
Abstract
Through anatomical morphology, to accumulate the relevant parameters of the A1 pulley of each adult finger. A total of 100 fingers were selected, dissected layer by layer, and the A1 pulley and neurovascular of each finger were observed. Measure the length of the A1 pulley, the distance between the needle knife insertion point and the proximal edge of A1 pulley, and the nerves and blood vessels on both sides. (1) The length of A1 pulleys of each finger is 6.18 ± 0.33 mm, 6.58 ± 0.73 mm, 5.98 ± 0.67 mm, 5.36 ± 1.08 mm, 5.63 ± 1.09 mm. (2) The distances between the needle knife entry point of each finger and the volar proper nerve of the ulnar finger are 7.00 ± 1.55 mm, 8.29 ± 1.46 mm, 5.10 ± 0.25 mm, 5.30 ± 0.24 mm, 0 mm; the distances from the volar proper nerve of the radial finger are 9.08 ± 0.87 mm, 4.70 ± 1.10 mm, 7.03 ± 0.72 mm, 6.81 ± 0.22 mm, 7.81 ± 0.57 mm. (3) The distances between the needle knife entry point of each finger and the proper volar artery of the ulnar finger are 10.40 ± 0.75 mm, 8.89 ± 0.53 mm, 6.35 ± 0.44 mm, 7.26 ± 0.16 mm, 0 mm, respectively; The distances from the volar proper artery of the radial finger are 8.75 ± 1.07 mm, 6.10 ± 0.35 mm, 11.44 ± 0.41 mm, 8.19 ± 0.60 mm, 9.78 ± 0.68 mm, respectively. The landmarks of the needle entry points are located at the position corresponding to the highest point of the metacarpal heads, except the tail finger. From the needle knife entry point to distal, cut the proximal edge of the A1 pulley longitudinally along the midline until the patient can flex autonomously, and pay attention to the distance between the two sides of 3.60–11.85 mm neurovascular bundle.
Similar content being viewed by others


Introduction
Trigger finger (TF), also called stenosing flexor tenosynovitis, can be described as a difference in diameters of the flexor tendon and the A1 pulley due to thickening and narrowing of the tendon sheath, located at the metacarpal head1. TF is one of the most common diseases of the hand occurring. The lifetime prevalence of adult population is approximately 2–3%2,3 and up to 20% in patients with diabetes4, and children is 0.05–0.33%5,6,7. It can occur at different ages and is mostly related to occupation. It is more common in manual labor and middle-aged women with the dominant hand being affected more often, also seen in infants8. The former is related to repeated mechanical stimulation, while the latter is mostly congenital. The most common finger is the thumb8.
The firtst-line treatment includes nonsteroidal anti-inflammatory medications, corticosteroid injections and splinting, and also includes Traditional Chinese Medicine such as acupuncture, massage, ointment therapy, and percutaneous release and open release1, which are very effective and are tailored to the severity and duration of symptoms. Surgical treatment is highly successful with low complication and recurrence rates for TF. However, percutaneous blind A1 pulley release is an alternative to the open release, but its risk–benefit relationship is under debate. Among them, ultrasound-guided percutaneous blind A1 pulley release is safer and more efficient, which is a new therapeutic trend9,10.
In this study, morphological anatomy and stereoscopic microscopy were used to observe the parameters of A1 pulley in 10 adult upper limb specimens, and needle knife treatment was simulated. To provide anatomical basis for needle knife therapy in the treatment of stenosing flexor tenosynovitis, and to improve the accuracy, effectiveness and safety of the treatment.
Materials and methods
The present study was performed in fresh frozen adult human cadavers that have been donated to the Department of Anatomy, Southern Medical University (SMU), Guangzhou through the Institutional body donation program following the ethical guidelines. The protocol for this research project was approved by the Biomedical Ethics committee, SMU, and informed consent was obtained from the donors. The study design involved the dissection of 20 preserved cadaver hands from the 20 adult upper extremities (Table 1). The study period was from April 2021 to December 2021. All specimens had intact hands, no deformity, no damage, and no history of surgery11.
Main reagents, instruments, and tools
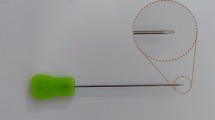
Pathological slicer (Shanghai Leica Instruments Co., Ltd.), stereomicroscope (Olympus SZ51-60); electronic vernier calipers (Accuracy 0.01 mm), ophthalmic scissors, ophthalmic forceps, scalpel, hemostatic forceps, skull gauge, marker, digital image acquisition (D610 camera, Nikon Corporation), image processing (photoshop 2020/Adobe Illustrator 2020, Adobe Corporation ), the needle knife ( Hanzhang Medical Instrument Co., Ltd., 1.2 × 50 mm) (Fig. 1).

The Hanzhang needle knife. The needle knife consists of three parts: tip, body, and handle, with a 1.2 mm blade on the tip, and a 50 mm length of the body.
Step 1
We straighten and separate the fingers of the specimen, fix the palm face upward with needles, mark the midline (M line) of the palm face of each finger with a marker, and locate the highest point of the metacarpophalangeal joint of each finger corresponding to the palm face with a craniometer, and intersect the midline of each finger. The point is recorded as the needle entry point (A point) (Fig. 2). Use a 5 ml syringe to draw emerald green dye, and inject a little dye solution at each needlepoint. Then, the 2nd to 4th fingers were dissected in turn, the skin was incised along the midline of the fingers, the soft tissues were separated layer by layer from superficial to deep, and soft tissues such as nerves, blood vessels, flexor tendons, and tendon sheaths were exposed, photographed and recorded.

Anatomical landmarks with needle entry point.
Step 2
Then, the tendon sheaths of each finger were removed. Then observed the general histological characteristics of the A1 pulley and the positional relationship between the needle insertion point and the proximal edge of the A1 pulley under a stereomicroscope.
Description of the measurement parameters
The A1 pulley, flexor tendon, and surrounding soft tissue structures were observed, and the following anatomical structures were measured using an electronic vernier caliper: the length (L) of the A1 pulley of each finger, and the distance between the midpoint of the proximal border of the A1 pulley and the volar proper nerves on both sides ( Ulnar side: N1, radial side: N2), the distance between the midpoint of the proximal border of the A1 pulley and the proper arteries on the palmar sides of the fingers on both sides (ulnar side: V1, radial side: V2), the distance (D) of the midpoint of the proximal border of the A1 pulley (B) (Fig. 3)and the needle entry point (A). The unit of distance is millimeters (mm).

Anatomy of A1 pulley and surrounding structures. Key structures were identified and visualized: C0 pulley, A2 pulley, flexor tendon, and neurovascular bundles.
Data analysis
Depending on the type of variable, mean values, SEM values, ranges, absolute frequencies, and percentages were recorded. Analysis of variance, the Chi-square test, and the paired t test were used to analyze differences. A 0.05 level of statistical significance was considered significant.
Informed consent statement
The protocol for this research project was approved by the Biomedical Ethics committee, SMU, and informed consent was obtained from the donors.
Results
The length of the A1 pulley
The general observation shows that the A1 pulleys of each finger are transverse fibers perpendicular to the flexor tendon, tough in texture, connected with synovial fibers at the proximal end, and difficult to distinguish, and connected with the oblique fibers at the distal end. The length of the A1 pulley of each finger is shown in Table 2. The A1 pulley of the index finger is the longest, and the A1 pulley of the ring finger is the shortest. And there was a statistically significant difference in the A1 pulley between the index finger and the tail finger (P = 0.015).
Palm landmarks of B (A1 pulley)
The distance (D) between A and B is shown in Table 3. B of the first to fourth fingers overlaps with A, while B of the little finger is (3.67 ± 0.54) mm on the radial side of A.
The distance between B and digit neurovascular bundles
Observation of anatomical specimens: two volar proper arteries of the thumb branched from the main artery of the thumb from below the A1 pulley, respectively wrapped around the inside of the sesamoid on both sides, and went to the end of the finger. Two volar proper nerves of the thumb run inside the corresponding arteries. Measure the distance between the midpoint of the proximal edge of the A1 pulley of each finger and the volar proper nerve and blood vessels on both sides of the finger, as shown in Table 4, except that B of the little finger overlaps with the ulnar digit volar proper nerve and blood vessel, the distance between the other fingers is 3.60 to 11.85 mm.
Observation of stereo microscope
Observed under the stereomicroscope (Fig. 4), the A1 pulley is a dense transverse fiber with a deep yellow dense connective tissue, and both ends are continuous with the synovial fibers. The synovial fibers are thin and translucent, and are loose connective tissue. At the far end is the pale yellow C0 pulley (cruciate pulley), which is also dense connective tissue. The needle entry points (emerald green marked point) of the 1st to 4th fingers are at the proximal edge of the A1 pulley, and the needle entry point of the tail finger is at the ulnar side of the proximal edge of the A1 pulley.

a-d are the A1 pulley of the 2nd to 5th fingers. Emerald green marked point on the proximal edge of the A1 pulley can be seen in the 2nd to 4th fingers (Original magnification ×7.8).
Discussion
Histological characteristics and adjacent relationship of the A1 pulley
Observed under a stereo microscope, the A1 pulley is a pale yellow dense transverse fiber whose ends are continuous with synovial fibers and difficult to distinguish.
Literature has shown that A1 pulley is composed of an outer layer and an inner layer12, in which the sliding layer in the inner layer has many fibrocartilage characteristics, and the friction layer in the inner layer contains chondrocytes, which is similar to the human synovial joint and can provide conditions for the sliding of the tendon. Our research also supports this conclusion.
In addition, studies have shown that increased pressure on connective tissue leads to fibrochondrogenesis13,14, and specifically friction leads to cartilage transformation in the sliding layer15. This suggests that the pathogenesis of TF may be due to the fibrochondrogenesis of A1 pulley caused by repeated friction, which leads to the difference in diameter of tendon sheath and flexor tendon, especially the stenosis of the proximal end of A1 pulley. Therefore, in clinical practice, TF is often cured by cutting the proximal end of A1 pulley, rather than all A1 pulley. Literature has shown that the success of the operation mainly depends on the complete or incomplete release of the proximal part of the A1 pulley, while the distal part of the A1 pulley is not necessarily related to the clinical outcome15.
Needle feeding position and depth
The success or failure of the percutaneous release of the TF depends on how to locate the starting point of the A1 pulley. In addition, the correct needle entry position can effectively avoid damage to the surrounding neurovascular bundles. However, we have found many papers lack precise parameters for the surface location of the A1 pulley16,17. Some kinds of literature suggest that the half distance (1/2 ab) between the transverse lines of the palmar fingers (a) and the transverse lines of the proximal interphalangeal joints (b), the needle entry position is at the proximal 1/2 ab of the transverse lines of the palmar fingers18,19,20. We choose the palm position corresponding to the highest point of the metacarpal head of each finger as the needle insertion point, in which the horizontal line of the metacarpophalangeal and the highest point of the metacarpal head of the thumb are at the same position, so the needle insertion point of the thumb is the intersection of the horizontal line of the metacarpophalangeal and the midline of the finger21. Our research shows (Table 2) that the A and B of the 1st to 4th fingers are the same, and the needle insertion point of the little finger is at the ulnar side of B (3.67 ± 0.54) mm. And research shows (Table 3), except that B of the little finger, overlaps with the ulnar digit volar proper nerve and blood vessel, the distance between the other fingers is 3.60 to 11.85 mm. The most dangerous place is the neurovascular bundle on the radial side of the index finger, and the closest distance is 3.60 mm. Strictly follow the needle insertion position and generally do not damage the neurovascular bundles on both sides22. In addition, for the depth of needle insertion, we suggest that the needle should be stopped after the needle tip touches the leather-like fibrosis, and the proximal edge of the A1 pulley can be cut. If it is too deep, the bursa and tendon will be cut, which theoretically will lead to tendon adhesion, which may increase the chance of recurrence, and straightening will lead to tendon rupture17.
Comparison of other treatments
A clinical study showed that in the short term, the percentage of pain and scarring was higher in open surgery than percutaneous release (P < 0.05), and the satisfaction was significantly worse (P < 0.05). Long-term, however, there were no significant differences in recurrence rates, pain, scarring, and satisfaction23. The literature suggests that the success rate of open release ranges from 60 to 97%24,25. The complication rate for open release, including digital nerve injury, infection, stiffness, weakness, scar tenderness, and bowstringing of the flexor tendons, ranges from 7 to 28%. The reported rate of infection and digital nerve damage is as high as 12%26,27,28. The success rate of percutaneous release is over 90%. Complications are rare but include digital nerve injury, bowstringing (if release extends into the A2 pulley), infection, hematoma, persistent pain, and flexor tendon injury17,29,30.
In addition, percutaneous release combined with splint immobilization can accelerate the recovery of interphalangeal joint flexion contracture15,31. And ultrasound can be used as a tool for better success by means of assisting the placement of the needle during percutaneous procedures. Therefore, needle knife percutaneous release under the guidance of ultrasound visualization may be the trend of the future10,32.
Steroid injection therapy is more effective for early TF. Notably, the literature showed that steroids injected into the subcutaneous tissue around the A1 pulley gave better clinical outcomes than that injected into the sheath alone33.
The major limitation of the present study is that cadavers might have altered landmarks and tissue turgor owing to soft tissue shrinkage or fluid shifts postmortem. Also, the presence of a nodule over the A1 pulley, a thickened pulley, or a history of triggering was not a requisite inclusion in this study. Further study is required to determine the usefulness of percutaneous release in the thumb.
Data availability
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
References
Makkouk, A. H. et al. Trigger finger: etiology, evaluation, and treatment. Curr. Rev. Musculoskelet Med. 1(2), 92–96 (2008).
David, M., Rangaraju, M. & Raine, A. Acquired triggering of the fingers and thumb in adults. BMJ 359, j5285 (2017).
Lunsford, D., Valdes, K. & Hengy, S. Conservative management of trigger finger: A systematic review. J. Hand Ther. 32, 212–221 (2019).
Kuczmarski, A. S., Harris, A. P., Gil, J. A. & Weiss, A. P. C. Management of diabetic trigger finger. J. Hand Surg. Am. 44, 152–153 (2019).
Ger, E., Kupcha, P. & Ger, D. The management of trigger thumb in children. J. Hand Surg. Am. 16, 944–947 (1991).
Rodgers, W. B. & Waters, P. M. Incidence of trigger digits in newborns. J. Hand Surg. Am. 19, 364–368 (1994).
Kikuchi, N. & Ogino, T. Incidence and development of trigger thumb in children. J. Hand Surg. Am. 31(4), 541–543 (2006).
Akhtar, S. et al. Management and referral for trigger finger/thumb. BMJ 331(7507), 30–33 (2005).
Rojo-Manaute, J. M. et al. Percutaneous intrasheath ultrasonographically guided first annular pulley release: anatomic study of a new technique. J. Ultrasound Med. 29(11), 1517–1529 (2010).
Pan, M. et al. Ultrasound-guided percutaneous release of A1 pulley by using a needle knife: A prospective study of 41 cases. Front. Pharmacol. 10, 267 (2019).
Zhong, W. X. et al. Morphometric study of percutaneous A1 pulley of thumb release. Sci. Rep. 12(1), 20944 (2022).
Sampson, S. P. et al. Pathobiology of the human A1 pulley in trigger finger. J. Hand Surg. Am. 16(4), 714–721 (1991).
Gillard, G. C. et al. The proteoglycan content and the axial periodicity of collagen in tendon. Biochem. J. 163(1), 145–151 (1977).
Gillard, G. C. et al. The influence of mechanical forces on the glycosaminoglycan content of the rabbit flexor digitorum profundus tendon. Connect Tissue Res. 7(1), 37–46 (1979).
Sbernardori, M. C., Mazzarello, V. & Tranquilli-Leali, P. Scanning electron microscopic findings of the gliding surface of the A1 pulley in trigger fingers and thumbs. J. Hand Surg. Eur. 32(4), 384–387 (2007).
Slesarenko, Y. A. et al. Percutaneous release of A1 pulley. Tech. Hand Up Extrem. Surg. 10(1), 54–56 (2006).
Eastwood, D. M., Gupta, K. J. & Johnson, D. P. Percutaneous release of the trigger finger: An office procedure. J. Hand Surg. Am. 17(1), 114–117 (1992).
Bain, G. I. et al. Percutaneous A1 pulley release: a cadaveric study. J Hand Surg Am 20(5), 781-784-785–786 (1995).
Wilhelmi, B. J. et al. Trigger finger release with hand surface landmark ratios: An anatomic and clinical study. Plast. Reconstr. Surg. 108(4), 908–915 (2001).
Fiorini, H. J. et al. Anatomical study of the A1 pulley: Length and location by means of cutaneous landmarks on the palmar surface. J. Hand Surg. Am. 36(3), 464–468 (2011).
Habbu, R., Putnam, M. D. & Adams, J. E. Percutaneous release of the A1 pulley: A cadaver study. J. Hand Surg. Am. 37(11), 2273–2277 (2012).
Hazani, R. et al. Safe treatment of trigger thumb with longitudinal anatomic landmarks. Eplasty 10(57), 476–479 (2010).
Wilhelmi, B. J. et al. Safe treatment of trigger finger with longitudinal and transverse landmarks: An anatomic study of the border fingers for percutaneous release. Plast. Reconstr. Surg. 112(4), 993–999 (2003).
Lin, C. J. et al. Open versus percutaneous release for trigger digits: Reversal between short-term and long-term outcomes. J. Chin. Med. Assoc. 79(6), 340–344 (2016).
Lapidus, P. W. & Guidotti, F. P. Stenosing tenovaginitis of the wrist and fingers. Clin. Orthop. Relat. Res. 83, 87–90 (1972).
Thorpe, A. P. Results of surgery for trigger finger. J. Hand Surg. Br. 13(2), 199–201 (1988).
Hodgkinson, J. P. et al. Retrospective study of 120 trigger digits treated surgically. J. R. Coll. Surg. Edinb. 33(2), 88–90 (1988).
Bonnici, A. V. & Spencer, J. D. A survey of “trigger finger” in adults. J. Hand Surg. Br. 13(2), 202–203 (1988).
Turowski, G. A., Zdankiewicz, P. D. & Thomson, J. G. The results of surgical treatment of trigger finger. J. Hand Surg. Am. 22(1), 145–149 (1997).
Pope, D. F. & Wolfe, S. W. Safety and efficacy of percutaneous trigger finger release. J. Hand Surg. Am. 20(2), 280–283 (1995).
Park, M. J., Oh, I. & Ha, K. I. A1 pulley release of locked trigger digit by percutaneous technique. J. Hand Surg. Br. 29(5), 502–505 (2004).
Yang, T. C. et al. Percutaneous A1 pulley release combined with finger splint for trigger finger with proximal interphalangeal joint flexion contracture. J. Hand Surg. Asian Pac. 24(3), 270–275 (2019).
Nikolaou, V. S. et al. Comparative clinical study of ultrasound-guided A1 pulley release vs open surgical intervention in the treatment of trigger finger. World J. Orthop. 8(2), 163–169 (2017).
Clark, D. D., Ricker, J. H. & MacCollum, M. S. The efficacy of local steroid injection in the treatment of stenosing tenovaginitis. Plast. Reconstr. Surg. 51(2), 179–180 (1973).
Funding
This work was supported by Innovation Team and Talents Cultivation Program of National Administration of Traditional Chinese Medicine (ZYYCXTD-C-202003), National Natural Science Foundation of China (82274669), President Foundation of The Third Affiliated Hospital of Southern Medical University (YP202210) and Sanming Project of Medicine in Shenzhen (SZZYSM202108013).
Author information
Authors and Affiliations
Contributions
W.Z., Z.C. and J.L. wrote the first draft and final version. Y.L. and C.C. offered suggestions and final revision. W.P. and R.G. collected the data and assisted in data analysis. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Zhong, Wx., Li, Jh., Chen, Zj. et al. Identification of the length and location of the A1 pulley combining palpation technique with palm landmarks: a cadaveric study. Sci Rep 13, 22801 (2023). https://doi.org/10.1038/s41598-023-49742-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-49742-6
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
