
Abstract
Hepatic sinusoidal obstruction syndrome (SOS) is a severe and life-threatening complication after allogeneic hematopoietic stem cell transplantation (HSCT). We conducted a multi-center retrospective study to evaluate the utility of our ultrasonographic scoring system for the diagnosis of SOS (HokUS-10) in predicting SOS-related mortality (SOS-RM). We analyzed a total of 42 patients who developed SOS after HSCT. The cumulative incidences of SOS-RM, non-relapse mortality (NRM), and overall survival at day 180 after the diagnosis of SOS were 26.4%, 28.8% and 54.5%, respectively. The area under the receiver operating characteristic curve analysis showed that the optimal cut-off value of HokUS-10 total score to predict SOS-RM was 8 points after the treatment of SOS. In the individual HokUS-10 score, ascites and portal vein flow-related scores (PV mean velocity and PV flow direction) after the treatment of SOS were shown as significant risk factors for SOS-RM. Our study suggested that US findings after the treatment can predict the treatment outcomes for SOS.
Similar content being viewed by others


Introduction
Hepatic sinusoidal obstruction syndrome (SOS) is a severe and life-threatening complication after allogeneic hematopoietic stem cell transplantation (HSCT), characterized by hepatomegaly with quadrant pain, jaundice, and ascites1. Its risk depends on patient characteristics, disease status, conditioning, and prior history of treatments2,3,4. Severe SOS is a risk for multi-organ failure and high mortality5. Therefore, rapid diagnosis and early intervention are critical to improve treatment outcome against SOS. We have established an ultrasonography (US) -based scoring system for the diagnosis of SOS: the Hokkaido US-based scoring system (HokUS-10), consisting of 10 parameters including hepatomegaly, gallbladder wall thickening, ascites, portal vein (PV) and paraumbilical vein (PUV) dilatation, and abnormal blood flow signals in the PV and PUV6. However, the prognostic impact of US findings on treatment outcomes for SOS has never been elucidated.
Materials and methods
Patients and study design
We conducted a multicenter retrospective study to evaluate the association of HokUS-10 scores and treatment outcomes, including engraftment, acute graft-versus-host disease (GVHD), relapse, non-relapse mortality (NRM), overall survival (OS), and SOS-related mortality (SOS-RM) in patients with hematological malignancies who received HSCT between March 2010 and June 2021 in Hokkaido University or Sapporo Hokuyu Hospital, and were clinically diagnosed SOS as modified Seattle criteria7 or EBMT criteria3 and evaluated HokUS-10 before and after the treatment (Table S1). The cut-off score of HokUS-10 for the diagnosis of SOS was defined to 5 (maximum score, 13)6. The study was performed in accordance with institutional ethical guidelines, including the World Medical Association Declaration of Helsinki, and was approved by the institutional review boards of the Hokkaido University (No. 021-0096). Informed consent was obtained from each patient for participation in the study. For patients who could not obtain informed consent, we disclosed the information about this clinical study on the website of our institution and guarantee the opportunity for refusal (opt-out). Since this study is a retrospective study, opt-out disclosure eliminates the need for patient consent.
Definitions
Neutrophil engraftment was defined as an absolute neutrophil count > 0.5 × 109/L on the first of 3 consecutive days, and platelet engraftment was defined as an absolute platelet count > 2.0 × 1010/L without transfusion support on the first of 7 preceding days. Acute GVHD was graded according to the consensus criteria7. Non-relapse mortality (NRM) was defined as death due to any cause other than relapse. Relapse and causes of death were determined based on the decision of each clinician. SOS-RM was defined as death due to organ failure by SOS without relapse8,9. Overall survival (OS) was calculated from the day of SOS diagnosis, with patients alive at the time of last follow-up censored. NRM, relapse and SOS-RM were also calculated from the day of SOS diagnosis. HokUS-10 was evaluated in each institution, and was performed central review at Hokkaido University for this study.
Statistical analysis
Statistical analysis was performed using Mann–Whitney U-test for continuous variables, Kaplan–Meier method, Log-rank test, and Cox proportional hazard model for OS, Gray’s test for engraftment, GVHD, relapse, NRM, and SOS-RM, and Fine and Gray competing risk regression model for NRM and SOS-RM. The cut-off value of HokUS-10 to predict SOS-RM was determined based on receiver operating characteristic (ROC)-curve analysis. Results were expressed as hazard ratio (HR) with the 95% confidence interval (95% CI). A value of P < 0.05 was used to determine statistical significance. All analyses were performed with EZR (Saitama Medical Center, Jichi Medical University, Japan), which is a graphic user interface for R (The R Foundation for Statistical Computing, Vienna, Austria)10.
The authors confirm that this study was conducted in accordance with relevant national, international, and institutional guidelines. The datasets used and/or analyzed during the current study available from the corresponding author on reasonable request.
Results
Patients and transplant characteristics
Patient and transplant characteristics in this study are shown in Table 1. A total of 42 patients were included in this study. The median patient age at the time of transplant was 50 years, ranging from 19 to 67 years. Diagnoses included acute myeloid leukemia (n = 11), malignant lymphoma (n = 11), acute lymphoblastic leukemia (n = 9), myelodysplastic syndrome (n = 6), myeloproliferative neoplasm (n = 4), and multiple myeloma (n = 1). Twenty-two patients were in complete remission at the time of transplantation. Seventeen patients received peripheral blood stem cell transplantation, 13 patients received cord blood transplantation, and 12 patients received bone marrow transplantation, respectively. The conditioning regimen was either total body irradiation-based myeloablative conditioning (n = 15), busulfan-based myeloablative conditioning (n = 13), or reduced-intensity conditioning (n = 14). Ten patients had prior history of transplantation. The median interval from HSCT to SOS diagnosis was 16 days, ranging from 4 to 133 days. Fifteen patients were diagnosed by the modified Seattle criteria, 11 patients were diagnosed by the EBMT classical criteria, and the other 16 patients were diagnosed by the EBMT late-onset criteria. EBMT severity included grade 1 (n = 8), grade 2 (n = 10), grade 3 (n = 15), and grade 4 (n = 9), respectively. Organ failure was observed in 10 patients at diagnosis, including renal failure (n = 6), respiratory failure (n = 3), and both (n = 1). Sixteen patients received defibrotide (DF) and the other received recombinant thrombomodulin (rTM) for the initial treatment.
Clinical outcomes
Neutrophil engraftment and platelet engraftment was achieved in 95.2% (95% CI 82.3–98.8%) and 58.4% (95% CI 41.5–72.0%), respectively (Fig. S1A). The cumulative incidence of overall and grade II–IV acute GVHD at day 100 were 50.4% (95% CI 34.5–64.4%) and 14.4% (95% CI 5.8–26.6%) (Fig S1B). The cumulative incidences of NRM and relapse at day 180 after the diagnosis of SOS were 28.8% (95% CI 15.9–43.0%) and 21.5% (95% CI 10.5–35.1%), respectively (Fig. 1A). With a median follow-up of 892 days for survivors, day 180 and 1-year OS after the diagnosis of SOS was 54.5% (95% CI 38.3–68.1%) and 46.8% (95% CI 31.1–61.0%), respectively (Fig. 1B). The cumulative incidences of SOS-RM at day 180 after the diagnosis of SOS were 26.4% (95% CI 14.1–40.5%) (Fig. 1C). Causes of death in 26 patients were primary diseases (n = 8), SOS (n = 11), multi-organ failure (n = 2), infection (n = 1), interstitial pneumonia (n = 1), GVHD (n = 1), and unknown cause in (n = 2) (Table S2).

NRM/relapse, OS, and SOS-RM. The cumulative incidence of NRM (solid lines) and relapse (dashed lines) (A), Kaplan–Meier plots of OS (B), and the cumulative incidence of SOS-RM (C) after the start of treatment for SOS.
Association of HokUS-10 score with SOS-RM and transplant outcomes
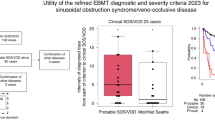
First, we evaluated the association of SOS-RM with total score of HokUS-10 before and after the treatment of SOS. The median days of HokUS-10 evaluation after the start of treatment was 15, ranging from 7 to 21. The median score of HokUS-10 was 6, ranging from 4 to 11, before the treatment, and 5, ranging from 1 to 11, after the treatment. Changes in an individual score of HokUS-10 before and after the treatment were shown in Fig. S2A. Most scores, except for hepatic left lobe vertical diameter and PV diameter, decreased after the treatment. The total HokUS-10 score was decreased in 25 patients, unchanged in 7 patients, and increased in 10 patients before and after the treatment. HokUS-10 scores after the treatment of SOS were significantly higher in patients with SOS-RM compared to that in patients without it (median score, 8.0 vs. 5.0, P = 0.019, Fig. 2A), whereas HokUS-10 scores before the treatment of SOS (median score, 7.5 vs. 6.0, P = 0.077, Fig. 2B) and ratio of HokUS-10 scores before and after the treatment of SOS (median ratio, 1.00 vs. 0.75, P = 0.10, Fig. 2C) were equivalent between the groups.

HokUS-10 total score in patients with or without SOS-RM. HokUS-10 scores in patients with or without SOS-RM post- (A) and pre- (B) treatment for SOS. Ratio of HokUS-10 scores post- and pre-treatment for SOS (C). The ends of the center box indicate the upper and lower quartile of the data, the line inside the rectangle indicates the median, the whiskers indicate the maximum and minimum values, and the dots outside the rectangle indicate outliers.
Next, we performed further analysis for the association of HokUS-10 total score before and after the treatment of SOS with SOS-RM. While our previous study showed the diagnostic value of 5 points on HokUS-10 for SOS, the cumulative incidence of SOS-RM at day 180 after the diagnosis of SOS was not significantly difference between in patients with < 5 and ≥ 5 points of HokUS-10 total score both before and after the treatment of SOS (before: < 5 points, 0.0% vs ≥ 5 points, 29.2%, P = 0.20, after: < 5 points, 13.3% vs ≥ 5 points, 33.6%, P = 0.31). We determined the optimal cut-off value of HokUS-10 to predict SOS-RM. The area under the ROC curve analysis showed that only 8 points after the treatment of SOS became moderate accuracy to predict day 180 SOS-RM (0.71; 95% CI 0.55–0.87, Fig. 3A–C). Consequently, the cumulative incidence of SOS-RM at day 180 after the diagnosis of SOS was significantly higher in patients with ≥ 8 points than < 8 points of HokUS-10 total score after the treatment of SOS (< 8 points, 13.5% vs ≥ 8 points, 58.3%, P = 0.004, Fig. 3D). HokUS-10 total score after the treatment of SOS affected significant prognostic impacts for not only SOS-RM but also NRM (< 8 points, 20.1% vs ≥ 8 points, 50.0%, P = 0.037) and OS (< 8 points, 63.0% vs ≥ 8 points, 33.3%, P = 0.028) (Table S3). Multivariate analysis showed that HokUS-10 total score after the treatment of SOS was a significant risk for SOS-RM (HR, 5.029; 95% CI 1.631–15.51; P = 0.005). On the other hand, no significant risk factor for NRM was identified and EBMT severity was only identified as a significant risk factor for OS (HR, 3.427; 95% CI 1.044–11.26; P = 0.042) (Table 2).

ROC curve analysis of HokUS-10 scoring system to predict SOS-RM. ROC curves to determine the cut-off values with the highest predictive performance by HokUS-10 scoring system before (A) and after (B) the treatment of SOS. Area under the ROC curves calculated by each cut-off value (C). The cumulative incidence of SOS-RM in patients with < 8 (solid line, N = 30) or ≥ 8 points (dashed line, N = 12) of HokUS-10 total score after the treatment of SOS (D).
We also evaluated the association of an individual HokUS-10 score before and after the treatment of SOS with SOS-RM (Table 3). Univariate analysis identified PV mean velocity (HR, 7.94; 95% CI 1.79–35.1; P = 0.006) before the treatment of SOS, and ascites (HR, 3.10; 95% CI 1.33–7.23; P = 0.009), PV mean velocity (HR, 4.13; 95% CI 1.28–13.4; P = 0.018), PV flow direction (HR, 35.6; 95% CI, 8.01–158; P < 0.001) after the treatment of SOS as risk factors for SOS-RM.
Discussion
This multi-center retrospective study showed that HokUS-10 scores 2 weeks after the initiation of SOS treatment was associated with treatment outcomes. HokUS-10 was established based on US finding reported by Lassau et al.11, with the high sensitivity (100%) and specificity (95.8%)6. The advantage of US for the diagnosis of SOS is its ability to detect blood flow abnormalities responsible for the pathogenesis of SOS. Gallbladder wall thickening, dilatation of PUV, or appearance of PUV flow signal reflects congestion of the cystic vein returning to the PV system downstream of sinusoids. However, it remained to be elucidated whether HokUS-10 could predict treatment outcomes for SOS. In this study, we showed that high total scores (≥ 8 points) and ascites and PV flow-related scores (PV mean velocity and PV flow direction) after the treatment of SOS was significantly associated with SOS-RM. EBMT criteria also emphasizes the US findings including ascites and decrease in velocity or reversal of the portal flow as the essential ultrasound evidence of SOS3. Especially, PV flow is converged from the stomach, intestines, pancreas, spleen, and gallbladder, which plays an important role in transporting amino acids absorbed in intestines, hormones produced in pancreas, and decomposition products excreted from spleen to liver. Failure to improve PV flow after the treatment of SOS may reflect extensive sinusoidal obstruction, suggesting poor prognosis. Previous studies also showed the association of PV flow abnormality with poor prognosis in patients with hepatic cirrhosis12,13. Prediction of treatment outcomes for SOS using HokUS-10 scoring system may help to determine timing of cessation of SOS treatment.
Our study has several limitations, including a retrospective design, small sample size. The day of HokUS-10 evaluation after the treatment of SOS was not fixed. Cases with rapid progression after the diagnosis of SOS were not included, because only cases who could evaluate HokUS-10 about 2 weeks after the start of treatment were included in this study. rTM was not used outside Japan, although the previous study showed comparable therapeutic effect between rTM and DF14,15. Treatment outcomes were comparable between patients who received DF and rTM in this study as well.
Nevertheless, our study showed the efficacy of US findings for the prediction of treatment outcomes for SOS. Larger studies should be conducted to confirm our findingsand establish a novel scoring system using US findings for treatment outcomes of SOS.
Data availability
The datasets used and/or analyzed during the current study available from the corresponding author on reasonable request.
References
Bonifazi, F. et al. Diagnosis and treatment of VOD/SOS after allogeneic hematopoietic stem cell transplantation. Front Immunol. 11, 489 (2020).
Yakushijin, K. et al. Sinusoidal obstruction syndrome after allogeneic hematopoietic stem cell transplantation: Incidence, risk factors and outcomes. Bone Marrow Transplant. 51, 403–409 (2016).
Mohty, M. et al. Revised diagnosis and severity criteria for sinusoidal obstruction syndrome/veno-occlusive disease in adult patients: A new classification from the European Society for Blood and Marrow Transplantation. Bone Marrow Transplant. 51, 906–912 (2016).
Corbacioglu, S., Jabbour, E. J. & Mohty, M. Risk factors for development of and progression of hepatic veno-occlusive disease/sinusoidal obstruction syndrome. Biol Blood Marrow Transplant. 25, 1271–1280 (2019).
Coppell, J. A. et al. Hepatic veno-occlusive disease following stem cell transplantation: Incidence, clinical course, and outcome. Biol Blood Marrow Transplant. 16, 157–168 (2010).
Nishida, M. et al. Novel ultrasonographic scoring system of sinusoidal obstruction syndrome after hematopoietic stem cell transplantation. Biol. Blood Marrow Transplant. 24, 1896–1900 (2018).
Przepiorka, D. et al. 1994 consensus conference on acute GVHD grading. Bone Marrow Transplant. 15, 825–828 (1995).
Mohty, M. et al. A multicentre, multinational, prospective, observational registry study of defibrotide in patients diagnosed with veno-occlusive disease/sinusoidal obstruction syndrome after haematopoietic cell transplantation: an EBMT study. Bone Marrow Transplant. 56, 2454–2463 (2021).
Shiratori, S. et al. Serum levels of albumin and creatinine predict the outcome of sinusoidal obstruction syndrome after allogeneic HSCT. Ann Hematol. 101, 2117–2118 (2022).
Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 48, 452–458 (2013).
Lassau, N. et al. Prognostic value of doppler-ultrasonography in hepatic veno-occlusive disease. Transplantation 15, 60–66 (2002).
Kondo, T. et al. Reversed portal flow: Clinical influence on the long-term outcomes in cirrhosis. World J. Gastroenterol. 21, 8894–8902 (2015).
Kirstein, M. M. et al. Retrograde portal vein flow and transarterial chemoembolization in patients with hepatocellular carcinoma—a case-control study. Scand. J. Gastroenterol. 52, 1398–1406 (2017).
Wang, X. et al. Defibrotide stimulates angiogenesis and protects endothelial cells from calcineurin inhibitor-induced apoptosis via upregulation of AKT/Bcl-xL. Thromb. Haemost. 118, 161–173 (2018).
Yakushijin, K. et al. Clinical effects of recombinant thrombomodulin and defibrotide on sinusoidal obstruction syndrome after allogeneic hematopoietic stem cell transplantation. Bone Marrow Transplant. 54, 674–680 (2019).
Acknowledgements
We thank all researchers in North Japan Hematology Study Group (NJHSG).
Author information
Authors and Affiliations
Contributions
S.S. designed the study, analyzed data, performed statistical analyses, and wrote the manuscript. S.S., K.O., J.S., and D.H. included patients. M.N. and T.I. performed ultrasonography and evaluated HokUS-10 scores. S.O. advised on the methods. T.T. advised on the methods, and revised the manuscript. All authors commented and approved the manuscript.
Corresponding author
Ethics declarations
Competing interests
SS, KO, TI, SO and DH have no conflict of interest to declare. JS reports honoraria from Pfizer and scholarship donation from Kyowa Kirin, MN reports grant from NIPPON SHINYAKU, and TT reports grant from Chugai, Kyowa Kirin, Sanofi, Astellas, TEIJIN PHARMA, Novartis, Fuji Pharma, and NIPPON SHINYAKU, honoraria from Merck Sharp & Dohme, Takeda, Kyowa Kirin, Bristol-Myers Squibb, and Pfizer, leadership or fiduciary role from Merck Sharp & Dohme, Takeda, and Novartis, and other financial interests from Janssen and Novartis, during the conduct of the study.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Shiratori, S., Okada, K., Sugita, J. et al. HokUS-10 scoring system predicts the treatment outcome for sinusoidal obstruction syndrome after allogeneic hematopoietic stem cell transplantation. Sci Rep 13, 17374 (2023). https://doi.org/10.1038/s41598-023-43806-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-43806-3
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.

{kind=link}
{kind=link}