
Abstract
A diet high in sodium contributes to a significant proportion of Disability Adjusted Life Years (DALYs) due to cardiovascular diseases. This paper describes the awareness, behaviour and determinants related to dietary salt intake in an adult population of 18–69 years that were assessed as part of the National NCD Monitoring Survey (NNMS) in India. A sub-sample of 3000 adults selected through simple random sampling from 150 nationally representative Primary Sampling Units (PSUs) was included. Data regarding awareness and behaviour related to dietary salt intake were collected. Urinary sodium excretion in spot urine samples was estimated and used to calculate dietary salt intake. The dietary salt intake’s sociodemographic, behavioural and metabolic determinants were also analysed. Less than one-third of the adults of both genders in all age groups in rural and urban areas were aware that daily high salt intake could affect health. The estimated mean daily salt intake was 8.0 g (8.9 g/day for men and 7.1 g/day for women). The salt intake was significantly higher in men [Adjusted OR = 17.66 (5.24–59.46)], rural areas [Adjusted OR = 6.14 (1.83–20.60)], overweight and obese respondents [Adjusted OR = 17.62 (3.17–98.07)]. The perception of the harmful effects of high salt intake and practices to limit salt intake was low in the study population. The mean daily salt intake was higher than the WHO recommendation of up to 5 g daily. The mean dietary salt intake is high in the Indian population, which calls for planning and implementing control of dietary salt consumption measures.
Similar content being viewed by others

Introduction
Cardiovascular diseases (CVD) account for an estimated 28.1% of the total deaths in India. In 2016, 1.63 million deaths were attributable to hypertension compared to 0.78 million deaths in 19901. A diet high in sodium could contribute to 70 million Disability Adjusted Life Years (DALYs’) and 3 million deaths globally because of its association with CVDs2. A high sodium level in the diet also increases the risk of stroke and cardiac failure severity3,4. Besides the harmful cardiovascular effects of salt consumption, it could also be a potential risk factor for gastric cancer5,6. Restricting daily salt intake to the World Health Organization (WHO) recommended level of up to 5 g for adults is a beneficial and cost-saving way to achieve a 25% reduction in the prevalence of raised blood pressure and a 30% reduction in mean population salt intake by 2025. India’s National NCD Monitoring Framework has defined a similar percentage reduction, adapted from WHO’s voluntary global NCD targets7,8.
The WHO urges its Member States to strengthen dietary salt reduction strategies9. The benefits of attaining the WHO’s objective of reducing daily salt consumption to 5 g per adult by 2030 are substantial. This achievement is estimated to prevent an additional 87,870 premature ischemic heart disease (IHD) cases by 2050 and avoid 126,010 premature strokes10. Realising this target would generate an estimated £1260 million in extra healthcare savings alongside these health improvements. While the rationale for salt reduction provided by scientific evidence is robust, the quantum of available data is insufficient to translate such scientific insights into policies for reducing population salt intake. Preventing dietary salt intake must be driven by perceptions, behaviours, and practices influenced by diverse socio-economic and socio-cultural factors. Studies on the assessment of salt intake in India have been done in limited geographical settings; hence the result findings may not apply at a national level11,12,13. The lack of comprehensive data draws attention to the need for a national-level monitoring system to generate evidence on dietary salt intake, knowledge, attitude and practices. Feasible and standard methods of salt estimation incorporated into surveys helps monitor and plan better. These include 24-h urine measurement and spot urine measurement14. Although the 24-h urine collection method is acknowledged as the ‘gold standard’ approach for assessing salt intake, collecting urine over a whole day is laborious, costly, inconvenient, and intricate for the individuals involved. Spot urine has been widely used and validated to estimate dietary sodium15,16,17,18.
The Indian Council of Medical Research—National Centre for Disease Informatics and Research, Bengaluru undertook a comprehensive National NCD Monitoring Survey (NNMS) to establish a monitoring system that addresses the progress toward achieving the national NCD targets19. This study aimed to estimate the mean dietary salt intake and assess the awareness, behaviour and determinants of salt intake in an adult population of 18–69 years.
Materials and methods
Survey setting, population and sampling
The National NCD Monitoring Survey (NNMS) 2017–18 was conducted on a sample of 12,000 adults in the 18 to 69 age group to generate national-level key NCD-related indicators identified in the national NCD monitoring framework, the details of which are published elsewhere20. Urinary sodium excretion in spot urine samples was estimated in a subsample of 3000 adults, selected through simple random sampling in 150 nationally representative Primary Sampling Units, of which 75 were in urban, and the other 75 were in rural areas. Data was collected regarding awareness of the adverse health effects of high salt intake and the importance of lowering dietary salt intake. ‘Behaviour’ alluded to actions regarding salt intake in the daily diet. The sociodemographic, behavioural and metabolic determinants of dietary salt intake estimated from spot urinary samples were also analysed.
Data and sample collection
The study instrument for the survey was developed from reliable resources related to NCD risk factor surveillance21,22,23. Study participants were recruited after written and verbal consent. Qualified and trained medical social workers collected details at the household, individual and health facilities. Data on behaviours, perceptions and attitudes related to salt use were collected through face-to-face interviews. Camps were organised to conduct anthropometric, blood pressure and blood glucose measurements and collection of urine samples. A day before the camp, consenting participants were given 30 mL wide-mouthed labelled sterile urine collection bottles with a barcode specific to a selected adult to avoid sample mismatch. The spot urine sample was gently shaken to ensure homogeneity and transferred to 2 mL collection vials using Pasteur’s pipettes. The vials were then placed in a 9 × 9 storage box in a vaccine carrier containing ice packs for safe transportation at 4 °C to pre-appointed storage facilities, stored at − 20 °C till further shipment to a reference laboratory at the Department of Cardiac Biochemistry, All India Institute of Medical Sciences, New Delhi. The samples were tested in batches of 80 to 100 each.
Estimation of urinary sodium
The indirect Ion-Selective Electrode (ISE) method was used to estimate urinary sodium (Na) and potassium (K) levels using automated analysers (AU680 Chemistry analyser, Beckman Coulter, CA, USA)24. The ISE method has several advantages: it is faster, more accurate, and has lesser sample requirements. The measurable range is 20–200 mmol/L with a precision of < 0.1%. Internal Quality Control (IQC) samples in normal and pathological ranges were run for each batch of urine samples. Jaffe’s method was employed for urinary creatinine level estimation using Roche analyser (P800 Modular Analytics, Roche Diagnostics, Mannheim, Germany) through a commercial kit (Ref. 11,875,418–216, Roche diagnostics, Germany). The dietary salt intake from the spot urine sample was estimated using the INTERSALT (International Cooperative Society on Salt and Blood Pressure) equation with potassium for each sex25. The value obtained in mmol/L was multiplied by 2.54 to derive the daily mean salt intake in grams per day.
Data analysis
Data were cleaned using the IBM Statistical Package for Social Sciences (SPSS) windows—version 22.0. The statistical analysis using weighted data was carried out in STATA 14.1 using a complex survey analysis method26. Descriptive analysis was used to present results on the behaviour, perception and practices related to salt intake. The data distribution was checked using the graphical representation and then tested for normality with the Shapiro–Wilk test. Mean weighted salt intake comparison between the subgroups (sociodemographic, rural/urban, behavioural, physiological and metabolic risk factors) was made using the Student’s independent samples t-test and Analysis of Variance (ANOVA) test. Logistic regression analysis was carried out to determine the relationship between independent variables, and those variables with a p-value < 0.25 were taken in the multivariate analysis27. The final multivariate-adjusted model was fitted by adjusting the variables which included age, gender, area of residence, educational status etc.
Ethics approval
This study was approved by the Institutional Ethics Committee of the Coordinating Centre, ICMR-NCDIR. Approval no: NCDIR/IEC/2017/4 dated 03 February 2017. Before starting the survey, every implementing agency obtained its ethics approval from its Institutional Ethics Committee. Informed consent was obtained from all the study participants. As a post-research benefit, trained social investigators counselled the study participants to reduce salt consumption. They were also provided with a brochure describing tips for a healthy lifestyle in the local language. Since the research involved human participants, it was conducted per the Declaration of Helsinki.
Results
10,659 adults aged 18–69 years participated in the survey (response rate of 96.3%). Among the subsample of adults selected for the urinary sodium excretion study, 2643 study participants provided spot urine samples, of which 2266 (85.7%) samples were the final number of samples processed and included for analysis. The remaining 377 either had incomplete interviews or the urine samples were contaminated. A flow diagram that indicates the inclusion of study participants is shown in the supplementary file.
Awareness and behaviour of the population on dietary salt intake
The proportion of adults who knew that daily high salt intake could affect health was less than one-third among respondents in all age categories, gender, rural–urban areas and those without education. However, over half of the participants were familiar with the importance of lowering salt intake in the diet. The percentage of adults who used extra salt in food or consumed too many salt-containing products was less than a quarter in all the sub-categories of sociodemographic, behavioural and metabolic factors (Table 1).
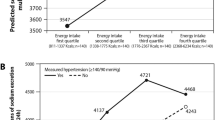
Weighted mean salt intake estimates according to the sociodemographic profile of the study population
A salt intake of > 5 g/day was observed across all the strata, as shown in Table 2. The estimated mean daily salt intake was 8.0 g (8.9 g/day for men and 7.1 g/day for women). The daily mean salt intake was significantly higher (p < 0.0001) in men (8.9 g), employed (8.6 g), current tobacco users (8.3 g), obese (9.2 g) and those with raised blood pressure (8.5 g). The population characteristics and their weighted mean dietary salt intake estimates in India from spot urinary samples according to age groups (18-44 and 45-69 years) and gender are shown in the Supplementary text.
Association between sociodemographic, behavioural, physiological and metabolic factors with salt intake
A salt intake of > 5 g per day was significantly higher in men than women [Unadjusted OR = 6.69 (2.52–17.72)]; [Adjusted OR = 17.66 (5.24–59.46)], among rural participants than in urban [Adjusted OR = 6.14 (1.83–20.60)], overweight and obese persons [Unadjusted OR = 10.95 (2.24–53.50); Adjusted OR = 17.62 (3.17–98.07)]. The findings are presented in Table 3.
Consumption of high salt containing foods among adults
Approximately 43.8% of adults indicated that they consumed high-salt homemade food items every week (1–6 days per week), while 36.1% reported consuming salty snacks like namkeen, papad, and packaged chips at least once a month (1–3 days or less than once a month), as seen in Fig. 1.

Frequency of consumption of high salt containing foods among adults.
Discussion
The present study provides a national-level description of the awareness and behaviour of dietary salt intake and its determinants in terms of the sociodemographic (age, sex, area, education and employment), behavioural (current tobacco and alcohol use, physical activity and yoga practice), physiological (body mass index, blood pressure) and metabolic factors (blood glucose and cholesterol level) in the Indian population. While most respondents knew the importance of reducing dietary salt consumption, the proportion of those who perceived that a daily high salt intake could affect one’s health was low. The pattern of perception and behaviour did not substantively vary according to sociodemographic, behavioural and metabolic factors. These findings are similar to the survey conducted in Delhi, Haryana, and Andhra Pradesh, in which salt intake-related awareness and behaviour did not vary across different levels of education28. Studies done in specific and geographically limited settings have shown varying results. Close to two-thirds (64%) of the participants residing in an urban slum in Chandigarh, North India, did not consider lowering the salt intake important29. In another community-based study in North India, 46·6% from rural Haryana and 45·1% from urban Delhi were aware of the need to reduce dietary salt content30. In our study, it was positive to note that less than a third of the respondents affirmed that they added extra salt to their food or consumed far too many salty items. However, less than half of the study participants practised measures to control dietary salt intake. The most commonly adopted step was avoiding meals outside of the home (Supplementary Table S1).
In the present study, the weighted mean salt intake was more than the WHO-recommended salt intake of up to 5 g per day across all groups categorised according to the sociodemographic, behavioural and metabolic factors groups. Similar findings have been reported in other studies done in India. A systematic review of the mean salt intake in India found the observed value of 11 g per day31. Analogous study findings for mean dietary salt intake were reported in Andhra Pradesh (8.72 g/day) and Delhi, Haryana (5.62 g/day), which was calculated from the average estimates from two 24-h dietary recall surveys. The Chennai Urban Rural Epidemiology (CURE) study also observed the mean salt intake as 8.5 g/day, using the food frequency questionnaire (FFQ)32. The mean salt intake in women in an urban resettlement colony in Delhi was 7.6 g/day based on spot urine sodium measurements13. Some methods, such as dietary surveys, are time-consuming and have a low validity33,34. Even samples of dried urine obtained from spot collection samples are a clinically valid and convenient alternative to liquid urine to analyse sodium concentration under field conditions35. The salt intake was significantly higher in men, the rural population, the employed, overweight and obese. Similar findings on higher salt intake in males36,37, rural people30, and obese individuals38,39 were seen in other studies.
The salt added during food preparation constitutes the primary source of dietary salt in low- and middle-income such as India40. Studies conducted in high-income countries observed the average salt intake of 9–12 g daily; processed foods comprised the primary source41,42. However, with the socio-economic progress and changing lifestyle, India is witnessing a ‘nutrition transition’ wherein there is a decrease in the consumption of wholesome foods and an increasing reliance on packaged and processed food43,44.
Our study showed that the mean dietary salt intake to be high in the Indian population, which calls for planning and implementing control of dietary salt consumption measures. The results pave the way for the planning and implementing control of dietary salt consumption measures in the Indian population. A universal reduction in the dietary sodium consumption of at least 1.2 g per day would help achieve a 50% reduction in the proportion of persons who require anti-hypertensive treatment45. An awareness of the adverse health effects could substantially influence the willingness to curb excessive salt consumption. The findings on perceptions and practices related to salt intake could help design effective consumer education and awareness programmes. However, awareness generation alone may not always successfully bring about behavioural change46. A multisectoral and coordinated approach is essential to ensure actual limitations of salt intake. Intensive efforts should be leveraged through National Multi-sectoral Action Plan, which includes salt reduction as an active component. The Food Safety and Standard Authority of India (FSSAI) has played a significant role in generating awareness and encouraging community involvement through ‘The Salt Challenge, Every Pinch Counts’47. Instead of sodium chloride, low sodium salt substitutes have potassium chloride for reducing sodium content, although these are more expensive than regular salt. Framing of policies to scale up the availability and affordability of low sodium salt substitutes should be promoted to ascertain a reduction in the mean population salt intake. Other potential measures include mass awareness, training of food vendors and clear labelling of sodium content in packaged foods.
Strength and limitations
Our study was conducted in a nationally representative sample wherein dietary sodium intake was estimated from spot urine samples, a validated method used to assess dietary sodium intake. The population mean was calculated using sampling weights; thus, the study findings could be generalised at a population level and used to plan and implement dietary salt control measures. The information on awareness and behaviour of salt intake was self-reported and could be subjected to information bias. The study did not capture data on the actual dietary sources of salt in food items and condiments for any correlation analysis.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Indian Council of Medical Research, Public Health Foundation of India and Institute for Health Metrics and Evaluation. India: Health of the Nation’s States—The India State-Level Disease Burden Initiative. New Delhi, India. https://phfi.org/the-work/research/the-india-state-level-disease-burden-initiative/ (2017).
Afshin, A. et al. Health effects of dietary risks in 195 countries, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 393, 1958–1972 (2019).
Li, X., Cai, X., Bian, P. & Hu, L. R. High salt intake and stroke: Meta-analysis of the epidemiologic evidence. CNS Neurosci. Ther. 18, 691–701 (2012).
de Wardener, H. & MacGregor, G. Harmful effects of dietary salt in addition to hypertension. J. Hum. Hypertens. 16, 213–223 (2002).
Wang, X. Q., Terry, P. D. & Yan, H. Review of salt consumption and stomach cancer risk: Epidemiological and biological evidence. World J. Gastroenterol. 15, 2204–2213 (2019).
D’Elia L, Galletti F, Strazzullo P. Dietary salt intake and risk of gastric cancer. Adv. Nutr. Cancer 83–95 (2014).
Ministry of Health and Family Welfare, Government of India. National Action Plan and Monitoring Framework for Prevention and Control of Non-communicable Diseases (NCDs) in India. Developed through the WHO-Government of India 2012–2013. http://origin.searo.who.int/entity/india/topics/cardiovascular_diseases/National_Action_Plan_and_Monitoring_Framework_Prevention_NCDs.pd
World Health Organization. NCD Global Monitoring Framework. https://www.who.int/publications/i/item/ncd-surveillance-global-monitoring-framework
World Health Organization. Salt Reduction. https://www.who.int/news-room/fact-sheets/detail/salt-reduction
Alonso, S. et al. Impact of the 2003 to 2018 population salt intake reduction program in England: A modeling study. Hypertension 77(4), 1086–1094 (2021).
Johnson, C. et al. Sources of dietary salt in North and South India estimated from 24 hour dietary recall. Nutrients 11, 318 (2019).
Ravi, S. et al. Sodium intake, blood pressure, and dietary sources of sodium in an adult South Indian population. Ann. Glob. Health 82, 234 (2016).
Aparna, P. et al. Salt intake among women in an urban resettlement colony of Delhi. Indian J. Public Health 64, 393 (2020).
WHO SEARO Salt Reduction Toolkit. https://cdn.who.int/media/docs/default-source/searo/healthy-diets/salt-reduction/measurement-of-population-salt-intake.pdf?sfvrsn=b8e360f4
Krishnan, A. et al. Performance of equations for estimation of 24-hour urinary sodium from morning fasting urine samples in a multisite study in India. Natl. Med. J. India 35, 4–10 (2022).
World Health Organisation. Strategies to Monitor and Evaluate Population Sodium Consumption and Sources of Sodium in the Diet. Report of a Joint Technical Meeting Convened by WHO and the Government of Canada. http://whqlibdoc.who.int/publications/2011/9789241501699_eng.pdf (2010).
Petersen, K. et al. Estimating population salt intake in India using spot urine samples. J. Hypertens. 35, 2207–2213 (2017).
Huang, L. et al. Mean population salt intake estimated from 24-h urine samples and spot urine samples: A systematic review and meta-analysis. Int. J. Epidemiol. 45, 239–250 (2016).
Indian Council of Medical Research–NCDIR. National Non -communicable Disease Monitoring Survey (NNMS) 2017–18. Bengaluru, India. https://www.ncdirindia.org/nnms/resources/Initial_Content.pdf
Mathur, P. et al. National noncommunicable disease monitoring survey (NNMS) in India: Estimating risk factor prevalence in adult population. PLoS ONE 16, e0246712 (2021).
National Institute of Medical Statistics, Indian Council of Medical Research (ICMR). 2009, IDSP Non-Communicable Disease Risk Factors Survey, Phase-I States of India, 2007–2008.
World Health Organization. Monitoring and surveillance of non-communicable diseases, STEP wise approach to surveillance (STEPS). https://www.who.int/ncds/surveillance/steps/en/
Centres for Disease Control and Prevention, Global Adult Tobacco Survey Collaborative Group. Global Adult Tobacco Survey (GATS): Core Questionnaire with Optional Questions, Version 2.0. (2010).
Pelleg, A. & Levy, G. B. Determination of Na+ and K+ in urine with ion-selective electrodes in an automated analyser. Clin. Chem. 21, 1572–1574 (1975).
Brown, I. et al. Estimating 24-hour urinary sodium excretion from casual urinary sodium concentrations in western populations. Am. J. Epidemiol. 177, 1180–1192 (2013).
Taylor Lewis. Analysing Categorical Variables from Complex Survey Data Using PROC SURVEYFREQ 2013. https://www.mwsug.org/proceedings/2013/AA/MWSUG-2013-AA10.pdf
Mickey, J. & Greenland, S. A study of the impact of confounder-selection criteria on effect estimation. Am. J. Epidemiol. 129, 125–137 (1989).
Johnson, C. et al. The association of knowledge and behaviours related to salt with 24-h urinary salt excretion in a population from North and South India. Nutrients 9, 144 (2017).
Bhattacharya, S., Thakur, J. S. & Singh, A. Knowledge attitude, and practice regarding dietary salt intake among urban slum population of North India. J. Fam. Med. Prim. Care. 7, 526–530 (2018).
Garg, V. et al. Knowledge, attitudes and practices related to dietary salt intake among adults in North India. Public Health Nutr. 22, 1606–1614 (2019).
Johnson, C. et al. Mean population salt consumption in India. J. Hypertens. 35, 3–9 (2017).
Radhika, G., Sathya, R. M., Sudha, V., Ganesan, A. & Mohan, V. Dietary salt intake and hypertension in an urban south Indian population—[CURES-53]. J. Assoc. Physicians India 55, 405–411 (2007).
Gemming, L., Jiang, Y., Swinburn, B., Utter, J. & Mhurchu, C. N. Under-reporting remains a key limitation of self-reported dietary intake: an analysis of the 2008/09 New Zealand Adult Nutrition Survey. Eur. J. Clin. Nutr. 68, 259–264 (2013).
Holbrook, J. et al. Sodium and potassium intake and balance in adults consuming self-selected diets. Am. J. Clin. Nutr. 40, 786–793 (1984).
Tarik, M. et al. Feasibility of measuring sodium, potassium and creatinine from urine sample dried on filter paper. Bioanalysis 11, 689–701 (2019).
Johnson, C. et al. Mean dietary salt intake in urban and rural areas in India: A population survey of 1395 persons. J. Am. Heart Assoc. 6, e004547 (2017).
Abdul, A. N. et al. Risk factors related with high sodium intake among Malaysian adults: Findings from the Malaysian Community Salt Survey (MyCoSS) 2017–2018. J. Health Popul. Nutr. 40(S1), 14 (2021).
Jiet, J. L. & Soma, R. M. High salt diets in young university adults and the correlation with blood pressure protein intake and fat free mass. Biosci. Horiz. Int. J. Stud. Res. 10, hzx003 (2017).
Oh, S., Koo, H., Han, K., Han, S. Y. & Chin, H. J. Associations of sodium intake with obesity, metabolic disorder, and albuminuria according to age. PLoS ONE 12, e0188770 (2017).
Brown, I., Tzoulaki, I., Candeias, V. & Elliott, P. Salt intakes around the world: implications for public health. Int. J. Epidemiol. 38, 791–813 (2009).
Fischer, P., Vigneault, M., Huang, R. & Arvaniti, P. Sodium food sources in the Canadian diet. Appl. Physiol. Nutr. Metab. 34, 884–892 (2009).
Mhurchu, C. N. et al. Sodium content of processed foods in the United Kingdom: Analysis of 44,000 foods purchased by 21,000 households. Am. J. Clin. Nutr. 93, 594–600 (2010).
Ramachandran, P. Nutrition transition in India. Nutr. Found India 32, 1–8 (2011).
Misra, A. et al. Nutrition transition in India: Secular trends in dietary intake and their relationship to diet-related non-communicable diseases. J. Diabetes 3, 278–292 (2011).
Reddy, K. & Katan, M. Diet, nutrition and the prevention of hypertension and cardiovascular diseases. Public Health Nutr. 7, 167–186 (2004).
Trivedi, M., Sridhar, K. & Kumar, A. Impact of healthy alternatives on consumer choice: A balancing act. J. Retail. 92, 65–82 (2016).
Food Safety and Standards Authority of India. The Salt Challenge, Every Pinch Counts. https://fssai.gov.in/NetProFaN/assets/netpro/events/Salt%20Challenge.pdf
Acknowledgements
The support provided by the World Health Organization (WHO), ICMR and MoHFW, GoI and the contribution of the implementing agencies is duly acknowledged.
Funding
This study was funded by the Ministry of Health and Family Welfare (MoHFW), Govt of India.
Author information
Authors and Affiliations
Contributions
P.M., A.N., V.K.: wrote the manuscript. P.M., V.K., V.U.K.S.: and L.R. did the investigations. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Mathur, P., Kulothungan, V., Nath, A. et al. Awareness, behavior, and determinants of dietary salt intake in adults: results from the National NCD Monitoring Survey, India. Sci Rep 13, 15890 (2023). https://doi.org/10.1038/s41598-023-42694-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-42694-x
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
