
Abstract
While previous research has explored the connection between video gaming and medical procedures, studies on the connection between video gaming and bronchoscopy techniques are lacking. This study aimed to investigate how video gaming experience influences bronchoscopy skills, particularly among beginners. This study was conducted at Fukujuji Hospital from January 2021 to October 2023. Twenty-three participants were assigned to the inexperienced group, and eighteen participants were assigned to the experienced group. The observational time during bronchoscopy, measured using a simulator, and the playing time of SPLATOON 2 (NINTENDO Co. Ltd., Japan) were analyzed. Video gaming skills were assessed based on game completion time, with shorter times indicating faster task completion. Participants were also divided into gamer and nongamer subgroups for further comparisons. A moderate linear relationship existed between bronchoscopic observation time and game completion time in the inexperienced group (r = 0.453, p = 0.030). However, no correlation was found in the experienced group (r = 0.268, p = 0.283). Among the inexperienced group, the gamer subgroup (n = 12) exhibited significantly shorter bronchoscopic observation times than did the nongamer subgroup (n = 11) (median [range]: 200 [129–229] s) vs. 281 [184–342] s, p = 0.005). This study demonstrated a relationship between bronchoscopy technique and video gaming skills among individuals with little bronchoscopy experience.
Similar content being viewed by others

Introduction
Flexible bronchoscopy is a widely used procedure for the assessment, diagnosis, and treatment of patients with respiratory disease1. Improving bronchoscopy techniques benefits patients by reducing discomfort during bronchoscopy2,3. Simulation-based training for bronchoscopy has shown significant advantages in enhancing skills and behaviors4. Recently, bronchoscopy simulators incorporating virtual reality technology and robotic-assisted bronchoscopy, in which instruments are controlled using a handheld controller while viewing a monitor, have increased in popularity5,6. These advanced devices have a similar setup to that of video games. Bronchoscopic procedures require skill sets that overlap with those of video games, including visuospatial awareness, rapid decision-making, and psychomotor skills7. Previous reports have shown that training with video games can improve various medical procedures, such as gastrointestinal endoscopy, laparoscopic surgery, and surgical techniques8,9,10,11,12,13. Studies have also reported a relationship between bronchoscopy techniques and previous video game experience among beginners7. However, in previous reports, active video game players were defined based on their self-reports, and their gaming skills were not evaluated7,8,9,10,11,12,13. Research evaluating both bronchoscopy techniques and video gaming skills is lacking. Therefore, this study aimed to investigate how video game experience affects bronchoscopy techniques, with a specific focus on these skills among beginners.
Materials and methods
Study design and setting
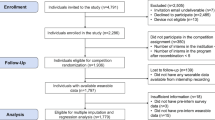
This study was conducted prospectively at Fukujuji Hospital from January 2021 to October 2023. Two groups of participants were recruited: the inexperienced group (consisting of medical students or residents without any surgical training or experience and no prior exposure to bronchoscopy) and the experienced group (consisting of respiratory physicians who had performed bronchoscopy ≥ 100 times). The exclusion criteria were as follows: patients who underwent bronchoscopy between 1 and 99 times and those who had played the game SPLATOON 2 (NINTENDO SWITCH) without gyro aiming. One participant was excluded based on the criteria. A total of 23 participants were included in the inexperienced group; these participants consisted of ten medical students, seven junior medical residents, and six senior medical residents. Two of the 23 participants in the inexperienced group aspired to become respiratory physicians, but many participants had not yet decided on their specialty. The experienced group included 18 respiratory physicians. Data on bronchoscopy techniques, video gaming skills, and other relevant variables were collected and compared between the inexperienced and experienced groups. Additionally, participants were further divided into two subgroups: the gamer subgroup and the non-gamer subgroup. Within each subgroup, data pertaining to bronchoscopy techniques and video gaming skills were compared, both in the inexperienced group and the experienced group. This study was approved by the Institutional Review Board of Fukujuji Hospital, and all participants provided written informed consent. The decisions made by this board were in accordance with the Declaration of Helsinki (Study number: 22033, IRB approval dates: January 1st, 2023).
Evaluation of bronchoscopy techniques
The participants’ bronchoscopy technique results were evaluated by assessing the duration of observation of the bronchial lumen (hereafter, observation time). Participants utilized a flexible bronchoscope (BF-P290, OLYMPUS Co., Ltd., Japan) on a simulator (11117-000, KYOTO KAGAKU Co., Ltd., Japan) to perform the observations in a specific order. The bronchoscope was inserted through the mouth of the simulator, and sequentially observed and capturedimages of the tracheal bifurcation, right main bronchus, right upper lobe bronchus, intermediate bronchial trunk, middle lobe branch, right S6 bronchus, right S7 bronchus, right S8-10 bronchi, tracheal bifurcation, left main bronchus, left upper lobe branch, left upper division branch, lingular branch, left lower lobe branch, left S6 bronchus, left S8-10 bronchi, and finally the tracheal bifurcation again. The inexperienced group received guidance and underwent training for approximately 10 min before the simulated bronchoscopy, and the route was guided during observation of the bronchial lumen under the supervision of an experienced doctor. The experienced group underwent bronchoscopy as usual, without any specific training or guidance.
Evaluation of video gaming skills
The participants’ video gaming skills were assessed by having them play the game SPLATOON 2 on a Nintendo Switch console, with shorter game completion time indicating the ability to complete tasks rapidly. SPLATOON 2 is a third-person shooter game in which the objective is to paint a field with paint bullets in a team game setting. Players control a character and use a gun with paint bullets to attack enemies and paint fields. In this study, participants played a trial mode involving defeating 8 enemies. The latency to attack all the enemies was measured (hereafter, the game completion time). Prior to the evaluation, participants were given an opportunity to practice by defeating all the enemies once. All participants used the starting weapon provided in the game. The game typically utilizes gyro aiming, which involves aiming to tilt the controller, which is equipped with a gyroscope. However, participants in this study played the game with the gyro aiming turned off and used a regular controller instead. SPLATOON 2 can choose gyro aiming or joystick, which are features that were recently developed; however, players generally play video gaming by using joystick. Therefore, participants in our study used a joystick when playing SPLATOON 2. The reasons for choosing SPLATOON 2 for an evaluation of video gaming skills were as follows: a third-person shooter game, easy operation even for gaming beginners (player uses 2 levers and 1 bottom only), and the presence of an easy stage for an evaluation of video gaming skills.
Definition of the gamer subgroup
In this study, participants were classified into two subgroups based on their video game experience. The gamer subgroup included participants with experience playing video games that involved controlling a character from a first-person or third-person perspective, such as shooter games and 3D-action games. These participants reported playing games for at least 1 h per week, and they had engaged in video gaming for 6 years or more. The definition was established according to a modified version of a previous report. The original report did not specify the duration of gaming experience; therefore, we decided to define the duration as 6 years or more, aligning with typical educational periods such as elementary school, between junior high school and high school, or university. In contrast, the non-gamer subgroup consisted of participants who either lacked prior gaming experience or who played games mainly within the genres of role-playing games, adventure games, puzzle games, and/or simulation games. These participants had limited exposure to games involving character control from a first-person or third-person perspective.
Statistical methods
All the data were analyzed and processed using EZR, version 1.5314. Spearman’s correlation analysis was performed to determine the relationships among the different variables. The interpretation of Spearman’s correlation was based on the Dancey & Reidy criteria as follows: perfect (r = 1 or − 1), strong (1 > r ≥ 0.7 or − 1 > r ≥ − 0.7), moderate (0.7 > r ≥ 0.4 or − 0.7 > r ≥ − 0.4), weak (0.4 > r ≥ 0.1 or − 0.4 > r ≥ − 0.1), or zero (r = 0)15. The Mann–Whitney U test and Fisher’s exact test were used for group comparisons. The level of statistical significance was set at p = 0.05 (2-tailed).
Ethics approval and consent to participate
The study was approved by the Institutional Review Board of Fukujuji Hospital (Study number: 22033, IRB approval dates: January 1st, 2023), and all participants provided written informed consent. The decisions made by this board are based on and in accordance with the Declaration of Helsinki.
Results
The baseline characteristics of the study participants are summarized in Table 1. Among participants in the inexperienced group, the median age was 27 years (range: 22–36), and 15 (65.2%) were male. The median bronchoscopic observation time and the median game completion time of this group were 215 s (range: 129–342) and 45 s (range: 22–153), respectively. Among participants in the experienced group, the median age was 33 years (range: 28–49), and 15 (83.3%) were male. The median bronchoscopic observation time in the experienced group (103 s, range: 79–165 s) was significantly shorter than that in the inexperienced group (p < 0.001). The median game completion time in the experienced group was 41 s (range: 26–134), which was not significantly different from that in the inexperienced group (p = 0.478). The number of participants categorized as gamers in each group did not significantly differ, with 12 participants (52.2%) in the inexperienced group and 10 participants (55.6%) in the experienced group categorized as gamers (p = 1.000).
The bronchoscopic observation time had a moderate linear relationship with the game completion time among participants in the inexperienced group (r = 0.453, p = 0.030) (Fig. 1A). There was no correlation between bronchoscopic observation time and game completion time among participants in the experienced group (r = 0.268, p = 0.283) (Fig. 1B).

Pearson’s correlation analysis of the relationship between bronchoscopic observation time and game completion time among participants. (A) Within the inexperienced group, there was a moderate linear relationship between bronchoscopic observation time and game completion time (r = 0.453, p = 0.030). (B) Within the experienced group, no correlation was found between bronchoscopic observation time and game completion time (r = 0.268, p = 0.283).
In the inexperienced group, 12 participants were in the gamer subgroup, and 11 participants were in the nongamer subgroup. The bronchoscopic observation time in the gamer subgroup was significantly shorter than that in the nongamer subgroup within the inexperienced group (median [range]: 200 [129–229] s vs. 281 [184–342] s, p = 0.005) (Fig. 2A). The game completion time was also shorter in the gamer subgroup than in the nongamer subgroup within the inexperienced group (median [range]: 34 [22–47] s vs. 93 [41–153] s, p < 0.001) (Fig. 2B). In the experienced group, there were 10 participants in the gamer subgroup and 8 participants in the nongamer subgroup. There was no significant difference in the bronchoscopic observation time between the gamer subgroup and the nongamer subgroup within the experienced group (median [range]: 101 [79–152] s vs. 105 [82–165] s, p = 0.534). However, the game completion time in the gamer subgroup was significantly shorter than that in the nongamer subgroup within the experienced group (median [range]: 34 [26–47] s vs. 69 [31–134] s, p = 0.006).

Comparison of bronchoscopic observation time and game completion time between the gamer subgroup (n = 12) and nongamer subgroup (n = 11) within the inexperienced group. (A) The bronchoscopic observation time in the gamer subgroup was significantly shorter than that in the nongamer subgroup (median [range]: 200 [129–229] s vs. 281 [184–342] s, p = 0.005). (B) The game completion time was shorter in the gamer subgroup than in the nongamer subgroup (median [range]: 34 [22–47] s vs. 93 [41–153] s, p < 0.001).
Discussion
This study examined the relationship between bronchoscopy techniques and video game playing skills. Within the inexperienced group, there was a correlation between bronchoscopic observation time and game completion time, indicating that participants with better video game skills were faster at performing bronchoscopic observation. Presumably, individuals who were accustomed to gaming may exhibit better baseline handling of bronchoscopy techniques, as suggested by a previous report7. However, a previous report showed that an 8-week video gaming program involving 2.5 h of training every week did not lead to mastery of bronchoscopy techniques7. One of the gamers’ skills is related to the use of handheld controllers for character manipulation on screens. Gamers have developed a sense that their controller-based manual actions correlate with on-screen actions, and this skill enables gamers to excel in playing even new games more proficiently. Gamers acquire skills through prolonged gaming habits. We believe that this skill could help gamers intuitively understand how to perform bronchoscopy and expedite their mastery of bronchoscopy techniques. Conversely, in the experienced group, there was no significant difference in bronchoscopic observation time according to gaming experience. This finding suggested that, in practice, operators can acquire proficiency in bronchoscopy regardless of their video gaming experience. Patients often experience discomfort during bronchoscopy16, and skilled operators can help reduce patient discomfort during bronchoscopy2,3, emphasizing the importance of acquiring proficient bronchoscopy techniques4.
Bronchoscopic procedures share similarities with video gaming7, as operators navigate through the bronchi displayed on a monitor and manipulate devices to perform tasks. Bronchoscopy is performed from a first-person perspective and with devices (such as forceps) aimed at accessing and inserted into the targeted bronchi. This system appears to involve skills similar to those of playing 3D shooter games, such as first-person or third-person shooter games. A previous report also indicated a lower airway collision rate during bronchoscopy among the gamer group7, while our study did not investigate bronchoscopy techniques based on assessment tools such as the Bronchoscopic Skills and Tasks Assessment Tool and the Bronchoscopy Step-by-Step Evaluation Tool, which is a validated tool for assessing competency in bronchoscopy17. In addition to bronchoscopy, previous studies have reported medical procedures. A video gaming experience provides benefits in laparoscopy11,18,19, robotic surgery11,20,21, gastrointestinal endoscopy22, arthroscopy23, ophthalmic surgery24, and endotracheal intubation25, and eye-hand and visual-spatial skills training through video gaming could be associated with various medical procedures. Therefore, gamers who are accustomed to using controllers to shift their position as indicated on a monitor may excel in performing bronchoscopy due to their gaming experience. Additionally, high visuospatial awareness, which is enhanced through gaming, may also enhance bronchoscopy techniques7. Video gaming has been shown to improve the ability to learn new tasks26 and enhance cortical plasticity and performance of minimally invasive skills8,27. While operators can improve their bronchoscopy techniques over time4,5, gamers may require less practice to achieve proficiency. Prolonged examination time during bronchoscopy can lead to intense coughing2,16, highlighting the benefits of operators who are proficient with advanced techniques that minimize the duration of the procedure2,3. Furthermore, simulation-based bronchoscopy training, including virtual reality gaming aspects, has also attracted attention for leading to improved skills in recent years5; thus, gaming experiences may further benefit beginners. However, the actual utilization of these training devices may not be high, potentially due to a lack of simulator availability28. It is considered that the application of games to education will become more important. On the other hand, brief exposure to video gaming has been found to have no impact on bronchoscopic procedures7. Therefore, tailored learning programs should be developed for individual learners, and considering their gaming experience and skills might prove beneficial.
Importantly, video gaming might have both positive and negative effects. While there are concerns about the potential adverse effects of video gaming on children, such as increased aggression, decreased empathy, or decreased academic performance29, the influences of gaming are generally minimal30,31,32. Furthermore, gaming during puberty has been associated with a temporary psychological state called Chūnibyō, in which children exhibit media-inspired behaviors, in Japan33. However, importantly, Chūnibyō is not considered a disease, and we do not believe that gaming has negative effects on children during puberty33. Studies have demonstrated the benefits of gaming for improving visuomotor control27,34, cascading action35, and information processing36 as well as increasing motivation through reward mechanisms7,37. It is crucial to prevent excessive reliance on gaming38; however, appropriate gaming experiences and training may have transferable learning benefits beyond video games26. Overall, video gaming has potential applications in the field of medicine as techniques continue to improve.
This investigation has several limitations. The study was conducted at a single clinical center. The sample size was small, although a significant relationship was observed between bronchoscopic observation time and video gaming time in the inexperienced group. Based on the sample size calculation for the comparison of mean values between two groups conducted in advance, each group (gamer and non-gamer groups) in the inexperienced group needed 9 participants. In the experienced group, each group needed 7 participants based on a non-inferior sample size calculation for the comparison of mean values between the two groups. Two participants had prior experience playing SPLATOON 2 before this study; however, they played with gyro aiming. All participants in this study used a joystick to play SPLATOON 2, which differs from gyro aiming. Therefore, their previous experience with gyro aiming at SPLATOON 2 may not have affected the recorded game completion time. We choose SPLATOON 2 for an evaluation of video gaming skills because of the use of a third-person shooter game, easy operation, and easy stage. A first-person shooting game might be more suitable for assessing bronchoscopic technique efficacy. However, most first-person shooting games feature too complex operations and stages for beginners, which may not be useful for effectively assessing participants’ gaming skills. Both first-person and third-person shooter games require aiming and shooting at targets and share many common controls. Therefore, we believe that the bias introduced by this difference is minimal. Another limitation is that only bronchoscopic observation time was used to evaluate bronchoscopy technique, and other factors, such as airway collision rates and the Purdue Visual Spatial test, were not evaluated. Generally, beginners focus on learning to perform bronchoscopic observation, and this technique becomes the basis of further techniques, such as bronchoalveolar lavage, brushing, and forceps biopsy; therefore, we chose to assess bronchoscopic observation time in this study. The specialty of participants in the inexperienced group and their aspiration of airway anatomy knowledge may have differed among participants in the inexperienced group. This may bias the results of this study.
Conclusion
This study demonstrated a correlation between bronchoscopy technique and video gaming skills among beginners lacking experience performing bronchoscopy. This finding suggested that individuals who are accustomed to playing video games may have rapid access to bronchoscopy techniques.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
References
Du Rand, I. A. et al. British Thoracic Society guideline for diagnostic flexible bronchoscopy in adults: Accredited by NICE. Thorax 68(Suppl 1), i1–i44. https://doi.org/10.1136/thoraxjnl-2013-203618 (2013).
Kobayashi, F. et al. Novel predictive factors for patient discomfort and severe cough during bronchoscopy: A prospective questionnaire analysis. PLoS ONE 15, e0240485. https://doi.org/10.1371/journal.pone.0240485 (2020).
Mitsumune, T., Senoh, E. & Adachi, M. Prediction of patient discomfort during fiberoptic bronchoscopy. Respirology 10, 92–96. https://doi.org/10.1111/j.1440-1843.2005.00642.x (2005).
Kennedy, C. C., Maldonado, F. & Cook, D. A. Simulation-based bronchoscopy training: Systematic review and meta-analysis. Chest 144, 183–192. https://doi.org/10.1378/chest.12-1786 (2013).
Aljohaney, A. A. Predictors of virtual reality simulation bronchoscopy performance among novice bronchoscopists. Adv. Med. Educ. Pract. 10, 63–70. https://doi.org/10.2147/AMEP.S186275 (2019).
Murgu, S. D. Robotic assisted-bronchoscopy: Technical tips and lessons learned from the initial experience with sampling peripheral lung lesions. BMC Pulm. Med. 19, 89. https://doi.org/10.1186/s12890-019-0857-z (2019).
Mallow, C. et al. Impact of video game cross-training on learning bronchoscopy. A pilot randomized controlled trial. ATS Sch. 1, 134–144. https://doi.org/10.34197/ats-scholar.2019-0015C (2020).
Harrington, C. M., Chaitanya, V., Dicker, P., Traynor, O. & Kavanagh, D. O. Playing to your skills: A randomized controlled trial evaluating a dedicated video game for minimally invasive surgery. Surg. Endosc. 32, 3813–3821. https://doi.org/10.1007/s00464-018-6107-2 (2018).
Giannotti, D. et al. Play to become a surgeon: Impact of Nintendo Wii training on laparoscopic skills. PLoS One 8, e57372. https://doi.org/10.1371/journal.pone.0057372 (2013).
Ju, R., Chang, P. L., Buckley, A. P. & Wang, K. C. Comparison of Nintendo Wii and PlayStation2 for enhancing laparoscopic skills. JSLS 16, 612–618. https://doi.org/10.4293/108680812X13462882737294 (2012).
Gupta, A. et al. Can video games enhance surgical skills acquisition for medical students? A systematic review. Surgery 169, 821–829. https://doi.org/10.1016/j.surg.2020.11.034 (2021).
de Araujo, T. B. et al. Impact of video game genre on surgical skills development: A feasibility study. J. Surg. Res. 201, 235–243. https://doi.org/10.1016/j.jss.2015.07.035 (2016).
Schlickum, M. K., Hedman, L., Enochsson, L., Kjellin, A. & Fellander-Tsai, L. Systematic video game training in surgical novices improves performance in virtual reality endoscopic surgical simulators: A prospective randomized study. World J. Surg. 33, 2360–2367. https://doi.org/10.1007/s00268-009-0151-y (2009).
Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 48, 452–458. https://doi.org/10.1038/bmt.2012.244 (2013).
Akoglu, H. User’s guide to correlation coefficients. Turk. J. Emerg. Med. 18, 91–93. https://doi.org/10.1016/j.tjem.2018.08.001 (2018).
Yildirim, F., Ozkaya, S. & Yurdakul, A. S. Factors affecting patients’ comfort during fiberoptic bronchoscopy and endobronchial ultrasound. J. Pain Res. 10, 775–781. https://doi.org/10.2147/JPR.S118047 (2017).
Davoudi, M., Osann, K. & Colt, H. G. Validation of two instruments to assess technical bronchoscopic skill using virtual reality simulation. Respiration 76, 92–101. https://doi.org/10.1159/000126493 (2008).
Sammut, M., Sammut, M. & Andrejevic, P. The benefits of being a video gamer in laparoscopic surgery. Int. J. Surg. 45, 42–46. https://doi.org/10.1016/j.ijsu.2017.07.072 (2017).
IJgosse, W., van Goor, H., Rosman, C. & Luursema, J. M. Construct validity of a serious game for laparoscopic skills training: Validation study. JMIR Serious Games 8(2), e17222. https://doi.org/10.2196/17222 (2020).
Harbin, A. C. et al. Prior video game utilization is associated with improved performance on a robotic skills simulator. J. Robot. Surg. 11, 317–324. https://doi.org/10.1007/s11701-016-0657-x (2017).
Kilincarslan, O. et al. Video gaming improves robotic surgery simulator success: A multiclinic study on robotic skills. J. Robot. Surg. 17, 1435–1442. https://doi.org/10.1007/s11701-023-01540-y (2023).
van Dongen, K. W., Verleisdonk, E. J., Schijven, M. P. & Broeders, I. A. Will the playstation generation become better endoscopic surgeons?. Surg. Endosc. 25, 2275–2280. https://doi.org/10.1007/s00464-010-1548-2 (2011).
Jentzsch, T. et al. Correlation between arthroscopy simulator and video game performance: A cross-sectional study of 30 volunteers comparing 2- and 3-dimensional video games. Arthroscopy 32, 1328–1334. https://doi.org/10.1016/j.arthro.2015.12.047 (2016).
Khimani, K. et al. Video game warm-up may suggest improvement in ophthalmic surgical simulator performance in surgically naive students. Clin. Ophthalmol. 16, 2561–2568. https://doi.org/10.2147/OPTH.S369697 (2022).
Simsek, T. et al. The impact of video games on training: Can it change the game of endotracheal intubation?. J. Clin. Monit. Comput. 36, 901–906. https://doi.org/10.1007/s10877-021-00796-9 (2022).
Green, C. S. & Bavelier, D. Learning, attentional control, and action video games. Curr. Biol. 22, R197–R206. https://doi.org/10.1016/j.cub.2012.02.012 (2012).
Granek, J. A., Gorbet, D. J. & Sergio, L. E. Extensive video-game experience alters cortical networks for complex visuomotor transformations. Cortex 46, 1165–1177. https://doi.org/10.1016/j.cortex.2009.10.009 (2010).
Huang, H. et al. Application of bronchoscopy in the diagnosis and treatment of peripheral pulmonary lesions in China: A national cross-sectional study. J. Cancer 14, 1398–1406. https://doi.org/10.7150/jca.84220 (2023).
Anderson, C. A. et al. Violent video game effects on aggression, empathy, and prosocial behavior in eastern and western countries: A meta-analytic review. Psychol. Bull. 136, 151–173. https://doi.org/10.1037/a0018251 (2010).
Ferguson, C. J. Do angry birds make for angry children? A meta-analysis of video game influences on children’s and adolescents’ aggression, mental health, prosocial behavior, and academic performance. Perspect. Psychol. Sci. 10, 646–666. https://doi.org/10.1177/1745691615592234 (2015).
Beck, V. & Rose, C. Is sexual objectification and victimization of females in video games associated with victim blaming or victim empathy?. J. Interpers. Viol. 36, NR3196–NR3221. https://doi.org/10.1177/0886260518770187 (2021).
Boxer, P., Groves, C. L. & Docherty, M. Video games do indeed influence children and adolescents’ aggression, prosocial behavior, and academic performance: A clearer reading of ferguson. Perspect. Psychol. Sci. 10, 671–673. https://doi.org/10.1177/1745691615592239 (2015).
Shimoda, M., Morimoto, K., Tanaka, Y., Yoshimori, K. & Ohta, K. Characteristics of “chunibyo’ identified by a questionnaire. PLoS One 16, e0260375. https://doi.org/10.1371/journal.pone.0260375 (2021).
Li, L., Chen, R. & Chen, J. Playing action video games improves visuomotor control. Psychol. Sci. 27, 1092–1108. https://doi.org/10.1177/0956797616650300 (2016).
Steenbergen, L., Sellaro, R., Stock, A. K., Beste, C. & Colzato, L. S. Action video gaming and cognitive control: Playing first person shooter games is associated with improved action cascading but not inhibition. PLoS One 10, e0144364. https://doi.org/10.1371/journal.pone.0144364 (2015).
Powers, K. L., Brooks, P. J., Aldrich, N. J., Palladino, M. A. & Alfieri, L. Effects of video-game play on information processing: A meta-analytic investigation. Psychon. Bull. Rev. 20, 1055–1079. https://doi.org/10.3758/s13423-013-0418-z (2013).
Lorenz, R. C., Gleich, T., Gallinat, J. & Kuhn, S. Video game training and the reward system. Front. Hum. Neurosci. 9, 40. https://doi.org/10.3389/fnhum.2015.00040 (2015).
King, D. L. & Delfabbro, P. H. The cognitive psychology of Internet gaming disorder. Clin. Psychol. Rev. 34, 298–308. https://doi.org/10.1016/j.cpr.2014.03.006 (2014).
Author information
Authors and Affiliations
Contributions
M.S. formulated the research idea, designed the study, analyzed the data, and drafted the manuscript. Y.T. drafted the manuscript with a coresponding author. K.M. and K.Y. collected the data. K.O. was a project administrator.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Shimoda, M., Tanaka, Y., Morimoto, K. et al. Video gamers demonstrate superior bronchoscopy skills among beginners. Sci Rep 14, 2290 (2024). https://doi.org/10.1038/s41598-024-52730-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-52730-z
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
