
Abstract
Autism spectrum disorder (ASD) are neurodevelopmental conditions characterised by deficits in social communication and interaction and repetitive behaviours. Maternal immune activation (MIA) during the mid-pregnancy is a known risk factor for ASD. Although reported in 15% of affected individuals, little is known about the specificity of their clinical profiles. Adaptive skills represent a holistic approach to a person's competencies and reflect specifically in ASD, their strengths and difficulties. In this study, we hypothesised that ASD individual with a history of MIA (MIA+) could be more severely socio-adaptively impaired than those without MIA during pregnancy (MIA-). To answer this question, we considered two independent cohorts of individuals with ASD (PARIS study and FACE ASD) screened for pregnancy history, and used supervised and unsupervised machine learning algorithms. We included 295 mother–child dyads with 14% of them with MIA+. We found that ASD-MIA+ individuals displayed more severe maladaptive behaviors, specifically in their socialization abilities. MIA+ directly influenced individual's socio-adaptive skills, independent of other covariates, including ASD severity. Interestingly, MIA+ affect persistently the socio-adaptive behavioral trajectories of individuals with ASD. The current study has a retrospective design with possible recall bias regarding the MIA event and, even if pooled from two cohorts, has a relatively small population. In addition, we were limited by the number of covariables available potentially impacted socio-adaptive behaviors. Larger prospective study with additional dimensions related to ASD is needed to confirm our results. Specific pathophysiological pathways may explain these clinical peculiarities of ASD- MIA+ individuals, and may open the way to new perspectives in deciphering the phenotypic complexity of ASD and for the development of specific immunomodulatory strategies.
Similar content being viewed by others


Introduction
Autism spectrum disorder (ASD) are heterogeneous neurodevelopmental conditions characterised by social communication impairment and interaction and repetitive or stereotyped behaviors. Its incidence is 1 in 50 to 1 in 100 births, affecting 52 million people worldwide1. The etiopathogenesis of ASD results from the close intertwining of genetic predispositions and environmental risk factors. Among known environmental insults, maternal immune activation in mid-pregnancy (MIA)—due to maternal autoimmune diseases or infections—is increasingly seen as a risk factor for ASD in offspring2. In accordance with epidemiological evidences, well-replicated pre-clinical studies show that this association leads to ASD by direct action of maternal immune mediators (i.e. cytokines) on fetal cortical neurons, disrupting normal neurodevelopment and leading to autism-like behaviours in the pups3. Years of intensive research have made it possible to divide the common and heterogeneous autism spectrum into rarer but etiopathogenically homogeneous entities, based mainly on common genetic variants4. This approach allows to identify and better understand common pathophysiological pathways and thus the emergence of potential targeted therapies. Nonetheless, few studies have attempted to characterise ASD subgroup according to common pathogenic environmental factors. Despite a history of MIA being frequent, approximatively reported in 15% of ASD individuals, there is surprisingly little data on their specific clinical profiles5,6.
Clinical studies often use symptom scales to assess the clinical characteristics of individuals and the severity of the condition, which do not reflect their adaptability to the environment. According to the American Association on Intellectual and Developmental Disorders (AAIDD), adaptive behaviour is «the collection of conceptual, social, and practical skills that all people learn in order to function in their daily lives»7. Adaptive skills thus represent a higher concept of functioning, taking into account all dimensions of a person in his/her environment8.
We hypothesized that individual with ASD and a history of MIA (MIA+) would display more severe socio-maladaptive behaviors than those without MIA during pregnancy (MIA-). To perform this study, we considered two independent cohorts of individuals with ASD (PARIS study and FACE ASD) screened for pregnancy history and used supervised and unsupervised machine learning algorithms to decipher the possible interactions between MIA and adaptive behaviors in ASD.
Methods
Participants recruitments
We included in our study children with ASD enrolled in the PARIS study, conducted by the Excellence Centre for Autism & Neuro-developmental Disorders (InovAND—Robert Debré Hospital, Paris, France) between March 2017 and April 2021. This study was approved by the local ethics committee (2021–27 N° IDRCB: 2021-A00489-32). Prior to inclusion, informed consent was obtained from a parent and/or legal guardian. We also enrolled ASD individuals from an independent sample from eight Expert Centers for ASD (Créteil, Bordeaux, Grenoble, Versailles, Marseille, Caen, Strasbourg, Lyon) coordinated by Fondation FondaMental. The relevant Ethical Review Board (CPP- Est IV) approved the appraisal protocol on 18 June 2019. All participants gave their informed consent. All methods in both studies were performed in accordance with relevant guidelines/regulations and have been performed in accordance with the Declaration of Helsinki. Patients with a diagnosis of MIA and information about the history of MIA were included, no family refused to participate. Considering the frequency of the MIA event (12–15%) and the number of individual per sample, we pooled all individuals to increase the power analysis of the study. Separate demographic information of each cohort is in Supplementary Table 1.
Clinical evaluation and questionnaires
The diagnosis of ASD was performed according to DSM-5 criteria9 by summing up the information from the Autism Diagnostic Interview-Revised (ADI-R)10, the Autism Diagnostic Observation Schedule -2nd edition (ADOS-2)11 and clinical records of individuals. The ADI-R is a parental interview for the diagnosis of autism, which can be carried out from the age of 24 months. It reviews the child's developmental history, investigating communication, social development and play, restricted interests and behaviours, general behaviours and the age of onset of difficulties. In the ADOS-2, the child is asked to perform activities to assess communication, reciprocal social interaction, play and/or imaginative use of materials, stereotyped behaviour, restricted interests and other abnormal behaviour. Different modules are offered depending on the age and level of functioning of the subject, ranging from pre-school children to verbal adults.
All participants were screened with a parental semi-structured interview for pre- and peri- natal history exploring pregnancy complications (Threatened preterm delivery, High blood pressure, Placenta Praevia, Premature rupture of membranes, Materno-foetal infection). This interview was conducted by a child and adolescent psychiatrist specialising in ASD at best in the presence of both parents, but often only the mother. We focused on any history of MIA during pregnancy based solely on the parents' declaration. Based on this information collected by the parents, children were then split either into MIA (MIA+) or in non-MIA (MIA-) sub-groups. We considered mothers with a significant history of an MIA-related event when they were: (i) with an autoimmune disease as listed by the American Autoimmune Related Diseases Association12 and (ii) with a viral or bacterial infection during pregnancy with a fever over 38.5 °C for more than 24 h. Mothers with an infection resulting from a pathogen with a well-documented direct brain cytopathic effect (such as cytomegalovirus infection) were excluded. Details of MIA are in Supplementary Table 2.
The level of autonomy and adaptation of children with neurodevelopmental conditions is assessed with the second edition of the Vineland Adaptive Behavior Scale (VABS) 8,13. The VABS is the reference test for assessing the level of autonomy and adaptation at all ages. The Vineland-II explores 3 major areas: Communication, Daily Life Skills and Socialisation. Assessing the overall level of autonomy and ability to adapt helps in diagnosis and provides information for setting up educational and remedial programmes. The Vineland scale comprises 117 questions and takes the form of a semi-structured interview with the parents or primary carer. It can be administered and scored by a psychologist or another professional trained in the evaluation and interpretation of tests. The test takes between 30 min and 1 h to complete, depending on the person concerned. At the end of the test, for each domain assessed, the result expresses the average level of competence achieved by the person in that domain, in age equivalence. It should be note that in this study, IQ and scales for others co-occuring conditions (ADHD, etc.) were not available. Missing data for each group are in Supplementary Table 3.
Statistical analysis
Prior to each analysis, we assessed the normality of variable distributions using the Shapiro–Wilk test. For continuous data, depending on its normality, we employed either the Student’s t-tests or the Wilcoxon tests. For categorical data, we utilized the Fisher's test. Additionally, only those linear models were adopted that demonstrated a normal distribution of residuals. We conducted hierarchical regression analyses to determine whether MIA significantly accounts for the variance in the dependent variables.. Hierarchical regression is a stepwise method where predictors are added or removed in stages or blocks. This approach facilitates the analysis of how multiple predictor variables explain variance in a dependent variable in the context of datasets which include confounding variables. Detailed results of the hierarchical regression analyses can be found in the supplementary materials. The final models from the multivariate analysis, available in the supplementary materials, were all adjusted based on sex and ASD scales (SRS T-score/ADOS total score). To infer the presence or absence of MIA based on multiple collected input variables, we used classification decision trees, which are supervised predictive machine learning models. Classification decision trees offer a visual and intuitive approach to data analysis, allowing for straightforward interpretation of complex datasets by segmenting the data into branches based on hierarchical decision rules, and facilitating the handling of both categorical and continuous variables without requiring extensive data preprocessing or assumptions about data distributions. Classification trees were generated using R package 'Party'14. The relevance of the groups identified by the classification trees was then tested using ANOVA with post-hoc Tukey for multiple mean comparisons. To complement the results of the classification tree and study which variables are the most important for predicting MIA, we performed supervised classification methods using the R package 'mlr3'15. For classification, we used both logistic regression classification learner and a linear discriminant analysis classification learner. Logistic regression classification learner predicts the probability of an outcome based on one or more predictor variables by modeling the data on a logistic function, while linear discriminant analysis classification learner seeks to find a linear combination of features that best separates two or more classes. The advantage of these methods is their ability to model relationships between predictors and categorical outcomes effectively, while providing clear coefficients or weightings for each predictor, aiding interpretability and decision-making. We divided samples into two groups: 80% for training and the remaining 20% for validation. As the MIA+ individuals were under-represented, we used an oversampling method with a 3.5 ratio. The sample characteristics before and after oversampling are in Supplementary Fig. 1. The learning parameters used by the model were then evaluated using the package R package 'iml'16 with three components: feature effects, Shapley values and feature importance. Finaly, to comprehensively understand both the direct and indirect effects of all variables on the MIA outcome across various causal pathways, we employed unsupervised path analysis utilizing the 'lavaan' R package17. We did not apply multiple test corrections for p-values since many of our models, especially Linear Discriminant Analysis (LDA) and classification decision tree, did not produce p-value outputs. Statistical analysis was performed using R studio version 4.2.1.
Ethical approval
As part of the PARIS study, this study was approved by the local ethics committee of Robert Debré Hospital (2021–27 N° IDRCB: 2021-A00489-32). Informed consents were obtained from patients or a parent and/or legal guardian before enrollment in the study. All methods in both studies was performed in accordance with relevant guidelines/regulations and have been performed in accordance with the Declaration of Helsinki.
Results
General characteristics
295 mother–child dyads were included in our study, with a history of MIA reported in 14% of mothers (n = 40) (MIA+). Details of MIA is on Supplementary Table 2. Dyads without a history of MIA (n = 255, 86%) were used as a comparison group (MIA-).
Demographic information, prenatal history, birth parameters and ASD scales are provided in Table 1.
We observed that mothers with MIA during pregnancy had more history of premature rupture of membranes (PROM) (p-value = 0.002) and maternofetal infection (MFI) (p-value = 0.02) than those without MIA. ASD-MIA+ individuals did not differ from those without a history of MIA in terms of symptom severity estimated with the SRS T-score (p-value = 0.6) or ADOS total score (p-value = 0.4). Univariate analysis did not reveal any difference in any of the three sub-domain of the VABS: communication (p-value = 0.3), socialisation (p-value = 0.2), daily living skills (DLS) (p-value = 0.4) domains.
More severe impact on adaptative behaviors related to socialization is associated with MIA during pregnancy
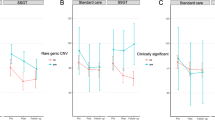
We found, that SRS T-score and ADOS total score were correlated with the three sub-scores of VABS (Fig. 1A). Accordingly, hierarchical regression analysis showed that more severe socio-maladaptive behaviors in ASD individuals were associated with a MIA during pregnancy (p-value = 0.006) (Supplementary Table 4 and Table 5). To confirm this association, we used a classification tree which isolated three groups (Fig. 1B): (i) a MIA low-probability group (VABS—Socialisation > 55 and ADOS total score > 15) with 1% of MIA+; (ii) a medium-probability group (VABS—Socialisation > 55 and ADOS total score = < 15) with 11% of MIA+; and (iii) a high-probability group (VABS—Socialisation = < 55) with 17% of MIA+. Significant differences between the high-probability group and the low-probability group were observed (p-value = 0.002).

More severe impact on adaptative behaviors related to socialization is associated with maternal immune activation during pregnancy. (A) Correlogram of the different subdomain of the Vineland II with clinical parameters. (B) Classification decision tree of the risk of maternal immune activation during pregnancy depending on Vineland II—Socialisation sub-score and ADOS total score on the autistic offspring. (C) Feature importance for the logistic analysis. Feature importance computes the importance of features by calculating the increase in the model prediction error after permuting the feature. (D) Feature importance for the linear discriminant analysis. (E) Classification decision tree of the risk of maternal immune activation during pregnancy depending on Vineland II—Communication sub-score and ADOS total score on the autistic offspring. MIA: Maternal immune activation, SRS: Social Responsiveness Scale 2nd edition; ADOS Autism Diagnostic Observation Schedule 2nd edition, VABS: Vineland Adaptive Behavior Scales 2nd edition.
Finally, we validated these results using two distinct supervised classification algorithms. Using logistic classification, we discriminated MIA+ individuals with an accuracy of 70%, a sensitivity of 84%, a specificity of 27% and an area under the curve (AUC) of 72%. In accordance with our initial hypothesis, the most robust parameter to classify children was the VABS—Socialisation score followed by ADOS total score (Fig. 1C and Supplementary Fig. 2A and 2B). Using linear discriminant analysis classification (LDA), we reported similar results with an accuracy of 72%, a sensitivity of 84%, a specificity of 33% and AUC of 66%. Of note, the VABS—Socialisation score was also the most important parameter allowing classification, but in LDA, both ADOS total score and SRS T-score were pertinent to classify children (Fig. 1D). Considering the communication domain, we observed that a lower score was also associated with a history of MIA (p-value = 0.045) (Supplementary Table 6). We next used a classification tree also isolating three groups of individuals (Fig. 1E): (i) a MIA low-probability group (VABS—communication > 66) with 10% of MIA+ ; (ii) a medium-probability group (VABS—Communication = < 66 and ADOS total score > 19) with 12% of MIA+ ; and (iii) a high-probability group (VABS—Communication = < 66 and ADOS total score < 19)) with 18% of MIA+. No significant differences were found between groups (p-value < 0.08). Thus, we considered that the communication domain of the VABS was not associated with MIA. Lastly, no association was observed between DLS and MIA (p-value = 0.2) (Supplementary Table 7).
MIA may directly affect the socio-maladaptive behaviors in ASD
We observed that MIA was associated with more pregnancy complications also known to increase independently the risk for ASD (Table 1)18. Pregnancy complications and more severe ASD symptomatology were correlated with more adaptive behaviours later on (Supplementary Fig. 3). Adjusting for these potential factors and corroborating our previous results, we investigated whether a history of MIA was associated with poorer adaptive behavior and if so, the mediator of this association.
Using adjustment models, we found no association between the history of MIA and communication (p-value = 0.15) or DLS (p-value = 0.63) sub-domain but a significant association with poorer socio-adaptive behaviours (p-value = 0.03) (Supplementary Table 8, 9 and 10). Analysis with a linear model regression learner confirmed this association (mean absolute error = 20.2; mean square error = 562.7; root mean square error = 23.7, R-square = 0.16) (Fig. 2A).

Maternal immune activation may directly affected the socio-maladaptive behaviors in autism children. (A) Predictions of the linear model on socialization sub scores compared to measured scores. (B) Feature Iimportance of the linear regression model. (C) Path analysis on the influence of MIA on socialization sub-score. MIA: Maternal immune activation, SRS: Social Responsiveness Scale 2nd edition; ADOS Autism Diagnostic Observation Schedule 2nd edition, VABS: Vineland Adaptive Behavior Scales 2nd edition, PROM: Premature rupture of membranes; MFI: Materno-fetal infection; TLI: Tucker-Lewis index; CFI comparative fit index; RMSEA root mean square error of approximation; SRMR: standardized root mean squared residual.
According to feature importance, MIA appeared to predict the intensity of communication deficit, just after the intensity of the global autistic symptom severity itself (Fig. 2B and Supplementary Fig. 4). Finally, we explored whether there was a causal link between the MIA and the impairment intensity of socio-adaptive skills. We used structural equation modelling and applied a path analysis to our dataset. We found, with a good model performance (Fig. 2C), that MIA directly influenced the socio-adaptive skills of children, independently of pregnancy complications or global severity of ASD symptoms (Fig. 2C).
Discussion
We found that ASD individuals with a history of MIA during pregnancy displayed more difficulties in socio-adaptive skills. For individuals with a VABS socialization subdomain score < 55, almost 20% of children had a history of MIA, compared to 1–10% for those with a VABS socialization subdomain score > 55. Social-adaptive skills are a central node of ASD symptomatology. Compared to healthy children, ASD children, no matter the MIA status, have more difficulties in adaptive social behaviors with other adaptive domains less impacted19. Our results were consistent with the literature with exploratory study reporting more severe symptoms of social impairment—assessed with the SRS- in case of immune activation during pregnancy (in case of asthma and allergies)5. One limitation is that we did not assess all the clinical variables likely to influence socio-adaptive behaviour. Intelligence quotient, for example, was not integrated, whereas there were significant entanglements between IQ and adaptive functioning20. This limitation must be contrasted with a previous study finding that MIA was not associated withdecreased cognitive functions6. Future studies should integrate all the dimensions of ASD children and frequent comorbidity, such as ID or ADHD, in order to decipher the socio-adaptive abnormalities in ASD children21.
We also observed that MIA directly influenced the socio-adaptive behaviors of ASD individuals The effect of MIA did not seem to bemediated by an increase in the severity of autistic symptoms. This hypothesis mirrored findings in children with neurodevelopmental conditions (excluding ASD), in whom a history of MIA was associated, in a dose–response effect, with more externalizing and internalizing problems22. In mice, MIA directly triggers autistic-like symptoms through an effect on neuronal cytokine receptors in the cerebral cortex3. Immunogenetic factors may also mediate the link between MIA, mother and unborn child. Indeed, a variant in HLA-G has been found in ASD patients but also in their mothers23. HLA-G is mainly expressed in placental tissues playing a role in maternal–fetal tolerance24 and could, therefore, modulate the impact of MIA on neurodevelopment. MIA also appears to disrupt neurodevelopment by altering microglia function, leading to deficits in synaptic pruning and abnormalities in synaptic connectivity25,26,27. However, MIA also induced epigenetic changes of major transcriptional factors in the offspring that are independent of the onset of ASD core symptoms28. This effect is mediated by the maternal microbiota and leads to a long-term immune imbalance in the offspring, characterised by a peripheral increase in the Th17 lymphocyte subtype (Th17)29. Th17 are major pro-inflammatory lymphocytes and are in a constant and dynamic equilibrium with its anti-inflammatory counterpart regulatory T lymphocytes (Tregs)30,31. Interestingly, ASD individuals displayed a peripheral increase in Th17 and a decrease in Tregs, which was more pronounced in those with a history of MIA32. Interestingly, a recent study on mice demonstrated that specific stimulation of Tregs in ASD pups from MIA mothers reverses autistic-like symptoms33. Overall, this suggests that the epigenetically mediated peripheral immune imbalance induced by MIA may participate in the socio-maladaptive behaviors in ASD and could be targeted by specific immunomodulatory strategies.
Limitations
One of the main limitations of our study is intrinsically linked to its retrospective design, which leads to a possible recall bias concerning MIA during pregnancy and, in particular, the timing of MIA in our cohort. To overcome this problem, we used a strict definition of MIA, but this will not replace a prospective study to confirm our results. Even if we pooled two cohorts, the population remains relatively small and to better decipher the influence of MIA, many clinical and biological factors need to be studied on larger cohorts to obtain the necessary statistical power. Nevertheless, all our results were validated by different and complementary statistical approaches with good model performance, highlighting the robustness of our data.
Finally, one additional limitation of our study was the limited number of covariables which potentially impacted socio-adaptive behaviors, that we included in the analysis. Intelligence quotient, for example, was not integrated, whereas there were significant entanglements between IQ and adaptive functioning20. In addition, we were unable to assess other dimensions of ASD, such as repetitive/restricted behaviors. Future studies should integrate additional dimensions related to ASD, such as intellectual developmental disorder or Attention Deficit / Hyperactive Disorder, to further decipher the impact of MIA on socio-adaptive impairment in ASD21.
Conclusions
MIA may affect in the long term the socio-adaptive behavioral trajectories of individuals with ASD. Specific pathophysiological pathways may explain these clinical peculiarities of ASD- MIA+ individuals, and may open the way to new perspectives in deciphering the phenotypic complexity of ASD and the development of targeted immunotherapy strategies.
Data availability
The PARIS dataset and the code used during the current study are available from the corresponding author upon request. Due to ethical and legal restrictions, data involving clinical participants of the FACE-ASD cohort cannot be made publicly available. All relevant data are available upon request to the Fondation FondaMental for researchers who meet the criteria for access to confidential data.
Abbreviations
- ADOS:
-
Autism Diagnostic Observation Schedule 2nd edition
- ASD:
-
Autism spectrum disorders
- MIA:
-
Maternal immune activation
- SRS:
-
Social Responsiveness Scale 2nd edition
- VABS:
-
Vineland Adaptive Behavior Scales 2nd edition
References
Lord, C. et al. Autism spectrum disorder. Nat. Rev. Dis. Primers. 6, 5 (2020).
Han, V. X., Patel, S., Jones, H. F. & Dale, R. C. Maternal immune activation and neuroinflammation in human neurodevelopmental disorders. Nat. Rev. Neurol. 17, 564–579 (2021).
Choi, G. B. et al. The maternal interleukin-17a pathway in mice promotes autism-like phenotypes in offspring. Science 351, 933–939 (2016).
Bourgeron, T. From the genetic architecture to synaptic plasticity in autism spectrum disorder. Nat. Rev. Neurosci. 16, 551–563 (2015).
Patel S., et al. Social impairments in autism spectrum disorder are related to maternal immune history profile. Mol Psychiatry (2017)
Patel, S. et al. Maternal immune conditions are increased in males with autism spectrum disorders and are associated with behavioural and emotional but not cognitive co-morbidity. Transl. Psychiatry. 10, 286 (2020).
Adaptive Behavior [Internet]. AAIDD_CMS. [cited 2022 Dec 15]. Available from: https://www.aaidd.org/intellectual-disability/definition/adaptive-behavior
Tillmann, J. et al. Investigating the factors underlying adaptive functioning in autism in the EU-AIMS Longitudinal European Autism Project. Autism Res. 12, 645–57 (2019).
Diagnostic and statistical manual of mental disorders. DSM-5 5th edn. (American psychiatric association, 2013).
Lord, C., Rutter, M. & Le Couteur, A. Autism diagnostic interview-revised: A revised version of a diagnostic interview for caregivers of individuals with possible pervasive developmental disorders. J Autism Dev. Disord. 24, 659–685 (1994).
Lord, C. et al. The autism diagnostic observation schedule—Generic: A standard measure of social and communication deficits associated with the spectrum of autism. J. Autism Dev. Disord. 30, 205–223 (2000).
Autoimmune Disease List • AARDA [Internet]. AARDA. 2016 [cited 2021 Feb 19]. Available from: https://www.aarda.org/diseaselist/
Kanne, S. M. et al. The role of adaptive behavior in autism spectrum disorders: Implications for functional outcome. J. Autism Dev. Disord. 41, 1007–1018 (2011).
Hothorn, T., Seibold, H., Zeileis, A. partykit: A Toolkit for Recursive Partytioning [Internet]. 2021 [cited 2022 Jun 7]. Available from: https://CRAN.R-project.org/package=partykit
Lang [cre M, aut, Bischl B, Richter J, Schratz P, Casalicchio G, et al. mlr3: Machine Learning in R - Next Generation [Internet]. 2022 [cited 2022 Dec 15]. Available from: https://CRAN.R-project.org/package=mlr3
Molnar, C., Schratz, P. iml: Interpretable machine learning [Internet]. 2022 [cited 2022 Dec 15]. Available from: https://CRAN.R-project.org/package=iml
Rosseel, Y., et al. lavaan: Latent variable analysis [Internet]. 2022 [cited 2022 Dec 15]. Available from: https://CRAN.R-project.org/package=lavaan
Pierrat, V. et al. Neurodevelopmental outcomes at age 5 among children born preterm: EPIPAGE-2 cohort study. BMJ 373, n741 (2021).
Kim, S. H., Bal, V. H. & Lord, C. Adaptive social abilities in autism. In Comprehensive Guide to Autism (eds Patel, V. B. et al.) (Springer, 2014).
Tamm, L., Day, H. A. & Duncan, A. Comparison of adaptive functioning measures in adolescents with autism spectrum disorder without intellectual disability. J. Autism Dev. Disord. 52, 1247–1256 (2022).
Nishimura, T. et al. Trajectories of adaptive behaviors during childhood in females and males in the general population. Front. Psychiatry 13, 817383 (2022).
Patel, S. et al. Maternal immune-related conditions during pregnancy may be a risk factor for neuropsychiatric problems in offspring throughout childhood and adolescence. Psychol. Med. 51, 2904–2914 (2021).
Guerini, F. R. et al. An HLA-G(∗)14bp insertion/deletion polymorphism associates with the development of autistic spectrum disorders. Brain Behav. Immun. 44, 207–212 (2015).
Carosella, E. D., Gregori, S. & LeMaoult, J. The tolerogenic interplay(s) among HLA-G, myeloid APCs, and regulatory cells. Blood 118, 6499–6505 (2011).
Fernández de Cossío, L., Guzmán, A., van der Veldt, S. & Luheshi, G. N. Prenatal infection leads to ASD-like behavior and altered synaptic pruning in the mouse offspring. Brain Behav. Immunol. 63, 88–98 (2017).
Mirabella, F. et al. Prenatal interleukin 6 elevation increases glutamatergic synapse density and disrupts hippocampal connectivity in offspring. Immunity 54, 2611-2631.e8 (2021).
Hayes, L. N. et al. Prenatal immune stress blunts microglia reactivity, impairing neurocircuitry. Nature 610, 327–334 (2022).
Lim, A. I. et al. Prenatal maternal infection promotes tissue-specific immunity and inflammation in offspring. Science 373, eabf3002 (2021).
Kim, E. et al. Maternal gut bacteria drive intestinal inflammation in offspring with neurodevelopmental disorders by altering the chromatin landscape of CD4+ T cells. Immunity 55, 145-158.e7 (2022).
Bettelli, E., Oukka, M. & Kuchroo, V. K. T(H)-17 cells in the circle of immunity and autoimmunity. Nat. Immunol. 8, 345–350 (2007).
Weaver, C. T. & Hatton, R. D. Interplay between the TH17 and TReg cell lineages: A (co-)evolutionary perspective. Nat. Rev. Immunol. 9, 883–889 (2009).
Ellul, P. et al. Regulatory T lymphocytes/Th17 lymphocytes imbalance in autism spectrum disorders: Evidence from a meta-analysis. Mol. Autism. 12, 68 (2021).
Xu, Z. et al. Rescue of maternal immune activation-induced behavioral abnormalities in adult mouse offspring by pathogen-activated maternal Treg cells. Nat. Neurosci. 24, 818–830 (2021).
Funding
This work was supported (in part) by the Fondation FondaMental, Créteil, France and by the Investissements d'Avenir programs managed by the ANR under references ANR-11-IDEX-0004-02 and ANR-10-COHO-10-01.
Author information
Authors and Affiliations
Contributions
P.E. and A.M. contributed to data collection. P.E., H.P. and N.T. analysed and interpreted the data. P.E. wrote the first version of the article and revised it after its revisions by co-authors. V.V., E.H., A.A., A.A., P.A., J.M.B., S.B., O.B., M.B., A.C., N.C., R.C., D.D.F., C.D., M.G., F.G.B., F.G., A.K., M.L., A.L., F.L., C.L., E.M., N.R., C.M.S., M.S., E.Z., participated in the inclusion of children and the revision of the article and approved its final version, and all agreed to be accountable for all aspects of the work. M.R., D.K. and R.D. supervised the conception of this study.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ellul, P., Maruani, A., Vantalon, V. et al. Maternal immune activation during pregnancy is associated with more difficulties in socio-adaptive behaviors in autism spectrum disorder. Sci Rep 13, 17687 (2023). https://doi.org/10.1038/s41598-023-45060-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-45060-z
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
