
Abstract
Socio-cognitive impairment is frequent in multiple sclerosis (MS). However, little is known about the relationship between other potentially relevant clinical symptoms (i.e., cognition, depression, fatigue) and the degree of socio-cognitive impairment, and neural mechanisms underlying socio-cognitive deficits in MS. Therefore, we meta-analytically quantified socio-cognitive impairment in MS. A systematic literature search in MEDLINE Ovid, Web of Science Core Collection, CENTRAL, and PsycInfo was conducted until December 2022. Studies investigating affective or cognitive theory of mind (a/cToM), visual perspective taking (VPT) and social decision making (SDM) in MS patients relative to healthy controls were included. Risk-of-bias (RoB) was assessed using the CLARITY group “Tool for Assessing RoB in Cohort Studies”. Mediation analysis investigated the contribution of clinical symptoms to socio-cognitive impairment. In total, n = 8534 studies were screened, 58 were included in the systematic review, 27 in the meta-analyses. Most studies were rated with a moderate RoB. Meta-analyses confirmed impairment of both aToM and cToM in MS patients, with larger effect sizes for aToM. Mediation analysis demonstrated that higher levels of fatigue selectively predicted the degree of cToM impairment. There was insufficient data available to quantify impairment in other socio-cognitive domains. Fourteen structural and functional imaging studies were identified and characterized by substantial heterogeneity. Summarized, this study confirmed substantial socio-cognitive impairment in MS and highlights the potential exacerbating role of comorbid clinical symptoms. We identify several evidence gaps that need to be addressed in future large-scale studies using comprehensive and coordinated assessments of socio-cognitive parameters, potential mediators, and neural correlates.
Trial registration: The pre-registered review protocol can be assessed at www.crd.york.ac.uk/PROSPERO/ (ID: CRD42020206225).
Similar content being viewed by others


Introduction
Multiple sclerosis (MS) is a chronic and progressive neurodegenerative disease leading to heterogenous neurological deficits1, including up to 70% of patients suffering from cognitive impairment2, fatigue3 or depression4. Besides these well-documented symptoms, impairment of social cognition (SC), an umbrella term describing how people process, store, and apply information relevant to social interactions5, have also been reported in MS6,7. For example, MS-patients may have problems understanding the emotions of others (affective Theory of Mind , aToM), or their cognitive states, beliefs, thoughts, or intentions (cognitive Theory of Mind, cToM)8. Several, recent meta-analyses have demonstrated moderate effect sizes for impairment of both aToM and cToM in patients with MS compared to healthy controls9,10,11. In the clinical presentation of MS-patients, there is a strong interplay between cognition, fatigue, and depression, which often complicates diagnostic evaluation and initiating adequate treatment12. However, the potential impact of these symptoms on socio-cognitive impairment has not yet been addressed. Moreover, while there is an extensive literature on the functional and structural brain correlates underlying impaired cognition8, fatigue13, and depression14 in MS, only a few studies have used brain imaging methods, such as functional and structural magnetic resonance imaging (MRI), to investigate the neural underpinnings of socio-cognitive deficits in MS.
To address these open issues, we initially performed a systematic review of all studies assessing SC in patients with MS across three broad socio-cognitive domains (i.e., social perception, social understanding and social decision making15), investigated methodological biases and conducted a meta-analysis to quantify the degree of socio-cognitive impairment in MS relative to healthy controls. In a second step, we conducted a meta-regression analyses to identify potential mediators of socio-cognitive impairment in MS. Finally, we also provide an overview of studies that also investigated the functional and structural correlates of SC impairment in MS using MRI based measures.
Results
Search results
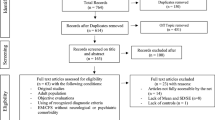
The search strategy yielded 10,615 articles (including the results of the update search). After deduplication, 8,534 unique articles had their titles and abstracts assessed for eligibility. From these articles, 8,424 articles were ineligible. 117 full-texts were assessed further and 58 studies included in the systematic review (Table 1), 14 of which also provided information on imaging data and the neural correlates of SC (Table 2). 27 studies were included in pairwise meta-analyses, 18 studies providing information on both social cognition and clinical outcomes in the mediation analysis. The PRISMA flow-diagram16 in Fig. 1 illustrates the study selection process.

PRISMA Diagram of the study selection process.
Included studies
In the following paragraphs, the results of the systematic review will be presented (1.1) as well as the systematic review results of studies including data on cognition, depression, and fatigue (1.2). In the following, the risk of bias analysis will be presented (1.3) and the results of the meta-analyses (1.4), which are divided in results for the analysis of cToM (1.4.1) and aToM (1.4.2). These results are followed by on overall sensitivity analysis (1.5). In a second step, we investigated the impact of depression, fatigue and cognitive status on socio-cognitive impairment in a meta-regression (2) and present the results on the neural correlates of socio-cognitive decline (3), again separately for aToM (3.1) and cToM (3.2).
Systematic review
Table 1 provides an overview of all included studies detailing demographic and clinical sample characteristics, socio-cognitive tasks used and the main results. Overall, 58 studies that investigated SC in patients with MS were included. Of those, all except for two studies17,18 provided information on the type of MS. The majority of patients were diagnosed with relapsing–remitting MS (RR-MS). MS is generally more prevalent in women19, which is also reflected in skewed sex distributions of the included study samples (with one exception20).
All except one study21 used ToM as one of their outcomes. Cognitive ToM was assessed in 31 studies and assessed using either variations of the faux-pas task (a task comprising a situation/context where one character (the speaker) makes a statement that is unintentionally offensive to the listener because the speaker has a false belief), a false-belief task (two different types: first-order false-belief tasks involve attribution about other’s false belief with regard to real events; second-order false-belief tasks assess what people think about other people’s thoughts), a strange stories task (a selection of stories that test pretense, jokes, lies, white lies, misunderstandings, persuasion, appearance/reality, figures of speech, irony, double bluffs, contrary emotions, and forgetting) or a video test (a series of videotaped vignettes of social scenarios followed by questions about thoughts, feelings, and/or intentions of the characters). Cognitive TOM was found to be impaired in patients with MS in 26 of 31 studies. Affective ToM was measured in 52 studies using different types of emotion recognition or processing tasks, in which either the eyes or the whole face of a person were presented. Participants were then asked to label the emotion represented by the eyes/face. 42 out of 52 studies showed an impairment in emotion recognition and/or emotion processing in MS patients compared to healthy controls. Two studies investigated VPT22,23, both showing significantly reduced imitation and poorer accuracy in perspective taking than healthy controls. SDM was investigated in two studies21,24 using either a moral/conventional distinction task (in which social situations and moral and conventional transgressions were presented, as well as an authority jurisdiction)24, or vignettes consisting of moral dilemmas (e.g. choice of whether or not to harm a person to save five other people)21. Results showed a lack of distinction between conventional and moral judgement in patients with MS24, as well as a reduced moral permissibility in patients with MS21.
Systematic review of studies including data on cognition, depression, and fatigue
Notably, even though information on the level of depressive symptoms, fatigue, and degree of cognitive impairment are essential for treatment decisions, only 18 out of 58 studies reported data on all three domains. All of them showed higher fatigue and depressive scores in patients with MS compared to healthy controls. In all studies, depression was described as mild because patients with severe symptoms were generally excluded. Several cognitive domains were reported as impaired in patients in MS compared to healthy controls, including executive functions25,26, semantic fluency27, and IQ scores27. Three studies17,28,29 included depressive and fatigue scores as control variables in their analyses; two of them found that even after controlling for these variables, patients with MS performed significantly worse on aToM28 and cToM tasks28,29, one study found no significant influence of these variables on impaired ToM performance17. Two studies showed a significant negative correlation between aToM performance and depressive symptoms (higher depressive scores were associated with lower aToM scores)1,30. Only one study did not demonstrate correlations between socio-cognitive measures and depression31. Three studies showed a significant positive correlation between aToM and cognition (higher aToM scores were associated with better performance on long-term storage and retrieval tasks, the Symbol-digit-modalities test32; and semantic fluency and IQ27). Reduced performance in ToM correlated with poorer executive function, intellectual ability and episodic memory31, and cToM and IQ and semantic fluency27. Pfaff et al. showed that inhibition and divided attention measures were predictive of difficulties in identifying facial emotions (aToM) in MS patients33, Montembeault et al. reported a positive correlation between general cognition (Montreal Cognitive Assessment, MoCA), but not with attention, measured with the Brief Test of Attention, the Symbol-Digit-Modalities Test, or the Stroop Inhibition task34.
Risk of bias assessment
Results of the RoB Assessment are shown in Table 3. Overall, only one domain was rated with a low RoB in all studies concerning the assessment of the study outcome, namely “Can we be confident in the assessment of the outcome?”. Most studies did not match their groups for possible confounders (e.g., comorbid depression) or controlled for possible confounding variables, leading to either an unsure RoB when no data was provided or to high RoB in cases were confounders were not assessed.
Meta-analyses
Meta-analyses were only possible for the primary outcome (ToM), because there was not enough data available for the remaining socio-cognitive domains (SDM, VPT). Due to the high heterogeneity of outcomes and ToM constructs, we decided to calculate separate analyses for cToM (Results of Faux-Pas Tests and results of Video tests) and aToM (often labelled as emotion recognition). Furthermore, if applicable, we subdivided the meta-analysis in the respective tests used for assessment to ensure better comparability.
Cognitive theory of mind
Faux-Pas test
Overall, ten studies were included in the meta-analysis that included variations of the faux-pas test and compared patients with MS and healthy controls. Four used the faux-pas task by Baron-Cohen et al.35, five the faux-pas task by Stone et al.36, and one study using a faux-pas task included in a Social Cognition battery. Results showed that healthy controls performed significantly better than MS patients across the different tasks: SMD = (− 0.50), 95% CI (− 0.85) to (− 0.16), I2 = 79%) and also in each of the two task versions where sufficient data was available for separate analyses (Baron-Cohen task: SMD = (− 0.35), 95% CI − 0.86 to 0.16, I2 = 78%; Stone Task: SMD = (− 0.70), 95% CI − 1.26 to 0.14, I2 = 84%). A forest plot for the outcome is displayed in Fig. 2a.

Forest plots of cognitive theory of mind tasks.
Video test
Seven studies were included that investigated differences in performance using four different types of ToM Video Tests between healthy controls and patients with MS. Overall results are reported, because there was not enough data available to consider individual outcomes. The overall result indicates that healthy controls performed significantly better on Video Tests than patients with MS (SMD = (− 0.70), 95% CI (− 1.21) to (− 0.30), I2 = 75%). The forest plot for the outcome is displayed in Fig. 2b.
Affective theory of mind/emotion recognition
Twenty studies were included in the meta-analyses that investigated aToM tasks. The overall effect size of the random effects analysis was − 0.75(CI:(− 0.93) to (− 0.57), favoring healthy controls. Nine studies used the Baron-Cohen Adult Eyes Test, showing better performance in healthy controls compared to MS patients (SMD = − 0.83, 95% CI (− 1.15) to (− 0.51), I2 = 77%). Two studies used the Emotion Recognition Florida Affective Battery (SMD = − 0.87, 95% CI (− 1.15) to (− 0.59), I2 = 0%); four studies used the Facial Expression of Emotion (FEEST) Tests (SMD = − 0.55, 95% CI (− 0.93) to (− 0.17), I2 = 71%) and four studies used similar experimental emotional recognition tasks that were grouped together as they all used different tests (SMD = − 0.71, 95% CI (− 1.15) to (− 0.59), I2 = 0%), all of them showing a better performance in healthy controls than patients with MS. The forest plot is displayed in Fig. 3.

Forest plots of affective theory of mind tasks.
Sensitivity analyses
The results of the sensitivity analyses using fixed effects models are displayed in Figs. 2a,b and 3 and did not show any significant differences compared to the random effects models.
Meta-regression analyses: Impact of depression, fatigue and cognitive status on socio-cognitive impairment
Meta-regressions analyses could be conducted for cToM(faux-pas), cTom(videos), and aToM, see Table 4. Due to the substantial heterogeneity of assessments that were used to quantify cognitive impairment, fatigue and depression, as well as insufficient data, we were not able to integrate the variable cognition, as well as depression for cToM(faux-pas) and fatigue for cTom(videos). In the analysis on cToM(faux-pas), that included three studies27,29,37, R2 was 100% (meaning 100% of the difference in true effect sizes can be explained by the predictor fatigue), and the intercept as well as the predictor fatigue were significant (intercept: − 1.73 (p < 0.001), fatigue: 0.02 (p < 0.05)). This means that performance on cTom (faux-pas) decreased with higher fatigue levels. In the meta-regression on cToM(video), four studies were included28,38,39,40. Yet, the overall model did not reach significance (R2 = 0%), so the predictor depression did not explain any additional variance in the results. Five studies that investigated aToM were included1,17,22,27,37. The intercept (the difference in performance between healthy controls and patients with MS when all predictors have a value of 0) was significant (− 1.82, p < 0.05) and favored healthy controls, similar to the other results. Both predictors, depression (0.13), and fatigue (0.01) did not reach significance. The overall R2 of the model was 28.73% and the I2 was at 32.76%, indicating only low heterogeneity.
Neural Correlates of socio-cognitive decline
Fourteen studies provided information on the neural correlates of socio-cognitive impairment in MS. Among those, thirteen studies investigated aToM, nine studies investigated cToM (for a detailed overview please see Table 2).
aToM
Eleven studies used structural MRI to investigate neural correlates of aToM using a number of different outcomes (e.g., eyes or faces tests, aToM composite scores). Of those, four studies demonstrated positive correlations between total white matter lesion volume and aToM performance41,42,43,44, one with total grey matter volume43. Using more regional approaches, two studies revealed association between aToM and white matter lesions44 or other DTI derived metrics (e.g., fractional anisotropy, mean diffusivity41), highlighting the potential role of disconnection of regions associated with socio-cognitive processing. Six studies that used voxel-based morphometry or assessed regional cortical thickness demonstrated positive correlations between aToM and integrity of the amygdala, fronto-temporal and other regions26,28,44,45, whereas two studies could not confirm these findings46,47.
Four studies used task-free resting-state functional imaging26,30,40,46 and three of these studies highlighted the contribution of frontal and temporal networks to aToM impairment in MS. Specifically, they demonstrated a negative correlation between implicit emotion recognition performance and functional connectivity of the fusiform gyrus with lateral occipital gyrus40, a positive association between RMET performance and functional connectivity between the left amygdala and frontal pole/paracingulate cortex26, or decreased functional connectivity between fronto-temporal regions in patients compared to controls during a facial affect recognition task30. On the other hand, Bisecco et al.46 did not find any correlations between the RMET performance and functional connectivity of the default mode, bilateral fronto-parietal executive, salience, cerebellar and limbic networks.
cToM
Eight out of nine studies investigated neural correlates of cToM using structural MRI. Three studies investigated the association to the total white matter lesion volume, with two studies demonstrating a negative association between the lesion volume and the video test performance28,43, and one study without an association between the lesion volume and the faux-pas task ability44. One study failed to show a significant correlation between cToM performance and total grey matter volume28.
Regional grey matter volume reductions were investigated in seven studies. Of those, three studies demonstrated a significant correlation between reduced volume of the thalamus and reduced cToM performance22,45,47 and additional positive correlations between grey matter volumes in different cortical regions (e.g., insula, frontal cortex, temporal and parietal cortex) and cToM. Four studies did not find any association between performance and regional grey matter integrity43,44,46,48. Two studies demonstrated an association between altered white matter DTI metrices (i.e., reduced FA and higher MD), especially in the corpus callosum and the superior fasciculus41,48. Two studies used resting-state fMRI and found that increased functional connectivity between the occipital cortex and the cerebellum/amygdala in MS-patients compared to controls was correlated with better cToM performance30, as well as positive and negative correlations between different subscales of a cToM picture sequencing task and functional connectivity of the right middle temporal and (posterior) cingulate cortex46.
Four imaging studies provided information on depression, fatigue and cognition, with three studies investigating aToM26,40,45, and two cToM22,45, but used different measures to quantify depression, fatigue and cognition, that complicate meaningful comparison of the results.
Discussion
The present systematic review and meta-analysis confirms previous reports demonstrating socio-cognitive impairment in patients with MS9,9,11 and suggests that comorbid cognitive and affective symptoms or fatigue can further exacerbate these impairments. The vast majority of eligible studies investigated different aspects of ToM and approximately 80% of the included studies reported impairment of either affective or cognitive ToM in MS patients relative to healthy control groups. Our meta-analyses demonstrated more pronounced impairment for aToM (ES = 0.8) compared to cToM (ES = 0.05-0.07). This pattern is in line with results of previous meta-analyses, that also demonstrated more pronounced impairment of aToM, especially for the RMET and facial emotion recognition tasks, compared to cToM (i.e., faux-pas tasks)9,11. While only 4/58 eligible studies investigated different aspects of social cognition in MS (VPT/SDM), all of them reported significant impairment compared to healthy control groups. This highlights the need to further investigate other socio-cognitive processes than ToM in MS and to determine the potential interplay with other clinical symptoms (i.e., depression, fatigue or cognitive status). This was not possible in the present study, due to the small number of available studies.
Eighteen of the included studies provided additional information on clinical symptoms that may impact on socio-cognitive impairment, but only three studies controlled for these variables in their analyses17,27,28. Nonetheless, the overall pattern of results from individual studies suggests that depression, fatigue and cognitive impairment can contribute to socio-cognitive impairment in MS. This was further supported by the results of our meta-regression analyses that demonstrated a specific contribution of fatigue to the degree of impairment in cToM, but not aToM. However, future research is needed, to systematically investigate whether specific clinical symptoms exacerbate the degree of impairment in different aspects of socio-cognitive functioning and to determine causal relationships between them.
It needs to be acknowledged that the results of this study are based on a relatively small number of studies and are therefore to be interpreted with caution. Nonetheless, our study included about 30% more studies compared to the most recent previous meta-analysis by Lin et al.11. Two earlier meta-analyses published in 2016 included only about half the number of studies9,10, which highlights an emerging interest in this topic. This not unsurprising, because intact social functioning has been linked to relationship and vocational success, and better life satisfaction in healthy individuals49. Moreover, socio-cognitive impairment can have a profound negative impact on social participation, resulting in loneliness and poor mental health50, which may be particularly detrimental in individuals attempting to cope with progressive conditions like MS. Nonetheless, the direct contribution of socio-cognitive impairment to reduced quality-of-life (QoL) in MS is currently unclear. For example, while Philips et al.51 demonstrated that emotion regulation capacity was positively correlated with higher QoL in MS patients, others failed to demonstrate independent contributions of socio-cognitive impairment to QoL (e.g.52). Such discrepancies are likely explained by mutual interdependencies of both social cognition and QoL with clinical symptoms that are frequent in MS53. However, only about ~ 30% of our included studies reported information on specific socio-cognitive outcomes and (substantially varying degrees of) cognition, fatigue and depression. Only three studies controlled for these symptoms in their analyses, none reported associations with QoL. Thus, future systematic research is needed to disentangle the complex interactions between socio-cognitive impairment and cognition, fatigue and depression, and how they affect real-life outcomes, including QoL or the ability to cope with disease progression.
Finally, the systematic review of the anatomical and functional brain correlates underlying socio-cognitive impairment in MS revealed substantial heterogeneity between studies with regard to characteristics of the included patients, imaging methods, and outcome measures. As for the behavioral studies described above, the majority of imaging studies focused on different aspects of ToM (cTOM: 9 studies, aTOM: 13 studies). With regard to imaging methods, twelve studies used structural imaging and investigated global or regional grey and white matter changes. Only five studies employed functional MRI. Despite partially conflicting findings, these studies demonstrated that lesions affecting major cortical or subcortical hubs (e.g., orbito-frontal or insular cortex, the amgydala) within task-relevant regions of the “social brain”54 or domain-general networks (e.g., ventral/dorsal attention, salience or default networks) can be related to the degree of specific socio-cognitive impairment. Similarly, several studies demonstrated the contribution of white matter pathways (e.g., corpus callosum, uncinate fasciculus, superior longitudinal fasciculus) or functional connectivity changes in specific networks to socio-cognitive impairment. However, aside from the general heterogeneity (including paradigms, methods for data acquisition and analyses, patient characteristics, etc.), the interpretation of neural findings in the included studies is often further complicated because the observed local or network level findings partially overlap with those reported in the much more extensive literature on neural underpinnings of cognition, depression and fatigue in MS3,55. Moreover, only four imaging studies provided additional information about these potentially conflicting variables, which were also not directly related to the imaging results. Therefore, results of individual studies need to be interpreted with caution.
In sum, the present study demonstrates substantial impairment of socio-cognitive processes in MS and highlights the potential mediating role of comorbid clinical symptoms. We identify several current evidence gaps and larger scale studies using comprehensive and coordinated assessments of socio-cognitive parameters (e.g., similar to current efforts for establishing core outcome parameters for clinical trials, https://www.comet-initiative.org/), potential mediators and neural correlates are urgently needed.
Methods
The present systematic review and meta-analysis followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline16. The pre-registered review protocol can be assessed at www.crd.york.ac.uk/PROSPERO/ (ID: CRD42020206225).
Systematic search, study selection and eligibility criteria
A systematic electronic search was conducted in MEDLINE Ovid, Web of Science Core Collection, CENTRAL, and PsycInfo up to 31st August 2020 with the following keywords: multiple sclerosis, theory of mind, mind reading, social cognition, social cognitive deficits, emotional expression, facial emotion, empathy, social decision making. An update search was conducted on the 15th December 2022. Our search string for MEDLINE Ovid is provided as an example in Supplementary Table 1.
Three review authors (MR, LG, LH) screened all obtained titles and abstracts according to pre-defined criteria using the Covidence Software (https://www.covidence.org/). Full-texts were again screened for studies meeting the inclusion criteria. Disagreements between the reviewers were solved by discussion.
We included studies that investigated social cognition in male and female patients ≥ 18 years old with multiple sclerosis diagnosis (all diagnostic types) compared to a healthy control group. We defined ToM as our primary outcome, because ToM is a key aspect of social cognition, adequate ToM performance is critical for establishing proper social interaction and also relevant for coping with chronic conditions such as MS56. ToM is defined as the ability to attribute mental states to others or the ability to understand and predict others’ behaviour based on their mental states and is the most frequently studied socio-cognitive process across development and in healthy and pathological aging. Please note, separate meta-analyses were calculated for cToM and aToM to reduce heterogeneity and because both are supported by partially different neural networks57. Secondary outcomes were chosen to represent two additional major socio-cognitive domains: social perception (recognizing others as “living persons” via the analysis of perceptual information including e.g. visual perspective taking), and social decision-making (using the obtained social information for social decision making)15. All socio-cognitive outcomes needed to be tested with standardized tests to be included in our review. If more than one assessment was conducted, only the first timepoint was considered. Studies specifically assessing empathy were not considered because of the highly heterogeneous nature of this concept (e.g., different aspects of empathy are associated with different neural networks) and overlap with emotion processing and ToM58.
Data extraction
Three review authors [MR, LG, LH] extracted the data using a study specific, standardized data extraction sheet. Disagreements were discussed with all authors until consensus was reached. We contacted n = 13 authors for missing data. Only four replies were received, two authors provided data1,59.
Quality assessment
We assessed risk of bias (RoB) for each included study using the first six signaling questions of the “Tool for Assessing Risk of Bias in Cohort Studies” by the CLARITY Group60. Signaling questions can either be answered with “definitely yes” (low RoB), “probably yes”, “probably no”, “definitely no” (high RoB). Note, that three signaling questions were not applicable to our research question and studies. Two review authors (LG, LH) individually assessed RoB for each study. If no consensus could be reached, a third author (MR) was involved.
Meta-analyses
We conducted random-effects pairwise meta-analyses to investigate the degree of SC impairment in patients with MS relative to healthy controls. Data was clustered according to our four outcomes aToM, cToM, SCD and VPT. For each outcome, we also clustered studies according to the tests that were used for assessments (e.g., aToM: Baron-Cohen’s Adult Eyes Test, Emotion Recognition Florida Affective Battery, and the Facial Expression of Emotion Test, FEEST). Meta-analyses were only calculated if n ≥ 3 studies were available.
Data analysis was conducted using R. For all analyses, the alpha level was set at 0.05. Standardized mean differences (SMD) were used as effect sizes, because constructs (e.g., ToM) were assessed with different tests. The mean score of the dependent variable, the mean standard deviation, and the number of included participants in each group were used to calculate SMD.
To address heterogeneity, we used the I2 statistic. As recommended in the Cochrane Handbook for systematic reviews of interventions61, heterogeneity was interpreted as: 0–40%: not important/low heterogeneity; 30–60%: moderate heterogeneity; 50–90%: substantial heterogeneity; 75–100%: considerable heterogeneity. A funnel plot for identifying possible publication bias was calculated in analyses including ≥ 10 studies. Sensitivity analysis were calculated using fixed effect models to control for small-study effects. If the effect estimates of both, the fixed and random effects model are similar, then any small-study effects have little effect on the effect estimate.
To further assess the impact of cognitive status, depressive symptoms, and fatigue on socio-cognitive abilities in patients with MS, meta-regression analyses were conducted using aToM and cToM as outcome variables and cognitive scores (measured via the neuropsychological test that was most frequently reported in the included studies) and depressive symptoms and fatigue (both measured with standardized questionnaires) as possible predictors. Meta-regressions on SDM and VPT could not be conducted as there was not enough data reported in the studies (Note: this analysis requires correlations between the investigated outcome variable and all possible predictors that are included in the model).
Data availability
All data generated or analyzed in this study are included in the published article [and its supplementary information files]. Aggregated data can be shared by the corresponding author on reasonable request.
Code availability
Code can be shared by the corresponding author on reasonable request.
References
Thompson, A. J., Baranzini, S. E., Geurts, J., Hemmer, B. & Ciccarelli, O. Multiple sclerosis. Lancet 391(10130), 1622–1636. https://doi.org/10.1016/s0140-6736(18)30481-1 (2018).
Benedict, R. H. B., Amato, M. P., DeLuca, J. & Geurts, J. J. G. Cognitive impairment in multiple sclerosis: clinical management, MRI, and therapeutic avenues. Lancet Neurol. 19(10), 860–871. https://doi.org/10.1016/S1474-4422(20)30277-5 (2020).
Penner, I.-K. & Paul, F. Fatigue as a symptom or comorbidity of neurological diseases. Nat. Rev. Neurol. 13, 662–675 (2017).
Patten, S. B. et al. Major depression in multiple sclerosis: A population-based perspective. Neurology 61, 1524–1527 (2003).
Brüne, M. & Brüne-Cohrs, U. Theory of mind–evolution, ontogeny, brain mechanisms and psychopathology. Neurosci. Biobehav. Rev. 30, 437–455 (2006).
Berneiser, J. et al. Impaired recognition of emotional facial expressions in patients with multiple sclerosis. Mult. Scler. Relat. Disord. 3, 482–488 (2014).
Banati, M. et al. Social cognition and Theory of Mind in patients with relapsing-remitting multiple sclerosis. Eur. J. Neurol. 17, 426–433 (2010).
Benedict, R. H. B. et al. Cognitive impairment in multiple sclerosis: Clinical management, MRI, and therapeutic avenues. Lancet Neurol. 19, 860–871 (2020).
Cotter, J. et al. Social cognition in multiple sclerosis: A systematic review and meta-analysis. Neurology 87, 1727–1736 (2016).
Bora, E. et al. Social cognition in multiple sclerosis: A meta-analysis. Neuropsychol. Rev. 26, 160–172 (2016).
Lin, X. et al. Social cognition in multiple sclerosis and its subtypes: A meta-analysis. Mult. Scler. Relat. Disord. 52, 102973 (2021).
Penner, I.-K. Evaluation of cognition and fatigue in multiple sclerosis: daily practice and future directions. Acta Neurol. Scand. 134(Suppl 200), 19–23 (2016).
Palotai, M. & Guttmann, C. R. Brain anatomical correlates of fatigue in multiple sclerosis. Mult. Scler. 26, 751–764 (2020).
Masuccio, F. G. et al. Imaging and depression in multiple sclerosis: A historical perspective. Neurol. Sci. 42, 835–845 (2021).
Arioli, M., Crespi, C. & Canessa, N. Social cognition through the lens of cognitive and clinical neuroscience. Biomed. Res. Int. 2018, 4283427 (2018).
Moher, D. et al. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 339, b2535 (2009).
Henry, A. et al. Social cognition and executive functioning in multiple sclerosis: A cluster-analytic approach. J. Neuropsychol. 16, 97–115 (2022).
Weinstein, K. M., Patterson & Stephen, M. R. Hemispheric Asymmetries and Processing of Affective Stimuli: Contribution of Callosal Communication (1996).
Harbo, H. F., Gold, R. & Tintoré, M. Sex and gender issues in multiple sclerosis. Ther. Adv. Neurol. Disord. 6, 237–248 (2013).
Prochnow, D. et al. Alexithymia and impaired facial affect recognition in multiple sclerosis. J. Neurol. 258, 1683–1688 (2011).
Gleichgerrcht, E., Tomashitis, B. & Sinay, V. The relationship between alexithymia, empathy and moral judgment in patients with multiple sclerosis. Eur. J. Neurol. 22, 1295–1303 (2015).
Czekóová, K. et al. Impaired self-other distinction and subcortical gray-matter alterations characterize socio-cognitive disturbances in multiple sclerosis. Front. Neurol. 10, 525 (2019).
Bruno, D., Galiani, A., Golfeder, M., et al. Perspective taking deficits and their relationship with theory of mind abilities in patients with relapsing-remitting multiple sclerosis (RRMS). Appl. Neuropsychol. Adult 1–11 (2022).
Ehrlé, N. et al. Social norms in patients with relapsing-remitting multiple sclerosis: Impairment of the moral/conventional distinction?. Soc. Neurosci. 15, 630–640 (2020).
Henry, A. et al. Facial emotion recognition and Faux Pas interpretation in multiple sclerosis. Brain Impairment 16, 158–172 (2015).
Koubiyr, I. et al. Amygdala network reorganization mediates the theory of mind performances in multiple sclerosis. J. Neurosc.i Res. 100, 537–550 (2022).
Henry, A. et al. Social cognition abilities in patients with different multiple sclerosis subtypes. J. Int. Neuropsychol. Soc. 23, 653–664 (2017).
Batista, S. et al. Theory of mind and executive functions are dissociated in multiple sclerosis. Arch. Clin. Neuropsychol. 33, 541–551 (2018).
Goitia, B. et al. The relationship between executive functions and fluid intelligence in multiple sclerosis. PLoS One 15, e0231868 (2020).
Labbe, T. P. et al. Social cognition in Multiple Sclerosis is associated to changes in brain connectivity: A resting-state fMRI study. Mult. Scler. Relat. Disord. 45, 102333 (2020).
Yap, S. M., Davenport, L., Cogley, C., et al. Word finding, prosody and social cognition in multiple sclerosis. J. Neuropsychol. (2022).
Cecchetto, C. et al. Facial and bodily emotion recognition in multiple sclerosis: The role of alexithymia and other characteristics of the disease. J. Int. Neuropsychol. Soc. 20, 1004–1014 (2014).
Pfaff, L. et al. Emotional experience is increased and emotion recognition decreased in multiple sclerosis. Sci. Rep. 11, 21885 (2021).
Montembeault, M. et al. Multimodal emotion perception in young and elderly patients with multiple sclerosis. Mult. Scler. Relat. Disord. 58, 103478 (2022).
Baron-Cohen, S., O’Riordan, M., Jones, R., et al. A New Test of Social Sensitivity: Detection of Faux Pas in Normal Children and Children with Asperger Syndrome (1999).
Stone, V. E., Baron-Cohen, S. & Knight, R. T. Frontal lobe contributions to theory of mind. J. Cogn. Neurosci. 10, 640–656 (1998).
Henry, A. et al. Social cognition impairments in relapsing-remitting multiple sclerosis. J. Int. Neuropsychol. Soc. 17, 1122–1131 (2011).
Ouellet, J. et al. Assessment of social cognition in patients with multiple sclerosis. J. Int. Neuropsychol. Soc. 16, 287–296 (2010).
Kraemer, M. et al. Theory of mind and empathy in patients at an early stage of relapsing remitting multiple sclerosis. Clin. Neurol. Neurosurg. 115, 1016–1022 (2013).
Golde, S. et al. Distinct functional connectivity signatures of impaired social cognition in multiple sclerosis. Front. Neurol. 11, 507 (2020).
Batista, S. et al. Disconnection as a mechanism for social cognition impairment in multiple sclerosis. Neurology 89, 38–45 (2017).
Adamaszek, M. et al. Clinical and neurophysiological patterns of impairments to emotion attention and empathy in multiple sclerosis. J. Integr. Neurosci. 21, 7 (2022).
Batista, S. et al. Impairment of social cognition in multiple sclerosis: Amygdala atrophy is the main predictor. Mult. Scler. 23, 1358–1366 (2017).
Mike, A. et al. Disconnection mechanism and regional cortical atrophy contribute to impaired processing of facial expressions and theory of mind in multiple sclerosis: A structural MRI study. PLoS One 8, e82422 (2013).
Labbe, T. P. et al. Regional brain atrophy is related to social cognition impairment in multiple sclerosis. Arq. Neuropsiquiatr. 79, 666–675 (2021).
Bisecco, A. et al. Resting-state functional correlates of social cognition in multiple sclerosis: An explorative study. Front. Behav. Neurosci. 13, 276 (2019).
Yokote, H., Okano, K. & Toru, S. Theory of mind and its neuroanatomical correlates in people with multiple sclerosis. Mult. Scler. Relat. Disord. 55, 103156 (2021).
Isernia, S. et al. Theory of mind network in multiple sclerosis: A double disconnection mechanism. Soc. Neurosci. 15, 544–557 (2020).
Amdurer, E. et al. Long term impact of emotional, social and cognitive intelligence competencies and GMAT on career and life satisfaction and career success. Front. Psychol. 5, 1447 (2014).
Eramudugolla, R. et al. Social cognition and social functioning in MCI and dementia in an epidemiological sample. J. Int. Neuropsychol. Soc. 28, 661–672 (2022).
Phillips, L. H. et al. Difficulties with emotion regulation in multiple sclerosis: Links to executive function, mood, and quality of life. J. Clin. Exp. Neuropsychol. 36, 831–842 (2014).
Grothe, M. et al. Testing social cognition in multiple sclerosis: Difference between emotion recognition and theory of mind and its influence on quality of life. Brain Behav. 11, e01925 (2021).
Fernández, O. et al. Patient characteristics and determinants of quality of life in an international population with multiple sclerosis: Assessment using the MusiQoL and SF-36 questionnaires. Mult. Scler. 17, 1238–1249 (2011).
Frith, C. D. The social brain?. Philos. Trans. R. Soc. Lond. B Biol. Sci. 362, 671–678 (2007).
Sumowski, J. F. et al. Cognition in multiple sclerosis: State of the field and priorities for the future. Neurology 90, 278–288 (2018).
Chalah, M. A. et al. Theory of mind in multiple sclerosis: A neuropsychological and MRI study. Neurosci. Lett. 658, 108–113 (2017).
Molenberghs, P. et al. Understanding the minds of others: A neuroimaging meta-analysis. Neurosci. Biobehav. Rev. 65, 276–291 (2016).
Walter, H. Social cognitive neuroscience of empathy: Concepts, circuits, and genes. Emotion Rev. 4, 9–17 (2012).
Pitteri, M. et al. Social cognition deficits and the role of amygdala in relapsing remitting multiple sclerosis patients without cognitive impairment. Mult. Scler. Relat. Disord. 29, 118–123 (2019).
Higgins, J. P. T. & Green, S. (eds) Cochrane Handbook of Systematic Reviews of Interventions 1st edn. (Wiley, 2008).
Higgins, J., Thomas, J., Chandler, J. et al. (eds) Cochrane Handbook for Systematic Reviews of Interventions 2nd edn. (Wiley, 2019).
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
M.R., M.G., and M.M. were responsible for study conception and design. L.G., L.H. and M.R. did the systematic search and screening, M.R. is responsible for data analysis, M.R., M.R. and M.M. are responsible for interpretation of the results and drafting of the manuscript. All authors reviewed the results and read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
MG is author of one of the included studies, however, he was not involved in the data extraction and quality rating of this study. Other than that, the authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Roheger, M., Grothe, L., Hasselberg, L. et al. A systematic review and meta-analysis of socio-cognitive impairments in multiple sclerosis. Sci Rep 14, 7096 (2024). https://doi.org/10.1038/s41598-024-53750-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-53750-5
Keywords
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
