
Abstract
A child’s body is highly sensitive to air quality, especially regarding the concentration of particulate matter (PM). Nevertheless, due to the high cost of precision instruments, measurements of PM concentrations are rarely carried out in school areas where children spend most of their daily time. This paper presents the results of PM measurements made by a validated, low-cost university air pollution measurement system operating in a rural area near schools. An assessment of children’s exposure to PM during school hours (8 a.m.–6 p.m.) at different times of the year was carried out. We show that PM10 concentrations in the air, particularly in winter, often exceeded the alert values of 50 µg m−3, posing a health risk to children, especially when children exercise outside the school building. We also calculated the rate and total PM10 deposition in the respiratory tract during various physical activities performed in clean and polluted air. Monitoring actual PM10 concentrations as presented in this paper, using a low cost sensors, offer school authorities and teachers an opportunity to reduce health risks for children. This can be achieved by adjusting the duration and exercise intensity of children’s outdoor physical activities according to the measured air quality.
Similar content being viewed by others

Introduction
Protecting the health of the population is an essential policy task for nations1, the European Union (EU)2, and worldwide3. Due to the high sensitivity to the impact of the environment, special attention must be paid to protecting the health of school children4. One of the key public health problems is currently exposure to high concentrations of particulate matter in ambient air, both in urban and rural populations.
Low-cost systems for monitoring the concentration of airborne particulate matter are made by government institutions5 and also are being developed at universities6, 7. Currently, almost every major city (e.g., in the EU8) possesses at least one air quality monitoring station provided by the government (state or local government)5. Unfortunately, highly accurate systems are too expensive to be purchased with available funds and for the needs of small communities. The use of low-cost measurement networks makes it possible to monitor air quality in smaller towns and villages, thereby reducing the technological exclusion of this mainly rural part of the population (e.g., the rural population comprised 40.1% of Poland’s total population in 2020)9.
The negative effects of particulate matter on human health are widely documented, with a particular focus on the harmful effects of the fine particles such as PM2.5 and PM1 on various tissues/organs of the human body10, 11. However, the most commonly measured indicator of air pollution worldwide is the PM10. Therefore, in this study we focus on this indicator in terms of its potential impact on children's health. It is worth noting that the particulate matter included in this indicator (PM10) also comprises particulate matter labelled as PM2.5, PM1, etc. For example, the PM2.5/PM10 ratio over the study area was ~ 0.82, as reported by Wilczyńska-Michalik and Michalik12 and Nieckarz and Zoladz7.
In this paper, we highlight a potential health hazard related to the outdoor physical activity of children conducted in polluted air. Results are reported of airborne particulate matter readings using the low-cost Storm&DustNet measurement network7. Measurements were taken near schools in several villages in the Małopolska (Lesser Poland) Province in Poland, and the degree of potential hazard to schoolchildren from the observed polluted air was assessed.
Materials and methods
Characteristics of measurements stations
In the present study, we measure air pollution, air temperature (T), humidity (H), and pressure (PR) utilizing university measuring stations (UMS). These stations belong to a low-cost air monitoring system that is part of the Storm&DustNet scientific project of Jagiellonian University in Kraków, Poland7. The UMS continuously measure the airborne mass concentration of particulate matter (PM), namely PM1, PM2.5, and PM10, and the concentration of suspended particulate matter (C) in five diameter ranges (0.3–0.5 µm, 0.5–1.0 µm, 1.0–2.5 µm, 2.5–5.0 µm, 5.0–10.0 µm). Samples are taken 30 times per minute, accumulated to obtain average values per minute, and transferred to a database server by wireless GSM technology. Finally, we analyzed the average values of concentrations calculated based on stored 1-min data. The UMS measure mass concentration with a precision of ± 9 µg·m−3 in a wide range of data (from a few up to 240 µg·m−3), while the levels of temperature, humidity, and pressure precision are ± 1 °C, ± 3% RH, and ± 1 hPa, respectively13.
UMS locations
Eleven UMS stations were mounted on buildings at a height of approximately 3 m above ground level. The UMS (labeled by letters: A, B, C, D, E, F, G, H, I, J, K) are distributed over the Małopolska Province in southern Poland. All selected places were away from highways and roads with heavy traffic. The study area was contained within a 6 × 10-km rectangle, with distances between stations ranging from 1.5 to 4 km. Particulate matter measurements were carried out over a period from 1 September 2018 to 31 August 2022 (1461 days) covering four heating periods in 11 locations. Station K was installed in a country town close to a primary school. The next eight stations were installed in villages close to primary schools (stations: A, B, D, E, F, G, H, I), and one was placed close to a nursery school (station C). An additional station (J) was installed as a background station in a village with a small population close to green areas where the building density was low.
Results
Dust hazards in the studied locations as places in everyday life
The analysis was carried out for both the entire 4-year period considered (1 September 2018 to 31 August 2022) and also for two separate periods: “cold” from October to March (X–III) and “warm” from April to September (IV–IX).
The highest values of average PM10 concentration over the overall period considered were recorded by stations K and A, equaling 43.1 µg·m−3 and 42.4 µg·m−3, respectively. Similarly, the highest mean concentration was recorded during the cold period, equaling 65.4 µg·m−3 and 65.3 µg·m−3 for stations K and A, respectively. The highest daily PM10 concentration occurred on 3 January 2021 in station A (328.8 µg·m−3).
On the other hand, throughout the period under review, the lowest average PM10 values were recorded by stations I and J, amounting to 28.7 and 29.0 µg·m−3, respectively. In all locations, the average PM10 value in the warm period did not exceed level 19 µg·m−3 (see Table 1).
In the analyzed period, each measuring station recorded several dozen days in each cold period during which PM10 concentrations exceeded the permissible level of 50 µg·m−3 (see Table 2, Fig. 1). The highest number of days (137) exceeding the permissible levels was recorded by station A in the cold period X 2020–III 2021, while the lowest number of days with the PM10 > 50 µg·m−3 was recorded by the station J in the cold period X 2019–III 2020.

Time distributions of a monthly number of days when the daily PM10 exceeded the value 50 µg·m−3 recorded by the 11 UMS stations (labeled with letters A to K) during the period 1 September 2018 to 31 August 2022.
The average number of days exceeding the permissible level of 50 µg·m−3 in the cold period for all stations in the analyzed period is 75.7. In period X 2020–III 2021, the highest average number of days exceeding the acceptable level was recorded 87.0; and the smallest (64.4 d) was recorded during the cold period X 2019–III 2020.
In the overall period under review (1 September 2018 to 31 August 2022), the highest number of days amounting to 390 exceedances of the daily permissible level of 50 µg·m−3 was reported by station K, and the smallest number of exceedance days (212) was recorded by station J (see Table 3). The maximum number of days exceeding the permissible level in monthly intervals is 27, which was recorded in March 2022 by station E (see Fig. 1).
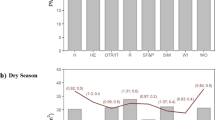
Average daily distributions of the hourly PM10 in all localization are bimodal (Fig. 2). The highest value of PM10 was achieved within the hours of 6–8 p.m. The second maximum is much weaker and occurs in the hours 6–8 a.m. On average, in the cold period, PM10 is several times higher than in the warm period (see Table 1). Moreover, the largest increase was recorded by station K (4.5), and the smallest increase in the cold period was recorded by station J (2.3).

Time distribution of hourly average PM10 [µg·m−3] concentration during all warm periods (thin line) and the cold period (bold line) recorded by 11 UMS stations (labeled with letters A to K).
In almost all locations, the optimal 2-h period with the lowest average PM10 concentration occurs between 12 and 2 p.m. except for station I, where this period falls from 11 a.m. to 1 p.m. The overall average value for the cleanest 2-h period across all locations is 34.6 µg m−3 (see Table 4), while for the same hours during the warm period, the average value is 10.0 µg m−3. Figure 2 shows a noticeable decrease in PM10 concentration at all locations around 10 a.m., indicating that the period between 10 a.m. and 2 p.m. has the lowest PM10 levels in the study area. This finding is consistent with research conducted by Nieckarz and Zoladz7.
Deposition factor (DF)
Based on previous research16,17,18,19, we assume that the value of the deposition factor at rest (DFAt rest) and deposition factor for exercising children (DFExercise) are equal to 0.60 and 0.40, respectively, which represents the average mass deposition fraction of PM10 in the human respiratory tract. We assume one DF value for boys and girls in all analyzed age groups (from 9 to 16 years).
where TD represents total deposition of PM10 calculated with Eq. (1) (using DF for at-rest and exercise, respectively, according to Table 6) in the volume of ventilated air (minute ventilation V̇E) during time activity (TA).
Discussion
Air quality in warm and cold periods. As presented in Table 1, the mean values of PM10 in the air in the locations included in this study vary significantly in warm and cold periods. In particular, the PM10 concentration in the air in the cold period is 3.4-fold higher than in the warm period (Table 1). Note that the PM10 level even in the warm period often exceeds the barrier of 50 µg m−3 (Table 3).
Children’s physical activities According to the Physical Activity Guidelines for Americans, 2nd edition20, issued by the U.S. Department of Health and Human Services, the recommended amount of physical activity for children and adolescents at ages 6 through 17 years is 60 min (1 h) or more of moderate-to-vigorous physical activity daily. The statement of this organization underlines the point that regular physical activity in children and adolescents promotes health and fitness. Physically active youth have higher levels of fitness, lower body fat, stronger bones and muscles, and better resilience to stressful situations. In addition, physically active children have better cognitive performance (for a review, see Physical Activity Guidelines for Americans, 2nd edition [health.gov]). Healthy children spontaneously undertake various kinds of physical activities such as soccer, football, handball, cycling, or running (for an overview, see Rowland21), which often exceeds the above-mentioned recommended 60 min of physical activity.
Interestingly, the endurance capacity of children at age 8–16 years old is remarkably good, as judged based on the levels of their maximal oxygen uptake (V̇O2max). For example, Reybrouck et al.15 reported the V̇O2max in boys aged 9–16 in the range of 50.6–56.6 mL O2 min−1 kg−1 and in girls at the same age between 42.2 and 43.7 mL O2 min−1 kg−1. Similar values of V̇O2max for the same age groups of children were recently reported by Lai et al.14. These findings show that the values of V̇O2max in children, expressed in relative values, are on a level similar to or even higher than healthy adults22,23,24. Moreover, Reybrouck et al.15 reported that the oxygen uptake of children at the ventilatory anaerobic threshold at age 9–16 years old amounted on average to 31.7 mL O2·min−1·kg−1 in boys and to 30.4 mL O2 min−1 kg−1 in girls. This result corresponds to about 60% and 65% of their V̇O2max, respectively, for girls and boys. Accordingly, it has been reported that prepubertal boys at age 11.6–14 years old could perform an exercise in laboratory conditions (walking/running on a treadmill) lasting 60 min, which required about 60% of their V̇O2max (31.4 − 32.6 mL O2 min−1 kg−1) without symptoms of fatigue (no blood lactate accumulation and submaximal HR during exercise)25.
Physical activity and the minute ventilation. Any form of sustained physical activity requires an adequate supply of oxygen to the working muscles to generate the needed amount of energy (ATP)22, 23, 26. A given metabolic rate (~ V̇O2) requires an appropriate minute ventilation (V̇E)22. The V̇E in children at ages between 9 and 16 years old when at rest amounts to ~ 7–10 L min−1, but during maximal exercise, V̇E increases to its maximal values (V̇Emax), ranging from ~ 60 to 85 L min−1 in girls and from ~ 60 to 115 L min−1 in boys depending on their age (see Table 5). The enhanced V̇E during exercise will increase the amount of the various PM inhalation and deposition in the respiratory tract19. This issue becomes especially relevant when exercising above the power output corresponding to the change point in V̇O2 (~ the lactate threshold)23, 24, 27, since above this exercise intensity the V̇E in humans increases non- proportionally to the increase of the exercise intensity22,23,24, 27.
Depending on individual children’s physical capacity, the exercise intensity of physical activities undertaken in the framework of physical education lessons as well as during additional spontaneous physical activities will vary between the children at varied ages. Exercise intensity will influence the magnitude of the absolute V̇E during exercise. In the present study (Table 5) we have presented data of simulations of varied exercise conditions including: (i) heavy–severe physical exercise, such as 1000-m competitive running with the V̇Emax, (ii) moderate–heavy intensity exercise with the V̇Eamounting to 75% V̇Emax, and (iii) moderate exercise intensity with the V̇E amounting to 40% V̇Emax.
Air quality and PM10 deposition. As presented in Table 6 and 7 we have calculated the rate (µg min−1) and the total PM10 (µg) deposition during various physical activities that require different levels of minute ventilation in children (girls and boys) for varied age groups. Note that the rate of deposition during all forms of exercise markedly increases above its levels at rest (see Tables 6 and 7). Regarding exercise, we show data for both variables (i.e., the rate and total PM10 deposition) as we believe that these variables should be considered separately. For example, in the case of intensive exercises (e.g., a 1000-m race) frequently practiced during physical education classes in school or other forms of intense exercise will result in a relatively low amount of the total deposition of PM10 but a high level of the deposition rate.
This scenario is opposite to the situation at rest or during prolonged modern exercise (40% of V̇Emax) where the deposition rate is much smaller, but the total deposition is much greater than during the short-term (3.5 min) maximal exercise. It seems to be likely, that the high deposition rate of PM10 might have a more acute harmful acute effect on the tissues of the respiratory tract, whereas the high total deposition rate might result in chronic illnesses of the respiratory tract. This hypothesis, however, requires detailed clinical studies in the future. Furthermore, it can be seen in Table 6 that the children at higher ages (see, e.g., groups AG3 and AG4 vs. AG2 and AG1) are exposed to a greater deposition rate and total deposition of PM10 as their absolute values of the V̇Emax are much higher than in younger children (see Tables 6 and 7). As shown in Table 1 the sessional and daily changes of the levels of PM10 in the inspired air strongly affect the rate and total deposition of PM10 in the respiratory tract of children.
PM10 deposition and health risk The deposited dose of inhaled PM was measured over varied areas (urban, roads, and rural), as well as the dose rates in terms of PM2.5 and PM1016,17,18,19, 28,29,30,31,32. These studies indicate that the dose rate was dependent on a few elements, such as geographic factors, physical characteristics of the particle number size distribution, activity type (exercise/at rest), age, gender, concentration metric (number versus mass), and particle diameter.
Studies have shown that the dose rate was nonlinearly proportional to the exposure level. Deep breathing pulls PM faster and farther into the lungs, bypassing initial areas of deposition33. According to Ginsberg et al.34, the pulmonary region of the lung has slower clearance; therefore, PM remains there longer. Consequently, the particle dose can be two- to four-fold higher among young children. A comprehensive review and description concerning the available models of inhaled particle deposition in the lungs can be found in Morawska et al.35. The above-discussed harmful effects of PM on the health of children become particularly relevant when children undertake various forms of physical activities in the polluted air, resulting in an enhancement of the rate and total PM deposition in the respiratory tract (see Tables 6 and 7).
As seen in Tables 6 and 7, the values of the deposition rate and the total deposition for boys from older age groups (AG2–AG4) when exercising at the same percentage of the V̇Emax, are systematically higher than in girls belonging to analogical age groups (AG2–AG4). This discrepancy is because the absolute V̇Emax (L min−1) values in the boys at a given age (above 10 years old) in boys are higher than in girls (see Table 5).
The presented low-cost particulate matter sensors allow for limiting the risk of health hazards in children by showing the actual PM concentrations and choosing the appropriate “time window” for the daily dose of exercise. The chosen period can be when air quality is the highest—in our research, the hours between 10 a.m. and 2 p.m. (see Fig. 2 and Table 4). In cases of heavy air pollution on a given day, teachers aware of this fact, might: perform their daily physical exercise inside the school or sports center buildings, or to limit the intensity and duration of outdoor exercise.
Conclusions
The use of a low-cost measurement network7 supported by a calibration system13 is a useful tool in air quality monitoring, particularly in rural areas where the use of expensive, highly accurate measuring devices is beyond the budget of small communities. This low-cost measurement solution eliminates the limitations and social and informational exclusion affecting small communities such as villages (currently about 40% of the population in Poland)9. The presence of such installations in rural areas raises the awareness of residents regarding the role of air quality on their health and contributes to activating these communities for environmental protection. As shown in this study, the described low-cost particulate matter sensors monitoring the actual PM10 concentrations allow for limiting the risk of health hazards in children. This information enables school authorities and teachers to choose an appropriate “time window” for the daily dose of physical exercise performed outdoors when the air quality is the best to minimize the rate and total PM10 deposition in children’s respiratory tracts.
Data availability
The datasets used and/or analyzed during the current study available from the corresponding author on every request.
References
Ministry. Regulation of the Minister of Climate and Environment of December 11, 2020 on assessing the levels of substances in the air (in Polish). https://isap.sejm.gov.pl/isap.nsf/download.xsp/WDU20200002279/O/D20202279.pdf (2020).
European Union. https://www.eea.europa.eu/publications/air-quality-in-europe-2021 (2021).
WHO. Global air quality guidelines. Particulate matter (PM2.5 and PM10), ozone, nitrogen dioxide, sulfur dioxide and carbon monoxide. World Health Organization (2021).
Saenen, N. D. et al. Recent versus chronic exposure to particulate matter air pollution in association with neurobehavioral performance in a panel study of primary schoolchildren. Environ. Int. 95, 112–119. https://doi.org/10.1016/j.envint.2016.07.014 (2016).
GOV. Chief Inspectorate for Environmental Protection. https://powietrze.gios.gov.pl
Chen, L.-J. et al. An open framework for participatory PM2.5 monitoring in smart cities. IEEE Access 5, 14441–14454. https://doi.org/10.1109/ACCESS.2017.2723919 (2017).
Nieckarz, Z. & Zoladz, J. A. Low-cost air pollution monitoring system—An opportunity for reducing the health risk associated with physical activity in polluted air. PeerJ 8, e10041. https://doi.org/10.7717/peerj.10041 (2020).
Report. Air quality in Europe 2022. European Environmental Agency. https://doi.org/10.2800/488115 (2022).
Yearbook. Concise Statistical Yearbook of Poland. https://www.stat.gov.pl (2021).
Thangavel, P., Park, D. & Lee, Y. C. Recent insights into particulate matter (PM2.5)-mediated toxicity in humans: An overview. Int. J. Environ. Res. Public Health 19(12), 7511. https://doi.org/10.3390/ijerph19127511 (2022).
Chen, G. et al. Effects of ambient PM1 air pollution on daily emergency hospital visits in China: An epidemiological study. Lancet Planet. Health 1(6), e221–e229. https://doi.org/10.1016/S2542-5196(17)30100-6 (2017).
Wilczyńska-Michalik, W. & Michalik, M. Air pollution in Krakow: A glance into the future from a historical perspective. Acta Geobalcanica 3(2), 79–82. https://doi.org/10.18509/AGB.2017.10 (2017).
Nieckarz, Z. & Zoladz, J. A. New calibration system for low-cost suspended particulate matter sensors with controlled air speed, temperature and humidity. Sensors 21, 5845. https://doi.org/10.3390/s21175845 (2021).
Lai, N., Fiutem, J. J., Pfaff, N., Salvadego, D. & Strainic, J. Relating cardiorespiratory responses to work rate during incremental ramp exercise on treadmill in children and adolescents: Sex and age differences. Eur. J. Appl. Physiol. 121, 2731–2741. https://doi.org/10.1007/s00421-021-04741-1 (2021).
Reybrouck, T., Weymans, M., Stijns, H., Knops, J. & van der Hauwaert, L. Ventilatory anaerobic threshold in healthy children. Age and sex differences. Eur. J. Appl. Physiol. Occup. Physiol. 54(3), 278–284. https://doi.org/10.1007/BF00426145 (1985).
Rissler, J. et al. Effective density and mixing state of aerosol particles in a near-traffic urban environment. Environ. Sci. Technol. 48(11), 6300–6308. https://doi.org/10.1021/es5000353 (2014).
Hussein, T. et al. Regional inhaled deposited dose of urban aerosols in an eastern Mediterranean city. Atmosphere 10(9), 530. https://doi.org/10.3390/atmos10090530 (2019).
Guo, L., Johnson, G. R., Hofmann, W., Wang, H. & Morawska, L. Deposition of ambient ultrafine particles in the respiratory tract of children: A novel experimental method and its application. J. Aerosol. Sci. 139, 105465. https://doi.org/10.1016/j.jaerosci.2019.105465 (2020).
Zoladz, J. A. & Nieckarz, Z. Marathon race performance increases the amount of particulate matter deposited in the respiratory system of runners: An incentive for “clean air marathon runs”. PeerJ 9, e11562. https://doi.org/10.7717/peerj.11562 (2021).
Physical Activity Guidelines for Americans 2nd edn. https://health.gov/sites/default/files/2019-09/Physical_Activity_Guidelines_2nd_edition.pdf (2018).
Rowland, T. W. Children’s Exercise Physiology 2nd edn. (Human Kinetics Publishers, 2005) (ISBN: 9780736051446).
Mácek, M., Vávra, J. & Novosadová, J. Prolonged exercise in prepubertal boys. I. Cardiovascular and metabolic adjustment. Eur. J. Appl. Physiol. Occup. Physiol. 35(4), 291–298. https://doi.org/10.1007/BF00423289 (1976).
Astrand, P.-O. & Rodahl, K. Textbook of Work Physiology 3rd edn, 295–253 (McGraw-Hill, 1986).
Wasserman, K., Hansen, J. E., Sue, D. Y., Stringer, W. W. & Whipp, B. J. Physiology of exercise. In Principles of Exercise Testing and Interpretation 4th edn (eds Wasserman, K. et al.) 10–65 (Lippincott Williams and Wilkins, 2005).
Zoladz, J. A., Szkutnik, Z. & Grassi, B. Metabolic Transitions and muscle metabolic stability: Effects of exercise training. In Muscle and Exercise Physiology (ed. Zoladz, J. A.) 391–422 (Elsevier, 2019).
Zoladz, J. A., Szkutnik, Z., Majerczak, J. & Duda, K. Detection of the change point in oxygen uptake during an incremental exercise test using recursive residuals: Relationship to the plasma lactate accumulation and blood acid base balance. Eur. J. Appl. Physiol. Occup. Physiol. 78(4), 369–377. https://doi.org/10.1007/s004210050433 (1998).
Zoladz, J. A., Duda, K. & Majerczak, J. Oxygen uptake does not increase linearly at high power outputs during incremental exercise test in humans. Eur. J. Appl. Physiol. Occup. Physiol. 77(5), 445–451. https://doi.org/10.1007/s004210050358 (1998).
Canha, N., Almeida, M., do Freitas, M. C., Almeida, S. M. & Wolterbeek, H. T. Seasonal variation of total particulate matter and children respiratory diseases at Lisbon primary schools using passive methods. Proc. Environ. Sci. 4, 170–183. https://doi.org/10.1016/j.proenv.2011.03.021 (2011).
Löndahl, J. et al. Measurement techniques for respiratory tract deposition of airborne nanoparticles: A critical review. J. Aerosol. Med. Pulm. Drug Deliv. 27, 229–254 (2014).
Nunes, R. A., Branco, P. T., Alvim-Ferraz, M. C., Martins, F. G. & Sousa, S. I. Particulate matter in rural and urban nursery schools in Portugal. Environ. Pollut. 202, 7–16. https://doi.org/10.1016/j.envpol.2015.03.009 (2015).
Gautam, S., Patra, A. K., Sahu, S. P. & Hitch, M. Particulate matter pollution in opencast coal mining areas: a threat to human health and environment. Int. J. Min. Reclam. Environ. 32(2), 75–92. https://doi.org/10.1080/17480930.2016.1218110 (2016).
Hussein, T., Al-Abdallat, A., Saleh, S. S. A. & Al-Kloub, M. Estimation of the seasonal inhaled deposited dose of particulate matter in the respiratory system of urban individuals living in an Eastern Mediterranean City. Int. J. Environ. Res. Public Health 19(7), 4303. https://doi.org/10.3390/ijerph19074303 (2022).
Zwozdziak, A. et al. Influence of PM1 and PM2.5 on lung function parameters in healthy schoolchildren—A panel study. Environ. Sci. Pollut. Res 23, 23892–23901. https://doi.org/10.1007/s11356-016-7605-1 (2016).
Ginsberg, G., Foos, B. & Firestone, M. Review and analysis of inhalation dosimetry methods for application to children’s risk assessment. J. Toxicol. Environ. Health A 68(8), 573–615. https://doi.org/10.1080/15287390590921793 (2005).
Morawska, L. et al. Indoor aerosols: From personal exposure to risk assessment. Indoor Air 23(6), 462–487. https://doi.org/10.1111/ina.12044 (2013).
Funding
The research for this publication has been supported by the budget of Anthropocene Priority Research Area (Earth System Science Core Facility Flagship Project) under the Strategic Programme Excellence Initiative at Jagiellonian University. The publication was also created with the use of equipment co-financed by the qLIFE Priority Research Area under the program “Excellence Initiative—Research University” at Jagiellonian University
Author information
Authors and Affiliations
Contributions
Z.N., and J.A.Z., provided idea and wrote the main manuscript text; Z.N., and K.P., participated in environmental measurements. All authors have read and agreed to the published this version of the manuscript. Z.N., and J.A. Z., contributed equally to this paper. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Nieckarz, Z., Pawlak, K. & Zoladz, J.A. Health risks for children exercising in an air-polluted environment can be reduced by monitoring air quality with low-cost particle sensors. Sci Rep 13, 18261 (2023). https://doi.org/10.1038/s41598-023-45426-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-45426-3
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
