
Abstract
Coronavirus disease 2019 (COVID-19) in kidney transplant recipients is a subject of much debate and became of interest to nephrologists amidst the pandemic. The main concerns are the influence of the chronic use of immunosuppressive drugs, the viral-related risk of acute rejection, and the long-term outcome of allograft function. This single-center prospective study included kidney transplant recipients with COVID-19 infection. Patients were maintained on immunosuppressive regimens. The severity of disease was defined as oxygen saturation < 94%, the need for hospitalization and/or hemodialysis, the occurrence of acute kidney injury (AKI), and mortality. Seventeen patients (54.8%) required hospital admission, four patients needed hemodialysis (12.9%), twelve patients (38.7%) had AKI, and three patients died (9.7%). Oxygen saturation < 94% showed a positive correlation with the presence of diabetes (p value 0.031) and a negative correlation with the maintenance steroid dose (p value 0.046). A negative correlation existed between the need for hemodialysis and average Cyclosporin level (p value 0.019) and between the need for hospitalization and average Tacrolimus level (p value 0.046). Severity of disease was associated with the presence of lymphopenia (p value 0.042), the cumulative steroid dose (p value 0.001), increased serum levels of LDH (p value 0.010), Ferritin (p value 0.020), AST (p value 0.047), and ALT (p value 0.006) and D-dimer levels more than 0.5 mg/L (p value 0.038). This study highlighted that the immunocompromised state of renal transplant recipients may not be regarded as a disadvantage in the setting of COVID-19 infection. Studies on a larger scale are needed to validate these results.
Similar content being viewed by others

Introduction
It is undetermined whether COVID-19 infection in the transplant population has similar symptoms and outcomes compared to the immunocompetent population1. The study of the transplant population is warranted to investigate the impact of maintenance immunosuppressive therapy on COVID-19 infection2. Unfortunately, data on allograft function in kidney transplant recipients with COVID-19 infection is still limited3. Since in vitro studies of Calcineurin inhibitors with SARS-COV yielded promising results, it is essential to investigate COVID-19 outcomes in similar settings4. The present study aims to describe COVID-19 infection among Egyptian living-donor kidney transplant recipients and to highlight the impact of long-term immunosuppression on the severity and outcome of the infection.
Methods
This prospective study included living-donor kidney transplant recipients who tested positive for COVID‐19, from a single center in Cairo, Egypt, between March 20, 2020, and March 20, 2021. All procedures followed are per the Helsinki Declaration of 19645. This study was approved by the Department of Internal Medicine local ethical committee at Cairo University, Egypt.
Data collection
Demographic data (age, sex, BMI, comorbidities, duration of post-transplant follow-up and maintenance immunosuppression drug levels), clinical characteristics (presenting symptoms, examination findings, laboratory results, and chest C.T. results), medications during COVID-19 (antiviral, antibiotic, anticoagulation treatment, and oxygen therapy), complications (Acute Kidney Injury (AKI), hospitalization, hemodialysis and Intensive care unit (ICU) admission) and outcome (recovery or death) were recorded for all participants. Information about hospitalized patients was gathered by the inpatient team. Baseline kidney function was considered as the mean of the patient's last three serum creatinine results before COVID-19 infection. AKI was defined according to the Kidney Disease Improving Global Outcomes (KDIGO) guidelines6. Cyclosporine (CsA) drug level measurement was done 2 h post-dose (C2)7.
COVID‐19 diagnosis
Diagnosis of COVID-19 infection was based on clinical, laboratory, and radiological findings. Confirmation of diagnosis was made by real-time polymerase chain reaction assay of nasopharyngeal swabs and the complementing findings on a chest C.T. scan8,9. Laboratory investigations included a complete blood count, serum C-reactive protein, LDH, ferritin, basal INR, kidney and liver function tests, and electrolytes, D-dimer, CsA, or Tacrolimus (Tac) drug level.
Patients
Informed consent was obtained from all participants. Patients were diagnosed according to the severity of the disease as per the protocol issued by the Egyptian Ministry of Health and Population guidelines at the time10. Patients with mild disease, who have an oxygen saturation of more than 94% and no lung involvement on chest C.T., were followed up on an outpatient basis. Corticosteroid therapy was not prescribed for these patients. Indications for hospitalization were moderate to severe disease, characterized by oxygen saturation less than 94%, respiratory rate more than 30 /min, positive chest findings on C.T., or the need for hemodialysis. Cytokine storm was diagnosed by persistent fever, high CRP and ferritin levels, abnormal liver function tests, D-dimer >0.5mg/dL, lymphopenia, and thrombocytopenia. ICU admission was based on low oxygen saturation of less than 90%, Systolic Blood Pressure of less than 90 mm Hg, or dysfunction in multiple organs.
Early in the pandemic, the most commonly used drugs were hydroxychloroquine, protease inhibitors, and Azithromycin11. Later, only Remdesivir became approved for the treatment of COVID-1912. A contraindication to its use was an estimated glomerular filtration rate (eGFR) of less than 30 mL/min/1.73 m2. Hydroxychloroquine was administered orally at a dose of 400 mg twice a day for the first 2 days and then 200 mg twice a day for four days, with routine ECG monitoring. Azithromycin was administered orally at a dose of 500 mg once a day for the first 3 days, then 250 mg once daily for four days. The FDA warned of a threefold increase in CsA level with concomitant use of chloroquine13,14,15 and advised for dose reduction in the presence of renal impairment, with a maximum of 5 days of treatment. Chloroquine is also known to cause a prolonged QTc-interval. Therefore, ECG monitoring was done regularly to these patients, especially in cases of renal impairment16.
Steroids were administered to patients with an oxygen saturation < 94%. Patients with moderate or severe disease received Tocilizumab or Remdesivir treatment and were treated at isolation hospitals. The corticosteroids were administered as dexamethasone 6 mg or the oral equivalent in moderate cases and methylprednisolone 1 mg/kg/d together with Tocilizumab 4–8 mg/kg/d in 2 doses, 12 h apart, and Remedesivir 200 mg as a 1st dose then 100 mg/d for 5 days in severe cases17,18,19,20,21. Drug interaction with immunosuppressive drugs was revised. Antibiotic therapy was added in cases of bacterial infection22,23.
A D-dimer level of more than 0.5 mg/L was considered an indication of anticoagulation. Prophylactic-dose low-molecular-weight heparin or Enoxaparin 40 IU every 24 h were administered subcutaneously to critically ill patients. Renal dose adjustments were done when needed. On an outpatient basis, anticoagulation was administered as Apixaban 2.5 mg PO bid or Rivaroxaban 10 mg daily for 6 weeks24. The immunosuppressive regimen was restored after a month of infection after recovery.
Statistical analysis
Data were statistically described in terms of mean ± standard deviation (± SD), median and interquartile range, or frequencies (number of cases) and percentages when appropriate. A comparison of numerical variables between the study groups was done using the Mann–Whitney U test for independent samples. For comparing categorical data, Chi-square (χ2) test was performed. An exact test was used instead when the expected frequency is less than 5. The Correlation between variables was done using the Spearman rank correlation equation for non-normal variables/non-linear monotonic relation. A two-sided p value less than 0.05 was considered statistically significant. All statistical calculations were done using the computer program IBM SPSS (Statistical Package for the Social Science; IBM Corp, Armonk, NY, USA) release 22 for Microsoft Windows.
Results
Patient baseline characteristics
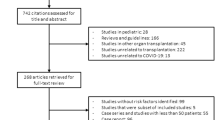
From March 2020 to March 2021, among kidney transplant recipients, 31 had confirmed COVID-19 infection, 18 males (58.1%) and 13 females (41.9%) with an age range of 30–78 years old and a range of 2–18 years duration after kidney transplantation. All had received a living-donor kidney transplantation. None of the patients received induction therapy.
Eight patients had diabetes (25.8%), 19 had hypertension (61.3%), and five patients had ischemic heart disease (16%). Patients were maintained on immunosuppressive regimens, 17 patients were on CsA (54.8%), 14 patients on Tac (45.2%), two patients on Azathioprine (6.4%), and 29 on Mycophenolate (93.5%). The average Tac level was 6.04 ± 1.083 ng/dL, while the average CsA level (C2) was 424.06 ± 89.437 ng/dL. The median serum creatinine was 1.65 (1.09–1.5). Demographic, laboratory characteristics and immunosuppression regimen of the participants are shown in Table 1.
Clinical presentation
During the COVID-19 infection, all patients had fever (100%), 24 had non-productive cough (77.4%), 15 had gastrointestinal symptoms (48.4%), 17 patients suffered a severe attack, with an oxygen saturation < 94% (54.8%), 26 patients had lymphopenia evident in the complete blood count (83.9%), 22 had a D-dimer > 0.5 mg/L (71%) and 29 (93.6%) of cases had a high CRP. Twelve patients were diagnosed with AKI (38.7%), 17 patients were hospitalized (54.8%), and four patients needed hemodialysis (12.9%).
Treatment
The general approach to immunosuppressive therapy was mycophenolate withdrawal only25.
Regarding the treatment regimen, 27 patients were treated with hydroxychloroquine (87.1%), 22 received anticoagulation (71%), 3 patients received antiviral treatment, Remdesivir (9.7%). Renal dose adjustment was not necessary since the eGFR of all recipients exceeded 30 mL/minute. No adverse drug effects were recorded. Drug interaction with the immunosuppressive drugs was revised, and no interaction was recorded. Those who were eligible for Remdesivir treatment were not receiving hydroxychloroquine concomitantly. One patient received Tocilizumab 4–8 mg/kg/d in 2 doses 12 h apart. Regarding anticoagulation, patients already on anticoagulant or antiplatelet therapies continued these medications. Patients with deep venous thrombosis were treated with therapeutic-dose anticoagulation. Patients treated on an outpatient basis received Rivaroxaban 10 mg daily. Inpatients were treated with Enoxaparin 40 IU subcutaneously every 24 for prophylaxis. Patients whose oxygen saturation was less than 92%, were given supplemental oxygen.
Outcomes
Regarding the outcome, 28 patients recovered (90.3%), while three patients died (9.7%). Improvement was confirmed on a clinical basis, normal follow-up C.T. and a twice-negative PCR. The median (IQR) follow-up (FU) creatinine after COVID-19 was 2.30 (1.1–1.9), Table 1.
Association and correlation studies with severity
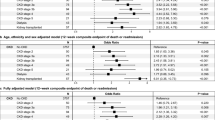
Correlation studies revealed a statistically significant positive correlation between oxygen saturation < 94% and the presence of diabetes (p value 0.031) and a statistically significant negative correlation with maintenance steroid dose (p value 0.046). There was a statistically significant negative correlation between the need for hemodialysis and the average CsA level (p value 0.019). A statistically significant negative correlation existed between the need for hospitalization and the average Tac level (p value 0.046).
In our study, oxygen saturation < 94%, the need for hospitalization, the development of AKI, and the need for hemodialysis were considered markers of severity. Patients were further stratified into two groups; 20 patients with severe disease and 11 patients without severe disease, based on the presence of any of these criteria as shown in Table 2.
Severity was associated with baseline creatinine (p value 0.007), the presence of lymphopenia (p value 0.042), the cumulative steroid dose (p value 0.001), increased serum levels of LDH (p value 0.010), Ferritin (p value 0.020), AST (p value 0.047), and ALT (p value 0.006) and D-dimer levels more than 0.5 mg/L (p value 0.038). Severity was not related to the number of years of transplantation.
Discussion
As stated by the Centers for Disease Control and Prevention (CDC), chronic immunosuppression, the presence of comorbidities, and repeated contact with the healthcare system predispose kidney transplant recipients to severe COVID-19 disease26, although they may be more easily diagnosed during regular follow-ups at the transplant centers27. Only a few studies examined the COVID-19 infection pattern in kidney transplant recipients, and ideal immunosuppression remains to be determined3.
The present study aims to describe the COVID-19 infection among kidney transplant recipients and examine its impact on kidney function, the development of AKI, and the relationship of maintenance immunosuppressive drugs to the outcome and severity of COVID-19 infection. Our study was conducted on 31 living-donor kidney transplant recipients; 25.8% had diabetes, 61.3% had hypertension, and 16% had ischemic heart disease, similar to the known characteristics of transplanted patients28.
Previous studies stated that symptoms of COVID-19 infection in this population may be somewhat different15,29. Fever, dry cough, and fatigue are the most common complaints. Some patients may also experience dyspnea, muscle pains, sore throat, and GIT symptoms30. In some cases, abdominal pain occurs before respiratory symptoms31 or atypical symptoms without respiratory symptoms32. A few other studies reported that symptoms in transplant recipients do not differ from immunocompetent cases33,34. In a study by Ng et al., 55% to > 80% were hospitalized35.
In our study, all patients complained of fever (100%), 24 had a non-productive cough (77.4%), 15 had gastrointestinal symptoms (48.4%), and two (3.2%) experienced DVT. Seventeen patients suffered a severe attack, with an oxygen saturation < 94% (54.8%), 26 patients had lymphopenia, evident in the complete blood count (83.9%), 22 had a D-Dimer > 0.5 mg/L (71%), and 29 (93.6%) had a high CRP. Regarding the outcome, 12 patients had AKI (38.7%), 17 patients were hospitalized (54.8%), four patients needed hemodialysis (12.9%), 28 patients recovered (90.3%), and three patients died (9.7%).
COVID-19 can affect the kidneys in many ways; AKI is one of the most common forms36, which has a direct effect on mortality37. The incidence of AKI was reported as high as 85% 38. AKI was reported as 39.9% with 6.6% requiring dialysis, in a large study of almost 9000 patients. In a study by Jewell et al., renal replacement therapy (RRT) was 29.3% in transplant patients versus 5.8% in the general population39. The main risk factors for AKI include old age, diabetes, the severity of respiratory symptoms, the use of mechanical ventilation, and pre-existing renal disease40. The outcome of AKI in COVID-19 infection is related to the balance between the viral infection and the immunosuppressive dose adjustment41. In our study, the development of AKI was not related to any of the studied parameters; age, gender, BMI, diabetes, hypertension, IHD, or immunosuppressive drug levels.
In renal transplant recipients, mortality was recorded as 18% and 43%, higher than in the general population42. Risk factors associated with mortality included advanced age, high viral load, and high inflammatory markers. None of the parameters related to immunosuppression had an association with mortality43. Some studies, on the contrary, revealed better survival with the use of cyclosporine44,45. In our study, mortality was not related to age, gender, BMI, diabetes, hypertension, IHD, or immunosuppressive drug levels.
In our study, the observation of increased levels of inflammatory markers such as ferritin and LDH among the patients who developed severe disease suggests a direct relationship between the magnitude of cytokine-release characteristics of COVID-19 and the risk and severity of disease in renal transplant recipients. The association between high D-dimer levels or the requirement for anticoagulant administration with disease severity aligns with the prothrombotic state observed in COVID-1946.
Disease severity was associated with lymphopenia which is in accordance with previous observations47.
The observed elevation of transaminases in the severe-disease group is in agreement with previous reports showing evidence of a correlation between the severity of COVID-19 infection and liver enzyme elevation. Liver cells express ACE2 receptors where SARS-CoV-2 can directly bind to ACE2-positive cells and disrupt liver functions. Other causes might be drug-induced or hypoxic liver injury and systemic inflammatory response48.
There is a statistically significant positive correlation between oxygen saturation < 94% and the presence of diabetes (p value 0.031). This is in agreement with many previous studies. Wu et al. stated that patients with diabetes, infected with COVID-19, are at a much higher risk for ICU admission and mortality. Mortality among diabetic patients with COVID-19 (7.3%) was higher in comparison with nondiabetic subjects (2.3%)49,50,51. Severity and mortality were associated with the glycemic ratio52,53,54,55,56. Lim et al. suggested that hyperglycemia modulates β-cell dysfunction and promotes endothelial dysfunction and increases the formation of advanced glycation end products57. It causes exaggerated inflammatory responses, decreased antiviral activity, and decreased T-cell activation50.
In our study, results showed a statistically significant negative correlation between oxygen saturation < 94% and maintenance steroid dose (p value 0.046). Some studies reported that the use of steroids is beneficial to patients with COVID-1958,59,60,61,62,63. Others showed that steroid use was associated with a higher risk of bloodstream infections and a lower recovery incidence64,65 and a delay in viral clearance66,67,68,69,70,71. Kidney transplant recipients are mostly maintained on maintenance steroid therapy, rendering them vulnerable during this pandemic72,73,74. Nevertheless, many transplant experts keep the steroid dose during COVID-19 infection, a practice that is supported by many studies including the: RECOVERY study, Metcovid, and CoDEX trials17,75,76,77. Administration of steroids was linked to fewer mortality rates in some studies75 and did not affect outcomes in other studies78.
Most studies, however, examined the role of therapeutic steroids in the treatment of COVID-19 in terms of dose, timing of administration, and type of steroid used. To our knowledge, this is one of the very few studies that evaluated the relationship between the maintenance of immunosuppressive drugs and the severity of COVID-19 infection.
A study by Hadi et al. stated that the spectrum of COVID-19 in kidney transplant recipients is related to the type of induction and immunosuppressive treatment72. Other studies argued against any role played by maintenance immunosuppressive drugs76. Corticosteroids control the intense immune response which is responsible for lung damage in COVID-19 patients17, by inhibiting pro-inflammatory cytokines, stimulation of apoptosis of T-lymphocytes, and reduction of leucocyte recruitment4,79. Nevertheless, increased susceptibility to infections during a pandemic is still a threat. The slow viral clearance, induced lung damage, and increased mortality are all underlying mechanisms. Patel et al., concluded that corticosteroid drugs are useful in COVID-19, with a few limitations80.
Results of our study also showed a statistically significant negative correlation between the need for hemodialysis and the average CsA level (p value 0.019). A statistically significant negative correlation between the need for hospitalization and the average Tac level (p value 0.046). Some studies suggest that immunosuppressive drugs could be harmful in the early phase of COVID-19 when an immune response is essential to guard against viral replication. On the other hand, immunosuppressive drugs might be of use, during the “cytokine storm62”. Schapiro et al. showed that wait-listed patients with COVID-19 needed more hospitalization, and had higher mortality, compared to a transplant group, on immunosuppressive therapy74. The evidence from the SARS and MERS outbreak shows that the immunocompetent and the immunocompromised have similar outcomes, regarding morbidity and mortality from COVID-1981. The RECOVERY trial concluded that the use of long-term immunosuppressive drugs for solid organ transplants carries no increased risk of mechanical ventilation or mortality, except for Rituximab24. Moreover, some studies proved the anti-viral properties of many immunosuppressive drugs, like Cyclosporine and mycophenolate against SARS-CoV82,83.
If lung affection in COVID‐19 is caused partly by overactive T cells, therefore, impairment in the function of T cells as in immunosuppression might decrease lung injury32.
CsA and TAC, in vitro, form complexes with cyclophilins and other binding proteins, decreasing the activation of T cells84. Cyclophilins alter cellular and viral proteins85, essential for viral replication83,84. Importantly, this effect is dose-dependent31,86,87,88. Both decrease interleukin‐2 production, which is essential for the survival of T cells89,90,91. Romanelli and Mascolo concluded that immunosuppressive medications might be a “protective factor” for serious COVID-1932. However, studies to demonstrate these effects in vivo are still lacking86,92,93,94.
Limitation
The main limitation of this study is the limited number of patients. Studies on a larger scale are needed to confirm the findings.
Conclusion
In summary, this prospective study discussed the COVID-19 infection in Egyptian renal transplant recipients. Severity was related to baseline serum creatinine, serum LDH, Ferritin, AST, ALT and cumulative steroid dose. The study also highlighted that the immunocompromised state of renal transplant recipients may not be regarded as a disadvantage in the setting of COVID-19 infection. A concept with a lot of controversy during this pandemic. A concept that is of value not only in COVID19 pandemic, but also in the study of future serious viral infections in immunocompromised patients. Studies on a larger scale are needed to validate these results.
Change history
19 December 2023
A Correction to this paper has been published: https://doi.org/10.1038/s41598-023-48743-9
References
Chang, L., Yan, Y., Wang, L. & Disease, C. Coronaviruses and blood safety. Transfus. Med. Rev. 34(2020), 75–80. https://doi.org/10.1016/j.tmrv.2020.02.003 (2019).
Lentine, K. L. et al. Survey of US living kidney donation and transplantation practices in the COVID-19 Era. Kidney Int. Rep. 5, 1894–1905. https://doi.org/10.1016/j.ekir.2020.08.017 (2020).
Demir, E. et al. COVID-19 in kidney transplant recipients: A multicenter experience from the first two waves of pandemic. BMC Nephrol. 23, 183. https://doi.org/10.1186/s12882-022-02784-w (2022).
Schoot, T. S., Kerckhoffs, A. P. M., Hilbrands, L. B. & van Marum, R. J. Immunosuppressive drugs and COVID-19: A review. Front. Pharmacol. 11, 1333. https://doi.org/10.3389/fphar.2020.01333 (2020).
Goodyear, M. D. E., Krleza-Jeric, K. & Lemmens, T. The declaration of Helsinki. BMJ. 335, 624–625. https://doi.org/10.1136/bmj.39339.610000.BE (2007).
Khwaja, A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin. Pract. 120, c179–c184. https://doi.org/10.1159/000339789 (2012).
Bączkowska, T. et al. Cyclosporine blood concentration at 2 hours (C2) from drug ingestion as the best single indicator of adequate cyclosporine immunosuppression in renal allograft recipients—A four-year follow-up. Transpl. Proc. 34, 556–557. https://doi.org/10.1016/s0041-1345(01)02844-5 (2002).
Kevadiya, B. D. et al. Diagnostics for SARS-CoV-2 infections. Nat. Mater. 20, 593–605. https://doi.org/10.1038/s41563-020-00906-z (2021).
Hanson, K. E. et al. The infectious diseases society of america guidelines on the diagnosis of COVID-19: Molecular diagnostic testing. Clin. Infect. Dis. https://doi.org/10.1093/cid/ciab048 (2021).
Ministry of Health and Population, Egyptian National Guidelines for COVID-19, (2020).
Gautret, P. et al. Hydroxychloroquine and azithromycin as a treatment of COVID-19: Results of an open-label non-randomized clinical trial. Int. J. Antimicrob. Agents. 56, 105949. https://doi.org/10.1016/j.ijantimicag.2020.105949 (2020).
Vijayvargiya, P. et al. Treatment considerations for COVID-19: A critical review of the evidence (or Lack thereof). Mayo Clin. Proc. 95, 1454–1466. https://doi.org/10.1016/j.mayocp.2020.04.027 (2020).
Nampoory, N., Nessim, J., Gupta, R. K. & Johny, K. V. Drug interaction of chloroquine with ciclosporin. Nephron 62, 108–109. https://doi.org/10.1159/000187007 (1992).
Finielz, P., Gendoo, Z., Chuet, C. & Guiserix, J. Interaction between cyclosporin and chloroquine. Nephron 65, 333. https://doi.org/10.1159/000187506 (1993).
Meziyerh, S. et al. Severe COVID-19 in a renal transplant recipient: A focus on pharmacokinetics. Am. J. Transpl. 20, 1896–1901. https://doi.org/10.1111/ajt.15943 (2020).
White, N. J. Cardiotoxicity of antimalarial drugs. Lancet Infect. Dis. 7, 549–558. https://doi.org/10.1016/s1473-3099(07)70187-1 (2007).
R.C. Group, P. Horby, et al. (2021) Dexamethasone in Hospitalized Patients with Covid-19. N. Engl. J. Med. 384, 693–704 DOI: https://doi.org/10.1056/NEJMoa2021436.
Bhimraj, A. et al. Infectious diseases society of america guidelines on the treatment and management of patients with COVID-19. Clin. Infect. Dis. 78, 478. https://doi.org/10.1093/cid/ciaa478 (2020).
Toapanta, N. et al. Kidney transplantation and COVID-19 renal and patient prognosis. Clin. Kidney J. 14, i21–i29. https://doi.org/10.1093/ckj/sfab030 (2021).
Strohbehn, G. W. et al. COVIDOSE: A phase II clinical trial of low-dose tocilizumab in the treatment of noncritical COVID-19 pneumonia. Clin. Pharmacol. Ther. 109, 688–696. https://doi.org/10.1002/cpt.2117 (2021).
Cattaneo, D. et al. Drug-drug interactions and prescription appropriateness in patients with COVID-19: A retrospective analysis from a reference hospital in Northern Italy. Drugs Aging. 37, 925–933. https://doi.org/10.1007/s40266-020-00812-8 (2020).
Buxeda, A. et al. Use and safety of remdesivir in kidney transplant recipients with COVID-19. Kidney Int. Rep. 6, 2305–2315. https://doi.org/10.1016/j.ekir.2021.06.023 (2021).
Andersen, K. M. et al. Long-term use of immunosuppressive medicines and in-hospital COVID-19 outcomes: A retrospective cohort study using data from the national COVID cohort collaborative. Lancet heumatol. 4, e33–e41. https://doi.org/10.1016/S2665-9913(21)00325-8 (2022).
Nugroho, J. et al. Relationship of D-dimer with severity and mortality in SARS-CoV-2 patients: A meta-analysis. Int. J. Lab. Hematol. 43, 110–115. https://doi.org/10.1111/ijlh.13336 (2020).
Favà, A. et al. Clinical characteristics and risk factors for severe COVID-19 in hospitalized kidney transplant recipients: A multicentric cohort study. Am. J. Transpl. 20, 3030–3041. https://doi.org/10.1111/ajt.16246 (2020).
Johnson, K. M., Belfer, J. J., Peterson, G. R., Boelkins, M. R. & Dumkow, L. E. Managing COVID-19 in renal transplant recipients: A review of recent literature and case supporting corticosteroid-sparing immunosuppression. Pharmacotherapy 40, 517–524. https://doi.org/10.1002/phar.2410 (2020).
Banerjee, D. et al. COVID-19 infection in kidney transplant recipients. Kidney Int. 97, 1076–1082. https://doi.org/10.1016/j.kint.2020.03.018 (2020).
Vivek, V. & Bhandari, S. Prevalence of modifiable cardiovascular risk factors in long-term renal transplant patients. Int. J. Nephrol. Renovasc. Dis. 3, 175–182. https://doi.org/10.2147/IJNRD.S13866 (2010).
Zhu, L. et al. Successful recovery of COVID-19 pneumonia in a renal transplant recipient with long-term immunosuppression. Am. J. Transpl. 20, 1859–1863. https://doi.org/10.1111/ajt.15869 (2020).
Baj, J. et al. COVID-19 specific and non-specific clinical manifestations and symptoms: The current state of knowledge. J. Clin. Med. 9, 1753. https://doi.org/10.3390/jcm9061753 (2020).
Sauerhering, L. et al. Cyclophilin inhibitors restrict the Middle East respiratory syndrome coronavirus via interferon-λ in vitro and mice. Eur. Respir. J. 56, 1901826. https://doi.org/10.1183/13993003.01826-2019 (2020).
Romanelli, A. & Mascolo, S. Immunosuppression drug-related and clinical manifestation of Coronavirus disease 2019: A therapeutical hypothesis. Am. J. Transplant. 20, 1947–1948. https://doi.org/10.1111/ajt.15905 (2020).
Xu, T. et al. Clinical features and dynamics of viral load in imported and non-imported patients with COVID-19. Int. J. Infect. Dis. 94, 68–71. https://doi.org/10.1016/j.ijid.2020.03.022 (2020).
Eastin, C. & Eastin, T. Clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 58, 711–712 (2020).
Ng, J. H., Zaidan, M., Jhaveri, K. D. & Izzedine, H. Acute tubulointerstitial nephritis and COVID-19. Clin. Kidney J. 14, 2151–2157. https://doi.org/10.1093/ckj/sfab107 (2021).
Gambella, A. et al. Spectrum of kidney injury following COVID-19 disease: Renal biopsy findings in a single italian pathology service. Biomolecules 12, 298. https://doi.org/10.3390/biom12020298 (2022).
da Costa, R. L. et al. Acute kidney injury in patients with Covid-19 in a Brazilian ICU: Incidence, predictors and in-hospital mortality. J. Bras. Nefrol. 43, 349–358. https://doi.org/10.1590/2175-8239-JBN-2020-0144 (2021).
Hirsch, J. S. et al. Acute kidney injury in patients hospitalized with COVID-19. Kidney Int. 98, 209–218. https://doi.org/10.1016/j.kint.2020.05.006 (2020).
Jewell, P. D. et al. Correction to: COVID-19-related acute kidney injury; incidence, risk factors and outcomes in a large UK cohort. BMC Nephrol. 22, 403. https://doi.org/10.1186/s12882-021-02617-2 (2021).
Cai, X., Wu, G., Zhang, J. & Yang, L. Risk factors for acute kidney injury in adult patients with COVID-19: A systematic review and meta-analysis. Front. Med. 8, 719472. https://doi.org/10.3389/fmed.2021.719472 (2021).
Nadim, M. K. et al. COVID-19-associated acute kidney injury: consensus report of the 25th acute disease quality initiative (ADQI) Workgroup. Nat. Rev. Nephrol. 16, 747–764. https://doi.org/10.1038/s41581-020-00356-5 (2020).
Mahalingasivam, V. et al. A systematic review of COVID-19 and kidney transplantation. Kidney Int. Rep. 6, 24–45. https://doi.org/10.1016/j.ekir.2020.10.023 (2021).
Herold, T. et al. Elevated levels of IL-6 and CRP predict the need for mechanical ventilation in COVID-19. J. Allergy Clin. Immunol. 146, 128-136.e4. https://doi.org/10.1016/j.jaci.2020.05.008 (2020).
Devresse, A. et al. Immunosuppression and SARS-CoV-2 infection in kidney transplant recipients, transplant. Direct 8, e1292–e1292. https://doi.org/10.1097/TXD.0000000000001292 (2022).
Yoo, J. et al. Admission NT-proBNP and outcomes in patients without a history of heart failure hospitalized with COVID-19. ESC Hear. Fail. 8, 4278–4287. https://doi.org/10.1002/ehf2.13548 (2021).
Mohamed, M. M. et al. Acute kidney injury associated with coronavirus disease 2019 in urban New Orleans. Kidney 1(7), 614 (2020).
Caillard, S. et al. Is COVID-19 infection more severe in kidney transplant recipients?. Am. J. Transpl. 21(3), 1295–1303 (2021).
Clark, R., Waters, B. & Stanfill, A. G. Elevated liver function tests in COVID-19: Causes, clinical evidence, and potential treatments. Nurse Pract. 46(1), 21 (2021).
Wu, Z. & McGoogan, J. M. Characteristics of and Important Lessons from the coronavirus disease 2019 (COVID-19) outbreak in China. JAMA 323, 1239. https://doi.org/10.1001/jama.2020.2648 (2020).
Viurcos-Sanabria, R. & Escobedo, G. Immunometabolic bases of type 2 diabetes in the severity of COVID-19, World. J. Diab. 12, 1026–1041. https://doi.org/10.4239/wjd.v12.i7.1026 (2021).
de Almeida-Pititto, B. et al. Severity and mortality of COVID-19 in patients with diabetes, hypertension, and cardiovascular disease: A meta-analysis. Diabetol. Metab. Syndr. 12, 75. https://doi.org/10.1186/s13098-020-00586-4 (2020).
Ramon, J. et al. Acute-to-chronic glycemic ratio as a predictor of COVID-19 severity and mortality. Diab. Care. 45, 255–258. https://doi.org/10.2337/dc21-1321 (2021).
Li, B. et al. Prevalence and impact of cardiovascular metabolic diseases on COVID-19 in China. Clin. Res. Cardiol. 109, 531–538. https://doi.org/10.1007/s00392-020-01626-9 (2020).
Onder, G., Rezza, G. & Brusaferro, S. Case-fatality rate and characteristics of patients dying in relation to COVID-19 in Italy. JAMA https://doi.org/10.1001/jama.2020.4683 (2020).
Gregory, J. M. et al. COVID-19 severity is tripled in the diabetes community: A prospective analysis of the pandemic’s impact in type 1 and type 2 diabetes. Diab. Care. 44, 526–532. https://doi.org/10.2337/dc20-2260 (2021).
Kumar, A. et al. Is diabetes mellitus associated with mortality and severity of COVID-19? A meta-analysis. Diabetes Metab. Syndr. 14, 535–545. https://doi.org/10.1016/j.dsx.2020.04.044 (2020).
Lim, S., Bae, J. H., Kwon, H.-S. & Nauck, M. A. COVID-19 and diabetes mellitus: from pathophysiology to clinical management. Nat. Rev. Endocrinol. 17, 11–30. https://doi.org/10.1038/s41574-020-00435-4 (2021).
Fadel, R. et al. Early short-course corticosteroids in hospitalized patients with COVID-19. Clin. Infect. Dis. 71(16), 2114–2120 (2020).
Fernández-Cruz, A. et al. A retrospective controlled cohort study of the impact of glucocorticoid treatment in SARS-CoV-2 infection mortality. Antimicrob. Agents Chemother. 64, e01168-e1220. https://doi.org/10.1128/AAC.01168-20 (2020).
Lu, X., Chen, T., Wang, Y., Wang, J. & Yan, F. Adjuvant corticosteroid therapy for critically ill patients with COVID-19. Crit. Care. 24, 241. https://doi.org/10.1186/s13054-020-02964-w (2020).
Sanz Herrero, F. et al. Methylprednisolone added to tocilizumab reduces mortality in SARS-CoV-2 pneumonia: An observational study. J. Intern. Med. 289, 259–263. https://doi.org/10.1111/joim.13145 (2021).
Wang, Y. et al. A retrospective cohort study of methylprednisolone therapy in severe patients with COVID-19 pneumonia. Signal Transduct. Target. Ther. 5, 57. https://doi.org/10.1038/s41392-020-0158-2 (2020).
Wu, C. et al. Risk factors associated with acute respiratory distress syndrome and death in patients with coronavirus disease 2019 pneumonia in Wuhan, China. JAMA Intern. Med. 180, 934–943. https://doi.org/10.1001/jamainternmed.2020.0994 (2020).
Giacobbe, D. R. et al. Bloodstream infections in critically ill patients with COVID-19. Eur. J. Clin. Invest. 50, e13319–e13319. https://doi.org/10.1111/eci.13319 (2020).
Mo, P. et al. Clinical characteristics of refractory coronavirus disease 2019 in Wuhan, China. Clin. Infect. Dis. 73, e4208–e4213. https://doi.org/10.1093/cid/ciaa270 (2021).
Chen, X. et al. Associations of clinical characteristics and treatment regimens with the duration of viral RNA shedding in patients with COVID-19. Int. J. Infect. Dis. 98, 252–260. https://doi.org/10.1016/j.ijid.2020.06.091 (2020).
Ling, Y. et al. Persistence and clearance of viral RNA in 2019 novel coronavirus disease rehabilitation patients. Chin. Med. J. Engl. 133, 1039–1043. https://doi.org/10.1097/CM9.0000000000000774 (2020).
Xu, K. et al. Factors associated with prolonged viral RNA shedding in patients with coronavirus disease 2019 (COVID-19). Clin. Infect. Dis. 71, 799–806. https://doi.org/10.1093/cid/ciaa351 (2020).
Zha, L. et al. Corticosteroid treatment of patients with coronavirus disease 2019 (COVID-19). Med. J. Aust. 212, 416–420. https://doi.org/10.5694/mja2.50577 (2020).
Zheng, C. et al. Risk-adapted treatment strategy for COVID-19 patients. Int. J. Infect. Dis. 94, 74–77. https://doi.org/10.1016/j.ijid.2020.03.047 (2020).
Shi, Y. et al. COVID-19 infection: The perspectives on immune responses. Cell Death Differ. 27, 1451–1454. https://doi.org/10.1038/s41418-020-0530-3 (2020).
Hadi, Y. B., Naqvi, S. F. Z., Kupec, J. T., Sofka, S. & Sarwari, A. Outcomes of COVID-19 in solid organ transplant recipients: A propensity-matched analysis of a large research network. Transplantation 105, 1365–1371. https://doi.org/10.1097/TP.0000000000003670 (2021).
Demir, E. et al. COVID-19 in kidney transplant recipients: A multicenter experience in Istanbul. Transpl. Infect. Dis. 22, e13371–e13371. https://doi.org/10.1111/tid.13371 (2020).
Craig-Schapiro, R. et al. COVID-19 outcomes in patients waitlisted for kidney transplantation and kidney transplant recipients. Am. J. Transpl. 21, 1576–1585. https://doi.org/10.1111/ajt.16351 (2021).
W.H.O.R.E.A. for C-19 T. (REACT) W. Group, J.A.C. Sterne, et al. Association between administration of systemic corticosteroids and mortality among critically Ill patients with COVID-19: A Meta-analysis. JAMA 324, 1330–1341 (2020) DOI: https://doi.org/10.1001/jama.2020.17023.
Jeronimo, C. M. P. et al. Methylprednisolone as adjunctive therapy for patients hospitalized with coronavirus disease 2019 (COVID-19; Metcovid): A randomized, double-blind, phase IIb, Placebo-controlled trial. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 72(1177), 373-e381. https://doi.org/10.1093/cid/ciaa1177 (2021).
Al-Otaibi, N. E. A review of the evidence for and against the use of steroids in renal transplant patients with COVID-19. Saudi Med. J. 42, 1149–1152. https://doi.org/10.15537/smj.2021.42.10.20210551 (2021).
Sahilu, T., Sheleme, T. & Melaku, T. Severity and mortality associated with steroid use among patients with COVID-19: A systematic review and meta-analysis. Interdiscip. Perspect. Infect. Dis. 2021, 6650469. https://doi.org/10.1155/2021/6650469 (2021).
Lansbury, L., Rodrigo, C., Leonardi-Bee, J., Nguyen-Van-Tam, J. & Lim, W. S. Corticosteroids as adjunctive therapy in the treatment of influenza. Cochrane Database Syst. Rev. 2, CD010406–CD010406. https://doi.org/10.1002/14651858.CD010406.pub3 (2019).
Patel, V. K. et al. Corticosteroids for treatment of COVID-19: Effect, evidence, expectation and extent. Beni Suef Univ. J. Basic Appl. Sci. 10, 78. https://doi.org/10.1186/s43088-021-00165-0 (2021).
Thng, Z. X. et al. COVID-19 and immunosuppression: A review of current clinical experiences and implications for ophthalmology patients taking immunosuppressive drugs. Br. J. Ophthalmol. 105, 306–310. https://doi.org/10.1136/bjophthalmol-2020-316586 (2021).
de Wilde, A. H. et al. Cyclosporin A inhibits the replication of diverse coronaviruses. J. Gen. Virol. 92, 2542–2548. https://doi.org/10.1099/vir.0.034983-0 (2011).
Al Ghamdi, M. et al. Treatment outcomes for patients with middle eastern respiratory syndrome coronavirus (MERS CoV) infection at a coronavirus referral center in the Kingdom of Saudi Arabia. BMC Infect. Dis. 16, 174. https://doi.org/10.1186/s12879-016-1492-4 (2016).
Ma, C., Li, F., Musharrafieh, R. G. & Wang, J. Discovery of cyclosporine A and its analogs as broad-spectrum anti-influenza drugs with a high in vitro genetic barrier of drug resistance. Antivir. Res. 133, 62–72. https://doi.org/10.1016/j.antiviral.2016.07.019 (2016).
Ma-Lauer, Y. et al. Influences of cyclosporin A and non-immunosuppressive derivatives on cellular cyclophilins and viral nucleocapsid protein during human coronavirus 229E replication. Antivir. Res. 173, 104620. https://doi.org/10.1016/j.antiviral.2019.104620 (2020).
Carbajo-Lozoya, J. et al. Replication of human coronaviruses SARS-CoV, HCoV-NL63 and HCoV-229E is inhibited by the drug FK506. Virus Res. 165, 112–117. https://doi.org/10.1016/j.virusres.2012.02.002 (2012).
Poulsen, N. N., von Brunn, A., Hornum, M. & Blomberg Jensen, M. Cyclosporine and COVID-19: Risk or favorable?. Am. J. Transplant. 20, 2975–2982. https://doi.org/10.1111/ajt.16250 (2020).
Li, H. S. et al. Effect of interferon alpha and cyclosporine treatment separately and in combination on middle east respiratory syndrome coronavirus (MERS-CoV) replication in a human in-vitro and ex-vivo culture model. Antivir. Res. 155, 89–96. https://doi.org/10.1016/j.antiviral.2018.05.007 (2018).
Xu, Z. et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet. Respir. Med. 8, 420–422. https://doi.org/10.1016/S2213-2600(20)30076-X (2020).
Aslam, S. & Mehra, M. R. COVID-19: Yet another coronavirus challenge in transplantation. J. Heart Lung Transplant. 39, 408–409. https://doi.org/10.1016/j.healun.2020.03.007 (2020).
Abadja, F., Atemkeng, S., Alamartine, E., Berthoux, F. & Mariat, C. Impact of mycophenolic acid and tacrolimus on Th17-related immune response. Transplantation 92, 396–403. https://doi.org/10.1097/tp.0b013e3182247b5f (2011).
Carbajo-Lozoya, J. et al. Human coronavirus NL63 replication is cyclophilin A-dependent and inhibited by non-immunosuppressive cyclosporine A-derivatives including Alisporivir. Virus Res. 184, 44–53. https://doi.org/10.1016/j.virusres.2014.02.010 (2014).
Cheng, K.-W. et al. Thiopurine analogs and mycophenolic acid synergistically inhibit the papain-like protease of middle east respiratory syndrome coronavirus. Antivir. Res. 115, 9–16. https://doi.org/10.1016/j.antiviral.2014.12.011 (2015).
Lin, M.-H. et al. Disulfiram can inhibit MERS and SARS coronavirus papain-like proteases via different modes. Antivir. Res. 150, 155–163. https://doi.org/10.1016/j.antiviral.2017.12.015 (2018).
Funding
Open access funding provided by The Science, Technology & Innovation Funding Authority (STDF) in cooperation with The Egyptian Knowledge Bank (EKB).
Author information
Authors and Affiliations
Contributions
Author contributions is as follows. Concept and design: M.S.E. Data acquisition: M.S.E. and K.M.S. Analysis and interpretation: M.S.E. and M.S.M.I. Article writing: M.S.E. and M.S.M.I. Revising: M.S.E., M.S.M.I. and K.M.S. Final approval: M.S.E. and K.M.S. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this Article was revised: The original version of this Article contained an error in Table 2, where the median (range) value was incorrect for ‘Cumulative steroid dose (mg)’ in the ‘Yes (n=20)’ column. Full information regarding the corrections made can be found in the correction notice for this Article.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
ElNahid, M.S., Issac, M.S.M. & Sadek, K.M. Outcome of COVID-19 in Egyptian living-donor kidney transplant recipients and relation to maintenance immunosuppressive drugs: a pilot study. Sci Rep 13, 19002 (2023). https://doi.org/10.1038/s41598-023-45750-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-45750-8
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
