
Abstract
General and electronic health literacy are important factors engaging in healthy behaviors and maintaining good health. The present study explored demographic factors associated with general and electronic health literacy in the Iranian adult population. Via stratified cluster sampling, trained interviewers visited adult residents in Qazvin Province, Iran between January, and April 2022. The participants (N = 9775; mean age = 36.44 years; 6576 [67.3%] females) completed the Health Literacy Instrument for Adults (HELIA) assessing health literacy and the eHealth Literacy Scale (eHEALS) assessing electronic health literacy. Demographic data, including age, gender, educational level, marital status, and living location (city or rural), were collected. Latent class analysis (LCA) was used to classify the participants into different health literacy/electronic health literacy levels. The relationships between health literacy/electronic health literacy levels and demographic factors were examined using χ2 or analysis of variance. The LCA used HELIA scores to suggest five classes of health literacy and eHEALS scores to suggest three classes of electronic health literacy. For general and electronic health literacy, similar relationships were with demographic factors: females as compared with males had better general/electronic health literacy; younger people as compared with older people had better general/electronic health literacy; higher educational level was associated with better general/electronic health literacy; and city residents as compared with rural residents had better general/electronic health literacy. In conclusion, Iranian governmental agencies may wish to target on males, older adults, people with low educational level, and rural residents to improve their health literacy.
Similar content being viewed by others

Introduction
The importance of health literacy has been well documented. Health literacy can promote engagement in healthy behaviors and reduce engagement in unhealthy ones1,2. When people engage in healthy behaviors (e.g., exercising) and reduce unhealthy one (e.g., smoking), their health, including life expectancy and life quality, are often substantially improved3,4,5,6. Such effects of health literacy may relate to specific qualities: health literacy may involve people’s abilities in reading, writing, comprehending, and understanding useful health information7. Moreover, the World Health Organization (WHO) indicated that high levels of health literacy will motivate people to promote and maintain good health8.
Given technological advances, health literacy has evolved into digital forms (i.e., electronic health literacy)9,10. Accordingly, health literacy includes general and electronic health literacy. Electronic health literacy has then been defined as “the ability to gather and appropriately process health information retrieved online”11. The importance of electronic health literacy is growing due to continuously advancing technologies. People with higher levels of electronic health literacy have demonstrated better knowledge of colorectal cancer and more engagement in cancer screening12. Electronic health literacy is an important factor associated with better preventive behaviors (e.g., medication adherence) among patients with heart failure and results in better health outcomes13. In addition, electronic health literacy was found to be associated with better mental health among adult population14, with better behavioral and cognitive performance among older people15, and higher adherence to health-promotion behaviors among adolescents16.
Given that health literacy and electronic health literacy are important for people to obtain and maintain healthy mental and physical and fitness, it is important to examine potential demographic factors associated with general and electronic health literacy. To date, several demographic factors have been associated with general or electronic health literacy, but findings are sometimes mixed. For example, males have demonstrated better health literacy than females17,18, females have demonstrated better health literacy than males19,20,21. and no significant differences in health literacy have been observed between genders22. Most studies have found that older people (especially those aged 65 years or above) demonstrate poorer health literacy as compared with t younger individuals20,22,23,24,25,26,27, with an exception being an Australian study showing that older people had slightly better health literacy than younger people17. Most studies showed that people having higher educational levels as compared with those having lower educational ones had better health literacy17,18,19,20,21,26,28. Moreover, people living in rural areas have demonstrated similar health literacy score to those living in urban areas17; single and married people have demonstrated better health literacy than those who are widowed, divorced, or separated22. As a result, health literacy may have different associations with gender according to the samples studied, with arguably the most consistent findings with age and educational level.
Multiple factors may influence relationships between health literacy and specific demographic features. For example, cultural factors may exert differential effects on specific relationships, e.g., how older versus younger adults or males versus females are enculturated in specific societies. Additionally, the use of digital technologies maty differ across jurisdictions. Most research has been conducted in WEIRD (Western, educated, industrialized, rich and democratic) countries. As such, there is a need to study relationships between health literacy and demographic measures in non-WEIRD countries like Iran.
To the best of the present authors’ knowledge, studies assessing associations between general and electronic health literacy and demographic factors have observed raw scores of general or electronic health literacy. Although using the raw scores can help understand associations, they may not help identify if a person is classified in a certain level of general or electronic health literacy, such as a high, middle, or low level of literacy. In other words, raw scores may help identify relative levels of general or electronic health literacy (e.g., score 20 is higher than score 18) but may not distinguish group levels (e.g., if score 20 is of a high, middle, or low level). Consequently, one may not identify important demographic factors associated with degrees of general or electronic health literacy using the scores. To overcome this concern, latent class analysis (LCA) may classify people into different groups based on general or electronic health literacy. In other words, the LCA helps researchers to cluster the people into different classes (or levels) using the latent features (e.g., the health literacy and electronic health literacy in the present study) of these participants. Specifically, LCA applies fit statistics to help researchers identify appropriate latent groups to ensure the robustness of classifications29. LCA utilizes probability calculated from raw scores to identify the classes to which individuals belong30. Therefore, estimations of an individual belonging to a specific latent class is arguably less biased as compared with other clustering statistics31.
To better understand associations between general/electronic health literacy and demographics, we sought to classify individuals based on general/electronic health literacy levels using LCA. Consequently, levels of general/electronic health literacy classified by LCA could be used to investigate relationships with demographic features. The present study used a large sample from the general Iranian population to classify individuals based on levels of general and electronic health literacy. Next, the study assessed which demographic factors related to the LCA-identified groups.
Methods
Participants and data collection
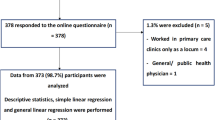
This cross-sectional study was conducted on a sample from the general population of adults in Qazvin, Iran between January, and April 2022. The Ethics Committee of Qazvin University of Medical Sciences (IR.QUMS.REC.1400.225) approved the study. All methods were performed in accordance with the relevant guidelines and regulations. Using a stratified cluster sampling technique from 70 strata in the Qazvin province, paper-and-pencil questionnaires were distributed by trained interviewers to adult residents in Qazvin. Specifically, the trained interviewers contacted the adults who were selected for participation to explain the research purpose and information. After the participants agreed to participate, they were asked to come to the health centers to complete the questionnaires using paper and pen under the supervision of the trained interviewers. Moreover, we have invited 14,100 participants to participate and 9775 completed the questionnaires with a response rate of 69%. The sample size was sufficient for the LCA used in the present study given that prior methodological evidence shows that a sample size > 500 is needed for LCA32,33. All participants provided written informed consent before beginning the survey34. The detailed information regarding the study procedure has been described elsewhere14,34,35. Although the data of the present study are the same as those used in other research14, different research questions have been investigated between the present study and prior research14.
Measures
Health Literacy Instrument for Adults (HELIA)
The HELIA is a subjective measure assessing health literacy using 33 items rated on a five-point Likert scale (1 = never; 5 = always). The 33 items were distributed in five types of health literacy: reading (four items; example item: “Reading educational materials about health (booklets, pamphlets, leaflets) is easy for me”), access to information (six items; example item: “I can find health information about healthy eating”), understanding (seven items; example item: “I can understand the recommendations for a healthy diet”), appraisal (four items; example item: “I can communicate trusted health information to others”), and decision-making/behavioral intention (12 items; example item: “I am helath-conscious in any situation”). Overall health literacy can be assessed using the HELIA total score (i.e., summing the 33 item scores), and higher scores indicate better health literacy34. The HELIA has been validated among Iranian adults with promising psychometric properties36.
eHealth Literacy Scale (eHEALS)
The eHEALS is a subjective measure assessing electronic health literacy using eight items rated on a five-point Likert scale (1 = strongly disagree; 5 = strongly agree). The eight items reflect the construct of electronic health literacy (example item: “I know how to find helpful health resources on the Internet”)10. Overall electronic health literacy can be assessed using the eHEALS total score (i.e., summing the eight item scores), and higher scores reflect better electronic health literacy13. The eHEALS has been validated among Iranian adults with promising psychometric properties37.
Demographic measures
Participants were asked to report their demographic information, including age, gender, educational level, living location, and marital status.
Data analysis
LCA is a modeling technique used for identifying subgroups of individuals with unobserved but distinct patterns of responses to a set of observed categorical indicators. The LCA model was fitted based on the score of each item in both HELIA and eHEALS questionnaires. First, each person's scores were converted to 1 and 2. In this way, scores higher than three were considered as two and scores three or lower were considered as one. The LCA model was fitted using the obtained variables. The LCA model was performed in R software using the PoLCA package. Based on the literature, a conservative and reliable group of fit indices and criteria was selected to evaluate the goodness of fit of the possible LCA models: Akaike Information Criterion (AIC), Bayesian Information Criterion (BIC), the adjusted BIC (aBIC), G2, χ2, Entropy, Lo-Mendell-Rubin adjusted likelihood ratio test (LMRT) and Bootstrapped likelihood ratio test (BLRT). The best-fitting models are those with the best balance between smaller values on the AIC, BIC, aBIC and χ2 statistics, higher log likelihoods, and fewer numbers of parameters in the model. Finally, χ2 tests were used to examine if the participants at different levels of general or electronic health literacy differed in their demographic characteristics.
Results
Descriptive characteristics
A total of 9775 adults completed the study measures. The mean age of the participants was 36.44 ± 11.97 years. Most participants were female (n = 6576, 67.3%), lived in city areas (n = 7287, 74.6%), had completed university degrees (n = 3851, 39.4%), and were married (n = 6987, 71.5%).
LCA Models for HELIA and eHEALS
LCA resulted in a final model with five latent classes in HELIA and three latent class in eHEALS questionnaires (Table 1). Models from one-class to seven-class solutions were analyzed and compared to decide upon the number of classes with the consideration of balancing better model fit (higher log likelihood) with parsimony (fewer parameters in the model). The fit indices in each model are shown in Table 1. With increases of classes, the following criteria decreased: AIC, BIC, aBIC and χ2. However, only from the fourth to the fifth class were there significant decreases according to χ2 tests. Both the BLRD and LMRT had statistical significance (P < 0.001). As a result, five latent classes for HELIA were selected. Similar considerations led to three latent classes for eHEALS being selected. The slopes of the AIC, BIC, and aBIC measures are presented in Fig. 1 (for HELIA) and Fig. 2 (for eHEALS).

Comparison of AIC, BIC, and Adj. BIC on Steep Slope Graphs for HELIA.

Comparison of AIC, BIC, and Adj. BIC on Steep Slope Graphs for eHEALS.
Class descriptions
Regarding the HELIA classes, Class 1 (35.8% of the sample) was labelled as a “very high health literacy” group and was characterized by high probability of endorsement of nearly all HELIA items. Class 2 (16.9%) was labelled as a “moderate health literacy” group and characterized by strong endorsement of understanding and appraisal. Class 3 (20.5%) was labelled as a “high health literacy” group characterized by high probability of endorsement of reading, access to information, understanding and appraisal. Class 4 (18.1%) was labelled as a “low health literacy” group characterized by similar patterns with Class 2 but with lower endorsement rates. Class 5 (8.7%) was labelled as a “very low health literacy” group characterized by low endorsement of all HELIA items (Fig. 3).

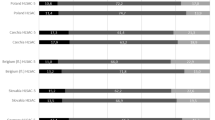
Conditional probability distribution on each item of the HELIA.
Regarding the eHEALS classes, Class 1 (25% of the sample) was labelled as a “moderate electronic health literacy” group and was characterized by strong endorsement of how to find helpful health resources on the internet (eHEALS1), how to use the internet to answer health questions (eHEALS2), what health resources are available on the internet (eHEALS3), where to find helpful health resources on the internet (eHEALS4), and how to use the health information (eHEALS5) (Fig. 4). Class 2 (14.3%) was labelled as a “low electronic health literacy” group and was characterized by low endorsement of all eHEALS items (Fig. 3). Class 3 (60.7% of sample) was labelled as “high electronic health literacy group” and was characterized by high probability of endorsement of nearly all eHEALS items.

Conditional probability distribution on each item of the eHEALS.
Demographic characteristics relating to specific classes
Univariate analyses of sociodemographic characteristics and latent classes for both HELIA and eHEALS latent classes are shown in Supplementary Tables S1, S2, S3 and S4. All latent classes for both HELIA and eHEALS differed across gender, age, HELIA total score, eHEALS total score, education level, and living location status. Latent classes of HELIA differed across marital status but those of eHEALS did not. There were more females than males in classes reflecting better general/electronic health literacy; more younger people than older people were in classes reflecting better general/electronic health literacy; more people with higher educational levels than those with lower educational levels were in classes reflecting better general/electronic health literacy; and more city residents than rural residents were in classes reflecting better general/electronic health literacy.
Discussion
To the best of the present authors’ knowledge, this is the first large-scale study assessing both general and electronic health literacy among a sample from the Iranian adult population analyzed using LCA. The findings indicate that individuals could be grouped into five different levels according to general health literacy and three different levels according to electronic health literacy. Higher levels of general and electronic health literacy were found in latent classes with more females, younger people, education, and city residents. Therefore, classes based on measures of general and electronic health literacy displayed largely similar relationships with multiple demographic factors. These findings suggests that electronic health literacy shares similar feature to general health literacy; that is, whether an individual could understand and use health information7,11.
A difference between general and electronic health literacy may involve the platform of obtaining health information (internet for electronic health literacy and no specific platform for general health literacy).
The findings that females had better health literacy than males in the present study are consistent with some prior findings19,20,21. However, other studies reported that males as compared with females had better health literacy17,18, whereas some found no differences between males and females22. The differences could reflect jurisdictional differences. For example, studied an Australian sample17 and studied a Turkish sample18. Prior studies of Iranian samples suggest that female Iranians had better general/electronic health literacy than male Iranians19,21, except for a study22. Finding no significant difference. A potential reason for the higher levels of general/electronic health literacy in women than in men could be explained by the gender roles in Iran. Specifically, Iranian women were not expected to work but to take care of the family’s health19. In this regard, Iranian women have time and motivations to learn health information, which subsequently reflect on their levels of health literacy. However, prior Iranian studies did not use LCA to examine relationships between health literacy and gender. The present findings are consistent with prior reports of Iranian females having better health literacy, including electronic health literacy, than Iranian males.
In agreement with other prior findings20,22,23,24,25,26,27, the present study found that younger Iranians had better general and electronic health literacy than older Iranians. A main reason may involve educational levels. Specifically, younger people had higher levels of education than older people, and higher levels of education were associated with better general/electronic health literacy, as evidenced by the present findings and prior research17,18,19,20,21,26,28.
Beauchamp et al. (2015) found that people living in rural areas had similar health literacy scores to those living in urban areas; however, we found that city residents in the present study had better general/electronic health literacy than rural residents. One potential explanation may involve educational levels between urban and rural regions across countries17. Beauchamp et al. (2015)17 conducted their study in Australia, which has a well-established educational system to ensure that education quality is similar between urban and rural regions38. In contrast, the present study was conducted in Iran, which may have more barriers in improving quality education in rural areas39. Potentially as a result, rural residents in the present study had poorer general and electronic health literacy than the city residents.
Limitations and implications for practice
Study limitations warrant mention. First, although this is a large-scale study with a cluster sampling method for participant recruitment, all participants were residing in Qazvin province. Therefore, the present sample is not representative of the general Iranian population; subsequently, the present findings may not generalize to Iran or other jurisdictions. Future studies should investigate other populations. Second, both general and electronic health literacy were assessed via self-report. Although both the HELIA and eHEALS are validated instruments with promising psychometric properties in Iranian samples34,36,37, some participants may have misestimated their general or electronic health literacy because of factors like social desirability. Third, this is a cross-sectional design study. Therefore, causal inferences should not be drawn. Apart from the limitations and future study directions, future studies may want to use both HELIA and eHEALS to examine the associations between different forms of healthy literacy and various health outcomes. For example, a recent study using the same set of the present data found that both general and electronic health literacy were associated with better mental wellbeing via the sleep hygiene behaviors14. Health literacy assessed using HELIA/eHELAS may thus also be examined with other health concepts, such as physical activity and physical health.
Conclusions
The present study found that Iranian people could be classified into five groups according to levels of general health literacy and three groups based on levels of electronic health literacy. People of female versus male gender, of younger versus older age, having higher versus lower educational levels, and living in cities (as compared with rural areas) had better general and electronic health literacy. Therefore, the Iranian government and other stakeholders focusing on improving the public health may wish to target males, older adults, people with low educational levels, and rural residents with respect to improving their health literacy.
Data availability
All data generated or analyzed during this study are included in this published article.
References
Bennett, I. M., Chen, J., Soroui, J. S. & White, S. The contribution of health literacy to disparities in self-rated health status and preventive health behaviors in older adults. Ann. Family Med. 7(3), 204–211 (2009).
Osborn, C. Y., Paasche-Orlow, M. K., Bailey, S. C. & Wolf, M. S. The mechanisms linking health literacy to behavior and health status. Am. J. Health Behav. 35(1), 118–128 (2011).
Hossain, M. I. et al. Determinants of regional prevalence and variations in handwashing practices among households in Bangladesh: An application of generalized mixed-effects model. Asian J. Soc. Health Behav. 5(3), 122 (2022).
Joveini, H., Malaijerdi, Z., Sharifi, N., Borghabani, R. & Hashemian, M. A theory-based educational intervention to promote behavior change and physical activity participation in middle-aged women: A randomized controlled trial. Asian J. Soc. Health Behav. 5(3), 93 (2022).
Lin, Y.-C. et al. Changes of health outcomes, healthy behaviors, generalized trust, and accessibility to health promotion resources in Taiwan before and during COVID-19 pandemic: Comparing 2011 and 2021 Taiwan Social Change Survey (TSCS) cohorts. Psychol. Res. Behav. Manag. 15, 3379–3389 (2022).
Soltani, R., Shamsi, M. & Moradi, A. Do perceived barriers, benefits, and severity have effect on mask-wearing habits during the coronavirus disease-2019 pandemic?. Asian J. Soc. Health Behav. 5(4), 186 (2022).
Schnitzer, A. E., Rosenzweig, M. & Harris, B. Health literacy: A survey of the issues and solutions. J. Consumer Health Internet 15(2), 164–179 (2011).
Nutbeam, D. & Kickbusch, I. Health promotion glossary. Health Promot. Int. 13(4), 349–364 (1998).
Mackert, M., Champlin, S. E., Holton, A., Muñoz, I. I. & Damásio, M. J. eHealth and health literacy: A research methodology review. J. Comput.-Mediat. Commun. 19(3), 516–528 (2014).
Norman, C. D. & Skinner, H. A. eHEALS: The eHealth literacy scale. J. Med. Internet Res. 8(4), e507 (2006).
Werts, N. & Hutton-Rogers, L. Barriers to achieving e-health literacy. Am. J. Health Sci. (AJHS) 4(3), 115–120 (2013).
Mitsutake, S., Shibata, A., Ishii, K. & Oka, K. Association of eHealth literacy with colorectal cancer knowledge and screening practice among internet users in Japan. J. Med. Internet Res. 14(6), e153 (2012).
Lin, C.-Y. et al. Mediated effects of insomnia, psychological distress and medication adherence in the association of eHealth literacy and cardiac events among Iranian older patients with heart failure: A longitudinal study. Eur. J. Cardiovasc. Nurs. 19(2), 155–164 (2020).
Alijanzadeh, M. et al. Sleep hygiene behaviours mediate the association between health/e-health literacy and mental wellbeing. Health Expect. 26, 2349–2360 (2023).
Xie, L. et al. Electronic health literacy and health-related outcomes among older adults: A systematic review. Prev. Med. 157, 106997 (2022).
Korkmaz Aslan, G., Kartal, A., Turan, T., Taşdemir Yiğitoğlu, G. & Kocakabak, C. Association of electronic health literacy with health-promoting behaviours in adolescents. Int. J. Nurs. Pract. 27(2), e12921 (2021).
Beauchamp, A. et al. Distribution of health literacy strengths and weaknesses across socio-demographic groups: A cross-sectional survey using the Health Literacy Questionnaire (HLQ). BMC Public Health 15(1), 1–13 (2015).
Özdemir, H., Alper, Z., Uncu, Y. & Bilgel, N. G. Health literacy among adults: A study from Turkey. Health Educ. Res. 25(3), 464–477 (2010).
Ansari, H., Almasi, Z., Ansari-Moghaddam, A. et al. Health literacy in older adults and its related factors: A cross-sectional study in Southeast Iran. Health Scope 5(4), (2016).
Cutilli, C. C. & Bennett, I. M. Understanding the health literacy of America: Results of the National Assessment of Adult Literacy. Orthop. Nurs. 28(1), 27–32 (2009).
Tavousi, M. et al. Health literacy in Iran: Findings from a national study. Payesh (Health Monitor) 15(1), 95–102 (2016).
Joveini, H., Rohban, A., Askarian, P., Maheri, M. & Hashemian, M. Health literacy and its associated demographic factors in 18–65-year-old, literate adults in Bardaskan, Iran. J. Educ. Health Promot. 8, 244–244 (2019).
Berens, E.-M., Vogt, D., Messer, M., Hurrelmann, K. & Schaeffer, D. Health literacy among different age groups in Germany: Results of a cross-sectional survey. BMC Public Health 16(1), 1–8 (2016).
Ghanbari, S., Majlessi, F., Ghaffari, M. & Mahmoodi, M. M. Evaluation of health literacy of pregnant women in urban health centers of Shahid Beheshti Medical University. Daneshvar Med. 19(6), 1–12 (2020).
Naghibi, A., Chaleshgar, M., Kazemi, A. & Hosseini, M. Evaluation of health literacy level among 18–65 year-old adults in Shahriar, Iran. J. Health Res. Community 3(2), 17–25 (2017).
Protheroe, J. et al. Health literacy, associated lifestyle and demographic factors in adult population of an English city: A cross-sectional survey. Health Expect. 20(1), 112–119 (2017).
Reisi, M. et al. The relationship between functional health literacy and health promoting behaviors among older adults. J. Educ. Health Promot. 3, 119–119 (2014).
Haerian, A., Moghaddam, M. H. B., Ehrampoush, M. H., Bazm, S. & Bahsoun, M. H. Health literacy among adults in Yazd, Iran. J. Educ. Health Promot. 4, 91–91 (2015).
Petersen, K. J., Qualter, P. & Humphrey, N. The application of latent class analysis for investigating population child mental health: A systematic review. Front. Psychol. 10, 1214 (2019).
Weller, B. E., Bowen, N. K. & Faubert, S. J. Latent class analysis: A guide to best practice. J. Black Psychol. 46(4), 287–311 (2020).
Karnowski V. Latent class analysis. Int. Encyclopedia Commun. Res. Methods 1–10 (2017).
Nylund, K. L., Asparouhov, T. & Muthén, B. O. Deciding on the number of classes in latent class analysis and growth mixture modeling: A Monte Carlo simulation study. Struct. Equ. Model. Multidiscip. J. 14(4), 535–569 (2007).
Henson, J. M., Reise, S. P. & Kim, K. H. Detecting mixtures from structural model differences using latent variable mixture modeling: A comparison of relative model fit statistics. Struct. Equ. Model. Multidiscip. J. 14(2), 202–226 (2007).
Alijanzadeh, M., Lin, C.-Y., Yahaghi, R. et al. Measurement invariance and differential item functioning of the health literacy instrument for adults (HELIA): A large-scale cross-sectional study in Iran. In Paper presented at: Healthcare (2022).
Pakpour, A. H. et al. Large-scale dataset on health literacy, sleep hygiene behaviors, and mental well-being in the general population of Qazvin, Iran. Data Brief 48, 109072 (2023).
Tavousi, M. et al. Development and validation of a short and easy-to-use instrument for measuring health literacy: The Health Literacy Instrument for Adults (HELIA). BMC Public Health 20, 1–11 (2020).
Lin, C.-Y., Broström, A., Griffiths, M. D. & Pakpour, A. H. Psychometric evaluation of the Persian eHealth Literacy Scale (eHEALS) among elder Iranians with heart failure. Eval. Health Prof. 43(4), 222–229 (2020).
Reagan, E. M. et al. Place matters: Review of the literature on rural teacher education. Teach. Teach. Educ. 80, 83–93 (2019).
Sajedifard, M. & Sajedifard, Z. High school students’ achievement goal adoption: Evidence from neglected rural high schools in Iran. Education 4(1), 58–64 (2022).
Acknowledgements
The authors are grateful to the study participants. This research was funded by research funds allocated by the Qazvin University of Medical Sciences.
Funding
Open access funding provided by Jönköping University.
Author information
Authors and Affiliations
Contributions
Conceptualization, MS.Y, M.A., R.Y. and A.H.P.; methodology, M.A., R.Y. and A.H.P.; software, J.R., N.Y., E.J., N.Sh and H.A.; validation, M.A., R.Y. and A.H.P.; formal analysis, MS.Y, A.H, A.H.P.; investigation, N.Z.,E.J., R.Y., R.F., M.Z., E.T.,Z.B, N.M., L.P., S.A., A.S., and M.A.; resources, A.H.P.; data curation, C.-Y.L. and A.H.P.; writing—original draft preparation, M.S.Y, C.-Y.L. and A.H.P.; writing—review and editing, A.H.P., M.N.P.; visualization, C.-Y.L.; supervision, A.H.P.; project administration, R.Y., M.A., Z.B., J.R., H.A. and A.H.P.; funding acquisition, A.H.P. All authors read and agreed to the published version of the manuscript.
Corresponding authors
Ethics declarations
Competing interests
M.N.P. has consulted for Opiant Therapeutics, Game Day Data, Baria-Tek, the Addiction Policy Forum, AXA and Idorsia Pharmaceuticals; has been involved in a patent application with Yale University and Novartis; has received research support from Mohegan Sun Casino, Children and Screens and the Connecticut Council on Problem Gambling; has participated in surveys, mailings or telephone consultations related to drug addiction, impulse-control disorders or other health topics; has consulted for and/or advised gambling and legal entities on issues related to impulse-control, internet use and/or addictive disorders; has performed grant reviews for research-funding agencies; has edited journals and journal sections; has given academic lectures in grand rounds, CME events and other clinical or scientific venues; and has generated books or book chapters for publishers of mental health texts. The other authors report no disclosures.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Yekaninejad, M.S., Hajiheidari, A., Alijanzadeh, M. et al. Exploring health literacy categories among an Iranian adult sample: a latent class analysis. Sci Rep 14, 776 (2024). https://doi.org/10.1038/s41598-023-49850-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-49850-3
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
