
Abstract
Reports indicate that Plasmodium infections influence methemoglobin levels. However, findings have been inconclusive or have varied across different geographic and demographic contexts. This systematic review and meta-analysis aimed to consolidate existing data regarding the association between Plasmodium infections and alterations in methemoglobin levels related to the severity of the infection. A comprehensive literature search of several databases, including Ovid, ProQuest, Embase, Scopus, MEDLINE, and PubMed, was conducted to identify relevant studies that examined methemoglobin levels in patients with malaria. Qualitative synthesis and meta-analysis of the pooled standardized mean difference were conducted to synthesize the differences in methemoglobin levels between: (1) patients with malaria and those without malaria and (2) patients with severe malaria and those with uncomplicated malaria based on various themes including publication year, study design, study area, Plasmodium species, age group, symptomatic status, severity status, and method of malaria detection. Of the 1846 studies that were initially identified from the main databases and additional searches on Google Scholar, 10 studies met the eligibility criteria and were selected for this review. The systematic review distinctly highlighted an association between malaria and elevated methemoglobin levels, an observation consistent across diverse geographical regions and various Plasmodium species. Furthermore, the meta-analysis confirmed this by demonstrating increased methemoglobin levels in patients with malaria compared to those without malaria (P < 0.001, Hedges’ g 2.32, 95% CI 1.36–3.29, I2 97.27, 8 studies). Moreover, the meta-analysis found elevated methemoglobin levels in patients with severe malaria compared to those with uncomplicated malaria (P < 0.001, Hedges’ g 2.20, 95% CI 0.82–3.58, I2 96.20, 5 studies). This systematic review and meta-analysis revealed increased methemoglobin levels in patients with P. falciparum and P. vivax infections, with a notable association between elevated methemoglobin levels and severe malaria. Future research should focus on elucidating the specific mechanisms by which changes in methemoglobin levels are related to infections by P. falciparum and P. vivax, particularly in terms of severity, and how these alterations could potentially impact patient management and treatment outcomes.
Similar content being viewed by others


Introduction
Malaria, a mosquito-borne infectious disease, remains one of the most prevalent and deadly illnesses worldwide1. It is caused by protozoan parasites belonging to the genus Plasmodium which are transmitted through the bite of female Anopheles mosquitoes2. Among the several species of this genus, five are well known to infect humans: Plasmodium falciparum (P. falciparum), Plasmodium vivax (P. vivax), Plasmodium ovale (P. ovale) (with two distinct species: P. o. curtisi and P. o. wallikeri), Plasmodium malariae (P. malariae), and Plasmodium knowlesi (P. knowlesi)3,4. In addition to those main species, Plasmodium cynomolgi (P. cynomolgi), Plasmodium inui (P. inui), and other simian malaria parasites can naturally infect humans5,6. The spread and prevalence of malaria varies considerably across global regions, with sub-Saharan Africa being disproportionately affected1. Malaria can infect individuals of all age groups, including children and adolescents7,8, adults9,10, and pregnant women11,12. Despite concerted efforts to control and eliminate this disease, malaria still results in significant morbidity and mortality, especially in vulnerable populations like children under 5 years1,13,14.
Methemoglobin is an oxidized form of hemoglobin containing iron in the ferric [Fe3+] form in red blood cells15. Under normal physiological conditions, methemoglobin levels are low (< 1%) because of the action of the enzyme cytochrome-b5 reductase16. However, methemoglobin levels can rise when these mechanisms are overwhelmed or compromised, resulting in a condition known as methemoglobinemia15. Elevated methemoglobin levels can reduce the oxygen-carrying capacity of the blood, leading to a range of clinical symptoms, from cyanosis to more severe respiratory and cardiovascular complications17,18.
Studies have indicated a potential association between malaria infection and increased methemoglobin levels19,20. In particular, there might be a heightened risk of methemoglobinemia in severe malaria cases, where intravascular hemolysis is common21. The increase in methemoglobinemia has been associated with the severity and fatality of malaria in infected patients22. Intravascular hemolysis produces methemoglobin products, with elevated levels in patients who either died or survived with neurological sequelae23. Understanding this association is crucial, as it could influence clinical outcomes and management strategies for malaria patients. Although some studies have explored the association between malaria and methemoglobin, findings have often been inconclusive or have varied across different geographical and demographic settings19,20,22. This systematic review and meta-analysis aimed to synthesize existing data to provide a more comprehensive and cohesive understanding of the association between malaria infections and severity-related alterations in methemoglobin levels. This study aims to shed light on potential diagnostic, prognostic, and therapeutic implications in malaria management.
Methods
Protocol and registration
The protocol of the systematic review and meta-analysis followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines24. The protocol was registered at PROSPERO (registration number: CRD42023468210).
Systematic review question
The systematic review questions were developed using the Population, Exposure, Comparator, Outcome (PECO) framework25. The primary question was, “In patients with malaria (P), how does the presence of Plasmodium infection (E), compared to those without the infection (C), affect the methemoglobin levels (O)?” The secondary question was, “How does the methemoglobin level vary in severe malaria compared to those with uncomplicated malaria?”.
Search strategy
Several databases, including Ovid, ProQuest, Embase, Scopus, MEDLINE, and PubMed, were comprehensively searched to identify relevant studies that evaluated methemoglobin levels in patients with malaria. The general search strategy used for querying the databases was “Methemoglobin AND “(‘malaria’ OR ‘plasmodium’ OR ‘Plasmodium Infection’ OR ‘Remittent Fever’ OR ‘Marsh Fever’ OR ‘Paludism’).” The specific search strategies were used for individual databases (Table S1). In addition to the main databases, a search on Google Scholar were conducted to identify any additional records that were not indexed in the main databases. Only the first 200 articles from Google Scholar were screened to identify potentially relevant studies, as suggested previously26. Moreover, reference lists of included studies were reviewed to ensure that no relevant studies were missed. The searches were conducted from inception to September 29, 2023. The searches were not limited to publication year or the language of articles.
Selection criteria
Studies were selected based on specific inclusion and exclusion criteria. Human studies that evaluated methemoglobin levels in patients with malaria and those that reported on methemoglobin levels either in patients with severe or uncomplicated malaria or provided a comparison group were included. In vitro studies, animal studies, and studies that lacked specific information on methemoglobin in malaria or only concerned methemoglobin levels after treatment were excluded. Reviews, assay developments, computational models, case reports or series, meta-analyses, conference abstracts, and studies with nonextractable data or that merely presented methemoglobin in malaria without a comparison group were also excluded.
Study selection and data extraction
Duplicate records were removed before screening, and the remaining records were screened for eligibility based on the inclusion and exclusion criteria. Full-text articles of potentially relevant studies were retrieved and assessed for final inclusion. Data was extracted from the included studies regarding the publication year, study design, study location, Plasmodium species, age range of participants, clinical presentation of malaria, severity status, method for measuring methemoglobin, and Plasmodium detection. Furthermore, methemoglobin levels in different groups of patients with malaria were extracted. Study selection and data extraction were performed independently by two reviewers (KUK, MK); a third reviewer (AM) resolved disagreements.
Quality assessment
A critical appraisal of studies included in this study was carried out using the Joanna Briggs Institute (JBI) checklist, which was specific for each study design. This ensured methodological quality of the selected studies in this review27. For cross-sectional studies, the JBI checklist emphasizes clear inclusion criteria, detailed descriptions of study subjects and settings, valid exposure and outcome measurements, and appropriate handling of confounding factors and statistical analysis. Cohort studies should have comparable groups, ensure participants are free from the outcome at the start, and implement reliable outcome measurements with suitable statistical handling. For case–control studies, the guidelines emphasize the importance of having comparable groups, consistent criteria for case and control identification, and accounting for confounding factors. Quasi-experimental studies should provide a distinct cause-and-effect relationship, have mechanisms to control confounders, ensure blinded outcome assessments, and employ appropriate statistical techniques. Each item or question on the checklist can be answered with “Yes,” “No,” “Unclear,” or “Not Applicable.” Two reviewers (KUK, MK) conducted the quality assessment independently; disagreements were resolved through discussion.
Data syntheses and statistical analysis
Qualitative synthesis28 was performed to evaluate the difference in methemoglobin levels between patients with malaria and those without malaria. Furthermore, methemoglobin levels were compared between those with severe malaria and those with uncomplicated malaria. The aforementioned comparison was based on independent covariates, including publication year, study design, study area, Plasmodium species, age group, symptomatic status, severity status, and method of malaria detection. For the meta-analysis, the primary outcome of interest was the pooled standardized mean difference in methemoglobin levels between patients with malaria and those without malaria and between patients with severe malaria and those with uncomplicated malaria. Hedges’ g and its 95% confidence interval (CI) represented the pooled effect estimate. The heterogeneity among studies was quantified using the I2 statistic, wherein I2 values > 50% indicated significant heterogeneity29. In cases of significant heterogeneity, meta-regression analysis was conducted to identify potential sources of heterogeneity; furthermore, this analysis was conducted if at least 6 to 10 studies were selected for the meta-analysis30. Subgroup analyses were conducted based on predefined criteria, such as publication year, study design, study location, Plasmodium species, age group, symptomatic status, severity status, and method of Plasmodium identification. A sensitivity analysis was conducted using the leave-one-out method to evaluate the stability and reliability of the findings from a meta-analysis by assessing the influence of individual studies on the overall results31. All analyses were performed using the Stata v17.0 software (StataCorp, College Station, TX). A P-value < 0.05 was considered as statistically significant.
Results
Search results
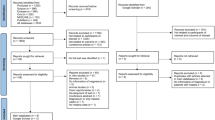
Of the total 1846 studies identified from databases, including Ovid (n = 783), ProQuest (n = 512), Embase (n = 197), Scopus (n = 173), MEDLINE (n = 92), and PubMed (n = 89), 448 duplicate records were removed prior to screening, and 1398 records were screened. Of these, 1308 were excluded for being unrelated to the participants of interest (n = 481) or the outcome of interest (n = 827). The remaining 90 reports were assessed for eligibility. Of these 90 reports, 84 were excluded for being in vitro studies (n = 28), lacking information on methemoglobin in malaria (n = 15), being animal studies (n = 14), assessing methemoglobin levels after treatment (n = 8), and for several other specific reasons such as being reviews, assay developments, computational models, case reports or series, meta-analyses, conference abstracts, or having data that were not extractable or only featured methemoglobin in malaria without a comparison group., Google Scholar provided four studies in addition to the main databases. Eventually, 10 studies were included in this review19,20,22,23,32,33,34,35,36,37 (Fig. 1).

Study flow diagram.
Characteristics of included studies
Of the 10 studies selected for the review, 2 (20%) were published before 200023,33, 1(10%) was published between 2000 and 200936, 6 (60%) were published between 2010 and 201919,20,22,32,34,37, and 1 (10%) was published between 2020 and 202335. Regarding study designs, 2 (20%) were cross-sectional studies23,37, 4 (40%) were case–control studies22,33,34,36, 3 (30%) were cohort studies19,20,35, and 1 (10%) was a quasi-experimental study32. Four studies (40%) were conducted in Asia19,22,33,35, with 2 (20%) in India19,35, 1 (10%) in Indonesia22, and 1 (10%) in Turkey33. Six (60%) originated from Africa20,23,32,34,36,37, including 4 (40%) from Nigeria32,34,36,37, 1 (10%) from Gabon20, and 1(10%) from Tanzania23. P. falciparum and P. vivax were the primary Plasmodium species investigated. Specifically, 6 studies (60%) focused on P. falciparum20,22,23,35,36,37 and 1 study (10%) focused on P. vivax33; the remaining 3 studies (30%) did not specify the Plasmodium species19,32,34. Three studies (30%) involved children20,23,36, 5 (50%) involved adults22,32,33,35,37, and 2 (20%) did not specify the age group19,34. Eight (80%) studies, a majority, enrolled patients with symptomatic malaria19,20,22,23,33,34,35,36, 1 (10%) enrolled a patient with asymptomatic malaria37, and 1 (10%) did not specify the symptomatic status of the patient. Two studies (20%) enrolled patients with severe malaria33,36; 4 (40%) enrolled patients with both severe and uncomplicated malaria19,20,34,35; 1 (10%) was focused on severe and moderately severe malaria22; 1 (10%) enrolled patients with severe, uncomplicated, and asymptomatic malaria23; 1 (10%) enrolled patients with asymptomatic malaria alone37; and 1 (10%) did not specify the severity status of patients32. Six studies (60%) used the microscopic method for malaria detection20,23,33,34,36,37; 2 (20%) used a combination of the microscopic method, quantitative buffy coat, and the rapid diagnostic test (RDT)19,35; 1 (10%) combined the microscopic method with RDT22, and 1 (10%) did not specify the method of malaria detection32 (Table 1, Table S2).
Quality of included studies
For analytical cross-sectional studies, one met all criteria23, while another had uncertainties about confounding factors37. In case–control studies, 333,34,36 had issues regarding confounding factors, while one met all criteria22. In cohort studies, 3 had unclear follow-up and confounding factor issues19,20,35. The quasi-experimental study was clear on cause–effect relationships and had consistent outcome measurements but unclear follow-up completeness32 (Table S3).
Thematic synthesis for methemoglobin levels in malaria
Methemoglobin levels in different groups of patients with malaria are shown in Table 2. Based on geographical overview, studies in Africa, such as in Tanzania23, Nigeria32,34,36,37, and Gabon20, consistently showed an increase in methemoglobin levels in malaria patients. Similarly, studies in Asia, such as in India19,35, Turkey33, and Indonesia22, also indicated elevated methemoglobin levels in those with malaria. Based on Plasmodium species, Anstey et al. reported elevated methemoglobin levels in cases of severe, uncomplicated, and cerebral malaria caused by P. falciparum in Tanzanian children23. In Gabon, Hänscheid et al. reported increased methemoglobin levels in children suffering from severe and uncomplicated P. falciparum malaria20. Yeo et al. from Indonesia found increased methemoglobin levels proportional to malaria disease severity caused by P. falciparum in adults22. They also observed no direct correlation between methemoglobin levels and the degree of parasitemia. In Nigeria, Zama et al. and Uko et al. reported that P. falciparum infections in adults and children, respectively, were associated with significantly higher methemoglobin levels compared to uninfected controls36,37. Both studies also found a direct correlation between methemoglobin levels and the degree of parasitemia. A study from Turkey by Erel et al. focusing on adult cases of severe malaria caused by P. vivax revealed that methemoglobin levels were significantly elevated in patients compared to uninfected controls33.
Based on clinical presentation, higher methemoglobin levels were noted in those with symptomatic and asymptomatic malaria than in uninfected controls, as observed in 2 studies23,37. Furthermore, several studies20,23,34,35 revealed that methemoglobin levels were significantly elevated in severe malaria cases compared to uncomplicated malaria cases. Based on age group dynamics, studies that enrolled children20,23,36 and adults22,32,33 found consistently elevated methemoglobin levels in malaria cases. For parasitemia correlation, 3 studies19,36,37 observed a direct correlation between methemoglobin levels and the degree of parasitemia. However, a study by Yeo et al. from Indonesia found no such association22.
Methemoglobin levels between patients with malaria and without malaria
The difference in methemoglobin levels between patients with malaria and those without malaria was estimated using the data from 8 studies19,20,22,32,33,34,35,36. The results demonstrated increased methemoglobin levels in patients with malaria compared to those without malaria (P < 0.001, Hedges’ g 2.32, 95% CI 1.36–3.29, I2 97.27, 8 studies, Fig. 2). Because the results were heterogeneous, meta-regression analysis was conducted to identify factors that affected the pooled effect estimate. The results revealed that only the country significantly affected the pooled effect estimate (P < 0.001, R2 = 51.47, Table S4).

The difference in methemoglobin levels between patients with and without malaria. Blue box effect estimate, green diamond pooled effect estimate, N number of participants, Mean mean methemoglobin level, SD standard deviation, CI confidence interval.
Subgroup analyses evaluated the difference in methemoglobin levels between patients with and without malaria. Notably, studies published between 2010 and 2019 showed a significant increase in methemoglobin levels in patients with malaria (P < 0.01)19,20,22,32. Regarding study design, the case–control and cohort studies revealed a significant rise in methemoglobin levels for patients with malaria (P < 0.01)19,20,22,33,34,35,36. Geographically, studies from Asia and Africa demonstrated significantly elevated methemoglobin levels in patients with malaria (P < 0.01)19,20,22,32,33,34,35,36. When analyzed by age group, a significant increase in methemoglobin levels was observed among studies that enrolled adults with malaria (P < 0.01)22,32,33,35 but not in those that enrolled children (P = 0.13)20,36.
Subgroup analysis based on the Plasmodium species revealed significantly elevated methemoglobin levels in patients with P. falciparum malaria compared to those without infection (P < 0.01). Furthermore, in terms of clinical presentation, patients with symptomatic malaria demonstrated significantly higher methemoglobin levels than the uninfected controls (P < 0.01). When considering methods of Plasmodium identification, using the microscopic method, either alone or combined with quantitative buffy coat and RDT, showed a significant rise in methemoglobin levels among malaria patients (P < 0.01) (Table 3).
Methemoglobin levels between patients with severe malaria and uncomplicated malaria
The difference in methemoglobin levels between patients with severe malaria and those with uncomplicated malaria was evaluated using data from 5 studies19,20,22,34,35. The results revealed elevated methemoglobin levels in patients with severe malaria compared to those with uncomplicated malaria (P < 0.001, Hedges’ g 2.20, 95% CI 0.82–3.58, I2 96.20, 5 studies, Fig. 3). Meta-regression and subgroup analyses were not performed because of the limited number of studies in the meta-analysis.

The difference in methemoglobin levels between patients with severe malaria and those with uncomplicated malaria. Blue box effect estimate, green diamond pooled effect estimate, N number of participants, Mean mean methemoglobin level, SD standard deviation, CI confidence interval.
Sensitivity analysis
The leave-one-out meta-analysis revealed the robustness of the meta-analysis results that showed significantly increased methemoglobin levels in patients with malaria compared to those without malaria (Fig. 4) and significantly increased methemoglobin levels in patients with severe malaria compared to those with uncomplicated malaria (Fig. 5). The leave-one-out method confirmed that these significant findings remained consistent even when individual studies were excluded one by one from the analysis.

The leave-one-out meta-analysis revealed the robustness of the meta-analysis results that showed significantly increased methemoglobin levels in patients with malaria compared to those without malaria. It confirmed that these significant findings remained consistent even when individual studies were excluded one by one from the analysis. Green dot pooled effect estimate, green line confidence interval, CI confidence interval.

The leave-one-out meta-analysis revealed the robustness of the meta-analysis results that showed significantly increased methemoglobin levels in patients with severe malaria compared to those with uncomplicated malaria. It confirmed that these significant findings remained consistent even when individual studies were excluded one by one from the analysis. Green dot pooled effect estimate, green line confidence interval, CI confidence interval.
Discussion
The systematic review primarily examined the methemoglobin levels in patients with malaria. The comprehensive search across multiple databases yielded 10 studies that met the eligibility criteria19,20,22,23,32,33,34,35,36,37. The review results can be used to draw several key observations and insights. First, the geographical spread of the studies reflects the endemic regions where malaria is prevalent. Asia and Africa, regions significantly burdened by malaria, have been actively involved in research to understand the nuances of this disease, as evidenced by the studies included in the review. Most studies were published between 2010 and 201919,20,22,32,34,37, underscoring the continued research interest in this period. Regarding study designs, case–control studies made up the largest proportion. This approach is advantageous for understanding associations between disease states and potential risk factors, in this case, the methemoglobin levels.
A significant observation from qualitative synthesis was the consistent rise in methemoglobin levels in patients with malaria across diverse geographical locations, such as Tanzania, Nigeria, India, Turkey, and Indonesia. This uniformity suggests a strong biological link between malaria infection and elevated methemoglobin levels. Furthermore, when the focus was narrowed down to specific Plasmodium species, such as P. falciparum, the observation remained consistent, with increased methemoglobin levels reported in most of the studies. Clinically, according to the data from the included studies, there is insufficient evidence to determine whether higher methemoglobin levels are present in both symptomatic and asymptomatic malaria compared to absent infection. Importantly, the severity of malaria also seems to influence methemoglobin levels, with those having severe malaria showing consistently higher levels compared to those with uncomplicated malaria. Furthermore, increased methemoglobin levels have been associated with increased mortality19. Elevated methemoglobin levels can reduce the blood’s oxygen-carrying capacity, leading to hypoxia and vice versa19. The subgroup analysis revealed a significant age-related variation in methemoglobin levels among patients with malaria. Specifically, studies focusing on adults with malaria showed a marked increase in methemoglobin levels, unlike those in children, where this increase was not statistically significant. This difference could be attributed to immunological variances between adults and children or to diverse levels of exposure or responses to the Plasmodium parasite38,39. Furthermore, it is plausible that differences in the metabolic pathways responsible for methemoglobin production and clearance exist between these age groups. This can be attributed to the fact that methemoglobin levels are typically higher in children than in adults, which may be because of the lower amounts of soluble cofactor cytochrome b5 and reduced activity of the cytochrome b5 reductase enzyme in their red blood cells, increasing their risk of methemoglobinemia40.
The results concerning the association of methemoglobin levels and parasitemia were mixed. Although some studies found a direct association19,36,37, one study from Indonesia did not observe such an association22. Such disparities may arise from various factors, including differences in study design, sample size, and population characteristics. Regarding study quality, while many met most of the criteria, certain aspects, such as confounding factors and follow-up completeness, remained areas of concern in some studies. This highlights the need for a more rigorous approach in future research endeavors.
The meta-analysis conclusively demonstrated a significant elevation in methemoglobin levels in patients with malaria compared to those without malaria. This observation was consistent across the reviewed studies. Sensitivity analysis further confirmed its reliability. In vitro studies have shed light on possible mechanisms: methemoglobin-driven red blood cell aggregation, coupled with the generation of reactive oxygen species (ROS) in the external microenvironment, seems pivotal in the pathophysiological effects observed during malaria41. Moreover, methemoglobin-treated endothelial cells exhibited heightened ROS levels, suggesting that methemoglobin can boost the cytoadherence of uninfected red blood cells to these cells42. This early ROS increase driven by methemoglobin contributes to the osmotic fragility and subsequent destruction of red blood cells43. Methemoglobin has been reported to mediate toxicity toward macrophages, which might lead to a weakened immune response during malaria44. In patients with malaria, increased methemoglobin levels have been observed after treatment with antimalarial drugs like primaquine45,46,47. However, in patients with normal glucose-6-phosphate dehydrogenase (G-6-PD) activity and in nonpregnant women, high doses of primaquine were not associated with elevated methemoglobin levels45,46. A decline in methemoglobin levels after treatment following the clearance of parasites was due to the partial restoration of the redox balance inside red blood cells and the consequent reduction of the methemoglobin level45.
The study has some limitations. First, the observed heterogeneity in the results could be attributed to variations in study designs, methodologies, and population demographics. Second, the limited number of studies available for certain subgroup analyses, such as the difference in methemoglobin levels between patients with severe and uncomplicated malaria, may have affected the conclusiveness of the results. Third, because of the limited number of studies, publication bias could not be assessed, potentially influencing the conclusions drawn from the meta-analysis. The systematic review accentuated the global significance of understanding the association between malaria and methemoglobin levels, especially in malaria-endemic regions. Elevated methemoglobin levels in patients with malaria, regardless of their symptomatic status, emerge as a potential biomarker, which, when correlated with severe malaria and increased mortality, underscored its clinical importance. Insights into the effects of antimalarial drugs, notably primaquine, suggested the necessity of vigilant drug administration. Furthermore, the observed pathophysiological effects highlighted possible therapeutic intervention areas. Despite the clear associations, discrepancies in some findings and inherent study limitations indicate the need for more rigorous, expansive research to solidify these observations and influence health policies in affected regions.
Conclusion
In conclusion, this systematic review and meta-analysis revealed increased methemoglobin levels in patients with P. falciparum and P. vivax infections, with a notable association between elevated methemoglobin levels and severe malaria. Future research should focus on elucidating the specific mechanisms by which changes in methemoglobin levels are related to infections by P. falciparum and P. vivax, particularly in terms of severity, and how these alterations could potentially impact patient management and treatment outcomes.
Data availability
All data relating to the present study are available in this manuscript and supplementary files.
References
White, N. J. et al. Malaria. Lancet 383(9918), 723–735 (2014).
Sato, S. Plasmodium—A brief introduction to the parasites causing human malaria and their basic biology. J. Physiol. Anthropol. 40(1), 1 (2021).
Lee, W. C. et al. Plasmodium knowlesi: The game changer for malaria eradication. Malar. J. 21(1), 140 (2022).
Joste, V. et al. Plasmodium ovale wallikeri and P. ovale curtisi infections and diagnostic approaches to imported malaria, France, 2013–2018. Emerg. Infect. Dis. 27(2), 372–384 (2021).
Yap, N. J. et al. Natural human infections with Plasmodium cynomolgi, P. inui, and 4 other simian malaria parasites, Malaysia. Emerg. Infect. Dis. 27(8), 2187–2191 (2021).
Kojom Foko, L. P., Kumar, A., Hawadak, J. & Singh, V. Plasmodium cynomolgi in humans: Current knowledge and future directions of an emerging zoonotic malaria parasite. Infection 51(3), 623–640 (2023).
Dao, F. et al. Burden of malaria in children under five and caregivers’ health-seeking behaviour for malaria-related symptoms in artisanal mining communities in Ghana. Parasit. Vectors 14(1), 418 (2021).
LendongoWombo, J. B. et al. Severe malaria in children and adolescents in Southeast Gabon. BMC Infect. Dis. 23(1), 207 (2023).
Bittaye, S. O. et al. Malaria in adults after the start of Covid-19 pandemic: An analysis of admission trends, demographics, and outcomes in a tertiary hospital in the Gambia. Malar. J. 22(1), 253 (2023).
Bittaye, S. O. et al. Clinical manifestations and outcomes of severe malaria in adult patients admitted to a tertiary hospital in the Gambia. Malar. J. 21(1), 270 (2022).
van Eijk, A. M., Hill, J., Noor, A. M., Snow, R. W. & ter Kuile, F. O. Prevalence of malaria infection in pregnant women compared with children for tracking malaria transmission in sub-Saharan Africa: A systematic review and meta-analysis. Lancet Glob. Health 3(10), e617–e628 (2015).
Chaponda, E. B. et al. High burden of malaria infection in pregnant women in a rural district of Zambia: A cross-sectional study. Malar. J. 14, 380 (2015).
Sarfo, J. O. et al. Malaria amongst children under five in sub-Saharan Africa: A scoping review of prevalence, risk factors and preventive interventions. Eur. J. Med. Res. 28(1), 80 (2023).
Tizifa, T. A. et al. Prevention efforts for malaria. Curr. Trop. Med. Rep. 5(1), 41–50 (2018).
Ludlow, J. T., Wilkerson, R. G. & Nappe, T. M. Methemoglobinemia. StatPearls [Internet] (StatPearls Publishing, 2023).
Skold, A., Cosco, D. L. & Klein, R. Methemoglobinemia: Pathogenesis, diagnosis, and management. South Med. J. 104(11), 757–761 (2011).
Umbreit, J. Methemoglobin—It’s not just blue: A concise review. Am. J. Hematol. 82(2), 134–144 (2007).
Ashurst, J. & Wasson, M. Methemoglobinemia: a systematic review of the pathophysiology, detection, and treatment. Del Med J. 83(7), 203–208 (2011).
Behera, G. C., Behera, S. K., Jena, R. K. & Bharati, V. S. Study of methaemoglobin in malaria patients. Indian J. Hematol. Blood Transfus. 32(1), 100–103 (2016).
Hänscheid, T. et al. Methaemoglobin and COHb in patients with malaria. Malar. J. 13, 285 (2014).
Eisenhut, M. Severe hemolysis as a potential contributing factor in the pathophysiology of cerebral malaria. Clin. Infect. Dis. 60(7), 1138 (2015).
Yeo, T. W. et al. Increased carboxyhemoglobin in adult falciparum malaria is associated with disease severity and mortality. J. Infect. Dis. 208(5), 813–817 (2013).
Anstey, N. M., Hassanali, M. Y., Mlalasi, J., Manyenga, D. & Mwaikambo, E. D. Elevated levels of methaemoglobin in Tanzanian children with severe and uncomplicated malaria. Trans. R. Soc. Trop. Med. Hyg. 90(2), 147–151 (1996).
Page, M. J. et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372, n71 (2021).
Morgan, R. L., Whaley, P., Thayer, K. A. & Schunemann, H. J. Identifying the PECO: A framework for formulating good questions to explore the association of environmental and other exposures with health outcomes. Environ. Int. 121(Pt 1), 1027–1031 (2018).
Haddaway, N. R., Collins, A. M., Coughlin, D. & Kirk, S. The role of Google Scholar in evidence reviews and its applicability to grey literature searching. PLoS One 10(9), e0138237 (2015).
Moola, S. M. Z., Tufanaru, C., Aromataris, E., Sears, K., Sfetcu, R., Currie, M., Qureshi, R., Mattis, P., Lisy, K. & Mu, P.-F. Chapter 7: Systematic reviews of etiology and risk: JBI. https://synthesismanual.jbi.global (2020).
Thomas, J. & Harden, A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med. Res. Methodol. 8, 45 (2008).
Higgins, J. P., Thompson, S. G., Deeks, J. J. & Altman, D. G. Measuring inconsistency in meta-analyses. BMJ 327(7414), 557–560 (2003).
Fu, R. G. G., Grant, M. et al. Conducting quantitative synthesis when comparing medical interventions: AHRQ and the effective health care program. (Agency for Healthcare Research and Quality (US), 2008). https://www.ncbi.nlm.nih.gov/books/NBK49407/
Willis, B. H. & Riley, R. D. Measuring the statistical validity of summary meta-analysis and meta-regression results for use in clinical practice. Stat. Med. 36(21), 3283–3301 (2017).
Chikezie, P. C. A study of erythro-cyte methaemoglobin concentration for diagnosis and monitoring of therapeutic events in malarial disease. Afr. J. Malar. Trop. Dis. 6(8), 421–426 (2018).
Erel, O., Kocyigit, A., Avci, S., Aktepe, N. & Bulut, V. Oxidative stress and antioxidative status of plasma and erythrocytes in patients with vivax malaria. Clin. Biochem. 30(8), 631–639 (1997).
Ifeanyi, O. E., Ndubuisi, O. T., Ifediora, A. & Kalu, O. N. Determination of methaemoglobin levels in malaria infected patients in University Health Services Department, Michael Okpara University of Agriculture, Umudike, Abia State, Nigeria. World J. Pharm. Res. 2(6), 3172–3177 (2013).
Karua, P. C., Mohapatra, M. K., Mishra, N. R. & Bariha, P. K. Methemoglobinemia and raised serum thiobarbituric acid reactive substance levels in malaria. Int. J. Adv. Res. 8, 45–51 (2020).
Uko, E. K., Udoh, A. E. & Etukudoh, M. H. Methaemoglobin profile in malaria infected children in Calabar. Niger. J. Med. 12(2), 94–97 (2003).
Zama, I. et al. Prevalence of malaria parasitaemia and methaemoglobin levels among blood donors in Sokoto, Nigeria. Intern. Med. Inside 1(1), 1–6 (2013).
Baird, J. K. Age-dependent characteristics of protection v. susceptibility to Plasmodium falciparum. Ann. Trop. Med. Parasitol. 92(4), 367–390 (1998).
White, M. & Watson, J. Age, exposure and immunity. Elife 7, e35832 (2018).
Rechetzki, K. F., Henneberg, R., da Silva, P. H. & do Nascimento, A. J. Reference values for methemoglobin concentrations in children. Rev. Bras. Hematol. Hemoter. 34(1), 14–16 (2012).
Balaji, S. N. & Trivedi, V. Extracellular methemoglobin primes red blood cell aggregation in malaria: an in vitro mechanistic study. FEBS Lett. 587(4), 350–357 (2013).
Kumar, S. & Trivedi, V. Extracellular methemoglobin promotes cyto-adherence of uninfected RBC to endothelial cells: Insight into cerebral malaria pathology. J. Cell. Biochem. 120(7), 11140–11149 (2019).
Balaji, S. N. & Trivedi, V. Extracellular methemoglobin mediated early ROS spike triggers osmotic fragility and RBC destruction: An insight into the enhanced hemolysis during malaria. Indian J. Clin. Biochem. 27(2), 178–185 (2012).
Deshmukh, R. & Trivedi, V. Methemoglobin exposure produces toxicological effects in macrophages due to multiple ROS spike induced apoptosis. Toxicol. In Vitro 27(1), 16–23 (2013).
Vieira, J. L., Ferreira, M. E. S., Ferreira, M. V. D. & Gomes, M. M. Primaquine in plasma and methemoglobinemia in patients with malaria due to Plasmodium vivax in the Brazilian Amazon Basin. Am. J. Trop. Med. Hyg. 96(5), 1171–1175 (2017).
Carmona-Fonseca, J., Alvarez, G. & Maestre, A. Methemoglobinemia and adverse events in Plasmodium vivax malaria patients associated with high doses of primaquine treatment. Am. J. Trop. Med. Hyg. 80(2), 188–193 (2009).
Ferreira, M. E. S., Gomes, M. S. M. & Vieira, J. L. F. Methemoglobinemia in patients with Plasmodium vivax receiving oral therapy with primaquine. Rev. Soc. Bras. Med. Trop. 44(1), 113–115 (2011).
Funding
KW is funded by Australian National Health and Medical Research Council (NHMRC) Investigator Grant (2008697).
Author information
Authors and Affiliations
Contributions
M.K., A.M., K.U.K. carried out the study design, study selection, data extraction, and statistical analysis; and drafted the manuscript. K.W., F.R.M., and P.W. participated in critically editing the manuscript. All authors read and approved the final manuscript. All authors consented to the publication of this study.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kotepui, M., Mahittikorn, A., Wilairatana, P. et al. Methemoglobin levels in malaria: a systematic review and meta-analysis of its association with Plasmodium falciparum and Plasmodium vivax infections and disease severity. Sci Rep 14, 3276 (2024). https://doi.org/10.1038/s41598-024-53741-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-53741-6
Keywords
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
