
Abstract
Syphilis is a global public health concern. This study aimed to assess the global and regional burden of syphilis from 1990 to 2019. Disease burden was evaluated using disability-adjusted life-years (DALYs) and prevalence. Data were extracted from the 2019 global burden of disease Study, an open database available for download. Age-standardized rates (ASR) and estimated annual percentage changes (EAPC) were calculated to evaluate the syphilis burden over time. In 2019, the total number of prevalent cases of syphilis was 49.71 million worldwide. The ASR of prevalence was stable from 1990 to 2019 with an EAPC of 0.00 (95% CI − 0.10–0.11). The number of DALYs caused by syphilis was 7.36 million in 2019, reflecting a reduction of 16.38% compared with that in 1990 (8.80 million). The ASR of DALYs exhibited a decreasing trend from 1990 to 2019 (EAPC = − 1.01; 95% CI − 1.19 to − 0.84), with the highest rates observed in the younger age group (< 14 years old). In 2019, the highest ASR of DALYs was found in low sociodemographic index (SDI) regions (239.21/100,000), and the lowest in high SDI regions (3.14/100,000). Generally, the ASR of DALYs decreased as the SDI increased. The top three countries with the highest ASR of DALYs for syphilis were the Solomon Islands, Equatorial Guinea, and Liberia. While the global prevalence of syphilis remained persistently high from 1990 to 2019, there has been a recent decrease in the ASR of DALYs. Increased attention should be dedicated to younger populations and regions characterized by low SDIs.
Similar content being viewed by others

Introduction
Syphilis is a sexually transmitted infection (STIs) caused by Treponema pallidum that has imposed a significant global burden in the past few decades1. Syphilis not only affects the genitourinary system2 but also impairs other systems, including the neurological, cardiovascular, ocular, or liver systems3,4. Patients diagnosed with syphilis may experience discrimination, stigma, exclusion, and pressure from society and family5. During the 69th World Health Assembly in 2016, a target was set to reduce the global incidence of syphilis by 90% from 2018 to 20306. Nevertheless, there has been a recent indication of an increase in the global prevalence of syphilis. To achieve the target set by the 69th World Health Assembly, countries need to revise their policies regarding syphilis and especially focus on high-risk populations.
The burden and rate of syphilis show variations based on time, location, and population. There has been a discernable rise in the prevalence of syphilis in Europe and Australia7,8. Additionally, syphilis has extended its reach beyond urban areas and is spreading to rural or remote areas8. A report from South–East Asia revealed the emergence of a subsequent wave of syphilis in the past 15 years9. Most studies have focused on examining the burden of syphilis within specific regions and did not extend their investigation to encompass global changes7,8,9. A recent systematic review revealed that the frequency of maternal and congenital syphilis in indigenous people varies but tends to be higher compared to that in their non-indigenous counterparts. Data from China indicated a substantial increase in syphilis diagnoses over time, particularly among less developed cities and older women10. These groups had received comparatively less attention. In a study conducted in the United States, a similar finding was reported, revealing an increase in the burden of syphilis among older adults; notably, this population has always been overlooked or neglected11.
Previous studies have indicated that the prevention of mother-to-child transmission (MTCT) could be key to reducing the burden of syphilis. In 2008, an estimated 1.36 million pregnant women were reported to have active syphilis, resulting in serious complications, including pelvic inflammatory disease, premature birth, low birth weight, stillbirth, and neonatal infection12. Antenatal screening and treatment of syphilis have played a crucial role in safeguarding the well-being of both the mother and newborn, as well as promoting child health13. However, the association between syphilis, economic status, and age group is not well established. Identifying the groups most affected by the disease and formulating effective programs and policies that specifically target these populations are essential for syphilis control.
The global burden of disease study (GBD) is an open database providing a systematic scientific assessment of the prevalence and disability-adjusted life-years (DALYs) of 369 diseases worldwide14. Based on this database, studies have been conducted to assess the burden of HIV and acute viral hepatitis. These studies have consistently demonstrated that HIV and acute viral hepatitis remain significant contributors to the loss of healthy life15,16. A systematic analysis of the burden of syphilis is still lacking. In this study, we used the 2019 GBD data to analyze the temporal trends and burden of syphilis. The results of our study will enhance our knowledge of the burden of syphilis and will assist in the formulation of strategies for effective prevention and control of the disease.
Methods
Study data
Syphilis data from 1990 to 2019 were obtained from the Global Health Data Exchange query tool (http://ghdx.healthdata.org/gbd-results-tool). In the GBD 2019 study, all statistics are presented as values with 95% uncertainty intervals (UI) after 100,000 simulations. The following selection criteria were applied to select the data for analysis. First, the study period was set to 1990–2019. Second, the location name was set to include “Global”, “the 21 geographic locations”, “sociodemographic index (SDI) areas”, and “the 204 countries or territories”17. Third, the cause was set to “syphilis”. Fourth, “prevalence” and “DALYs” were chosen as the evaluation index of syphilis burden. Finally, age was segregated into four categories: up to 14, 15–49, 50–69, and 70 + years.
Definitions
Age-standardized rate (ASR)18
Age-standardized rate (ASR) was based on the GBD 2019 global age (standard population). The ASR in this study mainly included the ASR of prevalence and ASR of DALYs.
Disability-adjusted life-years (DALYs)
The global burden of syphilis was estimated in terms of disability-adjusted life years (DALYs) in the GBD 2019 study, which was defined as the sum of years of life lost and years lived with a disability18.
Sociodemographic index (SDI)
The sociodemographic index (SDI) is a summary indicator of economic and societal development and was constructed using education, average income, and overall fertility rate under the age of 2519. In the GBD 2019, countries and territories were grouped into five SDI quintiles: low, low-middle, middle, high-middle, and high.
Estimated annual percentage change (EAPC)
The estimated annual percentage change (EAPC) and 95% confidence intervals (CI) were calculated as the average annual percentage change in ASR from 1990 to 2019. If the EAPC and lower 95% CI limit were both positive, the ASR was considered to have an upward trend. Conversely, if the EAPC and the upper 95% CI limit were both negative, the ASR was considered to have a decreasing trend. Otherwise, ASR was regarded to be consistent over time.
Joinpoint regression analysis
Joinpoint regression analyses were performed using Joinpoint software version 5.0, which was obtained from the US National Cancer Institute (https://surveillance.cancer.gov/joinpoint/). This software was used to calculate the annual percent change (APC) and average annual percentage change (AAPC). The Joinpoint regression technique has the advantage of characterizing the trend of disease burden changes at many stages.
Statistical analysis
Data were downloaded from the GBD database and statistical analyses were performed using R software version 4.2.2 (https://www.R-project.org/). Subgroup analysis was performed according to sex, age, SDI, and the 21 geographic locations.
Results
Worldwide burden estimates of syphilis
Globally, the number of prevalent cases of syphilis was 30.91 million in 1990 and 49.71 million in 2019, with an increase of 60.83% from 1990 to 2019. (Table 1) The ASR of prevalence was stable from 1990 to 2019 (Fig. 1A), with an EAPC of 0.00 (95% CI − 0.10–0.11). The prevalence of ASR in 2019 was 766.41/100,000 for men and 473.81/100,000 for women (male/female = 1.62). The number of DALYs caused by syphilis was 7.36 million in 2019, a reduction of 16.38% compared to that in 1990 (8.80 million) (Table 2). The ASR of DALYs showed a decreasing trend from 1990 to 2019 (EAPC = − 1.01; 95% CI − 1.19 to − 0.84) (Fig. 1B). A similar downward trend was observed in both men and women. The highest ASR prevalence was observed among those aged 15–49 years (1113.54/100,000), followed by the 50–69 years age group (364.20/100,000), and was the lowest in the < 14 years age group (31.53/100,000) (Fig. 1C). The highest ASR of DALYs was found in the < 14 years age group, which increased with increasing age. A reduction in DALYs over time was observed in all age-stratified subgroups (Fig. 1D). Joinpoint analysis was applied to divide the temporal trends into four time periods and estimate the APC by sex. The results showed that the ASR of prevalence increased slightly (AAPC = 0.24) between 1990 and 2019. The three periods of prevalence from 1990 to 2001, 2001 to 2010, and 2015 to 2019 showed an upward trend (APC > 0), whereas the period from 2001 to 2004 showed a downward trend (APC < 0). The upward trend in men was more pronounced than that in women (Fig. 2A). Joinpoint regression analysis revealed that the ASR of DALYs showed a downward trend in all four time periods (APC < 0 and AAPC < 0), and this trend was similar between men and women (Fig. 2B).

Trend of ASR of syphilis from 1990 to 2019. (A) ASR of prevalence grouped by sex; (B) ASR of DALYs grouped by sex; (C) ASR of prevalence grouped by age, age 15–49 and 50–69 groups are depicted on the left axis, while other age groups are depicted on the right Y-axis; (D) ASR of DALYs grouped by age, age 15–49, 50–69, and ≥ 70 groups are depicted on the left axis, while age group < 14 years is depicted on the right Y-axis; (E) ASR of prevalence grouped by SDI levels, and low and low middle SDI groups are depicted on the left axis, while other SDI groups are depicted on the right Y-axis. (F) ASR of DALYs grouped by SDI levels, and low and low middle SDI groups are depicted on the left axis, while other SDI groups are depicted on the right Y-axis. DALYs disability-adjusted life years, ASR age-standardized rate, SDI sociodemographic index.

Results of Joinpoint regression analysis grouped by sex. (A) ASR of prevalence; (B) ASR of DALYs. APC annual percent change, AAPC average annual percent change.
Prevalence in different regions
The ASR of syphilis prevalence has been investigated in different regions worldwide and is reported to be negatively associated with the SDI level. In 2019, the highest ASR of prevalence was observed in the low SDI regions (1459.13/100,000) and lowest in the high SDI regions (246.75/100,000) (Fig. 1E). There was an increasing trend in the ASR of prevalence in high SDI regions (EAPC: 0.15, 95% CI 0.10–0.20) and high-middle SDI regions (EAPC: 0.12, 95% CI 0.01–0.23), whereas the incidence decreased in low SDI regions (EAPC: − 1.03, − 1.13 to − 0.93).
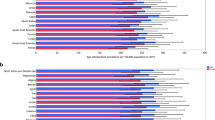
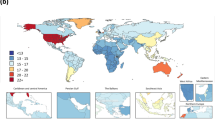
The highest observed ASR of prevalence in 2019 was in Central Sub-Saharan Africa, followed by Southern Sub-Saharan Africa and Eastern Sub-Saharan Africa (Fig. 3A). In addition, among the 204 countries or territories, the Central African Republic (4883.08/100,000), Equatorial Guinea (4429.62/100,000), and Angola (3892.36/100,000) exhibited the highest ASR of prevalence in 2019 (Supplementary Table 1, Fig. 4A). However, the ASR of prevalence decreased significantly over time among the three regions. The three countries and territories with the highest increase in ASR of prevalence were Greece, Mongolia, and Paraguay, with EAPCs of 3.59, 3.31, and 1.38, respectively.

ASR of syphilis in 21 geographical regions in 2019. (A) ASR of prevalence; (B) ASR of DALYs. DALYs disability‐adjusted life years, ASR age-standardized rate.

ASR of syphilis in 204 countries or territories in 2019. (A) ASR of prevalence; (B) ASR of DALYs. The world map chart was built using the R statistical software (version 4.2.2). Prevalence and DALYs of syphilis worldwide was mapped using the “sf” R package and “.shp file”. DALYs disability‐adjusted life years, ASR age-standardized rate.
DALYs in different regions
The highest ASR of DALYs occurred in low-SDI regions (239.21/100,000) and the lowest occurred in high-SDI regions (3.14/100,000). Generally, the ASR of DALYs decreased as the SDI increased. (Fig. 1F). We also found decreasing trends of DALYs in all SDI areas, particularly in low SDI areas (EAPC = − 2.10; 95% CI − 2.24 to − 1.95). In 2019, the highest observed ASR of DALYs was in Oceania, followed by Central Sub-Saharan Africa and Eastern Sub-Saharan Africa (Fig. 3B). The ASR of DALYs showed decreasing trends in most regions, particularly Eastern Europe (EAPC = − 8.12; 95% CI − 9.79 to − 6.45) and Southern Latin America (EAPC = − 3.85; 95% CI − 4.47 to − 3.22). An upward trend in the ASR of DALYs was observed exclusively in the Caribbean and Southeast Asia, with EAPCs of 0.64 (95% CI 0.30–0.99) and 0.52 (95% CI 0.31–0.74), respectively.
The top three countries and territories with the highest ASR of DALYs due to syphilis were the Solomon Islands (920.93/100,000), Equatorial Guinea (727.02/100,000), and Liberia (717.24/100,000), while those with the lowest were Slovenia, Lithuania, and Hungary (Fig. 4B). The details are listed in Supplementary Table 2. Overall, the ASR of DALYs exhibited a predominantly declining trend across most regions worldwide. Additionally, Turkmenistan (EAPC = − 9.58 95% CI − 11.48 to − 7.68) and Panama (EAPC = 3.51, 95% CI 2.46–4.56) exhibited the most significant downward and upward trend in ASR of DALYs, respectively.
Discussion
This study provides a comprehensive estimation of the global prevalence of syphilis and its associated DALYs, over the past three decades. The main findings were as follows: (1) The ASR of the prevalence of syphilis remained stable from 1990 to 2019, whereas the ASR of the DALYs due to syphilis decreased globally. (2) The highest ASR of the DALYs was observed among individuals younger than 14 years. (3) The burden of syphilis decreased with an increase in the SDI. Solomon Islands, Equatorial Guinea, and Liberia exhibited the highest age-standardized DALYs rates in 2019 among 204 countries or territories investigated.
Several regional studies have provided evidence that affirms the persistently high prevalence of syphilis7,8,9,20. The reason may be due to the development of diagnostic capacity in the countries studied, which has led to an increase in the number of declared cases. Additionally, the increased numbers of men engaging in same-sex sexual activity21, and the patterns of sexual behavior among adolescents may play a relatively crucial role22. Furthermore, an increase in the frequency of travel may be attributed to the transmission of syphilis23. While pre-exposure and post-exposure prevention measures are available to mitigate the risk of STIs24,25, insufficient awareness of syphilis may be a probable reason for its persistence in certain regions26. The use of condoms is the most economical and simple way to prevent the spread of syphilis and other STIs27. Several governments have implemented a series of measures and efforts to promote the use of condoms and prevent the spread of STIs28. For instance, government initiatives provide free or affordable condoms, while family planning and healthcare organizations distribute free condoms to individuals, concurrently promoting safe sex education. Volunteers are additionally mobilized within the community to raise awareness and educate people about condoms and safe sex practices. Furthermore, governments have actively promoted the implementation of comprehensive sex education programs in schools and communities. These initiatives aim to educate young individuals and adults about contraception, safe sexual practices, and the importance of understanding their own physical and sexual behaviors. The objective is to help individuals develop realistic reproductive health plans29,30.
Although syphilis has a high prevalence, the ASR of the DALYs has decreased over the past three decades. This may have been due to the effectiveness of the current therapy. Furthermore, the declining trend in syphilis cases may be attributed to the expanding diagnostic capabilities and improved access to health services, particularly in terms of antimicrobial agent treatment. Antibiotics are the most effective treatment for syphilis31 and can significantly reduce the morbidity and mortality of syphilis in humans32. However, antimicrobial resistance has increased worldwide as a consequence of the widespread use of antimicrobial agents. At present, many countries are experiencing an increase in antibiotic resistance, which poses a growing threat to the burden of syphilis33,34. Appropriate use of antibiotics is indispensable to minimize the burden of antibiotic resistance in syphilis35. In addition, there is an urgent need for the development of novel antibiotics36. Finally, syphilis has a wide variety of clinical manifestations and can be easily misdiagnosed if the specific antibody is not tested37. In addition to causing damage to the genitourinary system, syphilis has to potential to harm other organs, including the cardiovascular, nervous, and ocular systems38,39. If left untreated, syphilis can pose life-threatening risks.
Additionally, we observed a paradoxical phenomenon, in which the age group aged under 14 years exhibited the lowest prevalence but the highest rate of DALYs. This indicates that early exposure to syphilis can lead to adverse outcomes. Therefore, there is a critical need for sexual protection for syphilis among younger individuals40. Another important reason for the high burden of DALYs in this age group may be the vertical transmission of syphilis, which may contribute to poorer outcomes in younger individuals41. Congenital syphilis due to vertical transmission can cause neonatal death, as well as cutaneous and visceral manifestations. Early diagnosis and treatment are effective measures to reduce prevalence and mortality42. Therefore, it is crucial to strengthen the existing screening practices for pregnant women and establish thorough follow-up evaluations for women who have contracted syphilis43,44.
Another important finding of our study was that the burden of syphilis decreased with the increase in SDI level. This is consistent with the cross-sectional study by Costa et al., which showed a significant association between family income and STIs45. Additionally, the present study highlights the substantial disease burden of STIs in developing countries, particularly in Sub-Saharan Africa, Oceania, and the Caribbean. Hence, extensive strategies for the effective control and management of syphilis should be extensively implemented in developing countries for screening, education, and treatment46,47. The Solomon Islands, Equatorial Guinea, and Liberia were among the less developed countries in the world48,49 that exhibited the highest ASR of DALYs.
Limitations
The study is subject to certain inherent limitations. First, data from the GBD database primarily focuses on economically developed countries, and there may be a lack of comprehensive health data for certain poorer or developing countries. As a result, the health situation in these regions may not be fully represented50. Furthermore, the collection and update of data may have certain delays, particularly during emergencies or large-scale outbreaks. As a result, there could be some lag in the availability of updated data. There are several suggestions for future research in this field. With the advancement of technology and the development of data collection methods, more accurate data can be obtained by enhancing the speed of data updates. Furthermore conducting data analysis from multiple perspectives through the integration of different data sources, analysis methods, and disease classification standards can improve the accuracy and precision of the data.
Conclusion
The ASR of the prevalence of syphilis remained persistently high from 1990 to 2019 worldwide, with no significant changes observed. Conversely, the ASR of DALYs attributed to syphilis exhibited a decrease over the same period. There was an inverse relationship between the syphilis burden and SDI levels. Individuals under the age of 14 and regions with a low SDI require greater attention in addressing the burden of syphilis.
Data availability
The data used in this study were publicly accessed. To download the dataset, please visit the Global Health Data Exchange at http://ghdx.healthdata.org/gbd-results-tool.
Abbreviations
- STIs:
-
Sexually transmitted infections
- DALYs:
-
Disability‐adjusted life years
- ASR:
-
Age-standardized rate
- EAPC:
-
Estimated annual percentage changes
- GBD:
-
Global burden of diseases
- SDI:
-
Sociodemographic index
- UI:
-
Uncertainty intervals
- CI:
-
Confidence interval
References
Rowley, J. et al. Chlamydia, gonorrhoea, trichomoniasis and syphilis: Global prevalence and incidence estimates, 2016. Bull. World Health Organ. 97, 548–562p. https://doi.org/10.2471/blt.18.228486 (2019).
Spornraft-Ragaller, P. & Varwig-Janßen, D. Sexually transmitted infections and male fertility. Hautarzt 69, 1006–1013. https://doi.org/10.1007/s00105-018-4300-9 (2018).
Huang, J., Lin, S., Wan, B. & Zhu, Y. A systematic literature review of syphilitic hepatitis in adults. J. Clin. Transl. Hepatol. 6, 306–309. https://doi.org/10.14218/jcth.2018.00003 (2018).
Hook, E. W. 3rd. Syphilis. Lancet 389, 1550–1557. https://doi.org/10.1016/s0140-6736(16)32411-4 (2017).
Lee, A. S. D. & Cody, S. L. The stigma of sexually transmitted infections. Nurs. Clin. N. Am. 55, 295–305. https://doi.org/10.1016/j.cnur.2020.05.002 (2020).
Organization, W. H. Global health sector strategy on sexually transmitted infections, 2016–2021. Preprint at https://www.who.int/publications/i/item/WHO-RHR-16.09 (2017).
Stary, A. The changing spectrum of sexually transmitted infections in Europe. Acta Dermato-Venereol. 100, adv00114. https://doi.org/10.2340/00015555-3470 (2020).
Thng, C. C. M. A review of sexually transmitted infections in Australia—considerations in 2018. Acad. Forensic Pathol. 8, 938–946. https://doi.org/10.1177/1925362118821492 (2018).
Sharma, M. et al. Control of sexually transmitted infections and global elimination targets, South-East Asia region. Bull. World Health Organ. 99, 304–311. https://doi.org/10.2471/blt.20.254003 (2021).
Wang, C. et al. New syphilis cases in older adults, 2004–2019: An analysis of surveillance data from South China. Front. Med. (Lausanne) 8, 781759. https://doi.org/10.3389/fmed.2021.781759 (2021).
Htet, K. Z., Lindrose, A. R., O’Connell, S., Marsh, J. & Kissinger, P. The burden of chlamydia, gonorrhea, and syphilis in older adults in the United States: A systematic review. Int. J. STD AIDS 34, 288–298. https://doi.org/10.1177/09564624221149770 (2023).
Newman, L. et al. Global estimates of syphilis in pregnancy and associated adverse outcomes: Analysis of multinational antenatal surveillance data. PLoS Med. 10, e1001396. https://doi.org/10.1371/journal.pmed.1001396 (2013).
Woodring, J. et al. Integrating HIV, hepatitis B and syphilis screening and treatment through the Maternal, Newborn and Child Health platform to reach global elimination targets. West. Pac. Surveill. Response J. 8, 1–5. https://doi.org/10.5365/wpsar.2017.8.3.005 (2017).
GBD, Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet (Lond. Engl.) 396, 1204–1222. https://doi.org/10.1016/s0140-6736(20)30925-9 (2019).
Wu, J. et al. Global, regional and national disability-adjusted life years due to HIV from 1990 to 2019: Findings from the Global Burden of Disease Study 2019. Trop. Med. Int. Health TM & IH 26, 610–620. https://doi.org/10.1111/tmi.13565 (2021).
Zeng, D. Y. et al. Global burden of acute viral hepatitis and its association with socioeconomic development status, 1990–2019. J. Hepatol. https://doi.org/10.1016/j.jhep.2021.04.035 (2021).
Zhang, X., Zeng, Q., Cai, W. & Ruan, W. Trends of cervical cancer at global, regional, and national level: Data from the Global Burden of Disease study 2019. BMC Public Health 21, 894. https://doi.org/10.1186/s12889-021-10907-5 (2021).
Roth, G. A. et al. Global burden of cardiovascular diseases and risk factors, 1990–2019: Update from the GBD 2019 study. J. Am. Coll. Cardiol. 76, 2982–3021. https://doi.org/10.1016/j.jacc.2020.11.010 (2020).
GBD 2019 Viewpoint Collaborators. Five insights from the Global Burden of Disease Study 2019. Lancet (Lond. Engl.) 396, 1135–1159. https://doi.org/10.1016/s0140-6736(20)31404-5 (2020).
Rahimzadeh, S. et al. Burden of sexually transmitted infections in Iran from 1990 to 2010: Results from the global burden of disease study 2010. Arch. Iran. Med. 19, 768–773 (2016).
Bremer, V., Dudareva-Vizule, S., Buder, S., An der Heiden, M. & Jansen, K. Sexually transmitted infections in Germany: The current epidemiological situation. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 60, 948–957. https://doi.org/10.1007/s00103-017-2590-1 (2017).
Shannon, C. L. & Klausner, J. D. The growing epidemic of sexually transmitted infections in adolescents: A neglected population. Curr. Opin. Pediatr. 30, 137–143. https://doi.org/10.1097/mop.0000000000000578 (2018).
Rogstad, K. E. Sexually transmitted infections and travel. Curr. Opin. Infect. Dis. 32, 56–62. https://doi.org/10.1097/qco.0000000000000513 (2019).
Wang, Z. et al. HIV nonoccupational postexposure prophylaxis among men who have sex with men: A systematic review and meta-analysis of global data. AIDS Patient Care STDS 34, 193–204. https://doi.org/10.1089/apc.2019.0313 (2020).
Frickmann, H. Diversification of the prevention of sexually transmitted infections. Future Microbiol. 14, 1465–1468. https://doi.org/10.2217/fmb-2019-0261 (2019).
Nguyen, D. N. et al. Gaps of knowledge about HIV and sexually transmitted infections among industrial workers in Northern Vietnam. AIDS Behav. https://doi.org/10.1007/s10461-021-03370-1 (2021).
Steiner, R. J. et al. Long-acting reversible contraception, condom use, and sexually transmitted infections: A systematic review and meta-analysis. Am. J. Prev. Med. 61, 750–760. https://doi.org/10.1016/j.amepre.2021.04.032 (2021).
Hodder, R. K. et al. The association between adolescent condom use and individual and environmental resilience protective factors. Aust. N. Z. J. Public Health 42, 230–233. https://doi.org/10.1111/1753-6405.12744 (2018).
Farahani, F. K. Adolescents and young people’s sexual and reproductive health in Iran: A conceptual review. J. Sex Res. 57, 743–780. https://doi.org/10.1080/00224499.2020.1768203 (2020).
Muswede, N. J., Tshivhase, L. & Mavhandu-Mudzusi, A. H. Condom use education, promotion and reasons for condom use: Perspectives of healthcare providers and young adults in Vhembe district, Limpopo province. S. Afr. Fam. Pract. 2004(63), e1–e8. https://doi.org/10.4102/safp.v63i1.5326 (2021).
Stamm, L. V. Syphilis: Antibiotic treatment and resistance. Epidemiol. Infect. 143, 1567–1574. https://doi.org/10.1017/s0950268814002830 (2015).
Mohr, K. I. History of antibiotics research. Curr. Top. Microbiol. Immunol. 398, 237–272. https://doi.org/10.1007/82_2016_499 (2016).
Morehead, M. S. & Scarbrough, C. Emergence of global antibiotic resistance. Prim. Care 45, 467–484. https://doi.org/10.1016/j.pop.2018.05.006 (2018).
Alós, J. I. Antibiotic resistance: A global crisis. Enferm. Infecc. Microbiol. Clin. 33, 692–699. https://doi.org/10.1016/j.eimc.2014.10.004 (2015).
Wetzel, C., Lonneman, M. & Wu, C. Polypharmacological drug actions of recently FDA approved antibiotics. Eur. J. Med. Chem. 209, 112931. https://doi.org/10.1016/j.ejmech.2020.112931 (2021).
Crunkhorn, S. Prospecting for new antibiotics. Nat. Rev. Drug Discov. 18, 581. https://doi.org/10.1038/d41573-019-00108-6 (2019).
Tudor, M. E., Al Aboud, A. M. & Gossman, W. G. Syphilis. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing (2023).
Gonzalez, H., Koralnik, I. J. & Marra, C. M. Neurosyphilis. Semin. Neurol. 39, 448–455. https://doi.org/10.1055/s-0039-1688942 (2019).
Krivosheev, A. B., Nadeev, A. P., Kuimov, A. D. & Travin, M. A. Cardiovascular syphilis (current state of the problem and analysis of own observations). Ter. Arkh. 91, 81–85. https://doi.org/10.26442/00403660.2019.11.000246 (2019).
Skaletz-Rorowski, A. et al. Age specific evaluation of sexual behavior, STI knowledge and infection among asymptomatic adolescents and young adults. J. Infect. Public Health 13, 1112–1117. https://doi.org/10.1016/j.jiph.2020.04.005 (2020).
Ito, H., Yamamoto, T. & Morita, S. The type-reproduction number of sexually transmitted infections through heterosexual and vertical transmission. Sci. Rep. 9, 17408. https://doi.org/10.1038/s41598-019-53841-8 (2019).
Ricco, J. & Westby, A. Syphilis: Far from ancient history. Am. Fam. Phys. 102, 91–98 (2020).
Lochner, H. J. 3rd. & Maraqa, N. F. Sexually transmitted infections in pregnant women: Integrating screening and treatment into prenatal care. Paediatr. Drugs 20, 501–509. https://doi.org/10.1007/s40272-018-0310-4 (2018).
Tsai, S., Sun, M. Y., Kuller, J. A., Rhee, E. H. J. & Dotters-Katz, S. Syphilis in pregnancy. Obstet. Gynecol. Surv. 74, 557–564. https://doi.org/10.1097/ogx.0000000000000713 (2019).
Costa, M. et al. Adolescents in situations of poverty: Resilience and vulnerabilities to sexually transmitted infections. Revis. Bras. de Enferm. 73, e20190242. https://doi.org/10.1590/0034-7167-2019-0242 (2020).
Acharya, K., Thapa, R., Bhattarai, N., Bam, K. & Shrestha, B. Availability and readiness to provide sexually transmitted infections and HIV testing and counselling services in Nepal: Evidence from comprehensive health facility survey. BMJ Open 10, e040918. https://doi.org/10.1136/bmjopen-2020-040918 (2020).
Torrone, E. A. et al. Prevalence of sexually transmitted infections and bacterial vaginosis among women in sub-Saharan Africa: An individual participant data meta-analysis of 18 HIV prevention studies. PLoS Med. 15, e1002511. https://doi.org/10.1371/journal.pmed.1002511 (2018).
Gupta, S., Wong, E. G. & Kushner, A. L. Scarcity of protective items against HIV and other bloodborne infections in 13 low- and middle-income countries. Trop. Med. Int. Health TM & IH 19, 1384–1390. https://doi.org/10.1111/tmi.12371 (2014).
Adeyeye, S. A. O., Ashaolu, T. J., Bolaji, O. T., Abegunde, T. A. & Omoyajowo, A. O. Africa and the Nexus of poverty, malnutrition and diseases. Crit. Rev. Food Sci. Nutr. 1, 16. https://doi.org/10.1080/10408398.2021.1952160 (2021).
Adane, A. et al. Routine health management information system data in Ethiopia: Consistency, trends, and challenges. Glob. Health Action 14, 1868961. https://doi.org/10.1080/16549716.2020.1868961 (2021).
Acknowledgements
We thank all contributors to the global burden of diseases 2019 Study.
Funding
This research is supported by Joint Funds for the Innovation of Science and Technology, Fujian Province (No. 2020Y9105), Natural Science Fundation of Fujian Province (No. 2022J01700).
Author information
Authors and Affiliations
Contributions
C.T. and W.B. made the study design and wrote the paper. H.J.F. did the study design and data analysis. W.Y.L. and W.M.F. were involved in manuscript preparation and data collection. H.J.F. and C.T. constructed the tables and figures. H.J.F., W.B. and L.S. revised the final article for important intellectual content.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Chen, T., Wan, B., Wang, M. et al. Evaluating the global, regional, and national impact of syphilis: results from the global burden of disease study 2019. Sci Rep 13, 11386 (2023). https://doi.org/10.1038/s41598-023-38294-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-38294-4
This article is cited by
-
Social and individual vulnerability factors associated with syphilis among populations living on islands in the Brazilian Amazon
BMC Infectious Diseases (2024)
-
Hospitalizations for congenital syphilis in children under one year old in the state of Pará, Brazilian Amazon: ecological study
BMC Pediatrics (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
