
Abstract
Rectal mucinous adenocarcinoma (RMAC) is a rare and aggressive form of rectal cancer. The effectiveness of neoadjuvant radiotherapy (NRT) for RMAC has not been well studied, and the survival benefit remains controversial. The purpose of this work was to determine the prognostic role of NRT in patients with RMAC by propensity-score matching (PSM). A retrospective cohort study using the Surveillance, Epidemiology, and End Results from 2004 to 2015 was performed. In the multivariate analysis before PSM, NRT provided better OS (HR 0.61, 95% CI 0.52–0.71, p < 0.001) and CSS (HR 0.68, 95% CI 0.56–0.82, p < 0.001). Multivariate analysis after PSM (n = 844) confirmed that patients receiving NRT survived longer than those without NRT (OS: HR 0.60, 95% CI 0.50–0.78, p < 0.001 and CSS: HR 0.68, 95% CI 0.54–0.84, p < 0.001). Subgroup analysis indicated that NRT had significantly improved OS and CSS in stage II RMAC and OS in stage III RMAC after adjusting for various confounding factors.
Similar content being viewed by others


Introduction
The most common histologic subtype of rectal cancer is adenocarcinoma, of which mucinous adenocarcinoma is a distinct subtype characterized by abundant extracellular mucin that comprises at least 50% of the tumor tissue1,2. This subtype accounts for 5–15% of primary rectal cancer3,4. Compared to non-mucinous counterparts, rectal mucinous adenocarcinoma (RMAC) represents distinct clinicopathological characteristics and molecular features, which may lead to more advanced stage of disease, more rapid tumor progression, and worse therapeutic response5,6,7.
Accumulating studies have shown that neoadjuvant radiotherapy (NRT) has significantly reduced local recurrence and improved survival for patients with locally advanced rectal cancer (LARC, stage II and III) 8,9,10,11. Consequently, the National Comprehensive Cancer Network (NCCN) guidelines have recommended preoperative radiotherapy as standard neoadjuvant strategy for LARC 12,13. However, the tumor responses and prognostic outcomes to radiotherapy are variable, which may be related to the different histological types of rectal cancer14,15. The survival impact of NRT on patients with RMAC has not been clarified yet. Therefore, this issue urgently needs more research, so that clinicians can select more appropriate treatments for these patients.
Materials and methods
Patient selection
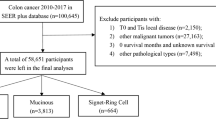
In order to determine prognostic factors for rare diseases such as RMAC, large population-based studies are the ideal method. The Surveillance, Epidemiology, and End Results (SEER) database consists of 18 cancer registries that covers approximately 28% of the U.S. population and contains basic demographics and clinical characteristics. In this study, we extracted data from the SEER database of individuals diagnosed between 2004 and 2015 to explore in more detail the correlation between NRT and the long-term survival benefit of RMAC patients. The inclusion criteria were as follows: (1) patients diagnosed from 2004 to 2015; (2) histologically confirmed RMAC; (3) patients at stage II or III (pathological stage); (4) patients received preoperative radiotherapy followed by radical surgery or radical surgery alone; (5) age at diagnosis over 18 years. Based on whether patients received radiotherapy or not before radical surgery, the entire cohort was further divided into neoadjuvant radiotherapy (NRT) and non-neoadjuvant radiotherapy (non-NRT) groups. Finally, 1514 cases were included in our study (Fig. 1).

Flow diagram of study cohort selection.
Variables definition and stratification
The demographic, clinicopathologic characteristics and treatment information of patients with RMAC: age at diagnosis (≤ 60 years, > 60 years), sex (male or female), race recorded by SEER (white, black, and other), pathological grading (well differentiated, moderately differentiated, poorly differentiated, undifferentiated, and unknown), carcinoembryonic antigen (CEA) level (normal, elevated, and unknown), tumor size (≤ 5 cm, > 5 cm, and unknown), TNM stage (pathological stage) (II, III), tumor stage (T1, T2, T3, and T4), node stage (N0, N1, and N2), number of dissected lymph nodes (LND) (< 12 or ≥ 12) ,chemotherapy (none, yes) and survival (months).
Outcome definition
The primary endpoints were overall survival (OS) and cancer-specific survival (CSS). OS was defined as the time from diagnosis to death from any cause. CSS was defined as the time from the date of diagnosis to the date of death from rectal cancer or the latest follow-up.
Propensity score matching
Propensity score matching (PSM) is a reliable statistical method for reducing selection bias in observational studies and achieving the balance of covariates across the study groups16. Baseline characteristics between the NRT group and the non-NRT group were matched using nearest neighbor matching (1:1) with a caliper of 0.2.
Statistical analyses
The chi-square test was used to compare the patients’ baseline characteristics between the groups. Cox proportional hazard models were used to determine the prognostic factors for OS and CSS. Kaplan–Meier survival analysis and log-rank tests were performed to compare the survival among different groups. All tests were two-sided, and P-value < 0.05 was applied to indicate statistical significance. All statistical analyses and graphics were performed using Statistical Product and Service Solutions (SPSS) software (ver.26.0), R software (ver.3.6.3) and GraphPad Prism software (ver.8.0).
Ethics approval
This study was partly based on the publicly available SEER database and we have got the permission to access them on purpose of research only (Reference number: 11806-Nov2021). It did not include interaction with humans or use personal identifying information. The informed consent was not required for this research.
Results
Patient characteristics
In this study, 1514 patients with RMAC fulfilled the eligibility criteria, including 1035 (68.4%) patients in the NRT group and 479 (31.6%) in the non-NRT group. The median follow-up time was 57 months (0–179 months). Patient demographics and baseline characteristics are listed in Table 1. In the cohorts of NRT and non-NRT, most of the patients were male (64.3% and 58.5% respectively) and white (81.4% and 85.4% respectively). For patients aged ≤ 60 years, they were more likely to receive NRT compared with patients aged > 60 years (83.1 vs. 58.7%). The proportion of patients with stage III RMAC receiving NRT is higher than those with stage II RMAC (73.2% vs. 61.1%). To balance the distribution of baseline characteristics, PSM was used. After matching, there was no significant differences between case and control groups except for chemotherapy (Table 1).
Survival analyses in the whole SEER cohort
OS and CSS for the entire cohort were 57.9% and 65.2% at 5 years, respectively, and 41.7% and 55.0% at 10 years, respectively. All baseline characteristics were selected for univariable and multivariate analysis to assess the effect on OS and CSS. Univariate analysis showed that older age (≥ 60 years), lager tumor size (> 5 cm), higher T stage (T4), N stage (N2), and number of LND < 12 were associated with worse OS and CSS, while NRT and chemotherapy were strongly associated with better survival (Table 2). In multivariate analysis, NRT was an independent prognostic factor for OS and CSS (OS: HR 0.61, 95% CI 0.52–0.71, p < 0.001; CSS: HR 0.68, 95% CI 0.56–0.82, p < 0.001) (Table 2). Furthermore, Kaplan–Meier curve analysis revealed that patients who received NRT had better OS (P < 0.001) and CSS (P = 0.001) than those who did not (Fig. 2A, B).

Kaplan–Meier curve of locally advanced RMAC. (A) OS curve of the non-NRT group versus NRT group before PSM; (B) CSS curve of the non-NRT group versus NRT group before PSM; (C) OS curve of the non-NRT group versus NRT group after PSM; (D) CSS curve of the non-NRT group versus NRT group after PSM.
Survival analysis in propensity score-matched cohort
In the matched cohort, univariate analysis showed similar prognostic factors for OS and CSS to the unmatched cohort: age, tumor size, T stage, N stage, number of LND, NRT and chemotherapy (Table 3). The multivariate analysis showed that NRT was an independent prognostic factor for OS and CSS; OS (HR 0.60, 95% CI 0.50–0.78, p < 0.001) and CSS (HR 0.68, 95% CI 0.54–0.84, p < 0.001) of NRT-receiving patients were better than their non-NRT-receiving counterparts (Table 3). Other clinicopathological parameters, including age, larger tumor size, higher N stage, Number of LND and chemotherapy were also independent indicators for OS and CSS. In fact, NRT-receiving patients had significantly improved OS (5-year OS: 61.8 vs. 46.2%; 10-year OS: 40.4 vs. 29.7%, p < 0.001) and CSS (5-year CSS: 68.9 vs. 58.6%; 10-year CSS: 57.1 vs. 47.9%, p = 0.007) than those without NRT (Fig. 2C,D).
Subgroup analysis according to TNM stage
To further identify patients who may benefit from NRT, subgroup analyses according to TNM stage were performed. Of note, no significant difference was found between the NRT and non-NRT groups in terms of baseline characteristics except for chemotherapy after PSM (all p > 0.05, Table 4). Per Kaplan–Meier survival analysis, NRT significantly improved OS and CSS of stage II RMAC compared to their non-NRT-receiving counterparts (OS: p < 0.001, CSS: p = 0.010). In addition, NRT improved OS, but not CSS, in stage III patients (OS: p = 0.014, CSS: p = 0.203) (Fig. 3).

Kaplan–Meier curve of subgroups stratified by TNM stage. (A) Comparisons of OS in stage II patients with RMAC after PSM; (B) Comparisons of CSS in stage II patients with RMAC after PSM; (C) Comparisons of OS in stage III patients with RMAC after PSM; (D) Comparisons of CSS in stage III patients with RMAC after PSM.
Discussion
During the first decade of the twenty-first century, preoperative radiotherapy became the standard neoadjuvant strategy for LARC due to its advantage on increasing sphincter preservation rate and reducing local recurrence17,18,19. Growing evidence has demonstrated that mucinous adenocarcinoma is a distinct histologic subtype with different natural history, biological behavior, pathologic and molecular features, which may make them respond differently to treatment compared to their non-mucinous counterparts20,21,22,23,24. Moreover, RMAC has a higher ratio of lymph node infiltration and peritoneal implant25,26. However, given the rarity of RMAC, there are few studies about treatment for patients with RMAC and, to date, RMAC is treated with the principles that are developed for more common non-mucinous rectal cancer. In the era of precise medicine and personalized treatment, it is extremely important to understand the prognostic value of NRT for RMAC.
To our knowledge, this is the first population-based study using PSM analysis to assess the role of NRT in locally advanced RMAC. Most studies showed that the histology of mucinous adenocarcinoma in rectal cancer served as a biomarker for poor prognosis after preoperative chemoradiotherapy. Sengul et al. demonstrated that patients with RMAC had obvious tumor regression and a decreased transrectal ultrasound score after receiving preoperative irradiation and 5-FU infusion, although not to the same degree as in non-mucinous adenocarcinoma15. Simha et al. came to a similar conclusion where RMAC patients were treated with preoperative radiation and 5-FU plus leucovorin chemotherapy27. In addition, Hugen et al. showed that short-term preoperative radiotherapy could narrow the survival gap between mucinous and non-mucinous rectal adenocarcinoma and led to a decrease in local recurrence of RMAC28. However, none of these studies had evaluated the efficacy of NRT on long-term outcomes in patients with RMAC or performed subgroup analyses to further investigate the relationship between NRT and survival outcomes. The results of the present study showed that NRT was independently associated with better OS and CSS, both before and after PSM for the entire cohort. Furthermore, the subgroup analysis revealed that NRT had significantly improved OS and CSS in stage II RMAC and OS in stage III RMAC. The reason why NRT did not result in better CSS in stage III RMAC might be attributed to the inadequacy of cases; another possible explanation was that NRT was less likely to influence the CSS of this subgroup, who tended to be more advanced at baseline and had worse prognosis.
Our study used a population-based cancer registry; unlike single-institution studies, which inevitably have a referral bias, the SEER database provides a more realistic clinical practice environment with information from all levels of healthcare institutions. Although there are many strengths of this study including the large sample size, PSM test and subgroup analysis, we acknowledge some limitations to our study. First, there were no information regarding preoperative radiotherapy in the SEER database, including clinical target volume and radiation regimen, which may cause confusion. Second, data on chemotherapy, such as regimen and courses, were also unavailable, so that further case–control studies failed to be performed. Finally, the SEER database did not include local recurrence and disease-free survival, which made the local control benefit of radiation therapy unanalyzable. However, the association of NRT with better OS and CSS in stage II RMAC and better OS in stage III RMAC was sufficient to support the advantage of preoperative radiotherapy.
Conclusions
In conclusion, our results have shown that locally advanced RMAC can gain survival benefit from NRT, which could provide better OS and CSS in stage II and better OS in stage III RMAC. Nonetheless, our results should be interpreted with caution, and further prospective clinical trials are needed, given the observational bias caused by their retrospective nature.
Data availability
The data that support the findings of this study are available from Surveillance, Epidemiology, and End Results (SEER) database (https://seer.cancer.gov/) but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the corresponding author upon reasonable request and with permission of SEER database.
References
Hanski, C. Is mucinous carcinoma of the colorectum a distinct genetic entity?. Br. J. Cancer 72(6), 1350–1356. https://doi.org/10.1038/bjc.1995.514 (1995).
Compton, C. C. Colorectal carcinoma: diagnostic, prognostic, and molecular features. Modern Pathol. Off. J. United States Can. Acad. Pathol. Inc, 16(4): 376–88 https://doi.org/10.1097/01.Mp.0000062859.46942.93 (2003)
Rullier, A. et al. Impact of colloid response on survival after preoperative radiotherapy in locally advanced rectal carcinoma. Am. J. Surg. Pathol. 29(5), 602–606. https://doi.org/10.1097/01.pas.0000153120.80385.29 (2005).
Compton, C. C. et al. Prognostic factors in colorectal cancer. College of American pathologists consensus statement 1999. Arch. Pathol. Lab. Med. 124(7), 979–994. https://doi.org/10.5858/2000-124-0979-pficc (2000).
Yamaguchi, T. et al. Clinicopathological characteristics and prognostic factors of advanced colorectal mucinous adenocarcinoma. Histopathology 61(2), 162–169. https://doi.org/10.1111/j.1365-2559.2012.04235.x (2012).
Mekenkamp, L. J. et al. Mucinous adenocarcinomas: poor prognosis in metastatic colorectal cancer. Eur. J. Cancer (Oxford, England 1990) 48(4), 501–509. https://doi.org/10.1016/j.ejca.2011.12.004 (2012).
Leopoldo, S. et al. Two subtypes of mucinous adenocarcinoma of the colorectum: Clinicopathological and genetic features. Ann. Surg. Oncol. 15(5), 1429–1439. https://doi.org/10.1245/s10434-007-9757-1 (2008).
van Gijn, W. et al. Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer: 12-year follow-up of the multicentre, randomised controlled tme trial. Lancet Oncol. 12(6), 575–582. https://doi.org/10.1016/s1470-2045(11)70097-3 (2011).
Cammà, C. et al. Preoperative radiotherapy for resectable rectal cancer: A meta-analysis. JAMA 284(8), 1008–1015. https://doi.org/10.1001/jama.284.8.1008 (2000).
Glimelius, B. Neo-adjuvant radiotherapy in rectal cancer. World J. Gastroenterol. 19(46), 8489–8501. https://doi.org/10.3748/wjg.v19.i46.8489 (2013).
Allal, A. S. et al. Sphincter-sparing surgery after preoperative radiotherapy for low rectal cancers: Feasibility, oncologic results and quality of life outcomes. Br. J. Cancer 82(6), 1131–1137. https://doi.org/10.1054/bjoc.1999.1052 (2000).
Benson, A. B. et al. Rectal cancer, version 2.2018, Nccn clinical practice guidelines in oncology. J. Natl. Compr. Cancer Netw. JNCCN 16(7), 874–901. https://doi.org/10.6004/jnccn.2018.0061 (2018).
Glynne-Jones, R. et al. Rectal cancer: Esmo clinical practice guidelines for diagnosis, treatment and follow-Up. Annals Oncol. Off. J. Eur. Soc. Med. Oncol. 28(Suppl_4), iv22–iv40. https://doi.org/10.1093/annonc/mdx224 (2017).
Janjan, N. A. et al. Prospective trial of preoperative concomitant boost radiotherapy with continuous infusion 5-fluorouracil for locally advanced rectal cancer. Int. J. Radiat. Oncol. Biol. Phys. 47(3), 713–718. https://doi.org/10.1016/s0360-3016(00)00418-1 (2000).
Sengul, N. et al. Effects of radiotherapy on different histopathological types of rectal carcinoma. Colorectal Dis. Off. J. Assoc. Coloproctol. G. B. Irel. 8(4), 283–288. https://doi.org/10.1111/j.1463-1318.2005.00934.x (2006).
Little, R. J. & Rubin, D. B. Causal effects in clinical and epidemiological studies via potential outcomes: Concepts and analytical approaches. Annu. Rev. Public Health 21, 121–145. https://doi.org/10.1146/annurev.publhealth.21.1.121 (2000).
Kapiteijn, E. et al. Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer. N. Engl. J. Med. 345(9), 638–646. https://doi.org/10.1056/NEJMoa010580 (2001).
Sauer, R. et al. Preoperative versus postoperative chemoradiotherapy for locally advanced rectal cancer: Results of the German Cao/Aro/Aio-94 randomized phase iii trial after a median follow-up of 11 years. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 30(16), 1926–1933. https://doi.org/10.1200/jco.2011.40.1836 (2012).
Roh, M. S. et al. Preoperative multimodality therapy improves disease-free survival in patients with carcinoma of the rectum: nsabp R-03. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 27(31), 5124–5130. https://doi.org/10.1200/jco.2009.22.0467 (2009).
Madbouly, K. M., Mashhour, A. N. & Omar, W. Is it safe to omit neoadjuvant chemo-radiation in mucinous rectal carcinoma?. Int. J. Surg. (London, England) 23(Pt A), 120–127. https://doi.org/10.1016/j.ijsu.2015.08.081 (2015).
Zhang, H., Evertsson, S. & Sun, X. Clinicopathological and genetic characteristics of mucinous carcinomas in the colorectum. Int. J. Oncol. 14(6), 1057–1061. https://doi.org/10.3892/ijo.14.6.1057 (1999).
Catalano, V. et al. Prognosis of mucinous histology for patients with radically resected stage Ii and Iii colon cancer. Annals Oncol. Off. J. Eur. Soc. Med. Oncol. 23(1), 135–141. https://doi.org/10.1093/annonc/mdr062 (2012).
Garcia-Aguilar, J. et al. Identification of a biomarker profile associated with resistance to neoadjuvant chemoradiation therapy in rectal cancer. Annals Surg. 254(3), 486–492. https://doi.org/10.1097/SLA.0b013e31822b8cfa (2011).
Park, E. T. et al. Aberrant expression of sox2 upregulates muc5ac gastric foveolar mucin in mucinous cancers of the colorectum and related lesions. Int. J. Cancer 122(6), 1253–1260. https://doi.org/10.1002/ijc.23225 (2008).
Gruia, C., Foarfă, C., Streba, L., Mănescu, P. Synchronous carcinoma of the ascending colon and caecum. Romanian Journal of Morphology and Embryology = Revue roumaine de morphologie et embryologie (2011) 52(4):1369–75.
Nozoe, T., Anai, H., Nasu, S. & Sugimachi, K. Clinicopathological characteristics of mucinous carcinoma of the colon and rectum. J. Surg. Oncol. 75(2), 103–107. https://doi.org/10.1002/1096-9098(200010)75:2%3c103::aid-jso6%3e3.0.co;2-c (2000).
Simha, V., Kapoor, R., Gupta, R., Bahl, A. & Nada, R. Mucinous adenocarcinoma of the rectum: A poor candidate for neo-adjuvant chemoradiation?. J. Gastrointest. Oncol. 5(4), 276–279. https://doi.org/10.3978/j.issn.2078-6891.2014.020 (2014).
Hugen, N. et al. Modern treatment of rectal cancer closes the gap between common adenocarcinoma and mucinous carcinoma. Ann. Surg. Oncol. 22(8), 2669–2676. https://doi.org/10.1245/s10434-014-4339-5 (2015).
Acknowledgements
The authors acknowledge the efforts of the Surveillance, Epidemiology, and End Results (SEER) Program tumor registries in the creation of the SEER database.
Funding
This work was supported by the National Natural Science Foundation of China (81972869, 32270955); the Key R&D Program of Jiangsu Province (BE2022719); Social Development Science and Technology Project of Changzhou (CE20215030); the Science and Technology Planning Project of Changzhou (CJ20210158).
Author information
Authors and Affiliations
Contributions
C.C.: conceptualization, data curation, formal analysis, methodology, project administration, writing original draft. X.C.: data curation, formal analysis, and reviewing and editing the manuscript. J.J.: supervision and reviewing and editing the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Chen, C., Chen, X. & Jiang, J. Long-term effect of neoadjuvant radiotherapy in patients with locally advanced rectal mucinous adenocarcinoma: a population-based study of 1514 patients. Sci Rep 13, 11696 (2023). https://doi.org/10.1038/s41598-023-38846-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-38846-8
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
