using SPM.
The inability of the KD to prevent lithium-pilocarpine SE was already documented. A prior investigation by Linard et al. explored the effects of the ketogenic diet in the lithium-pilocarpine rat model, using an electroencephalogram and histological analysis. Their study demonstrated a significant decrease in hippocampal neuronal loss, specifically in CA1 and CA3 regions, in the KD-rats compared to SD-rats. However, no significant difference were observed in the characteristics of clinical events during the acute phase of lithium-pilocarpine SE between the two groups15.
Limitations and perspectives
Although the lithium-pilocarpine model reproduces the main clinical features of human TLE, extrapolation to the human epileptogenesis process remains difficult. In addition, it is likely that the KD effects could be different between rats and humans.
No histopathologic analyses were performed in the present study, which constitutes an additional limit. However, a number of previous studies published on this model, including a study from our team, have shown that most damaged neurons were located in the structures showing a significant increase in the metabolic activity during the status epilepticus30,53,54,55,56. The neuron damages and their potential prevention by a diet would be closely tied to the capacity of neurons to manage the extreme metabolic demands (3 to 6-folds increases) from certain brain regions57,58.
In these conditions and despite the preference for ketones, these brain areas should maintain a high glycolytic activity to meet the energy needs of the lithium-pilocarpine model.
As already discussed above, a 7-day KD may not be sufficiently long to complete the transition of the brain into a state of complete ketosis, using ketone bodies as the exclusive energy substrate. Achieving all the requisite metabolic alterations in the brain, might require a more prolonged period of ketogenic intervention.59,60.
The acute SE produced by the lithium-pilocarpine model is particularly aggressive, and it could be interesting to test KD on model gradually developing clinical and electroencephalographic seizure manifestations, such as the pentylenetetrazol (PTZ) perfusion rat model.
Another limitation is that the glycolytic metabolism assessed with [18F]-FDG-PET would not precisely correspond to the severity of neuronal loss61. The area of abnormal metabolism identified by interictal [18F]-FDG-PET often extends well beyond the epileptogenic zone, covering a large portion of the temporal lobe and surrounding regions55,61. Consequently, it may be worthy to explore alternative radiotracers such as [18F]flumazenil for a more precise delineation of the epileptogenic areas62,63.
A last limitation is that our study did assess the early stage of SE but did not extend to the later and chronic stages of the epileptogenesis process. A continued administration of throughout KD the chronic phase of epilepsy, would have provided a more comprehensive understanding of the KD impact on the epileptogenic process.
Conclusion
A one-week ketogenic diet does not prevent the status epilepticus (SE) and metabolic brain abnormalities in the lithium-pilocarpine rat model. Further explorations are needed to determine whether a significant prevention could be achieved by more prolonged ketogenic diets and by testing this diet in less severe experimental models, and moreover, to analyze the diet effects on the later and chronic stages leading to epileptogenesis.
Methods
Animals and study design
All experiments involving animals complied with the ARRIVE guidelines and were approved by the Lorraine Ethics Committee N°66 according to Guidelines of Animal Care and Use (APAFIS no. 16424-2018080814271998). Sprague–Dawley male rats (175–200 g) were purchased from Janvier Laboratories (Le Genest-Saint-Isle. France) and housed in ventilated cages including filter tops, under controlled environmental conditions (22 ± 2 °C, 55 ± 20% humidity) and 12-h light‐dark cycle.
The imaging timeline is illustrated in Fig. 3. A brain [18F]-FDG PET was recorded in 24 adult male rats (D-8) and then, after 7 days of a KD (D-1, Fig. 3) (3% carbohydrate, 73% fat, 15% protein, 0% fiber, 9% vitamins, and minerals; ketocal® SDS. France)31,64,65. A status epilepticus (SE) was thereafter induced in these KD-rats, with a third [18F]-FDG PET being recorded 4 h after the SE induction (H+4). A total of 24 KD rats were initially included in the study, but 4 rats had to be withdrawn due to technical issues encountered during the PET experiments. Additionally, 5 other rats were excluded from the analysis due to either a lack of MRI scans or the poor quality of PET images.

Anatomical localization of the areas of increased metabolic activity between Day (-8) and Day (-1) and for KD subjects (n = 11). The SPM-T maps were obtained using a paired test (p < 0.001, uncorrected, k > 50 voxels) then projected onto two-dimensional slices of T1-weighted MRI. The colorbar represents the T-values.
The same protocols of SE induction and H+4 [18F]-FDG PET recording were applied, for comparisons, in a control group of 15 rats submitted to a standard diet (SD-rats; 44% carbohydrate, 6% fat, 19% protein, 18% fiber, 13% vitamins, and minerals; Envigo. Gannat. France). In these SD-rats, a baseline [18F]-FDG PET scan was also performed, 7 days before SE induction (D-8). Moreover, for both groups, an MRI was realized before D-8. Food and water were given ad libitum in both groups and each rat was weighed daily at a fixed time with a dedicated small-animal scale (Mettler Toledo. DeltaRange-PR5002. France). Before each PET, two drops of blood were taken from the tip of the tail for the measurement of blood glucose and β-hydroxybutyrate levels by using Medisense Optium Xceed reader (Abbott France Division Medisense. Rungis.France)64.
Induction of the Status epilepticus
The SE was induced as described in previous studies21,64, by a subcutaneous injection of pilocarpine at a dose of 25 mg/kg, 1 h after a subcutaneous injection of 1 mg/kg of methyl scopolamine which limits the peripheral effects of pilocarpine, and 20 h after an intraperitoneal injection of 3 mEq/kg of lithium chloride allowing a significant reduction of the dose of pilocarpine required for seizure induction. Two hours after the onset of SE, all rats received an intramuscular injection of diazepam for muscle relaxation without halting status epilepticus (2.5 mg/kg, i.m. Valium; Roche.Basel, Switzerland)21,64. To assess the occurrence of seizures, all rats were monitored and video-recorded, for 4 h, immediately after pilocarpine injection. The SE was considered to start after 5 seizures including these three consecutive stages: clonic seizures, rearing and falling31,53,64.
PET imaging
Using a previously described methodology21, approximately 0.2 MBq/g of [18F]-FDG were injected in the tail vein under short-term anesthesia by inhalation of an isoflurane-oxygen mixture (2%–1.5 v/v) in the SD- and KD-rats. Then, the rats were put in their home cage back, in a quiet environment. The brain [18F] FDG-PET was recorded 45 min later with an Inveon PET system (Siemens. Knoxville. TN. USA), under the same isoflurane-oxygen anesthesia and with a 30-min emission sequence followed by a 10-min transmission sequence with Co-57 providing an attenuation correction map. Their respiration was monitored and maintained constant throughout the experiment. As previously described21, the brain [18F]-FDG PET images were reconstructed in kBq/ml using an OSEM-3D iterative method involving 4 iterations with 12 subsets and corrected for attenuation. The images were finally displayed with 0.26 × 0.26 × 0.80 mm3 voxels, reoriented and cropped to suppress most of the extracerebral signal.
MR imaging
Animals were anesthetized by inhalation of an isoflurane-oxygen mixture (3%–1.5 v/v) and their respiration was monitored and maintained constant throughout the experiment. Anatomical MRI reference images of the brain were obtained on a 3 Tesla scanner (Prisma, Siemens Healthineers®, Erlangen, Germany) with a rat-dedicated 8-channel volume coil (Rapid Biomedical GmbH®, Rimpar, Germany). T2‐weighted (T2-w) anatomical images were acquired using a 2D Turbo Spin-Echo sequence and with the following parameters: repetition time (TR)/echo-time (TE) = 2500/61 ms, voxel size = 0.255 × 0.255 × 1 mm3, 24 slices from the olfactory bulb to the brain stem, field of view (FOV) = 49 × 49 mm2, 8 averages.
At the end of the study, animals were sacrificed by intraperitoneal injection of Euthasol overdose (200 mg kg−1; Euthasol Vet. 400 mg ml−1).
Statistical parametric mapping
The PET images were pre-processed using SPM12 (Wellcome Department of Cognitive Neurology, Institute of Neurology, London, UK) running on Matlab 2020a (MathWorks Inc., Sherborn, MA).
MRI images of each animal were spatially normalized using the SIGMA MRI rat brain template66. The corresponding non-linear transformations were applied to the PET images previously co-registered to the MRI images of the same rats (see Fig. 4 for the overall normalization pipeline), and an isotropic 3D Gaussian kernel of 0.8 mm FWHM was subsequently applied. An intensity normalization was performed using the histogram-based (HB) method of Fuster et al.43 with a control PET template obtained by averaging the spatially normalized PET images of the 11 control rats (before the SE induction, D-8).

Areas of increased [18F]-FDG uptake observed at the 4th hour after induction of SE (i.e., with a paired comparison between the PET images recorded before SE and at the 4th hours after SE induction) in the 11 SD-rats (left panel) and 15 KD-rats (right panel). SPM-T maps are displayed with a Z score-based color scale, projected on T1-weighted MRI slices, and with the following parameters: p < 0.001 (no correction for multiple comparisons), and k > 38 voxels. The colorbar represents the T-values.
Paired sample t-tests were used to assess the brain metabolic effects of (i) the ketogenic diet before the SE induction, while comparing the D-8 and D-1 normalized PET images of KD group, and (ii) the SE while comparing the D-8 and H+4 normalized PET images of both KD and SD groups. Unpaired two-sample t-tests were also applied for direct comparisons of the KD and SD groups at H+4. For all tests and for each voxel setting in the main sites known to be involved in the epileptogenesis process of this model, notably the temporal cortical area (entorhinal and piriform cortex), the hippocampal and parahippocampic areas41,67,68, a p value < 0.001 corrected for cluster volume (by using the expected volume provided by SPM and based on the random field theory) was considered to reflect a significant metabolism change. Others regions were masked using the SIGMA rat brain atlas66.
Statistical analysis
All data are expressed as mean ± SEM. Statistical analyses were performed using the SPSS Statistics Software package v. 20 (IBM, NY, USA). Comparisons of quantitative variables were performed with ANOVA-test after verifying for distribution normality. P values < 0.05 were considered as statistically significant.
Ethical approval
All applicable international. national. and/or institutional guidelines for the care and use of animals were followed. This study was approved by the Lorraine Ethics Committee on Animal Experimentation (CELMEA LORRAIN N°66). (APAFIS number. 16424-2018080814271998).
Data availability
The datasets generated during the current study are available from the corresponding author on reasonable request.
References
Barañano, K. W. & Hartman, A. L. The ketogenic diet: Uses in epilepsy and other neurologic illnesses. Curr. Treat Options Neurol. 10, 410–419 (2008).
Simeone, T. A., Simeone, K. A., Stafstrom, C. E. & Rho, J. M. Do ketone bodies mediate the anti-seizure effects of the ketogenic diet?. Neuropharmacology 133, 233–241 (2018).
French, J. A. et al. Characteristics of medial temporal lobe epilepsy: I. Results of history and physical examination. Ann. Neurol. 34, 774–780 (1993).
Verger, A. et al. Temporal epilepsy lesions may be detected by the voxel-based quantitative analysis of brain FDG-PET images using an original block-matching normalization software. Ann. Nucl. Med. 30, 272–278 (2016).
Ren, E. & Curia, G. Synaptic reshaping and neuronal outcomes in the temporal lobe epilepsy. Int. J. Mol. Sci. 22, 3860 (2021).
Twible, C., Abdo, R. & Zhang, Q. Astrocyte role in temporal lobe epilepsy and development of mossy fiber sprouting. Front. Cell Neurosci. 15, 725693 (2021).
Weaver, D. F. & Pohlmann-Eden, B. Pharmacoresistant epilepsy: unmet needs in solving the puzzle(s). Epilepsia 54(Suppl 2), 80–85 (2013).
Peterman, M. G. The ketogenic diet in epilepsy. J. Am. Med. Assoc. 84, 1979–1983 (1925).
Neal, E. G. et al. The ketogenic diet for the treatment of childhood epilepsy: A randomised controlled trial. Lancet Neurol. 7, 500–506 (2008).
Lambrechts, D. J. E. et al. A randomized controlled trial of the ketogenic diet in refractory childhood epilepsy. Acta Neurol. Scand. 135, 231–239 (2017).
Sourbron, J. et al. Ketogenic diet for the treatment of pediatric epilepsy: review and meta-analysis. Childs Nerv. Syst. 36, 1099–1109 (2020).
Wickstrom, R. et al. International consensus recommendations for management of New Onset Refractory Status Epilepticus (NORSE) including Febrile Infection-Related Epilepsy Syndrome (FIRES): Summary and Clinical Tools. Epilepsia https://doi.org/10.1111/epi.17391 (2022).
Bough, K. J. et al. Mitochondrial biogenesis in the anticonvulsant mechanism of the ketogenic diet. Ann. Neurol. 60, 223–235 (2006).
Bough, K. J., Valiyil, R., Han, F. T. & Eagles, D. A. Seizure resistance is dependent upon age and calorie restriction in rats fed a ketogenic diet. Epilepsy Res. 35, 21–28 (1999).
Linard, B., Ferrandon, A., Koning, E., Nehlig, A. & Raffo, E. Ketogenic diet exhibits neuroprotective effects in hippocampus but fails to prevent epileptogenesis in the lithium-pilocarpine model of mesial temporal lobe epilepsy in adult rats. Epilepsia 51, 1829–1836 (2010).
Appleton, D. B. & DeVivo, D. C. An animal model for the ketogenic diet. Epilepsia 15, 211–227 (1974).
Rho, J. M., Szot, P., Tempel, B. L. & Schwartzkroin, P. A. Developmental seizure susceptibility of kv11 potassium channel knockout mice. Dev. Neurosci. 21, 320–327 (1999).
Nehlig, A. Age-dependent pathways of brain energy metabolism: the suckling rat, a natural model of the ketogenic diet. Epilepsy Res. 37, 211–221 (1999).
Sokoloff, L. et al. The [14 C]Deoxyglucose method for the measurement of local cerebral glucose utilization: theory, procedure, and normal values in the conscious and anesthetized albino rat. J. Neurochem. 28, 897–916 (1977).
Martinez-Hernández, A., Cloche, K. & Norenberg, M. Glutamine synthétase : localisation glial. Glutamine synthétase Localisation gliale dans le cerveau. Sciences 195, 1356–1358 (1977).
Poussier, S. et al. Quantitative SPM analysis involving an adaptive template may be easily applied to [18F]FDG PET images of the rat brain. Mol. Imaging Biol. 19, 731–735 (2017).
Willmann, O., Wennberg, R., May, T., Woermann, F. G. & Pohlmann-Eden, B. The contribution of 18F-FDG PET in preoperative epilepsy surgery evaluation for patients with temporal lobe epilepsy A meta-analysis. Seizure 16, 509–520 (2007).
Prieto, E. et al. Statistical parametric maps of 18F-FDG PET and 3-D autoradiography in the rat brain: a cross-validation study. Eur. J. Nucl. Med. Mol. Imaging 38, 2228–2237 (2011).
Zhang, L. et al. FDG-PET and NeuN-GFAP immunohistochemistry of hippocampus at different phases of the pilocarpine model of temporal lobe epilepsy. Int. J. Med. Sci. 12, 288–294 (2015).
Kim, Y. K. et al. (18)F-FDG PET in localization of frontal lobe epilepsy: comparison of visual and SPM analysis. J. Nucl. Med. 43, 1167–1174 (2002).
Kim, M. A. et al. Relationship between bilateral temporal hypometabolism and EEG findings for mesial temporal lobe epilepsy: analysis of 18F-FDG PET using SPM. Seizure 15, 56–63 (2006).
Plotkin, M. et al. Use of statistical parametric mapping of (18) F-FDG-PET in frontal lobe epilepsy. Nuklearmedizin 42, 190–196 (2003).
Kumar, A. et al. Objective detection of epileptic foci by 18F-FDG PET in children undergoing epilepsy surgery. J. Nucl. Med. 51, 1901–1907 (2010).
Da Silva Fernandes, M. J., Dubé, C., Boyet, S., Marescaux, C. & Nehlig, A. Correlation between hypermetabolism and neuronal damage during status epilepticus induced by lithium and pilocarpine in immature and adult rats. J. Cereb. Blood Flow Metab. 19, 195–209 (1999).
Dubé, C., Boyet, S., Marescaux, C. & Nehlig, A. Progressive metabolic changes underlying the chronic reorganization of brain circuits during the silent phase of the lithium-pilocarpine model of epilepsy in the immature and adult Rat. Exp. Neurol. 162, 146–157 (2000).
Raffo, E., François, J., Ferrandon, A., Koning, E. & Nehlig, A. Calorie-restricted ketogenic diet increases thresholds to all patterns of pentylenetetrazol-induced seizures: Critical importance of electroclinical assessment. Epilepsia 49, 320–328 (2008).
Doyen, M. et al. Metabolic connectivity is associated with seizure outcome in surgically treated temporal lobe epilepsies: A (18)F-FDG PET seed correlation analysis. Neuroimage Clin. 36, 103210 (2022).
Paoli, A. Ketogenic diet for obesity: Friend or foe?. IJERPH 11, 2092–2107 (2014).
Al-Mudallal, A. S., LaManna, J. C., Lust, W. D. & Harik, S. I. Diet-induced ketosis does not cause cerebral acidosis. Epilepsia 37, 258–261 (1996).
Melø, T. M., Nehlig, A. & Sonnewald, U. Neuronal–glial interactions in rats fed a ketogenic diet. Neurochem. Int. 48, 498–507 (2006).
Kuter, K. Z., Olech, Ł, Głowacka, U. & Paleczna, M. Increased beta-hydroxybutyrate level is not sufficient for the neuroprotective effect of long-term ketogenic diet in an animal model of early Parkinson’s disease. Exploration of brain and liver energy metabolism markers. IJMS 22, 7556 (2021).
Gispert, J. D. et al. Influence of the normalization template on the outcome of statistical parametric mapping of PET scans. Neuroimage 19, 601–612 (2003).
Ashburner, J. & Friston, K. J. Nonlinear spatial normalization using basis functions. Hum. Brain Mapp. 7, 254–266 (1999).
Martino, M. E. et al. Comparison of different methods of spatial normalization of FDG-PET brain images in the voxel-wise analysis of MCI patients and controls. Ann. Nucl. Med. 27, 600–609 (2013).
López-González, F. J. et al. Intensity normalization methods in brain FDG-PET quantification. NeuroImage 222, 117229 (2020).
Goffin, K., Van Paesschen, W., Dupont, P. & Van Laere, K. Longitudinal microPET imaging of brain glucose metabolism in rat lithium–pilocarpine model of epilepsy. Exp. Neurol. 217, 205–209 (2009).
Jupp, B. et al. Hypometabolism precedes limbic atrophy and spontaneous recurrent seizures in a rat model of TLE. Epilepsia 53, 1233–1244 (2012).
Martí Fuster, B. et al. FocusDET, a new toolbox for SISCOM analysis evaluation of the registration accuracy using Monte Carlo simulation. Neuroinform 11, 77–89 (2013).
Proesmans, S. et al. Voxel-based analysis of [18F]-FDG brain PET in rats using data-driven normalization. Front. Med. 8, 744157 (2021).
Tryon, V. L. & Mizumori, S. J. Y. A novel role for the periaqueductal gray in consummatory behavior. Front. Behav. Neurosci. 12, 178 (2018).
Rizvi, T. A., Ennis, M., Behbehani, M. M. & Shipley, M. T. Connections between the central nucleus of the amygdala and the midbrain periaqueductal gray: topography and reciprocity. J. Comp. Neurol. 303, 121–131 (1991).
Krukoff, T. L., Harris, K. H. & Jhamandas, J. H. Efferent projections from the parabrachial nucleus demonstrated with the anterograde tracer Phaseolus vulgaris leucoagglutinin. Brain Res. Bull. 30, 163–172 (1993).
Krout, K. E., Jansen, A. S. & Loewy, A. D. Periaqueductal gray matter projection to the parabrachial nucleus in rat. J. Comp. Neurol. 401, 437–454 (1998).
Depaulis, A. & Bandler, R. The midbrain periaqueductal gray matter: functional, anatomical, and neurochemical organization (Springer Science & Business Media, Berlin, 2012).
Behbehani, M. M., Park, M. R. & Clement, M. E. Interactions between the lateral hypothalamus and the periaqueductal gray. J. Neurosci. 8, 2780–2787 (1988).
Stincone, A. et al. The return of metabolism: biochemistry and physiology of the pentose phosphate pathway. Biol. Rev. 90, 927–963 (2015).
Zilberter, Y. & Zilberter, M. The vicious circle of hypometabolism in neurodegenerative diseases: Ways and mechanisms of metabolic correction. J. Neurosci. Res. 95, 2217–2235 (2017).
Turski, L., Ikonomidou, C., Turski, W. A., Bortolotto, Z. A. & Cavalheiro, E. A. Review: Cholinergic mechanisms and epileptogenesis. The seizures induced by pilocarpine: A novel experimental model of intractable epilepsy. Synapse 3, 154–171 (1989).
Cavalheiro, E. A. The pilocarpine model of epilepsy. Ital. J. Neuro Sci. 16, 33–37 (1995).
Dubé, C. & Nehlig, A. Conséquences des crises épileptiques subintrantes sur le développement cérébral: Relation entre l’agression initiale et le développement d’une épilepsie temporale. Epilepsies 13, 147–158 (2001).
Perosa, S. R. et al. Kinin B1 and B2 receptors are overexpressed in the hippocampus of humans with temporal lobe epilepsy. Hippocampus 17, 26–33 (2007).
Maalouf, M., Rho, J. M. & Mattson, M. P. The neuroprotective properties of calorie restriction, the ketogenic diet, and ketone bodies. Brain Res. Rev. 59, 293–315 (2009).
Gasior, M., Rogawski, M. A. & Hartman, A. L. Neuroprotective and disease-modifying effects of the ketogenic diet. Behav. Pharmacol. 17, 431–439 (2006).
Kossoff, E. H. et al. Optimal clinical management of children receiving dietary therapies for epilepsy: Updated recommendations of the International Ketogenic Diet Study Group. Epilepsia Open 3, 175–192 (2018).
Stafstrom, C. E. & Rho, J. M. The ketogenic diet as a treatment paradigm for diverse neurological disorders. Front. Pharmacol. 3, 59 (2012).
Foldvary. Correlation of Hippocampal Neuronal Density and FDG-PET in Mesial Temporal Lobe Epilepsy (1999).
Ryvlin, P. Clinical utility of flumazenil-PET versus [18F]fluorodeoxyglucose-PET and MRI in refractory partial epilepsy. A prospective study in 100 patients. Brain 121, 2067–2081 (1998).
Vivash, L. et al. 18 F-Flumazenil: A γ-aminobutyric acid A-specific PET radiotracer for the localization of drug-resistant temporal lobe epilepsy. J. Nucl. Med. 54, 1270–1277 (2013).
Linard, B., Ferrandon, A., Koning, E., Nehlig, A. & Raffo, E. Ketogenic diet exhibits neuroprotective effects in hippocampus but fails to prevent epileptogenesis in the lithium–pilocarpine model of mesial temporal lobe epilepsy in adult rats. Epilepsia 51, 1829–1836 (2010).
Clément, A. et al. A 1-week extension of a ketogenic diet provides a further decrease in myocardial 18F-FDG uptake and a high detectability of myocarditis with FDG-PET. J. Nucl. Cardiol. 27, 612–618 (2020).
Barrière, D. A. et al. The SIGMA rat brain templates and atlases for multimodal MRI data analysis and visualization. Nat. Commun. 10, 5699 (2019).
Curia, G., Longo, D., Biagini, G., Jones, R. S. G. & Avoli, M. The pilocarpine model of temporal lobe epilepsy. J. Neurosci. Methods 172, 143–157 (2008).
Guo, Y. et al. In vivo mapping of temporospatial changes in glucose utilization in rat brain during epileptogenesis: An 18F-fluorodeoxyglucose-small animal positron emission tomography study. Neuroscience 162, 972–979 (2009).
Funding
This study was funded by the Lorraine University through a dedicated Nancyclotep call for proposal and by the French National Health Ministry (“early research funding for residents”).
Author information
Authors and Affiliations
Contributions
M.D., C.L., E.Ro., H.B., B.C., J.P., A.V., E.Ra., G. K., P.M., F.M. contributed substantially to the study design, data collection, and/or data analysis and interpretation. M.D., E.Ro., and F.M. wrote the manuscript and C. L., B.C., A.V., P.M., critically revised the manuscript. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Doyen, M., Lambert, C., Roeder, E. et al. Assessment of a one-week ketogenic diet on brain glycolytic metabolism and on the status epilepticus stage of a lithium–pilocarpine rat model. Sci Rep 14, 5063 (2024). https://doi.org/10.1038/s41598-024-53824-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-53824-4
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
