
Abstract
Sodium-glucose cotransporter type 2 (SGLT2) inhibitors have demonstrated to reduce cardiovascular risk in patients with type 2 diabetes mellitus (T2DM) in large trials independent of glycemic control. The mechanisms of this cardioprotective property remain uncertain. Evidence suggests positive hemodynamic changes and favorable cardiac remodeling contributing to the clinical outcomes but results were conflicting. We aim to investigate the potential impact on hemodynamic parameters, cardiac structure and functions. This prospective observational study included T2DM patients receiving canagliflozin 100 mg per day in addition to their antidiabetic treatment. We analyzed hemodynamic parameters assessed by echocardiographic measurements and impedance cardiography (ICG) to evaluate systolic and diastolic functions from baseline to 24 weeks after treatment. A total of 47 patients (25 males and 22 females) averaging 64.6 ± 10.9 years had a significant reduction in HbA1c, body weight, and systolic blood pressure. Hematocrit increased significantly, while NT-proBNP remained unchanged. E/e′, left atrium (LA) volume, and LA stiffness were reduced, while left ventricle (LV) global longitudinal strain (GLS) and LA strain rates increased at 24 weeks by conventional and speckle tracking echocardiography. LV mass and ejection fraction showed no differences. ICG suggested significant improvement in hemodynamic parameters with increased stroke volume index and cardiac output index and decreased systemic vascular resistance index at 12 and 24 weeks. Canagliflozin improved hemodynamic parameters and had a favorable impact on LA and LV reverse remodeling. These changes may explain the beneficial effect on cardiovascular outcomes in large clinical trials.
Similar content being viewed by others

Introduction
Sodium-glucose cotransporter type 2 (SGLT2) inhibitors are a novel class of oral diabetes drugs that block the reabsorption of glucose via SGLT2 in the proximal tubules of the kidneys, allowing glucose to be excreted in the urine, and achieve the therapeutic effect of lowering blood sugar1. Additionally, they reduce body weight, blood pressure, and uric acid level, independent of their hypoglycemic effects. Several SGLT2 inhibitors, such as empagliflozin, dapagliflozin, and canagliflozin, have been found to have cardiovascular benefits in large placebo-controlled clinical trials and are the first oral diabetes drugs that can reduce cardiovascular risk2, 3. In contrast, other hypoglycemic drugs like dipeptidyl peptidase-4 inhibitors (DDP4i) and thiazolidinediones are ineffective in cardiovascular risk reduction and are even associated with increased heart failure in patients with type 2 diabetes mellitus (T2DM).
The most significant and consistent cardiovascular outcome from SGLT2 inhibitors is the reduction of hospitalization for heart failure (HHF). Recent meta-analyses of cardiovascular outcome trials show a 32–33% reduction of HHF without heterogeneity, and this effect extends to patients without type 2 diabetes4, 5. EMPEROR-Preserved further demonstrates the benefits in patients with heart failure and a preserved ejection fraction (HFpEF) with a 29% lower risk of HHF with empagliflozin6. Moreover, SGLT2 inhibitors have impressive renal outcomes with improvement in albuminuria, declining kidney function, and renal death independent of glycemic control and the presence of diabetes7, 8.
Despite the cardiovascular benefits of SGLT2 inhibitors, the underlying mechanisms of action remain unclear and are to be elucidated. Several hypotheses have been postulated to explain these cardiorenal benefits, including diuresis effect, hemodynamic improvement, or augmented cardiac metabolism9, 10.
Impedance cardiography (ICG) is a convenient, non-invasive method to approximate valuable hemodynamic parameters and is often used in surgical and intensive care units to guide therapy11. It utilizes skin sensors placed on the neck and chest to measure changes in electrical conductivity within the thorax to calculate cardiac output, stroke volume, systemic vascular resistance (SVR), thoracic fluid status, and other contractility indexes12. Previous studies have demonstrated that ICG improved and predicted clinical outcomes in patients with acute and chronic heart failure13, 14. Several parameters measured by ICG also predicted mortality in the general population, even after adjustment for multiple confounders and blood pressure15.
Our observational study aims to assess the effect of canagliflozin on hemodynamic parameters measured by ICG and left ventricular functions evaluated by echocardiography in patients with T2DM. The results of this study will provide valuable insights into the mechanisms of action of SGLT2 inhibitors and their effects on cardiovascular and renal outcomes in patients with T2DM.
Methods
Study design
This prospective, single-center observational study was conducted at Hsinchu MacKay Memorial Hospital, a regional hospital in Northern Taiwan, to investigate the effect of canagliflozin on patients with T2DM. The study was approved by the Institutional Review Board of MacKay Memorial Hospital (Registration Number: 18MMHIS162e) and followed the principles of the Declaration of Helsinki. Each study participant provided informed consent. The enrolled patients with T2DM who were SGLT2 inhibitor-naive received canagliflozin 100 mg once daily in addition to previously prescribed antidiabetic agents. Physical examinations and hemodynamic monitoring were performed at baseline and in the 4th, 12th, and 24th weeks after administration of canagliflozin. Body weight and fat mass were measured using a commercially available scale with a bioelectrical impedance-based (BIA) body composition monitor (Tanita-305 Body-Fat Analyzer, Tanita Crop, Tokyo, Japan). Blood tests were conducted at baseline and in the 12th and 24th weeks, except for hs-CRP, aldosterone, and renin, which were measured at baseline and in the 24th week only. Echocardiography was performed at baseline and in the 24th week.
Participants
The target patient population was T2DM patients who had not taken any SGLT2 inhibitor prior to the study. These patients were recruited from outpatients at Hsinchu Mackay Memorial Hospital, Taiwan, and received standard care for T2DM during the study period. Other inclusion criteria were: (1) age ≥ 20 years old, (2) eGFR ≥ 30 mL/minute/1.73 m2, and (3) patients taking metformin alone or taking metformin and other antidiabetic drugs. The key exclusion criteria included: (1) patients with type 1 diabetes, (2) pregnant or breastfeeding patients, (3) New York Heart Association (NYHA) Class III and IV, (4) acute or chronic inflammatory disease, (5) patients who are allergic to canagliflozin and its excipients, and (6) severe obesity (BMI ≥ 40 kg/m2).
Echocardiography
Echocardiography was performed by a single trained sonographer blinded to clinical information using a commercially available ultrasound system (GE Vivid 7, GE Medical System, Vingmed, Norway). Standardized echocardiographic measurements were obtained according to the American Society of Echocardiography (ASE) recommendations. Left atrium (LA) and left ventricle (LV) volumes were obtained via the modified biplane Simpson method from the apical two- and four-chamber views. Diastolic function was assessed from early mitral inflow velocity (E), late mitral inflow velocity (A), deceleration time (DT), and tissue Doppler imaging (TDI)-derived mitral annular early diastolic velocity (E′) from LV septal and lateral segments. The mean values of septal and lateral E′ were reported in our tables.
LV and LA strains were assessed by speckle tracking analysis. Baseline 2D images were analyzed offline by manually tracing the endocardial border using proprietary software (version 10.8, EchoPAC, GE Vingmed Ultrasound, Norway). Based on automated speckle-tracking algorithms, LV global longitudinal strain (LV GLS) curves were obtained from the three standard apical views (long-axis, 4-chamber, and 2-chamber). Peak atrial longitudinal strain (PALS) and strain rate (SR) curves (systolic, early, and late diastolic LA strain rate [LA SRs, SRe, and SRa, respectively]) were generated for each atrial segment from apical 2- and 4-chamber views. The ratio of E/e′ to peak LA strain was used to estimate LA stiffness. Minor manual adjustment was used as necessary to ensure the best tracking quality. The absolute values of longitudinal strain (instead of negative values) were reported in this manuscript, and the corresponding tables and figures to avoid confusion regarding the directionality of the strain changes.
Hemodynamic monitoring
The non-invasive cardiac hemodynamic measuring instrument, AESCULON (OSYPKA Medical, USA), was used to provide the hemodynamic parameters. The device sends a low-amplitude, high-frequency electrical current through the thorax, and two sensors attached to the neck and another two to the left side of the thorax measure the changes in conductivity created by the circulatory system. The hemodynamic parameters were available after three minutes, and the report was printed for analysis. Table 3 contains the detailed variables evaluated in this study.
Statistical analysis
Data were expressed as mean ± stand deviation for continuous variables and numbers (%) for categorical variables. The comparison of each parameter before and after treatment with canagliflozin was calculated by paired sample t-test. All statistics were two-sided and statistically significant at p < 0.05.
Statistical analyses were performed using IBM SPSS Statistics for Windows, version 24.0 (IBMCorp., Armonk, NY, USA).
Ethics approval and consent to participate
The study was approved by the Institutional Review Board of MacKay Memorial Hospital (Registration Number: 18MMHIS162e).
Results
Baseline characteristics
From November 2019 to February 2021, 52 T2DM patients were included in the study, and five patients did not complete the study. Three stopped the medication because of adverse drug effects (1 due to dysuria, two due to palpitation), one could not have the examinations due to Covid travel restrictions, and one withdrew consent. Table 1 shows the clinical characteristics of the 47 patients analyzed at baseline.
The mean age of the participants was 64.6 ± 10.9 years. There were 25 (53%) males and 22 (47%) females. The mean body mass index (BMI) and fat content were 28.2 kg/m2 and 23.3 kg, respectively, indicating that the patients were overweight on average and some had a high body fat percentage. The majority of patients had a history of cardiovascular disease (95.7%), and most were taking antihypertensive medications and statins. The patient’s medications, including antihypertensives, diuretics, and antidiabetic agents, remained similar during the study period.
The mean weight changed from 74.1 ± 13.4 to 72.6 ± 13.8 kg, and the mean body mass index (BMI) 28.2 ± 4.3 to 27.6 ± 4.3 kg/m2, both statistically significant. However, the fat mass and ratio measured by BIA showed no difference 6 months after the administration of canagliflozin. Both fasting blood glucose level (141.2 ± 45.3–135.7 ± 57.9 mg/dL, p < 0.001) and HbA1c (7.5 ± 1.4–7.0 ± 1.0%, p = 0.008) showed a considerable drop. The mean hemoglobin (13.5 ± 1.4–14.1 ± 1.4 g/dL, p < 0.001) and hematocrit (40.1 ± 3.6–42.5 ± 4.1%, p < 0.001) increased at 6 months. The above changes were observed and statistically significant at 12 weeks and continued until the end of the study. There was a trend for reduction of microalbuminuria/creatine ratio, albeit statistically insignificant. No difference was seen in lipid profiles, renal functions, electrolytes, uric acid, levels of NT-proBNP, hs-CRP, renin, and aldosterone. Clinical changes are shown in Table 2.
Echocardiography
There were no significant differences in the LV mass, LV volume, LV ejection fraction, and cardiac output derived from echocardiography 24 weeks after the administration of canagliflozin (Table 3). Nevertheless, the LV diastolic function assessed by E/e′ ratio improved significantly (11.3 ± 3.2–9.1 ± 2.9, p < 0.001). LV global longitudinal strain (GLS), LV systolic and early strain rate (LVSRs and LVSRe) also significantly increased from 16.6 ± 2.8 to 18.0 ± 3.4 (p < 0.001), 1.08 ± 0.31 to 1.15 ± 0.35 (p = 0.013), and 0.90 ± 0.25 to 1.09 ± 0.31 (p < 0.001), respectively. Moreover, LA volume and LA stiffness decreased while LA systolic function assessed by PALS and LA strain rates increased with canagliflozin treatment at 24 weeks. Data are shown in Table 3.
Hemodynamic monitoring
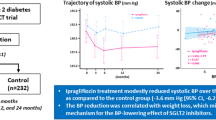
The hemodynamic parameters by ICG at baseline, 4 weeks, 12 weeks, and 24 weeks of canagliflozin are summarized in Table 4. The mean systolic blood pressure decreased significantly at 24 weeks (136.4 ± 15.4–130.7 ± 14.8 mmHg, p = 0.019). The average heart rate also dropped at 24 weeks from 75.0 ± 11.3 bpm to 71.5 ± 12.4 bpm (p = 0.003).
ICG parameters of blood flow and vascular system, including cardiac output, cardiac index, stroke volume, stroke index, and systemic vascular resistance index, showed significant improvement at 12 and 24 weeks after starting canagliflozin. The index of contractility (ICON™) increased significantly, but the other parameters of contractility, including left ventricular ejection time, pre-ejection time, and systolic time ratio, did not change. Unexpectedly, thoracic fluid content (TFC), which reflects the extravascular and intravascular fluid, increased from 24.6 ± 5.3 to 32.7 ± 7.1 k/Ω (p < 0.001).
Discussion
In this prospective study, canagliflozin significantly improved the hemodynamic parameters of blood flow, including stroke volume, stroke index, cardiac output, and cardiac index, as well as systemic vascular resistance by ICG. Furthermore, we observed the beneficial effects of canagliflozin on LV diastolic function and subtle improvement in LA and LV systolic functions evaluated by speckle tracking.
The mechanisms underpinning the overwhelming effect of cardiorenal protection by SGLT2 inhibitors are not yet fully understood. It is postulated that SGLT2 inhibitors may augment erythropoiesis and suppress sympathetic hyperactivity16,17,18, which are supported by the elevation of hematocrit and reduction of the resting HR and SVRI in this study. Elevated levels of erythropoietin (EPO) increased erythropoiesis and hematocrit and helped reduce the risk of heart failure and ischemic heart disease19, 20. The reduction of afterload by lowering blood pressure and decreasing vascular resistance likely contributed to the observed overall increase in hemodynamic parameters of blood flow, as well as the improvements in subclinical systolic functions. Studies have demonstrated that SGLT2 inhibitors can directly improver vascular function by inducing vasorelaxation and reducing endothelial cell dysfunction associated with atherogenesis21, 22. Moreover, the “fuel hypothesis” suggests that SLGT2 inhibitors increase ketone bodies, thereby optimizing cardiac energy metabolism and cardiac function may ameliorate the outcomes23, 24.
Elevated E/e′ is a valuable marker for diagnosing heart failure with preserved ejection fraction and predicting prognosis25. The decrease in E/e′, indicative of decreased LV filling pressure and diastolic function improvement, is a consistent finding observed in this and other SGLT2 inhibitors’ studies26,27,28. In the IDDIA trial, E/e′ only decreased significantly during exercise in T2DM patients with dapagliflozin29. The other echocardiographic parameters for diastolic function, including LV mass, LA volume, and E/A ratio, are less sensitive. MRI imaging also did not detect an apparent change in the LA or LV geometry30, 31. Nevertheless, our data from speckle tracking provided additional evidence suggesting beneficial effects on cardiac remodeling and function. LV GLS increased significantly while LVEF did not change, suggesting early and subclinical LV systolic improvement, which was similarly found in other studies32, 33. The administration of canagliflozin was also associated with significant improvement in LA strain indices and LA stiffness.
To our knowledge, few prior studies reported a comprehensive analysis of LA deformation with the administration of SGLT2 inhibitors. Decreased LA strain and increased LA stiffness have been strongly correlated with atrial fibrillation and adverse clinical outcomes in patients with heart failure with reduced EF (HFrEF) or HFpEF34, 35. However, our findings contradicted previous studies that found empagliflozin and dapagliflozin had no effect on any hemodynamic parameters evaluated by ICG in T2DM patients at 3 months and 12 weeks, respectively28, 36. Although all studies enrolled T2DM patients without overt heart failure, there were differences in baseline characteristics. Patients in our study were predominately female, had smaller BMIs, better diabetic control, greater reductions of SBP, and received less diuretic therapy. Additionally, the number of patients enrolled in these studies was limited.
Another possible explanation is that canagliflozin is more selective towards SGLT1 receptors, which are expressed abundantly in the distal proximal tubules of kidneys, the small intestine, and the cardiomyocytes. Suppression of SGLT1 can facilitate glucose uptake, decrease oxidative stress, reduce myocardial fibrosis and ventricular hypertrophy, and improve cardiac function37, 38. A previous study has shown oxidative stress was strongly associated with impaired myocardial performance and decreased GLS39. Dual SGLT1/2 inhibitor, sotagliflozin, has also been shown to reduce the overall risk of cardiovascular death, hospitalization for HF and emergent HF visit40, 41. Thus, the additional SGLT1 inhibition may potentiate the hemodynamic effect of canagliflozin.
Large clinical trials have recognized the effect of SGLT2 inhibitors in reducing the risk of hospitalization for heart failure, regardless of the presence of diabetes or glycemic control. Furthermore, SGLT2 inhibitors have been found to be effective in non-diabetic patients with HFrEF or HFpEF, who previously had no effective therapy6, 42,43,44. Our data suggest that positive cardiac remodeling, improved LV systolic and diastolic functions, and reduced systemic vascular resistance contribute to the broad therapeutic efficacy of SGLT2 inhibitors. Although it is postulated that SGLT2 inhibitors exert a diuretic effect that removes interstitial fluid to reduce the risk of HF, this effect is transient and modest and cannot account for the long-term outcome in clinical trials. In our study cohort, baseline measurements revealed normal level of Nt-proBNP and relatively low TFC. Interestingly, the level of Nt-proBNP did not decrease, and TFC even exhibited an elevation, despite positive hemodynamic changes observed after 6 months of canagliflozin treatment. These findings suggest that other mechanisms may be responsible for the therapeutic effect of SGLT2 inhibitors. The observed increase in TFC may be attributed to the counteracting mechanism of fluid regulation following the inhibition of SGLT2, as evident by the trending elevation in plasma renin activity45.
This study has several limitations. Firstly, the non-randomized, uncontrolled design affects the validity of our findings. Secondly, the small sample size and short follow-up duration may limit the generalizability of our results. A large randomized controlled trial is needed to confirm the positive hemodynamic effects of canagliflozin. The small percentage of patients with heart failure also made it difficult to detect the subclinical difference in some endpoints by conventional echocardiography over the 6-month period. Lastly, ICG utilizes the changes in electrical conductivity of the aortic arch blood flow detected by the skin sensors to estimate stroke volume and cardiac output46. A recent meta-analysis has indicated limitations in the inability of electrical cardiometry to measure absolute cardiac output values, and it may be applicable as a trend monitor if performed precisely47. Factors affecting the tissue and device conductivity, time and postural variability, and different algorithms may influence the calculated values. Nevertheless, our clinical and echocardiographic changes in response to canagliflozin treatment demonstrated favorable trends in positive cardiac remodeling, aligning with most available data in the literature.
Conclusions
This study suggests that canagliflozin has a positive impact on hemodynamics and cardiac function. Specifically, it increases cardiac index, reduces systemic vascular resistance, improves diastolic function, and promotes favorable LA remodeling. These findings may help explain the beneficial effects of SGLT2 inhibitors on cardiovascular outcomes.
Data availability
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- SGLT2i:
-
Sodium-glucose co-transporter-2 inhibitors
- T2DM:
-
Type 2 diabetes
- ICG:
-
Impedance cardiography
- GLS:
-
Global longitudinal strain
- HHF:
-
Hospitalization for heart failure
- HFrEF:
-
Heart failure with reduced EF
- HFpEF:
-
Heart failure with preserved EF
References
Clar, C., Gill, J. A., Court, R. & Waugh, N. Systematic review of SGLT2 receptor inhibitors in dual or triple therapy in type 2 diabetes. BMJ Open. 2(5), e001007 (2012).
Zinman, B. et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N. Engl. J. Med. 373(22), 2117–2128 (2015).
Neal, B. et al. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N. Engl. J. Med. 377(7), 644–657 (2017).
Teo, Y. N. et al. Effects of sodium/glucose cotransporter 2 (SGLT2) inhibitors and combined SGLT1/2 inhibitors on cardiovascular, metabolic, renal, and safety outcomes in patients with diabetes: A network meta-analysis of 111 randomized controlled trials. Am. J. Cardiovasc. Drugs 22(3), 299–323 (2022).
Giugliano, D. et al. SGLT-2 inhibitors and cardiorenal outcomes in patients with or without type 2 diabetes: A meta-analysis of 11 CVOTs. Cardiovasc. Diabetol. 20(1), 236 (2021).
Anker, S. D. et al. Empagliflozin in heart failure with a preserved ejection fraction. N. Engl. J. Med. 385(16), 1451–1461 (2021).
Perkovic, V. et al. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. N. Engl. J. Med. 380(24), 2295–2306 (2019).
Heerspink, H. J. L. et al. Dapagliflozin in patients with chronic kidney disease. N. Engl. J. Med. 383(15), 1436–1446 (2020).
Verma, S. & McMurray, J. J. V. SGLT2 inhibitors and mechanisms of cardiovascular benefit: A state-of-the-art review. Diabetologia 61(10), 2108–2117 (2018).
Kashihara, N., Kidokoro, K. & Kanda, E. Renoprotective effects of sodium-glucose cotransporter-2 inhibitors and underlying mechanisms. Curr. Opin. Nephrol. Hypertens. 29(1), 112–118 (2020).
Nguyen, L. S. & Squara, P. Non-invasive monitoring of cardiac output in critical care medicine. Front. Med. (Lausanne). 4, 200 (2017).
Cybulski, G., Strasz, A., Niewiadomski, W. & Gasiorowska, A. Impedance cardiography: recent advancements. Cardiol. J. 19(5), 550–556 (2012).
Packer, M. et al. Utility of impedance cardiography for the identification of short-term risk of clinical decompensation in stable patients with chronic heart failure. J. Am. Coll. Cardiol. 47(11), 2245–2252 (2006).
Shochat, M. K. et al. Non-invasive lung IMPEDANCE-guided preemptive treatment in chronic heart failure patients: A randomized controlled trial (IMPEDANCE-HF Trial). J. Card. Fail. 22(9), 713–722 (2016).
Medina-Lezama, J. et al. Hemodynamic patterns identified by impedance cardiography predict mortality in the general population: The PREVENCION study. J. Am. Heart Assoc. 7(18), e009259 (2018).
Sano, M. & Goto, S. Possible mechanism of hematocrit elevation by sodium glucose cotransporter 2 inhibitors and associated beneficial renal and cardiovascular effects. Circulation 139(17), 1985–1987 (2019).
Sano, M. A new class of drugs for heart failure: SGLT2 inhibitors reduce sympathetic overactivity. J. Cardiol. 71(5), 471–476 (2018).
Herat, L. Y. et al. SGLT2 inhibitor-induced sympathoinhibition: A novel mechanism for cardiorenal protection. JACC Basic Transl. Sci. 5(2), 169–179 (2020).
Mazer, C. D. et al. Effect of empagliflozin on erythropoietin levels, iron stores, and red blood cell morphology in patients with type 2 diabetes mellitus and coronary artery disease. Circulation 141(8), 704–707 (2020).
Guglin, M. E. & Koul, D. Cardiovascular effects of erythropoietin: Anemia and beyond. Cardiol. Rev. 14(4), 200–204 (2006).
Mancini, S. J. et al. Canagliflozin inhibits interleukin-1beta-stimulated cytokine and chemokine secretion in vascular endothelial cells by AMP-activated protein kinase-dependent and -independent mechanisms. Sci. Rep. 8(1), 5276 (2018).
Juni, R. P. et al. Cardiac microvascular endothelial enhancement of cardiomyocyte function is impaired by inflammation and restored by Empagliflozin. JACC Basic Transl. Sci. 4(5), 575–591 (2019).
Ferrannini, E., Mark, M. & Mayoux, E. CV protection in the EMPA-REG OUTCOME Trial: A “thrifty substrate” hypothesis. Diabetes Care 39(7), 1108–1114 (2016).
Verma, S. et al. Empagliflozin increases cardiac energy production in diabetes: Novel translational insights into the heart failure benefits of SGLT2 Inhibitors. JACC Basic Transl. Sci. 3(5), 575–587 (2018).
Nauta, J. F. et al. Correlation with invasive left ventricular filling pressures and prognostic relevance of the echocardiographic diastolic parameters used in the 2016 ESC heart failure guidelines and in the 2016 ASE/EACVI recommendations: A systematic review in patients with heart failure with preserved ejection fraction. Eur. J. Heart Fail. 20(9), 1303–1311 (2018).
Matsutani, D. et al. Effect of canagliflozin on left ventricular diastolic function in patients with type 2 diabetes. Cardiovasc. Diabetol. 17(1), 73 (2018).
Soga, F. et al. Impact of dapagliflozin on left ventricular diastolic function of patients with type 2 diabetic mellitus with chronic heart failure. Cardiovasc. Diabetol. 17(1), 132 (2018).
Rau, M. et al. Empagliflozin does not change cardiac index nor systemic vascular resistance but rapidly improves left ventricular filling pressure in patients with type 2 diabetes: A randomized controlled study. Cardiovasc. Diabetol. 20(1), 6 (2021).
Shim, C. Y. et al. Randomized, controlled trial to evaluate the effect of dapagliflozin on left ventricular diastolic function in patients with type 2 diabetes mellitus: The IDDIA trial. Circulation 143(5), 510–512 (2021).
Lee, M. M. Y. et al. Effect of empagliflozin on left ventricular volumes in patients with type 2 diabetes, or prediabetes, and heart failure with reduced ejection fraction (SUGAR-DM-HF). Circulation 143(6), 516–525 (2021).
Singh, J. S. S. et al. Dapagliflozin versus placebo on left ventricular remodeling in patients with diabetes and heart failure: The REFORM trial. Diabetes Care 43(6), 1356–1359 (2020).
Gamaza-Chulian, S. et al. Effect of sodium-glucose cotransporter 2 (SGLT2) inhibitors on left ventricular remodelling and longitudinal strain: A prospective observational study. BMC Cardiovasc. Disord. 21(1), 456 (2021).
Tanaka, H. et al. Positive effect of dapagliflozin on left ventricular longitudinal function for type 2 diabetic mellitus patients with chronic heart failure. Cardiovasc. Diabetol. 19(1), 6 (2020).
Freed, B. H. et al. Prognostic utility and clinical significance of cardiac mechanics in heart failure with preserved ejection fraction: Importance of left atrial strain. Circ. Cardiovasc. Imaging. 9(3), e003754 (2016).
Bytyci, I. et al. Speckle tracking-derived left atrial stiffness predicts clinical outcome in heart failure patients with reduced to mid-range ejection fraction. J. Clin. Med. 9(5), 1244 (2020).
Bonora, B. M., Vigilide Kreutzenberg, S., Avogaro, A. & Fadini, G. P. Effects of the SGLT2 inhibitor dapagliflozin on cardiac function evaluated by impedance cardiography in patients with type 2 diabetes. Secondary analysis of a randomized placebo-controlled trial. Cardiovasc. Diabetol. 18(1), 106 (2019).
Garcia-Ropero, A., Vargas-Delgado, A. P., Santos-Gallego, C. G. & Badimon, J. J. Inhibition of sodium glucose cotransporters improves cardiac performance. Int. J. Mol. Sci. 20(13), 3289 (2019).
Song, P., Onishi, A., Koepsell, H. & Vallon, V. Sodium glucose cotransporter SGLT1 as a therapeutic target in diabetes mellitus. Expert Opin. Ther. Targets 20(9), 1109–1125 (2016).
Cassano, V. et al. Oxidative stress and left ventricular performance in patients with different glycometabolic phenotypes. Nutrients 14(6), 1299 (2022).
Bhatt, D. L. et al. Sotagliflozin in patients with diabetes and recent worsening heart failure. N. Engl. J. Med. 384(2), 117–128 (2021).
Bhatt, D. L. et al. Sotagliflozin in patients with diabetes and chronic kidney disease. N. Engl. J. Med. 384(2), 129–139 (2021).
McMurray, J. J. V. et al. Dapagliflozin in patients with heart failure and reduced ejection fraction. N. Engl. J. Med. 381(21), 1995–2008 (2019).
Packer, M. et al. Cardiovascular and renal outcomes with empagliflozin in heart failure. N. Engl. J. Med. 383(15), 1413–1424 (2020).
Solomon, S. D. et al. Dapagliflozin in heart failure with mildly reduced or preserved ejection fraction. N. Engl. J. Med. 387(12), 1089–1098 (2022).
Schork, A. et al. Effect of SGLT2 inhibitors on body composition, fluid status and renin-angiotensin-aldosterone system in type 2 diabetes: a prospective study using bioimpedance spectroscopy. Cardiovasc. Diabetol. 18(1), 46 (2019).
Bernstein, D. P. A new stroke volume equation for thoracic electrical bioimpedance: Theory and rationale. Crit. Care Med. 14(10), 904–909 (1986).
Sanders, M., Servaas, S. & Slagt, C. Accuracy and precision of non-invasive cardiac output monitoring by electrical cardiometry: A systematic review and meta-analysis. J. Clin. Monit. Comput. 34(3), 433–460 (2020).
Funding
This study was supported by grant from Hsinchu MacKay Memorial Hospital (MMH-HB-10812).
Author information
Authors and Affiliations
Contributions
H.H.K. collected the data, performed the statistical analysis, and wrote the manuscript. Y.H.L. and P.L.L. acquired, analyzed and interpreted the data. H.C.C., C.L.H., C.K.Y. reviewed and edited the manuscript. L.Y.L. designed the study and revised the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kuo, HH., Lai, YH., Lin, PL. et al. Effects of canagliflozin on cardiac remodeling and hemodynamic parameters in patients with type 2 diabetes mellitus. Sci Rep 13, 21327 (2023). https://doi.org/10.1038/s41598-023-48716-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-48716-y
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
