
Abstract
To investigate the effects of radiation exposure due to the Fukushima nuclear power plant accident, following the disaster Fukushima Prefecture launched thyroid ultrasound examinations of residents who were generally younger than 18 years at the time of the earthquake. As the rate of pediatric thyroid cancer was higher than expected, we conducted biological dose assessment based on the frequency of translocated chromosome (Tr) aberrations using peripheral blood lymphocytes. Tr formation frequency was compared among the thyroid cancer (n = 38, median age 18 years, age range 12–26 years), thyroid-related disease (n = 30, median age 21 years, age range 15–28 years), and healthy controls (n = 31, median age 22 years, age range 20–23 years) groups. Tr aberration frequency was initially significantly higher in the thyroid cancer than in the other two groups; however, differences among the groups disappeared after adjusting for history of CT scan, as 92%, 67%, and 28% of those in the thyroid cancer, thyroid-related disease, and control groups, respectively, had undergone CT previously. Therefore, the significant difference in the initial number of Tr formations is presumably due to radiation exposure from CT. Accordingly, the effects of medical exposure on the chromosomes of children and adolescents should be noted.
Similar content being viewed by others

Introduction
The Great East Japan Earthquake (GEJE) of 11 March, 2011 and the subsequent tsunami caused an accident at the Fukushima Daiichi Nuclear Power Plant that resulted in widespread of radioactive contamination in Fukushima Prefecture (FP). After the accident at the Chernobyl Nuclear Power Plant in 1986, there was an increase in cases of pediatric thyroid cancer due to internal radiation exposure, which is characterized by a 4–5 year latent period followed by a rapid increase in incidence1,2,3,4. Therefore, primary examination of the Thyroid Ultrasound Examination (TUE) program conducted in FP in 2011–2013, and included 367,649 subjects (81.7% coverage)) who were generally ≤ 18 years old and living in FP at the time of the disaster. Conducting the TUE immediately after the GEJE enabled comparison of the obtained results with subsequent occurrence of thyroid cancer (5). Thereafter, primary examinations of TUE were conducted every two years until the examined individual was ≥ 20 years, with milestone examinations conducted every five years thereafter. As of 30 June, 2021, 263 of the examined individuals were found to have malignant or suspected malignant5.
The prevalence of thyroid cancer in Japan can be estimated from its incidence in people aged 15–19 years, which is 1.2 per 100,000 men and 3.3 per 100,000 women6. The number of patients in FP diagnosed with thyroid cancer through the TUE is clearly high. However, no significant differences in the incidence rate of thyroid cancer has been found between regions within FP, and no association has been identified between external radiation dose and the prevalence of thyroid cancer5,7,8,9,10,11. It has therefore been speculated that the increase in the incidence of thyroid cancer in FP after the GEJE is due to the effect of aggressive screening by the pediatric TUE12,13. As of 1 August, 2022, thyroid equivalent doses (the sum of internal and external doses) could be estimated based on the GEJE behavioral survey for 108 individuals (41.1% of patients with thyroid cancer), with a median value of 2.2 mSv (range 0.11–22.70)14.
However, biological dose assessment has not been performed for each thyroid cancer patient, and it has been 12 years since the nuclear accident, which makes it very difficult to estimate the dose to the thyroid gland. As alternative techniques, two biological dosimetry methods employ biomarkers of chromosome damage biomarker of peripheral bloods (PB) at the time of ionizing radiation exposure: one is based on the number of dicentric chromosomes (Dic), which is the international gold standard for acute exposure; and the other is based on the number of translocated chromosomes (Tr), which are stable type chromosomes, for chronic exposure15. In the case that several years have passed since radiation exposure, the latter method can be used to evaluate the effective dose, which is the dose to the whole body. For this purpose, dose–response curves are required for each institution. We have generated response curves in the low-dose range (8 doses: 0–1000 mGy) for Dic and Tr analysis from the PB of five healthy subjects16. We have also showed an increase in the number of Dic formations after a single CT scan examination17,18 and reported that it is difficult to find significant changes in the number of Tr formations after a single CT examination18,19.
In this study, we analyzed the number of Tr formations among patients with thyroid cancer, patients with thyroid-related disease (non-thyroid cancer), and healthy individuals of the same age as control in FP, with the aim of elucidating whether the occurrence of thyroid cancers detected in the TUE program is related to radiation exposure.
Results
Subject background data
Of 38 individuals diagnosed with thyroid cancer, 34 had papillary carcinoma and 4 had follicular carcinoma (Table 1). Thirty-five of the 38 (92%) patients had undergone a CT examination prior to PB collection (Fig. 2A), including 5 who had undergone CT more than once. In most of these patients, the scan sites were the neck and chest. In three patients, the scan range was from the neck to abdomen or from the neck to pelvis, and CT of the head was performed in one patient (Table 1).
The 30 patients with thyroid-related diseases (non-thyroid cancer) were diagnosed mainly based on pathological examination of the surgical specimens, including 14 patients with adenomatous goiter (AG), 7 with follicular adenoma (FA), and 3 with Basedow's disease. The remaining patients were diagnosed with benign diseases due to the lack of a definite pathological diagnosis (Table 2). Twenty of the 30 (67%) patients had undergone a CT examination prior to PB collection (Fig. 2A), including 2 patients who had undergone CT more than once. The body regions scanned were similar to those for the patients with thyroid cancer and were most commonly the neck and chest. The scan range was from the neck to abdomen in two patients (Table 2).
Seven of the 31 (23%) individuals in the control group had undergone a CT examination prior to PB collection (Fig. 2A), of whom one had undergone CT more than once. The body regions scanned were the abdomen in two individuals and the head in five individuals; one individual underwent one abdominal CT examination because of a surgery for appendicitis in childhood, and another one individual underwent three abdominal CT examinations because of suspected ischemic enteritis due to bloody stools in childhood. The other five individuals who underwent head CT examination were for examination at the time of head contusion in childhood (Table 3).
Frequency of Tr formations
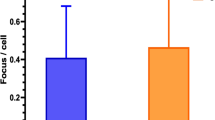
First, we compared the number of age-adjusted Tr aberration among the thyroid cancer, thyroid-related disease (non-thyroid cancer), and control groups. Significant difference was found between the thyroid cancer and thyroid-related diseases groups (p = 0.0124) and between the thyroid cancer and control groups (p = 0.0037), but not between the thyroid-related diseases and control groups (p = 0.7035) (Fig. 1).

Comparison of age-adjusted translocated chromosome (Tr) frequency (per 100 cells) among three groups: thyroid cancer, thyroid-related disease (non-thyroid cancer), and controls. Significant difference was found between the thyroid cancer and thyroid-related disease groups (p = 0.0124) and between the thyroid cancer and control groups (p = 0.0037), but not between the thyroid-related disease and control groups (p = 0.7035). The top of the box indicates the position of 75% and the bottom the 25% of the inter-quartile range, the horizontal line inside the box indicates the median value, and the diamond indicates the mean value. The circle above is an outlier, the line above the vertical line is the largest value indicating [the top of the box + inter-quartile range × 1.5], and the line below the vertical line is the smallest value indicating [the bottom of the box + inter-quartile range × 1.5].
Second, there was no significant difference in age-adjusted Tr aberration frequency between males and females (Supplementary Fig. S1). In patients with thyroid cancer or non-thyroid cancer, CT examination of the neck and chest was performed as part of the standard pre-surgical workup, particularly in those with thyroid cancer, 92% of whom underwent CT (Fig. 2A).

Comparison of age-adjusted Tr frequency (per 100 cells) among the three groups after adjustment for sex and a history of CT examination. (A) Number of individuals in each group with a history of CT examination. (B) After adjusting for sex and a history of CT examination, comparison of age-adjusted Tr frequency showed no significant difference between the thyroid cancer and thyroid-related disease groups (p = 0.0951), between the thyroid cancer and control groups (p = 0.0657), and between the thyroid-related disease and control groups (p = 0.6354). (C) In those who had undergone CT examination, comparison of age-adjusted Tr frequency after adjustment for sex showed no significant difference between the thyroid cancer and thyroid-related disease groups (p = 0.1730), between the thyroid cancer and control groups (p = 0.0598), and between the thyroid-related disease and control groups (p = 0.3690). See note on Fig. 1 for figure description.
In our previous study, we reported chromosome aberrations due to radiation exposure during a single CT scan17,18,19, and recommended that the effects of CT examination should be considered, especially in children. In fact, there was a significant difference in age-adjusted Tr aberration frequency between those who did and did not undergo CT examination (Supplementary Fig. S2). Therefore, although there was no significant difference in age-adjusted Tr aberration frequency between males and females, we compared the frequency (per 100 cells) among the thyroid cancer, thyroid-related disease (non-thyroid cancer), and control groups after adjusting for sex and history of CT examination. The results showed no significant difference among the three groups (Fig. 2B). Furthermore, we found no significant difference in frequency when we compared age-adjusted Tr aberration frequency among those with a history of CT examination (Fig. 2C).
In conclusion, a comparison of age-adjusted Tr aberration frequency among the three groups of thyroid cancer patients, thyroid-related disease (non-thyroid cancer) patients, and the controls revealed a slight increase in age-adjusted Tr formation in patients with thyroid cancer, but the difference was not significant after adjusting for sex and a history of CT examinations. These findings suggest that CT examinations performed prior to treatment may have affected Tr formation in patients with thyroid cancer.
We also compared Tr frequency before age-adjustment among the same three groups as above, and similar results were obtained (Supplementary Fig. S3).
Discussion
The purpose of this study was to investigate whether radiation exposure due to the nuclear accident is the cause of the higher number of thyroid cancer cases found in the pediatric TUE program in FP compared with the estimated number from the cancer registry6. More than 10 years after the GEJE, the relationship between the occurrence of thyroid cancer and thyroid equivalent dose has not been fully analyzed, for the reason that estimated individual thyroid equivalent doses based on the behavioral survey for the 4 months immediately after the GEJE conducted by FP20 have only been analyzed for about 40% of patients with thyroid cancer14. Alternatively, effective doses above 250 mSv can be estimated based on the number of Tr formations using PB lymphocytes15. However, unlike analysis of Dic formation, which is used to estimate dose in the acute phase after radiation exposure, analysis of Tr formation is susceptible to long-term effects such as smoking, drugs, and natural radiation. Our previous studies revealed an increase in Dic formations after a single CT scan17, but it was impossible to find a significant increase in Tr formations19, which theoretically are produced in about an equal ratio to Dic formations21,22, and we did not find an accumulative increase in Tr formations after three consecutive CT scans18. It is thought that the reason for these findings is the influence of the above confounding factors, especially in subjects who are middle-aged or older. Conversely, the present subjects were young (mean age, approximately 20 years), and we therefore considered the effect of confounding factors to be small. If the Tr formations in the present study were caused mainly by radiation exposure, the majority might have been exposed to about 100 mSv, regardless of their history of CT examination based on the calibration curves of our 23-year-old healthy subjects16, which is too high when compared to the external exposure dose estimated from the behavioral survey23,24. As we have learned from our dose–response curves16, there are age-related differences in the Tr formation even in healthy subjects, which accordingly suggests that a dose–response curve for at least every 10 years might be necessary. Therefore, it is difficult to determine radiation exposure below 100 mSv based on the number of Tr formations.
A significant feature of the present study is that rather than performing a comparison between two groups (thyroid cancer and healthy control groups), Tr aberration frequency was compared among three groups, and included patients with benign thyroid tumors and other thyroid-related diseases other than thyroid cancer. Initially, Tr aberration frequency was significantly higher in patients with thyroid cancer (Fig. 1), which we suspected was due to genetic instability, as has been proposed for many cancer diseases25. In fact, the thyroid cancer found in patients in Fukushima was reported to have a different genetic abnormality to those in Chernobyl26,27. However, there was a significant difference in Tr aberration frequency between patients with and without a history of CT examination (Supplementary Fig. S2), and the difference was no longer statistically significant after adjusting for sex and a history of CT examination (Fig. 2B). In addition, comparison of Tr aberration frequency among only those subjects with a history of CT examination showed no significant difference (Fig. 2C).
Almost all of patients with thyroid cancer or with a benign thyroid tumors had underwent CT examination prior to surgical treatment of the thyroid gland, which was mainly CT of the neck and chest. As in our previous studies17,19, in which subjects were analyzed using the WAZA-ARI system, we estimated the effective dose28,29,30 as 7.1 ± 1.3 (mean ± standard deviation) mSv (n = 8) for CT of the neck, 22.8 ± 9.4 mSv (n = 4) for CT of the chest, and 54.5 ± 7.9 mSv (n = 3) for CT from the chest to pelvis. Furthermore, the effective dose for the head using the same CT equipment as above was approximately 1.8 mSv for a standard Japanese body type of adult. Although WAZA-ARI could have been used to estimate past exposure doses based on the specific detailed of each CT scanning site, in the present study we did not consider differences in the number of CT examinations or CT scanning sites for the following reasons: (1) CT equipment differed between facilities; (2) some thyroid cancer and non-thyroid cancer patients, including some of the control subjects, had multiple CT examinations; (3) effective dose of head CT, which was more frequently performed in the control subjects, is lower than those for other CT scanning sites by WAZA-ARI; and (4) estimation of radiation exposure dose below 100 mSv based on the number of Tr formation is difficult, as mentioned above.
If the initial higher Tr aberration frequency in the thyroid cancer group had been caused by radiation exposure from the nuclear power plant accident, then the frequency should have remained significantly higher in that group even after adjusting for a history of CT examination. However, the significant difference among the three groups disappeared after adjusting for a history of CT examination. Furthermore, the subjects in this study were younger than 30 years of age, and the effect of confounding factors is considered small. Therefore, we consider the CT examinations to have the greatest impact on the occurrence of chromosomal translocations. Accordingly, we consider that radiation exposure by CT examination is the most likely cause of the increased Tr aberration frequency.
Unfortunately, external exposure doses based on behavioral surveys have been obtained in only about 28% of residents of FP23,24, and thus there were insufficient such results in the present subjects for inclusion in this study. However, in more than 97% of the evacuees who do have behavioral survey records, the external exposure dose has been reported as 3 mSv or less23, and an analysis of the representativeness of individual external doses has indicated that if they lived in the same area where the residents with known exposure doses lived at the time of the GEJE, their exposure dose levels were the same as those of residents with known exposure doses31. Therefore, as already reported, no relationship has been found between the occurrence of pediatric thyroid cancer in FP and external exposure doses, absorbed doses in the thyroid gland, or place of residence5,7,8,9,10,11. The results of this study support the claim that the occurrence of pediatric thyroid cancer in FP was not caused by radiation exposure due to the nuclear accident.
In contrast, the present results suggest that CT examination in young people aged ≤ 20 years can induce an increase in lymphocytes with Tr formation in PB. Previous studies have reported that CT examinations in children increased the risk of cancer development (especially brain tumors)32,33,34, suggesting the possibility that DNA or chromosome damage due to radiation exposure by CT examination might be responsible for inducing chromosomal abnormalities or genetic mutations. However, Pearce MS et al.’s report did not state why those children needed to undergo CT examinations32. On the other hand, when children with cancer-predisposing factors (PFs) such as congenital genetic abnormalities and immunodeficiency were excluded, there was no relationship between CT examination and risk of developing cancer34. This might suggest, conversely, that children with PFs would be at risk of cancer development by CT examinations. A recent study has reported that radiation dose from head and neck CT examinations before the age of 22 is associated with the subsequent development of brain tumors35. The study had a 5-year observation period after the CT examination to rule out latent cancer at the time of the CT scan, and it is of interest that the excess relative risk (ERR) of brain tumor was highest in 5 to > 10 years and lowest in \(\ge \) 15 years since the exposure. Therefore, it is important to minimize medical exposures from such as CT examination, especially in young people.
In conclusion, the analysis of Tr aberration frequency using PB lymphocytes, an indicator of radiation exposure, supports the claim that there was no evidence of additional exposure without CT examinations in pediatric thyroid cancer patients compared with the control. Furthermore, it should be noted that medical exposure from CT scans in children and adolescents can affect chromosomes or genes.
Patients and methods
Ethics statement
The use of samples and the medical records in this study was approved by the Ethics Committee of the Fukushima Medical University School of Medicine (approval No. 2654). Written informed consent was obtained from all participants for analysis of their PB samples, and the protocols were carried out in accordance with approved guidelines of the Council for International Organizations of Medical Science36.
Subjects
Residents under the age of 18 in FP at the time of the GEJE undergo the TUE (primary examination). If nodules are found, a more detailed TUE (confirmatory examination) is performed, and if necessary, fine needle aspiration cytology (FNAC) according to the guidelines for thyroid diseases7,37,38. If diagnosed with cancer, the patient undergoes surgical treatment of the tumor according to the guidelines for thyroid diseases5,7. Initially, 40 patients with thyroid cancer were enrolled, but one was excluded because of a history of radiotherapy and chemotherapy for a brain tumor. Another one patient was excluded because the patient was found outside of FP and was unrelated to the TUE program in FP. As controls, we enrolled 32 healthy students over 20 years of age from Fukushima Medical University, but one patient with a history of CT examination was excluded because of a history of surgery for a cervical tumor in childhood.
Three groups were included in the analyses: the thyroid cancer group (n = 38; 15 males, 23 females; age range 12–26 years; median age, 18 years), the thyroid-related disease (non-thyroid cancer) group (n = 30; 6 males, 24 females; age range 15–28 years; median age, 21 years), and the control group (n = 31; 20 males, 11 females; age range 20–23 years; median age, 22 years). The number of CT examinations and examination sites prior to sample collection are shown for patients with thyroid cancer, patients with thyroid-related diseases (non-thyroid cancer), and individuals of the control group in Tables 1, 2, and 3, respectively. Age information is not included in those tables to protect individual information.
Separation of lymphocytes from PBs and cell culture conditions
Mononuclear blood cells were isolated from heparinized PBs using BD Vacutainer CPT tubes (BD Biosciences, San Jose, CA, USA) according to the manufacturer’s instructions. Cells were suspended in RPMI 1640 medium (Nacalai Tesque, Kyoto, Japan) containing 20% fetal bovine serum (Equitech Bio, Keilor East, Australia), 2% phytohaemagglutinin-HA15 (Remel, Lenexa, KS, USA), and 60 μg/mL of kanamycin solution (Life Technologies, Carlsbad, CA, USA) in a 15-mL Falcon tube. Lymphocytes were cultured in a 5% humidified CO2 incubator at 37 °C for 48 h. First-division metaphase cells were obtained by treating the culture with colcemid (final concentration, 0.05 μg/mL; Life Technologies) for 48 h. For samples younger than 18 years, colcemid was added for the last 24 h to prevent overcontraction.
Cell harvesting
After 48 h of culture, cells were harvested, treated with 0.075 M KCL, and fixed with methanol/acetic acid (3:1) according to the standard cytogenetic procedure15,39. Finally, the cell pellets were suspended in 1–2 mL of fixative, depending on the size of the pellets. One drop (around 20 μL) of the suspension was dispensed onto a slide and spread on a water bath.
Chromosome painting
Each slide was first dried at 65 °C for at least 1 h for hardening. Next, 6–7 μL of a Customized XCP-Mix probe (Mix-#1R-#2G-#4RG; MetaSystems, Altlussheim, Germany) solution was applied per 22 × 22-mm area, and the slide was covered with a glass coverslip and sealed with paper bond. Subsequent operations were carried out according to the manufacturer’s instructions. Nuclear DNA was denatured by incubating the slides on a hot plate at 75 °C for 2 min followed by incubation overnight at 37 °C in a humidified chamber to allow for hybridization. The glass coverslips were removed and the slides were washed in 0.4 × SSC at 72 °C for 2 min. After draining, the slides were then washed in 2 × SSC/0.05% Tween-20 at room temperature (RT) for 30 s. Subsequently, the slides were briefly rinsed in distilled water to avoid crystal formation and then air dried at RT. Finally, nuclei were counterstained with Vectashield Mounting Medium containing DAPI (Vector, Burlingame, USA), and the slides were covered with a glass coverslip and sealed with nail polish.
Image capturing and scoring of chromosomal aberrations (chromosome 1, 2, and 4 painting)
Soon after completion of the chromosome preparations, FISH images were captured in AutoCapt mode using two sets of AXIO Imager Z2 microscopes (Carl Zeiss AG, Oberkochen, Germany) equipped with CCD cameras and Metafer 4 software (MetaSystems GmbH, Altlussheim, Germany). Metaphase cells were selected for scoring in manual mode. Chromosome analysis was performed according to the International Atomic Energy Agency (IAEA) manual (IAEA 2001)39 by a trained, experienced observer blinded to information of the subjects’ backgrounds.
In our previous study, we analyzed Dic formation using Giemsa staining and centromere-FISH, and analyzed 2000 metaphases per patient17,18,19. Accordingly, to match the number of cells analyzed between the Dic and Tr analyses, we analyzed approximately 5000 cells, which was equivalent to whole-genome analysis of almost 2000 cells (Tables 1, 2, and 3, respectively.).
Only metaphase figures with about 44–46 chromosomes were selected for chromosomal analysis. Some clonal chromosome aberrations were suspected, but we did not correct the number of Tr accordingly. Thus, cells with three chromosome (1, 2, and 4) pairs colored in three different paintings were selected for analysis. Metaphase cells exhibiting tetraploidy were omitted from the analysis. When no translocated chromosome partner was found, it was counted as one-way (non-reciprocal); when the partner was found, it was counted as two-way (reciprocal). And in both cases, it was counted as one translocated chromosome. In the case of complex chromosomal abnormalities, the translocation number was determined based on the number of color junctions (NCJ)40. For example, an NCJ of 1 or 2 indicates one translocation, an NCJ of 3 or 4 indicates two translocations, an NCJ of 5 or 6 indicates three translocations, and so on.
For scoring, the formula used to calculate the frequency of translocations across the whole genome (FG) was based on the following formula, using three colors (chromosome 1, red; chromosome 2, green; chromosome 4, yellow) for the detected translocations:
FG: the full genome aberration frequency, Fp: the translocation frequency detected by FISH, fp: the fraction of genome hybridized, taking into account the sex of the subject (female: fp = 0.2234, male: fp = 0.2271).
The proportion of the genome occupied by chromosomes 1, 2, and 4 is about 23%. Therefore, FG is determined by the following formula:
To unify the cell numbers of the analysis, we determined FG as per the 2000-cell equivalents, which were obtained according to the above formulas for females and males, respectively. In addition, age-adjusted Tr frequency was determined based on the method of Sigurdson et al.41.
Statistical analysis
First, differences in age-adjusted Tr aberration frequency between those with and without a history of CT examination and between men and women were analyzed by Student's t-test. Differences in age-adjusted Tr aberration frequency among patients with thyroid cancer, thyroid-related disease (non-thyroid cancer), and controls were then tested using ANOVA. If the test by ANOVA was significant, differences between groups were compared by Tukey's test. Because a history of CT examination affected the age-adjusted Tr frequency, we made the same comparisons only among those with a history of CT scan. In addition, differences in age-adjusted Tr aberration frequency among patients with thyroid cancer, thyroid-related disease (non-thyroid cancer), and controls were compared by ANCOVA after adjusting for sex and history of CT examination. SAS version 9.4 (SAS Institute, Cary, NC, USA) was employed for all statistical analyses, with two-tailed probability values for the statistical tests. P values less than 0.05 were considered statistically significant.
Data availability
The datasets generated and/or analyzed during the current study are not publicly available due [Even in Fukushima Prefecture, the number of thyroid cancer patients is limited, and there is a risk that individuals could be identified, which could lead to harmful rumors, so the information cannot be disclosed. In fact, some patients have legal battles with the Fukushima nuclear power plant company] but are available from the corresponding author on reasonable request.
References
Kazakov, V. S., Demidchik, E. P. & Astakhova, L. N. Thyroid cancer after chernobyl. Nature 359, 21 (1992).
Cardis, E. et al. Cancer consequences of the Chernobyl accident: 20 years. J. Radiol. Prot. 26, 127–140 (2006).
Saenko, V. et al. The Chernobyl accident and its consequences. Clin. Oncol. (R Coll Radiol). 23, 234–243 (2011).
United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCEAR). Volume II: Effects of ionizing radiation. United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCEAR) Reports. 47–66 (2008).
Shimura H, et al. A comprehensive review of the progress and evaluation of the thyroid ultrasound examination program, the Fukushima Health Management Survey. J. Epidemiol. 32(Suppl XII), S23–S35 (2022).
National Cancer Center, Epidemiology and Prevention Division. Cancer prediction (2015–2039). https://ganjoho.jp/data/reg_stat/statistics/dl/cancer_prediction (2015–2039).xlsx. Accessed March 9, 2023 (in Japanese).
Suzuki, S. Childhood and adolescent thyroid cancer in Fukushima after the Fukushima Daiichi nuclear power plant accident: 5 years. Clin. Oncol. (R Coll Radiol). 28, 263–271 (2016).
Ohira, T., et al. Comparison of childhood thyroid cancer prevalence among 3 areas based on external radiation dose after the Fukushima Daiichi nuclear power plant accident: The Fukushima health management survey. Medicine (Baltimore). 95, e4472 (2016).
Ohira, T. et al. Associations between childhood thyroid cancer and external radiation dose after the Fukushima Daiichi nuclear power plant accident. Epidemiology 29(4), e32–e34 (2018).
Ohira, T. et al. External radiation dose, obesity, and risk of childhood thyroid cancer after the Fukushima Daiichi nuclear power plant accident: The Fukushima health management survey. Epidemiology 30, 853–860 (2019).
Takahashi H, et al. Nested matched case control study for the Japan Fukushima Health Management Survey's first full-scale (second-round) thyroid examination. Medicine (Baltimore). 99, e20440 (2020).
Midorikawa, S. et al. Comparative analysis of the growth pattern of thyroid cancer in young patients screened by ultrasonography in Japan after a nuclear accident: The Fukushima health management survey. JAMA Otolaryngol. Head Neck Surg. 144, 57–63 (2018).
Ohtsuru, A. et al. Incidence of thyroid cancer among children and young adults in Fukushima, Japan, screened with 2 rounds of ultrasonography within 5 years of the 2011 Fukushima Daiichi nuclear power station accident. JAMA Otolaryngol. Head Neck Surg. 145, 4–11 (2019).
19th Thyroid Examination Evaluation Subcommittee. Document 3–1. 1 August at Fukushima City (2022) [in Japanese]
International Atomic Energy Agency. Cytogenetic dosimetry: Applications in Preparedness for and Response to Radiation Emergencies, Emergency Preparedness and Response, IAEA, Vienna (2011).
Abe, Y. et al. Dose-response curves for analyzing of dicentric chromosomes and chromosome translocation following doses of 1000 mGy or less based on irradiated peripheral blood samples from 5 healthy individuals. J. Rad. Res. 59, 35–42 (2018) (Correction to J Rad Res. 64: 480–484, 2023).
Abe, Y. et al. Increase in dicentric chromosome formation after a single CT scan in adults. Sci. Rep. 5, 13882 (2015).
Abe, Y. et al. Investigation of the cumulative number of chromosome aberrations induced by three consecutive CT examinations in eight patients. J. Rad. Res. 60, 729–739 (2019).
Abe, Y. et al. Analysis of chromosome translocation frequency after a single CT scan in adult. J. Rad. Res. 57, 220–226 (2016).
Yasumura S, et al. Fukushima health management survey group. Study protocol for the Fukushima health management survey. J. Epidemiol. 22, 375–383 (2012).
Kanda, R. & Hayata, I. Comparison of the yields of translocations and dicentrics measured using conventional Giemsa staining and chromosome painting. Int. J. Radiat. Biol. 69, 701–705 (1996).
Zhang, W. & Hayata, I. Preferential reduction of dicentrics in reciprocal exchanges due to the combination of the size of broken chromosome segments by radiation. J. Hum. Genet. 48, 531–534 (2003).
Ishikawa, T. et al. The latest update on individual external doses in an early stage after the Fukushima nuclear accident. Radiat. Prot. Dosimetry. 187, 402–406 (2019).
Ishikawa T, et al. External doses available for epidemiological studies related to the Fukushima health management survey: First 4-month individual doses and municipality-average doses for the first year. J. Epidemiol. 32 (Suppl_XII), S11–S22 (2022).
Alexandrov, L. B. et al. Signatures of mutational processes in human cancer. Nature 500, 415–421 (2013).
Mitsutake, N. et al. BRAF(V600E) mutation is highly prevalent in thyroid carcinomas in the young population in Fukushima: A different oncogenic profile from Chernobyl. Sci. Rep. 5, 16976 (2015).
Iyama, K. et al. Identification of three novel fusion oncogenes, SQSTM1/NTRK3, AFAP1L2/RET, and PPFIBP2/RET, in thyroid cancers of young patients in Fukushima. Thyroid 27, 811–818 (2017).
Takahashi F, et al. WAZA-ARI: computational dosimetry system for X-ray CT examinations. I. Radiation transport calculation for organ and tissue doses evaluation using JM phantom. Radiat. Prot. Dosimetry. 146: 241–243 (2011).
Ban, N. et al. WAZA-ARI: computational dosimetry system for X-ray CT examinations II: Development of web-based system. Radiat. Prot. Dosimetry. 146, 244–247 (2011).
Ban, N. et al. Development of a web-based CT dose calculator: WAZA-ARI. Radiat. Prot. Dosimetry. 147, 333–337 (2011).
Ishikawa, T. et al. Representativeness of individual external doses estimated for one quarter of residents in the Fukushima Prefecture after the nuclear disaster: The Fukushima Health Management Survey. J. Radiol. Prot. 37, 584–605 (2017).
Pearce, M. S. et al. Radiation exposure from CT scans in childhood and subsequent risk of leukaemia and brain tumours: A retrospective cohort study. Lancet 380, 499–505 (2012).
Mathews, J. D. et al. Cancer risk in 680,000 people exposed to computed tomography scans in childhood or adolescence: data linkage study of 11 million Australians. BMJ 346, f2360 (2013).
Journy, N. et al. Are the studies on cancer risk from CT scans biased by indication? Elements of answer from a large-scale cohort study in France. Br. J. Cancer. 112, 185–193 (2015).
Hauptmann, M. et al. Brain cancer after radiation exposure from CT examinations of children and young adults: Results from the EPI-CT cohort study. Lancet Oncol. 24, 45–53 (2023).
International guidelines for ethical review of epidemiological studies. Law. Med Health Care. 19, 247–258 (1991).
Shimura, H. et al. Distinct diagnostic criteria for ultrasonographic examination of papillary thyroid carcinoma: A multicenter study. Thyroid 15, 251–258 (2005).
Kitaoka, M. et al. Ultrasound diagnostic criteria for thyroid nodule. Jpn J. Med. Ultrasonics. 36, 669–670 (2011).
International Atomic Energy Agency. Cytogenetic Analysis for Radiation Dose Assessment: A Manual. Technical Reports Series No. 405, IAEA, Vienna, (2001).
Nakano, M. et al. Detection of stable chromosome aberrations by FISH in A-bomb survivors: comparison with previous solid Giemsa staining data on the same 230 individuals. Int. J. Radiat. Biol. 77, 971–977 (2001).
Sigurdson, A. J. et al. International study of factors affecting human chromosome translocations. Mutat. Res. 652, 112–121 (2008).
Acknowledgements
This work was supported in part by a Grant for Strategic Research Promotion of Fukushima Medical University School of Medicine, and Network-type Joint Usage/Research Center for Radiation Disaster Medical Science.
Author information
Authors and Affiliations
Contributions
Conceptualization, A.S.; investigation, A.S., Y.M., I.M., S.S., M.S., M.H., T.I., and S.S.; validation, A.S. and N.T.; methodology, N.T., T.O., Y.A., and M.ST.; writing—original draft and editing, A.S. funding acquisition, A.S., N.T., T.O., M.ST., Y.A., S.S., M.S., M.H., T.I., and S.S.; project administration, A.S.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Sakai, A., Tsuyama, N., Ohira, T. et al. No increase in translocated chromosomal aberrations, an indicator of ionizing radiation exposure, in childhood thyroid cancer in Fukushima Prefecture. Sci Rep 13, 14254 (2023). https://doi.org/10.1038/s41598-023-41501-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-41501-x
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
