
Abstract
Aging changes in the facial skeleton are concentrated mostly in orbits, maxilla and mandible. The aim of this study was to analyze metric traits of the adult viscerocranium in a medieval sample from Cedynia (Poland, Central Europe) and confront the results with literature data for modern populations. It was assumed that diet-related greater biomechanical forces generated during mastication in medieval versus modern times led to slower rate of bone resorption with age. 3D models of the facial skeleton are created for 230 individuals, categorized into young, middle and old adults, and a subgroup of edentulous middle adults is distinguished. Orbits, piriform aperture, maxilla and mandible are measured using Geomagic Studio 12 and analyzed among age categories as well as dentate and edentulous subgroups. The values of the orbital and piriform aperture measurements tend to increase with age and reached statistical significance in males (right orbit height, left orbit width, piriform aperture surface area). In females, maxillary height significantly decrease at right first premolar and first molar, together with height of the right mandibular ramus. In edentulous individuals of both sexes the orbits are wider, and maxillary and mandibular heights are lower than in dentate individuals. This study reveals similar character and direction of the aging process of the facial skeleton in medieval and modern adults, however slower rate of resorptive changes is found in the former sample, which suggests, that diet-related biomechanical forces can influence intensification of the aging processes in the facial skeleton.
Similar content being viewed by others


Introduction
Facial aging is a complex, multifactorial process that leads to changes in ligaments, muscles, adipose tissue, skin, and bones1. It represents a transition from youth, when the bone morphology and soft tissue envelope volume stay in balance, to the elderly, when this balance gets disturbed2. Skin undergoes atrophy with the reduction of collagen and weakening of the elastin structure. Muscles can undergo hypo- or hypertonicity. Also, the loss of facial fat compartments can occur. Bone structures, after reaching their peak bone mass, gradually lose their volume and density1. Involutional changes progress in separate tissues and together lead to the appearance of an aged face.
A better understanding of the facial aging process has been an object of multiple studies, but most of them have focused on changes occurring in soft tissues and how to surgically correct them3,4,5. Thus, facial aging mainly has been analyzed within medical sciences and hard tissue alterations have not been considered. Recent research, has found that aging also affects facial bones, and those changes significantly contribute to the appearance of an aging face6. Since the facial skeleton is a scaffolding for other tissues, resorption and volume loss of midface elements reflect weakened skeletal support7. In consequence, the elements of the facial skeleton most severely affected by resorption correspond with the most visible signs of aging8,9.
Bone tissue, like any other tissue, has its own metabolism, which gets disturbed in aging process. In normal conditions bone metabolism is defined by the balanced relationship between bone resorption and bone formation. At different stages of life this relationship may take on different values, favoring one of those phenomena. Bone formation is more intense during childhood, while in adulthood both processes stay in balance, and in the elderly resorption starts to dominate1,10. We know that involutional bone loss in the craniofacial skeleton is uneven and site specific. Structures most severely affected are: superomedial and inferolateral parts of orbital rim, piriform area of maxilla and the prejowl region of the mandible. The explanation of the mechanism of changes occurring in the facial skeleton with age was proposed by Sharabi et al.9. They formulated a hypothesis about the significant role of mechanotransduction in facial skeleton aging, which is the process of intercellular transduction of a mechanical signal into the effector cells—osteoblasts11. With age facial muscles are getting weaker and that results in decrease of mechanical stimulation of bone tissue. This signal received by bone tissue cells results in favoring bone resorption over bone formation, in accordance with the Wolff’s law. Indeed, several studies revealed that with age muscle quality deteriorates12,13 and medical and experimental research found a relationship between changes in craniofacial complex and ablation of facial muscles and nerves14,15. Numerous studies specifically showed a correlation between mastication muscles parameters and craniofacial morphology, concentrating mainly on the relationship between chewing muscle features (volume and cross-sectional area) and facial height and width (e.g.16,17,18).
Mechanical loading has been repeatedly shown to play a crucial role in modelling the cortical and trabecular bone tissue19. Some authors suggested that certain parts of the facial skeleton are prone to resorption related to aging in result of the lack of biomechanical stress9,20, which is in accordance with mechanotransduction hypothesis. Mendelson and Wong8 suggest that regions most susceptible to resorption are more mobile areas during facial animation. They focused on the orbital area and noted that muscles of this region must have less ligamentous fixation of the soft tissues to the bone because of their intensive movement. Therefore, it would explain why selective resorption is present in orbital rims. William and Slice20 have claimed that changes in superomedial part of the orbital rim may be related to enlargement of the frontal sinuses21. Enlow22 proposed an idea, which became widely accepted, that the craniofacial skeleton has a tendency to expand or enlarge with age. Applying cephalometry, he examined growth of the facial skeleton from infancy to adulthood and noted an increase in face length, width and depth8. Numerous studies have reported this trend also in adults in the process of aging, and using different anthropometric measurements revealed that the skull continuously expands in horizontal and vertical dimensions23,24,25. Shaw and Khan26 challenged the idea that facial aging is a process of volume loss and skeletal atrophy, from analyzing aging changes in specific regions of the facial skeleton. Since the beginning of the twentieth century, selective resorption in some areas of the facial skeleton has been confirmed (e.g.26,27,28,29). Application of new methods and technologies have had a great impact on growing understanding of the aging process8. However, involutional changes in the facial skeleton are still not entirely recognized, partly because of contradictory findings in the studies published so far. The character of changes and even the presence of the processes are still being questioned. This situation may be caused by several factors, including the variety of methods, as well as different age ranges, diverse ethnic background and various sampling methods of the examined persons30.
Changes occurring with age in soft and hard tissues are influenced to a variable degree by muscular function, genetics and environmental factors31,32,33. Additionally, jaw resorption can be moderated by tooth loss30. Those factors differ in the past in comparison to modern times, especially biomechanical forces, which are related to the texture and consistency of food. The medieval diet was composed of much more coarse, abrasive and unrefined foods and required longer and more powerful chewing34. Nowadays people consume highly processed products, and their diet is softer, therefore less energy must be put into mastication, which results in lower biomechanical forces affecting the masticatory apparatus35. Combing the knowledge about differences in diet in medieval and modern populations with the Wolff’s law, which describes the role of mechanical stimulation of the bone tissue and how bone responds to it, we can expect, that aging processes of the facial bones were different in the past than today. Differences should be most pronounced in the maxilla and mandible because of their straightforward relationship with chewing, but we have to bear in mind, that those biomechanical processes do not occur in isolation. Forces produced during mastication also affect other areas of the facial skeleton, including orbits and piriform aperture36. Those structures are also associated with aging of the viscerocranium. Greater biomechanical loads generated by the medieval diet could have a negative impact on aging processes of the facial bones.
The aim of this study is to identify changes associated with the aging process in the facial skeleton in a medieval sample from the territory of present-day Poland and to evaluate if the nature and direction of those processes are consistent with publisheddata for modern populations. Considering that the maxilla is the bone most prone to resorption, we also aim to test the hypothesis about diet-related slower resorption of maxillary height in medieval versus modern times.
Material
Material
Human skeletal remains used for the analysis was recovered from an archaeological proto-urban site in Cedynia, Poland. The socio-economic features of the site have been characterized elsewhere37. The human remains date from 10th to fourteenth century AD. The study embraced 230 skulls of adult individuals, males and females (Table 1), however some analyses included fewer number of individuals, because of post-mortem damage (see 4. Results). Two groups of individuals were included, differing in their dental status: dentate and edentulous. In the dentate group, each individual has been assigned to one of three age categories: young adult (YA), middle adult (MA), and old adult (OA). Additional selection criteria were applied to maxilla measurements, because of its height being affected by ante mortem tooth loss. To avoid such an influence, individuals with resorption at any measurements point were excluded from the analysis. Exception to this rule was the group of old adults, where cases with single ante mortem tooth loss were taken into consideration, because of low number of senile individuals with all teeth present prior to death. For all other measurements, the individuals with no more than a single ante mortem tooth loss in maxilla and mandible qualified for the study in the dentate group.
The edentulous group embraced those individuals who had lost all of their teeth during lifetime and displayed resorption of the entire alveolar process. This group was established to allow direct comparisons with living individuals, for whom the measurement data are available from the literature. As a result of low number of edentulous old adults in the osteological sample of Cedynia, this analysis was conducted for MA individuals with complete antemortem tooth loss.
Methods
Age and sex distribution
Sex assessment was performed based on cranial and pelvic features38. Age was assessed through pubic symphysis changes39 and dental wear40. As a complementary method, cranial sutures closure was used41.
3D Scanning
The skulls were scanned using a white light 3D ScanBright scanner (detector resolution up to 5 Mpix and point accuracy between 0.08 and 0.5 mm, www.smarttech3d.com) and Mesh3D software made by SMARTTECH, Poland to achieve three dimensional models of the facial skeleton. The point clouds created this way was cleaned and converted to 3D models using Geomagic Qualify 12 software (3D systems, USA).
Measurements
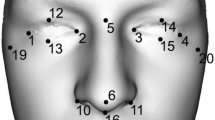
All measurements were taken by the first author of the study, with the use of Geomagic Qualify 12 software. Four elements of the facial skeleton: orbits, piriform aperture, maxilla and mandible were measured (Table 2 and Fig. 1). To maintain reproducibility of measurements while working on 3D models, the first step was to create two reference planes: the sagittal and Frankfort plane. To establish the sagittal plane, it was necessary to first determine anthropometric landmarks in the medial line of the skull (nasion, nasospinale and gnathion), and then to create the plane through connecting those points. The Frankfort plane was established through joining porion and two orbitale landmarks (Supplementary Table S1).

Measurements of facial skeleton: frontal view.
Orbits
Orbital breadth, height, X-axis and surface area were measured (Table 2). Additionally, the measurement of interorbital length was taken. To perform the remaining measurements of the orbits, a new plane was created. It had to be parallel to the Frankfort plane and go through the frontomalare orbitale point (fmo). This plane was then used to determine the location of the point d on the surface of the posterior lacrimal crest. Connecting those two landmarks (fmo-d) established the X-axis. This axis was then divided into ten equal segments (deciles), which resulted in nine measurement points located at equal intervals along the entire length of the X-axis (referred to as deciles from 10 to 90). Through every point a plane parallel to the sagittal plane was created. They were later used to locate points on the upper and lower edge of the orbit at their intersection. Using created points on X-axis and on orbital edges OB[s]10–90, Ob[i]10–90, OB[h]10–90 measurements could be performed (Table 2 and Fig. 2).

Orbital measurements: 10–90 deciles.
Piriform aperture
Linear measurements of height and breadth of the piriform aperture was performed. Surface area of the aperture was also measured (Table 2).
Maxilla
The height of the maxillary body was measured at midline, first premolar and first molar. Two last mentioned measurements were taken bilaterally. To take all measurements, the sagittal and Frankfort planes were used as reference planes. The next step was to establish the points on the alveolar process: between the two first incisors, and in the middle of the first premolar and molar sockets. The plains perpendicular to the or-or line were drawn through those points. At the intersection of those plains with the Frankfort plane, the points were located. Together with the points on the alveolar process, they were used to perform maxillary measurements (Table 2 and Fig. 3). The choice of the maxillary measurements was dictated by the measurements performed by other authors for modern populations, available from the literature.

Measurements of maxillary body height.
The availability of comparative data on edentulous and dentate individuals was used to determine the percentage reduction of the maxilla. This parameter was calculated in accordance with the formula (Eq. 1):
in which HoD is the height of the dentate maxilla and HoE is the height of the edentulous maxilla44.
The generated data were compared with publisheddata for modern populations. If authors have not calculated this parameter, it was determined based on the data included in their papers.
Mandible
Chin height, bigonial breadth and body length of the mandible were measured, together with maximum height and minimum breadth of both mandibular rami (Table 2 and Fig. 4).

Measurements of mandible.
Statistical analysis
Prior to performing statistical procedures, the outliers have been removed from the database to avoid their interference with the analysis. Non-parametric statistical tests were used: Kruskal–Wallis ANOVA to identify trends among age categories, and U-Mann–Whitney test to examine the differences between dentulous and edentulous individuals. To reveal potential differences between left and right side of the skull and in sex subgroups U-Mann Whitney test was performed. In order to show measurement sensitivity and specificity in sex assessment we applied ROC curves. Additionally, to detect fluctuating asymmetry in the examined skulls we calculated FA1 ([R − L|) and FA2 (|R − L|)/[(R + L)/2)] indices in accordance with the Palmer's classification45. Repeated measurements of vertical and horizontal parameters of orbits and piriform aperture were taken on 10 randomly chosen skulls by the same observer to establish the intraobserver error. Consequently, absolute differences for 6 measurements were taken into account (left and right OB-B and OB-H, PA-H, PA-B). To determine differences between repeated and initial measurements a Student's t test was applied. The statistical analyses were performed with Statistica (TIBCO Software Inc., USA), while for ROC curves SPSS Statistics (IBM, USA) was used.
Results
For almost all measurements, differences between the male and female group in the young and middle adult age categories were statistically significant, with males reaching higher values (Table 3). ROC curves analysis revealed that the highest values of the area under the ROC curve (AUC) were obtained for mandibular parameters. ROC curves, together with AUC, are presented in Supplementary Information (Supplementary Fig. S2 and Table S3). Measurements done for orbits, maxilla and mandible showed no significant difference between the left and right side both in females and males. Descriptive data for FA1 and FA2 indices are included in Table S4 (Supplementary Table S4). Intraobserver error calculated for repeated measurements was as follows: 0.32 (left OB-B), 0.81 (right OB-B), 0.59 (left OB-H), 0.32 (right OB-H), 0.53 (PA-H), 0.22 (PA-B) and proved to be insignificant.
Age differences
Orbits
In males there was a statistically significant increase in values in older age categories for right OB-H and left OB-B between YA and OA groups. The remaining measurements in males except for OB-IT showed similar, but an insignificant tendency for greater values in older age categories. In females statistically significant differences have not been found and a non-statistically significant tendency for increasing the values with age was apparent only in the case of left and right OB-X, right OB-B and left OB-B. The increase was observed for all measurements between YA and MA groups but was not continued in OA group (Table 4).
In females, both left and right orbits distance from X-axis to the superior and inferior rim increased with age between YA and MA groups in every measured point. In males this tendency was observed only for measurements of the inferior segment of both orbits, but was continued through all age groups, while in the case of OB[s]10-OB[s]90 a reverse tendency was found.
In females, a statistically significant increase was present in points corresponding to the outermost elements of the superior orbital rim (OB[s]10-OB[s]30 and OB[s]80-OB[s]90). In males, a reverse tendency was found, while the observed decrease was statistically significant in the measurements taken at the superomedial part of the orbit (OB[s]10-OB[s]40) (Table 5).
Height at particular deciles showed a slight statistically significant increase in value for right OB[h]10 (YA vs. OA) and both sides in OB[h]20 for females (left-YA vs. MA, right-YA vs. OA) (Supplementary Table S5).
Piriform aperture
All measurements had higher values in older age groups for both sexes, except for PA-H in females, but the differences were statistically significant only in males in the case of PA-A (YA vs. OA) (Table 4).
Maxilla
All maxillary parameters decreased with age, besides left MX-P1 in females. Statistically significant differences were noticed only for females for right MX-P1 (YA vs. MA) and right MX-M1 (YA vs. OA) (Table 4).
Mandible
In both female and male groups, no changes in mandibular dimensions with age were noticed (Table 4). Mean values differed only slightly between age groups, except in females, where MD-RH significantly increased between YA and MA groups and decreased in OA group.
Differences between dentate and edentulous middle adults
For almost all maxillary measurements, differences between males and females were statistically significant in the edentulous group. Measurements for orbits, maxilla and mandible did not show a significant difference between the left and right side both in females and males.
Orbits
The measurements of the orbits tend to reach higher values in edentulous individuals. Most of the measured parameters show this pattern, except for left and right OB-A, and left OB-H in both sexes. Differences between dentate and edentulous individuals were statistically significant for OB-IT, left OB-B, right and left OB-X for females and OB-IT, right and left OB-A, and left OB-B for males (Table 6). Edentulous individuals tend to have lower values of the distance from X-axis to the superior and inferior orbital rim. Only in the case of the lateral part of the upper orbital ridge (60–90 deciles), higher values of this distance are present in both sex groups. In females, the results are statistically significant in both left and right OB[s]10-OB[s]20, and in males in the left OB[s]10-OB[s]30. For both groups statistically significant differences in distances to the inferior rim were noted in points corresponding to the medial part of the inferior orbital rim (OB[i]10-OB[i]30) (Table 7). A decrease in orbital height measurements for particular deciles in females was statistically significant for the superior part of the orbit (OB[h]10-Ob[h]30 for both sides). Measurements of the medial part of the orbital rims (OB[h]10–40 for left side and OB[h]10-Ob[h]20 for right) were statistically significant in males (Supplementary Table S6).
Piriform aperture
All measurements in both female and male group were lower in edentulous group except for PA-B in males but statistically insignificant (Table 6).
Maxilla
In males and females, a statistically significant decrease of all values between dentate and edentulous groups was noted (Table 6). In accordance with the formula described in the Material and Methods section, the percentage reduction of maxilla was calculated. For females, the values were 14.37% for midline, 14.96% for P1 and 15.28% for M1, and in males they were 7.76%, 12.53% and 13.58%, respectively.
Mandible
The majority of the mandibular measurements tended to decrease in edentulous group. It was statistically significant in females for right and left MD-RH and in males for MD-H (Table 6).
Discussion
Our research revealed the character and direction of the facial skeleton aging processes in the medieval sample and compared the metric data between the medieval sample and modern populations. To our knowledge, this is the first study which has examined facial skeleton changes associated with age in a past population. We also investigated alterations in the facial bones caused by the reduction of biomechanical forces during chewing, as represented by edentulism. The most important finding confirms that the total antemortem tooth loss influences the whole craniofacial complex, even in the orbital region, which has been very often overlooked. Our study is also one of a few analyses carried out entirely in three dimensions. Even though the obtained results give a consistent image of age-related changes, they must be treated with caution, due to the main limitations of our study—cross-sectional character and limited sample sizes (see “Limitations” section). A potential confounding factor of random environmental effects, which may manifest itself as fluctuating asymmetry46, has been considered here. However, the performed analysis of two FA indicators showed that this variable was negligible in our sample.
Craniofacial skeletal changes with age
Orbits
Left OB-B and right OB-H measurements in males showed a significant increase with age. Those results indicate that the orbits of medieval individuals increased in vertical and horizontal dimensions with age, which was caused by bone resorption of their rims, leading to an increase in orbital surface area. Those results are consistent with the data obtained for modern populations28,47,48,49,50,51,52. Although it should be noted that some authors failed to show significant changes with age in orbital parameters29,53 or even suggested a decrease in some orbital dimensions27,54,55. According to Karunanayake27 those contradictions arise from varying location of the measurements among researchers, which can be an important factor considering that resorption in orbital area is not homogeneous. In our study of the medieval population, values tended to increase with age for the medial (OB[s]10–30) and lateral (OB[s]80–90) parts of the upper rim. In males, upper edge measurements have an opposite trend, which was significant in its medial part (OB[s]10–40). For modern populations, it has been established that resorption in orbits occurs along their whole border, but superomedial and inferolateral parts manifest the greatest intensification of changes27,29,49. Our results suggest that upper rim resorption focused on two extreme areas (medial and distal). These changes in the medial part of the superior rim are consistent with living populations. However, the observed resorption in the lateral area of this edge is difficult to explain, because it has not been found in modern populations and this is the only element of the orbit in the immediate vicinity of the chewing muscles56. Decreased values in males suggests that changes in the area of the superior rim differ depending on sex. The lower edge changes had the same direction for both sexes, but an intensification of resorption in the lateral part of this edge found in living populations27,29,49 was not present in the examined sample at a statistically significant level. It is possible that those changes could not be demonstrated, because they manifest themselves late in life8, and the examined individuals were too young for this phenomenon to occur. However, it could be also attributed to stronger biomechanical forces associated with a medieval diet.
Piriform aperture
Our results suggest that piriform aperture edges are being resorbed with age, which causes an increase in its horizontal and vertical parameters. It is consistent with the results of other studies, which showed significant changes of this kind26,27,47,52,54,57,58. In our medieval sample, the only statistically significant result was the increase of the surface area in successive age groups. This suggests that changes with age in the medieval adults were less intense than in the present times, but the direction and character of changes are the same.
Maxilla
Maxilla undergoes resorption with age, accompanied by reduction of its vertical height. In our sample maxillary height tended to decrease, but observed differences were statistically significant only for right P1 and M1 measurements in females. The one-side significance of the results could suggest that the resorption was more prominent on the right side of the examined individuals because of the left side chewing preferences, and therefore higher biomechanical forces affecting this side of the maxilla, leading to reduction of the resorption rate. However, left and right side measurements in each age category showed no differences, so it cannot be confirmed. For modern populations, some authors reported that midfacial height increases with age59,58,61. Others showed that aging changes result in a reduction of maxillary parameters24,27,55. However, those studies differ in applied methodology from our study, and thus they cannot be directly compared.
Mandible
In the medieval population, the only significant result is the decreasing right ramus height in females. In modern individuals, the same tendency was observed by Shaw et al.62 and Parr et al.63, and the opposite by Garib64. Patterns of changes with age in the mandibular region are still unclear. Despite the similarities of taking measurements, the results are inconsistent. It is still debated if the mandible of elderly individuals is shaped only by tooth loss30 or if aging is a co-factor acting together with it62,63. Studies, which actually found the age effect on mandible, indicated different mandibular elements to be affected and different direction of aging processes (increase vs decrease of measurements’ values). Recent studies suggest that contradictory findings may result from varying methodology. Masticatory muscle strength was shown to correlate with the mandibular shape analyzed by geometric morphometry, and not by linear measurements64. Mendes65 proved that changes in shape occur with age and showed that males and females express different patterns of those changes. In females, they begin earlier and beside resorption in the vertical dimension in the anterior and inferior region, which similarly occurs in males, they are also present in the sagittal and lateral dimension.
Skull areas most susceptible to aging
The obtained results clearly confirm that with age come multiple changes in the craniofacial area, mainly consisting in specific site resorption, which is most intense in the orbits, piriform aperture and maxilla. With age, the margins of both the orbits and the piriform aperture resorb, which consequently leads to an increase in their surface area, and maxillary vertical height decrease. These changes contribute to the morphology of aging face, which is described by Mendelson and Wong8 as an increase of the orbital volume and surface causing deeper setting of the eyeballs in the elderly and drooping of the upper eyelids. Resorption in area of the piriform aperture and retraction of its lower part is responsible for weakening of the skeletal support for the soft tissues, which makes the nose appear longer. Bone loss is most intense in maxilla, because of mutual relationships of the age-related resorption and tooth loss. Intensively shrinking maxilla can significantly contribute to the nasolabial folds appearing, tear valleys (furrows located below the eye), or zygomatic eminence (a bulge in the form of a bag under the eye)6,8,62. The pattern of changes of the craniofacial skeleton with age as revealed in our medieval sample is presented in Fig. 5.

Intensification of aging changes in facial skeleton (the more intense the changes, the thicker the arrow).
Differences between dentate and edentulous individuals
Orbits
An increase in orbital parameters between dentate and edentulous individuals is marked mostly in the horizontal dimensions (OB-X and OB-B). It leads to reduction of interorbital distance in edentulous skulls in comparison to dentate group. A tendency for lower values in the edentulous group is present for superomedial (OB[s]10–30) and inferomedial and central (OB[i]10–50) parts of the rim. Until now, not much is known about the influence of edentulism on orbital region. Williams and Slice66 performed shape analysis in a modern population, which showed an association between edentulism and positioning of orbital rims: superior rim is orientated more posteriorly, and inferior rim more anteriorly, while the lateral orbital border moves superiorly and medial border inferiorly in edentulous skulls. It is possible that those changes have impacted the measured distance in the medieval sample.
Piriform aperture
A comparison of dimensions of the piriform aperture in dentate and edentulous individuals showed nonsignificant differences. This region of the facial skeleton is subject to biomechanical influences to a small extent, which has been already suggested by confirming its stability against influence of extrinsic and intrinsic factors that cause alterations of the craniofacial skeleton20,66,67.
Maxilla
In this study, all measurements of maxilla are statistically significant, which is consistent with analyzes performed in modern populations44,68,69. Maxillary reduction rate (see “Maxilla” section) varies from study to study. The discrepancies are most likely due to different criteria qualifying individuals to the edentulous group. Only Cangers and Celenk’s68 study distinguished between prosthesis users and non-users, which may be an important factor in alveolar process reduction70. Generally, the rate of maxillary reduction in examined medieval females and males (Fig. 6) has lower values in comparison with the living population. In the medieval population, bone loss is severe in area of posterior teeth, which is compatible with the results for modern populations44,69.

Mandible
A comparison of dentate and edentulous individuals in the examined population revealed a significant chin and ramus height reduction. Multiple studies have confirmed the relationship between tooth loss and the reduction of vertical parameters of the mandible30,44,63,68,69,71. Loss of teeth also causes shortening of the ramus height, which follows the widening of the gonial angle72. The proposed explanation for this phenomenon is a disequilibrium between the elevator and depressor muscles, with the dominant role of the latter or by the absence of the molar buttress73. However, it should be noted that other authors reported no correlation between tooth loss and mandibular ramus height30,63,73 or even observed its increase59.
Skull areas most affected by edentulism
The results of comparisons between dentate and edentulous individuals in this research are mainly consistent with previous studies. Most authors have focused on changes in masticatory apparatus because of its direct relationship with tooth loss, while Williams and Slicer66 performed a shape analysis of influence of edentulism on the facial skeleton. They showed that the weakening of biomechanical forces produced during the chewing process affects the whole facial skeleton. This has been supported by the present study (Fig. 7). Our results indicate that the changes associated with tooth loss are less severe in the medieval population from Cedynia compared to modern populations, most likely because the observed resorption processes are susceptible to the influence of biomechanical forces, and greater biomechanical loads generated by coarser diet reduced the resorption rate.

Intensification of changes caused by edentulism in facial skeleton (the more intense the changes, the thicker the arrow).
Limitations
The presented research is not without limitations. The most important concerns relate to the cross-sectional character of the research, which is inherent to skeletal samples. However, the examined osteological series is biologically and culturally homogeneous, as revealed by anthropological and archaeological data, and in the analyzed time period no significant socio-cultural and/or environmental changes occurred74,75, which, we believe, justifies our research. Additionally, it should be borne in mind, that comparative data of facial skeleton aging are scarce. Thus, contrasting our findings with modern data should be treated with caution, because of different ethnical background of the populations, which constituted the comparative database. As already suggested, facial aging processes may differ depending on the origin of the examined individuals76. Even the results obtained for similar ethnic groups by different authors are inconsistent.
Another difficulty relates to the small number of the oldest individuals in bioarchaeological samples, as ours. Studies of living populations include individuals over 80 years of age, which is almost impossible to acquire for past populations, due to relatively short lifespan and the difficulty in estimating age-at-death of individuals over 70 years of age, based on changes in bones and teeth. This results in limited comparability of age ranges applied in past and modern samples. Small number of old individuals can be a reason why some tendencies of changes were marked only between YA and MA groups and were not continued in OA groups. This also resulted in failure to show expected sex differences, while, generally, resorption is more intense in females, due to their hormone predispositions to bone loss77. In turn, scarcity of edentulous individuals made it difficult to indicate changes caused by reduction of biomechanical forces. Also, it was hard to obtain a satisfactory number of maxillary measurements at first molars, because most of them were lost during lifetime. This may result from poor dental status of females in past populations, partly caused by pregnancy and lactation78,79. During pregnancy the level of sex hormones increases, which is a factor predisposing to inflammatory changes in gums, and gingivitis in turn predisposes to tooth loss80,81.
Conclusions
Our research revealed that the character and direction of age-related changes in the facial skeleton are similar in the examined medieval sample and modern populations. The major change is associated with maxillary height decrease, which is accompanied by enlargement of the piriform aperture and orbits. Our findings, which are inconsistent with previous studies, relate to the specific areas of progressive resorption and direction of changes in orbits. The rate of craniofacial complex changes with age and their intensity is lower in the examined medieval sample in comparison with modern populations, and, as such, our results correspond with the theory of the role of mechanotransduction in the facial skeleton aging process. Our research also suggests that edentulism mainly leads to reduction of the maxillary and mandibular vertical dimension, together with widening of the orbits and shortening of the mandibular ramus in toothless individuals. It should be emphasized, however, that our results are preliminary and might be affected by limited sample sizes, thus it would be advisable to carry out similar analyzes on more numerous populations with greater number of old and edentulous individuals. To obtain reliable results such research should definitely involve 3D measurements, used in our study. Moreover, considering the complexity of changes in the facial skeleton, advanced 3D shape analysis would be particularly informative. Because of contradictory findings about aging of the facial skeleton, it is recommended that a rigorous methodical approach and unified measurement protocols must be adopted.
Data availability
The data that support the findings of this study are available from the corresponding authors upon reasonable request.
References
Avelar, L. E. T., Cardoso, M. A., Bordoni, L. S., De Miranda Avelar, L. & De Miranda Avelar, J. V. Aging and sexual differences of the human skull. Plast. Reconst. Surg. 5, e1297. https://doi.org/10.1097/GOX.0000000000001297 (2017).
Skomina, Z., Verdenik, M. & Hren, N. I. Effect of aging and body characteristics on facial sexual dimorphism in the Caucasian population. PLoS ONE 15, e0231983. https://doi.org/10.1371/journal.pone.0231983 (2020).
Furnas, D. W. Festoons, mounds, and bags of the eyelids and cheek. Clin. Plast. Surg. 20, 367–385. https://doi.org/10.1016/S0094-1298(20)31228-1 (1993).
Gosain, A. K., Klein, M. H., Sudhakar, P. V. & Prost, R. W. A volumetric analysis of soft-tissue changes in the aging midface using high-resolution MRI: implications for facial rejuvenation. Plast. Reconst. Surg. 115, 1143–1152. https://doi.org/10.1097/01.prs.0000156333.57852.2f (2005).
Lambros, V. Facial aging: a 54-year, three-dimensional population study. Plast. Reconst. Surg. 145, 921–928. https://doi.org/10.1097/PRS.0000000000006711 (2020).
Mendelson, B. C., Hartley, W., Scott, M., McNab, A. & Granzow, J. W. Age-related changes of the orbit and midcheek and the implications for facial rejuvenation. Aesthetic Plast. Surg. 31, 419–423. https://doi.org/10.1007/s00266-006-0120-x (2007).
Shaw, R. B. et al. Facial bone density: Effects of aging and impact on facial rejuvenation. Aesthet. Surg. J. 32, 937–942. https://doi.org/10.1177/1090820X12462865 (2012).
Mendelson, B. C. & Wong, C. H. Changes in the facial skeleton with aging: implications and clinical applications in facial rejuvenation. Aesthetic Plast. Surg. 36, 753–760. https://doi.org/10.1007/s00266-012-9904-3 (2012).
Sharabi, S. E., Hatef, D. A., Koshy, J. C., Hollier, L. H. Jr. & Yaremchuk, M. J. Mechanotransduction: the missing link in the facial aging puzzle?. Aesthetic Plast. Surg. 34, 603–611. https://doi.org/10.1007/s00266-010-9519-5 (2010).
Kloss, F. R. & Gassner, R. Bone and aging: effects on the maxillofacial skeleton. Exp. Gerontol. 41, 123–129. https://doi.org/10.1016/j.exger.2005.11.005 (2006).
Moss, M. L. The functional matrix hypothesis revisited. 1. The role of mechanotransduction. Am. J. Orthod. Dentofacial. Orthop. 112, 8–11. https://doi.org/10.1016/s0889-5406(97)70267-1 (1997).
Porter, M. M., Vandervoort, A. A. & Lexell, J. Aging of human muscle: structure, function and adaptability. Scand. J. Med. Sci. Sports 5, 129–142. https://doi.org/10.1111/j.1600-0838.1995.tb00026.x (1995).
Peyron, M.-A., Blanc, O., Lund, J. P. & Woda, A. Influence of age on adaptability of human mastication. J. Neurophysiol. 92, 773–779. https://doi.org/10.1152/jn.01122.2003 (2004).
Houston, K., Buschang, P. H., Iannaccone, S. T. & Seale, N. S. Craniofacial morphology of spinal muscular atrophy. Pediatr. Res. 36, 265–269. https://doi.org/10.1203/00006450-199408000-00020 (1994).
Sinsel, N. K., Opdebeeck, H. & Guelinckx, P. J. The effect of unilateral partial facial paralysis and muscle ablation on craniofacial growth and development: An experimental study in the rabbit. Plast. Reconst. Surg. 102, 1894–1912. https://doi.org/10.1097/00006534-199811000-00014 (1998).
Kitai, N. et al. Human masticatory muscle volume and zygomatico-mandibular form in adults with mandibular prognathism. J. Dent. Res. 81, 752–756. https://doi.org/10.1177/0810752 (2002).
Weijs, W. A. & Hillen, B. Correlations between the cross-sectional area of the jaw muscles and craniofacial size and shape. Am. J. Phys. Anthropol. 70, 423–431. https://doi.org/10.1002/ajpa.1330700403 (1986).
Boom, H. P. W. et al. A comparison of human jaw muscle cross-sectional area and volume in long- and short-face subjects, using MRI. Arch. Oral Biol. 53, 273–281. https://doi.org/10.1016/j.archoralbio.2007.08.013 (2008).
Figus, C. et al. Human talar ontogeny: Insights from morphological and trabecular changes during postnatal growth. Am. J. Biol. Anthropol. https://doi.org/10.1002/ajpa.24596 (2022).
Williams, S. E. & Slice, D. E. Regional shape change in adult facial bone curvature with age. Am. J. Phys. Anthropol. 143, 437–447. https://doi.org/10.1002/ajpa.21332 (2010).
Fatu, C., Puisoru, M., Rotaru, M. & Truta, A. M. Morphometric evaluation of the frontal sinus in relation to age. Ann. Anat. 188, 275–280. https://doi.org/10.1016/j.aanat.2005.11.012 (2006).
Enlow, D. H. The Human Face: An Account of the Postnatal Growth and Development of the Craniofacial Skeleton (Harper and Row, New York, 1968).
Akgül, A. A. & Toygar, T. U. Natural craniofacial changes in the third decade of life: a longitudinal study. Am. J. Orthod. Dentofacial. Orthop. 122, 512–522. https://doi.org/10.1067/mod.2002.128861 (2002).
Bartlett, S. P., Grossman, R. & Whitaker, L. A. Age-related changes of the craniofacial skeleton: an anthropometric and histologic analysis. Plast. Reconst. Surg. 90, 592–600. https://doi.org/10.1097/00006534-199210000-00007 (1992).
Behrents, R. G. Growth in the Aging Craniofacial Skeleton., (Center for Human Growth and Development, University of Michigan, Ann Arbor, 1985).
Shaw, R. B. & Kahn, D. M. Aging of the midface bony elements: A three-dimensional computed tomographic study. Plast. Reconst. Surg. 119, 675–681. https://doi.org/10.1097/01.prs.0000246596.79795.a8 (2007).
Karunanayake, M., To, M. D., Efanov, J. I. & Doumit, G. Analysis of craniofacial remodeling in the aging midface using reconstructed three-dimensional models in paired individuals. Plast. Reconst. Surg. 140, 448e–454e. https://doi.org/10.1097/PRS.0000000000003590 (2017).
Mustafa, A. et al. Morphometric study of the facial skeleton in Jordanians: A computed tomography scan-based study. Forensic Sci. Int. 302, 109916. https://doi.org/10.1016/j.forsciint.2019.109916 (2019).
Pessa, J. E. & Chen, Y. Curve analysis of the aging orbital aperture. Plast. Reconst. Surg. 109, 751–755. https://doi.org/10.1097/00006534-200202000-00051 (2002).
Ozturk, C. N. et al. Dentition, bone loss, and the aging of the mandible. Aesthet. Surg. J. 33, 967–974. https://doi.org/10.1177/1090820X13503473 (2013).
Enlow, D. H. Facial growth and development. IJOM 5, 7–10. https://doi.org/10.52010/ijom.1979.5.4.3 (1979).
Moss, M. L. & Salentijn, L. The primary role of functional matrices in facial growth. Am. J. Orthod. 55, 566–577. https://doi.org/10.1016/0002-9416(69)90034-7 (1969).
Pratt, J., Boreham, C., Ennis, S., Ryan, A. W. & De Vito, G. Genetic associations with aging muscle: A systematic review. Cells 9, 12. https://doi.org/10.3390/cells9010012 (2019).
Esclassan, R. et al. Dental caries, tooth wear and diet in an adult medieval (12th–14th century) population from Mediterranean France. Arch. Oral Biol. 54, 287–297. https://doi.org/10.1016/j.archoralbio.2008.11.004 (2009).
Harper, C. A comparison of medieval and modern dentitions. Eur. J. Orthod. 16, 163–173. https://doi.org/10.1093/ejo/16.3.163 (1994).
Endo, B. Distribution of stress and strain produced in the human facial skeleton by the masticatory force. J. Anthropol. Soc. Nippon 73, 123–136. https://doi.org/10.1537/ase1911.73.123 (1965).
Krenz-Niedbała, M. Did children in medieval and post-medieval Poland suffer from scurvy? Examination of the skeletal evidence. Int. J. Osteoarchaeol. 26, 633–647. https://doi.org/10.1002/oa.2454 (2016).
Buikstra, J. E. & Ubelaker, D. H. Standards for Data Collection from Human Skeletal reMains. (AR: Arkansas Archaeological Survey, 1994).
Todd, T. W. Age changes in the pubic bone. Am. J. Phys. Anthropol. 4, 1–70. https://doi.org/10.1002/ajpa.1330040102 (1921).
Lovejoy, C. O. Dental wear in the Libben population: Its functional pattern and role in the determination of adult skeletal age at death. Am. J. Phys. Anthropol. 68, 47–56. https://doi.org/10.1002/ajpa.1330680105 (1985).
Meindl, R. S. & Lovejoy, C. O. Ectocranial suture closure—A revised method for the determination of skeletal age at death based on the lateral-anterior sutures. Am. J. Phys. Anthropol. 68, 57–66. https://doi.org/10.1002/ajpa.1330680106 (1985).
Nikita, E. Osteoarchaeology: A guide to the macroscopic study of human skeletal remains. (Academic Press, 2016).
Moore-Jansen P. H. & Jantz R. L. A computerized skeletal data bank for forensic anthropology. (University of Tennessee, Knoxville, 1986)
Panchbhai, A. S. Quantitative estimation of vertical heights of maxillary and mandibular jawbones in elderly dentate and edentulous subjects. Spec. Care Dentist. 33, 62–69. https://doi.org/10.1111/j.1754-4505.2012.00301.x (2013).
Palmer, A. R. in Developmental Instability: Its Origins and Evolutionary Implications: Proceedings of the International Conference on Developmental Instability: Its Origins and Evolutionary Implications, Tempe, Arizona, 14–15 June 1993 (ed Therese Ann Markow) 335–364 (Springer Netherlands, 1994).
Mączka, G. et al. Symmetry and asymmetry of the antegonial notch. Symmetry 14, 1558 (2022).
Buziashvili, D., Tower, J. I., Sangal, N. R., Shah, A. M. & Paskhover, B. Long-term patterns of age-related facial bone loss in black individuals. JAMA Facial Plast. Surg. 21, 292–297. https://doi.org/10.1001/jamafacial.2019.0028 (2019).
Furuta, M. Measurement of orbital volume by computed tomography: Especially on the growth of the orbit. JJO 45, 600–606. https://doi.org/10.1016/S0021-5155(01)00419-1 (2001).
Kahn, D. M. & Shaw, R. B. Aging of the bony orbit: A three-dimensional computed tomographic study. Aesthet. Surg. J. 28, 258–264. https://doi.org/10.1016/j.asj.2008.02.007 (2008).
Ugradar, S. & Lambros, V. Orbital volume increases with age: A computed tomography-based volumetric study. Ann. Plast. Surg. 83, 693–696. https://doi.org/10.1097/SAP.0000000000001929 (2019).
Zhang, K. R., Chon, B. H., Hwang, C. J., Jellema, L. M. & Perry, J. D. Comparison of orbital volume in young versus senescent human skulls. Ophthalmic. Plast. Reconstr. Surg. 36, 139–143. https://doi.org/10.1097/IOP.0000000000001492 (2020).
Velemínská, J. et al. Age-related differences in cranial sexual dimorphism in contemporary Europe. Int. J. Legal. Med. 135, 2033–2044. https://doi.org/10.1007/s00414-021-02547-6 (2021).
Ching, J. A., Ford, J. M. & Decker, S. J. Aging of the adult bony orbit. J. Craniofac. Surg. 31, 1082–1085. https://doi.org/10.1097/scs.0000000000006311 (2020).
Cotofana, S. et al. The relationship between bone remodeling and the clockwise rotation of the facial skeleton: A computed tomographic imaging-based evaluation. Plast. Reconst. Surg. 142, 1447–1454. https://doi.org/10.1097/PRS.0000000000004976 (2018).
Feng, W.-J., Li, F.-W., Zhan, W.-F., Lin, F.-C. & Luo, S.-K. Three-dimensional analysis of age-related orbital and midfacial bone remodeling in Asians. Dermatol. Surg. 46, e139–e145. https://doi.org/10.1097/DSS.0000000000002399 (2020).
Arnaud-Brachet, M. et al. Could mastication modify the shape of the orbit? A scannographic study in humans. Surg. Radiol. Anat. 42, 63–67. https://doi.org/10.1007/s00276-019-02315-7 (2020).
Ozturk, C. et al. Craniometric analysis of the nasal skeleton and midface in Caucasian population. Eur. J. Plast. Surg. 40, 499–506. https://doi.org/10.1007/s00238-017-1303-1 (2017).
Paskhover, B., Durand, D., Kamen, E. & Gordon, N. A. Patterns of change in facial skeletal aging. JAMA Facial Plast. Surg. 19, 413–417. https://doi.org/10.1001/jamafacial.2017.0743 (2021).
Garib, D. et al. Cephalometric changes during aging in subjects with normal occlusion. J. Appl. Oral Sci. 29, e20210199. https://doi.org/10.1590/1678-7757-2021-0199 (2021).
Pecora, N. G., Baccetti, T. & McNamara, J. A. The aging craniofacial complex: A longitudinal cephalometric study from late adolescence to late adulthood. Am. J. Orthod. Dentofacial. Orthop. 134, 496–505. https://doi.org/10.1016/j.ajodo.2006.11.022 (2008).
West, K. S. & McNamara, J. A. Jr. Changes in the craniofacial complex from adolescence to midadulthood: A cephalometric study. Am. J. Orthod. Dentofacial. Orthop. 115, 521–532. https://doi.org/10.1016/s0889-5406(99)70274-x (1999).
Shaw, R. B. et al. Aging of the mandible and its aesthetic implications. Plast. Reconst. Surg. 125, 332–342. https://doi.org/10.1097/PRS.0b013e3181c2a685 (2010).
Parr, N. M., Passalacqua, N. V. & Skorpinski, K. Investigations into age-related changes in the human mandible. J. Forensic Sci. 62, 1586–1591. https://doi.org/10.1111/1556-4029.13475 (2017).
Sella-Tunis, T., Pokhojaev, A., Sarig, R., O’Higgins, P. & May, H. Human mandibular shape is associated with masticatory muscle force. Sci. Rep. 8, 6042. https://doi.org/10.1038/s41598-018-24293-3 (2018).
Costa Mendes, L. et al. Sexual dimorphism of the mandibular conformational changes in aging human adults: A multislice computed tomographic study by geometric morphometrics. PLOS One 16, e0253564. https://doi.org/10.1371/journal.pone.0253564 (2021).
Williams, S. E. & Slice, D. E. Influence of edentulism on human orbit and zygomatic arch shape. Clin. Anat. 27, 408–416. https://doi.org/10.1002/ca.22194 (2014).
Anton, S. C. Intentional cranial vault deformation and induced changes of the cranial base and face. Am. J. Phys. Anthropol. 79, 253–267. https://doi.org/10.1002/ajpa.1330790213 (1989).
Canger, E. M. & Celenk, P. Radiographic evaluation of alveolar ridge heights of dentate and edentulous patients. Gerodontology 29, 17–23. https://doi.org/10.1111/j.1741-2358.2010.00391.x (2012).
Xie, Q., Wolf, J. & Ainamo, A. Quantitative assessment of vertical heights of maxillary and mandibular bones in panoramic radiographs of elderly dentate and edentulous subjects. Acta Odontol. Scand. 55, 155–161. https://doi.org/10.3109/00016359709115409 (1997).
Parkinson, C. F. Similarities in resorption patterns of maxillary and mandibular ridges. J. Prosthet. Dent. 39, 598–602. https://doi.org/10.1016/s0022-3913(78)80066-3 (1978).
Mays, S. Resorption of mandibular alveolar bone following loss of molar teeth and its relationship to age at death in a human skeletal population. Am. J. Phys. Anthropol. 153, 643–652. https://doi.org/10.1002/ajpa.22465 (2014).
Joo, J.-K., Lim, Y.-J., Kwon, H.-B. & Ahn, S.-J. Panoramic radiographic evaluation of the mandibular morphological changes in elderly dentate and edentulous subjects. Acta Odontol. Scand. 71, 357–362. https://doi.org/10.3109/00016357.2012.690446 (2013).
Merrot, O. et al. Changes in the edentate mandible in the elderly. Surg. Radiol. Anat. 27, 265–270. https://doi.org/10.1007/s00276-005-0323-x (2005).
Juras, A. Etnogeneza Słowian w Świetle Badań Kopalnego DNA, Adam Mickiewicz University, (2012).
Malinowska-Łazarczyk, H. Cmentarzysko Średniowieczne w CEDYNI. (Muzeum Narodowe w Szczecinie, 1982).
Jeon, A. et al. Anatomical changes in the East Asian midface skeleton with aging. Folia Morphol. 76, 730–735. https://doi.org/10.5603/FM.a2017.0027 (2017).
Alswat, K. A. Gender disparities in osteoporosis. J. Clin. Med. Res. 9, 382–387. https://doi.org/10.14740/jocmr2970w (2017).
Han, K., Ko, Y., Park, Y.-G. & Park, J.-B. Associations between the number of natural teeth in postmenopausal women and duration of lactation: The 2010–2012 Korea National Health and Nutrition Examination Survey. Maturitas 85, 73–78. https://doi.org/10.1016/j.maturitas.2015.12.010 (2016).
Rundgren, Å. & Österberg, T. Dental health and parity in three 70-year-old cohorts. Commun. Dent. Oral. Epidemiol. 15, 134–136. https://doi.org/10.1111/j.1600-0528.1987.tb00500.x (1987).
Ziskin, D. E. & Nesse, G. J. Pregnancy gingivitis: History, classification, etiology. Am. J. Orthod. Dentofac. Orthop. 32, A390–A432. https://doi.org/10.1016/0096-6347(46)90140-8 (1946).
Hemalatha, V., Manigandan, T., Sarumathi, T., Nisha, A. & Amudhan, A. Dental considerations in pregnancy-a critical review on the oral care. J. Clin. Diagn. Res. 7(5), 948–953. https://doi.org/10.7860/JCDR/2013/5405.2986 (2013).
Acknowledgements
The work was supported in part by the grant ID-UB Initiative of Excellence—Research University (009/34/UAM/0007).
Author information
Authors and Affiliations
Contributions
A.W.: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing – original draft. M.K-N.: Conceptualization, Methodology, Supervision, Writing – review & editing, supervision. S.Ł.: Methodology, Visualization, Writing – review & editing, supervision.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Walczak, A., Krenz-Niedbała, M. & Łukasik, S. Insight into age-related changes of the human facial skeleton based on medieval European osteological collection. Sci Rep 13, 20564 (2023). https://doi.org/10.1038/s41598-023-47776-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-47776-4
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
