
Abstract
In an aging society, it is necessary to detect the cognitive decline of individuals at an early stage using simple measurement methods. This makes early health care possible for those affected. The aim of the study was to develop a classifier for cognitive state in older adults with and without mild cognitive impairment (MCI) based on kinematic parameters of linear and curvilinear aiming arm movements. In a group of 224 older adults over 80 years of age (cognitively healthy and MCI), the movement duration and intersegment intervals of linear and curvilinear arm movements of 20 cm were recorded. Movement duration was significantly longer in the curvilinear condition than in the straight movement, and MCI participants required significantly more time than cognitively healthy participants. Post-hoc analysis on the fluidity of movement in the curvilinear condition showed that MCI men had significantly longer inter-segmental intervals than non-MCI men. No difference was found in women. Based on the inter-segmental intervals, a simple classifier could be developed that correctly classified 63% of the men. In summary, aiming arm movements are only conditionally suitable as a classifier for cognitive states. For the construction of an ideal classifier, age-related degeneration of cortical and subcortical motor areas should be considered.
Similar content being viewed by others


Introduction
Aging is a progressive biological process that leads to structural and functional changes that reduce one’s ability to adapt to environmental stressors1,2. Aging negatively affects cognition, so that even in physically healthy older adults, a slight decline in brain function is observed, which predisposes them to dementia later in life3,4,5. Specifically, fluid intelligence (e.g., perceptual speed, memory, reasoning, verbal knowledge, and verbal fluency) has been shown to decline continuously over the course of life after age 203,5. The decline increases between ages 60 and 703,5 and correlates with hippocampal volume decline3. Large studies have shown that the incidence of dementia increases rapidly after age 65, doubling every 5 years6, with Alzheimer’s disease (AD) accounting for 60% to 70% of all cases7. In Germany, according to the German Alzheimer Society8, the number of dementia patients will increase to three million by 2050. Compared to the prevalence of dementia, the prevalence of a mild cognitive impairment (MCI) is more than double9. Further, in AD the progression of MCI to dementia is estimated to occur in 10% of affected individuals per year9,10. The public health implications are enormous, because AD is also associated with an increased risk of death in addition to incident dementia11. Early detection of dementia and its precursors can enable more sustainable disease management and optimal health care for those affected12. Detected early enough, people with a precursor of dementia (e.g., MCI) could begin programs that help them maintain or change their lifestyles. Many psychometric questionnaires are based on subjective patient reports. These reports may be inaccurate due to disease-related memory impairment and associated loss of insight into the progression of one’s own disease13,14. Alternatively, reports from physicians or family members and caregivers can be used13,14,15. For the latter two groups, prior instruction in the administration of the questionnaires is necessary13. Therefore, the validity of patient questionnaires is limited. Yet, difficulties exist in accurately identifying MCI and early stages of dementia in the population at large using traditional psychometric testing, so it is desirable to develop alternative or additional methods (e.g., easily administered motor tests) for case ascertainment.
Older adults show decreased motor performance, which has been attributed to three factors16: a decrease in central and peripheral sensorimotor functions (e.g., increased noise, reduced tactile sensation), a reduction of information processing (e.g., slowing of movement), and/or changes in the motor system (e.g., loss of motor units, motor unit reorganization) that lead, e.g., to a decreased ability to produce a consistent force result. As such, older subjects show an increased proportion of secondary partial movements in rapid aiming tasks compared to younger subjects16,17,18. According to the optimized submovement model19, motor planning produces a primarily ballistic movement, whereas sensory feedback guides secondary corrective movements during movement execution. Pauses (inter-segment intervals, or ISIs) sometimes occur between each segment of the movement, and these pauses are generally longer or more variable when participants’ motor control or motor planning is less developed or reduced (e.g.17,18,20,21). Therefore, measuring ISIs during aiming movements is a useful measure for assessing human arm movement control18,21. In this context, good motor programming during fast and multi-segment aiming movements is characterized by short movement durations and short ISIs, whereas reduced motor planning ability (such as in MCI or dementia) is characterized by prolonged movement durations and/or ISIs22,23,24,25. This is especially observed in diadochokinetic movements, such as finger tapping (e.g.26).
The aim of this study was to investigate the effects of cognitive state on movement planning and movement production in people over 80 years old. To this end, participants performed two fast aiming arm movements (linear condition and curvilinear condition) with a pen on a tablet. Outcome measures were movement duration and ISIs, with MCI participants expected to perform the tasks more slowly and haltingly than adults without MCI. To classify MCI, participants completed a neuropsychological test battery that included the German version of the MoCA27 and the German version of the Consortium to Establish a Registry for Alzheimer’s Disease Neuropsychological Test Battery (CERAD-NP)28. The CERAD-NP also includes the Mini-Mental State Examination (MMSE). The MoCA was used to measure global cognitive performance and screen for MCI and has a higher sensitivity for mild cognitive impairment than the MMSE29. In addition, we aimed to investigate whether the group differences found were suitable to serve as classifiers for the two cognitive groups. Finger tapping experiments with self-selected or fast paced tapping behavior were also conducted with the same sample of subjects26. The results of the finger tapping experiments (e.g. tap-cycle, tap-duration, force-peak, velocities of flexion and extension as well as the duration of application of constant force to the force plate and the duration without contact to the force plate) were also used as a classifier for the cognitive groups26. Therefore, the classification result of the aiming arm movements was compared with the result of the finger tapping experiments. Since the investigation of the tapping parameters revealed a sex-dependent difference in some parameters26, we further investigated whether women and men solve the two aiming tasks differently. The investigation of the movement results will lead to a better understanding of the basis of motor planning in older adults.
Results
This study investigated the performance of 224 participants over 80 years old while making aiming arm movements consisting of drawing linear and curvilinear lines. Demographic characteristics as well as measures for fine motor skills are reported in Table 1. In particular, fluency by means of ISIs were examined; that is, we examined whether the movements were performed in one motion or haltingly. To minimize the influence of corrective movements to the beginning or end of the movement, the analysis was limited to the middle half of the distance (i.e., 10 cm).
The analysis of the movement duration showed a significant main effect for the factor condition, with longer durations in the curvilinear than in the linear condition (medians: 699 ms vs 1215 ms, respectively; Kruskal–Wallis test, χ2(1) = 113.18, P < 0.001, effect size φ = 0.72). MCI participants needed more time to perform the movements than non-MCI participants (medians: 1073 ms vs 925 ms, respectively; Kruskal–Wallis test, χ2(1) = 6.84, P < 0.009, φ = 0.18). A sex-dependent difference in the duration of all movements could not be shown (median(female): 961 ms, median(male): 971 ms; Kruskal–Wallis test, χ2(1) = 0.001, P < 0.970).
The analysis of movement durations by condition showed that for the condition linear, a main effect was found for the factor cognitive state on trend level (Kruskal–Wallis test, χ2(1) = 3.328, P = 0.068, φ = 0.12) but no significant effect was found for the factor sex (Kruskal–Wallis test, χ2(1) = 0.220, P = 0.639) nor for the interaction of cognitive state and sex (Kruskal–Wallis test, χ2(3) = 3.726, P = 0.293). For the curvilinear condition, a significant effect was found for the factor cognitive state (Kruskal–Wallis test, χ2(1) = 6.358, P = 0.012, , φ = 0.17), but no effect was found for sex (Kruskal–Wallis test, χ2(1) = 0.661, P = 0.416) and an effect on the trend level was found for the interaction cognitive state and sex (Kruskal–Wallis test, χ2(3) = 7.046, P = 0.070, φc = 0.13). The movement durations divided by condition, cognitive state, and sex are reported in Table 2.
Inter-segment intervals (ISIs)
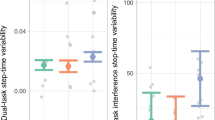
In the curvilinear condition, halting movements occurred in the region of the middle point (Fig. 1A). At this point, it was necessary to convert the abduction in the shoulder and combined extension and pronation in the elbow performed at the beginning of the movement into adduction in the shoulder and combined flexion and supination in the elbow. Thus, diadochokinesis was necessary to execute the movements of both segments. MCI participants showed halting movements with ISIs at the time of movement change. A characteristic example for an MCI participant (Fig. 1A inset, red points) showed a dense accumulation of points and abrupt, choppy changes in direction of movement. These uneven movements with halting were also evident in the time differences of the data points, which could be 100 ms or more (Fig. 1C, delta-time at ~ 12.5 cm y position). In contrast, the example for a non-MCI participant (Fig. 1A inset, blue points) showed a fairly even spacing between the individual data points, indicating that the movement was performed as one segment with the same average speed. The time intervals of the individual data points in this area corresponded to the sample interval (Fig. 1D), and there was no halting of the movement. The halting movements occurred more frequently and for a longer time in MCI men than in all other groups (Fig. 2). The analysis of the ISIs showed a significant main effect for the factor cognitive state with longer duration for MCI participants (medians: 145 ms vs 94 ms, respectively; Kruskal–Wallis test, χ2(1) = 9.682, P = 0.002, φ = 0.21), no difference for the factor sex (female: 82 ms, male: 84 ms; Kruskal–Wallis test, χ2(1) = 0.541, P = 0.462) and a significant effect for the interaction of cognitive state and sex (Kruskal–Wallis test, χ2(3) = 10.511, P = 0.015, φc = 0.15). The ISIs divided by cognitive state and sex are shown in Fig. 2. The post-hoc analysis on the fluidity of movement in the curvilinear condition showed that MCI men had significantly longer ISIs than non-MCI men, whereas no difference was found in women (male: P = 0.039, female: P = 0.972, both Bonferroni corrected; Fig. 2). Using the estimators of the 95% confidence interval of the medians (notches of the boxplots in Fig. 2B), a classification threshold of 100.4 ms was calculated for the male participants as the mean of the upper estimator of the non-MCI participants and the lower estimator of the MCI participants. Overall, 73/116 (63%, φ = 0.26, Table 3: curvilinear task) of the participants could be correctly classified, which was better than the theoretical value of 56% (see “Methods” section).

Methods. (A) Characteristic examples of drawing motion of a non-MCI participant (blue line) and an MCI participant (red line). Only the drawing movement between the horizontal dashed lines was used in the analysis, i.e., in the range from 8 to 18 cm for the vertical position of the tablet. The individual sequence of measuring points during the drawing movement in the area of the middle circle is shown in the inset; x-axis = x position and y-axis = y position of the tablet in cm. (B) The experimental setup. (C,D) Time difference between the individual measurement points of the drawing movement for an MCI participant (C) and for a non-MCI participant (D). The vertical dashed lines in (C,D) indicate the range of the y position used for further analysis (see A). The horizontal thin line indicates the mean sampling interval of about 5.7 ms, and the dashed horizontal line indicates the threshold of 1.5 times the sampling interval (8.6 ms).

Boxplots of inter-segment intervals (ISIs) in the curvilinear condition. (A) Female participants, (B) male participants. The boxes represent the mean 50th percentile, the thick line represents the median, and the whiskers the range of data belonging to each group. Outliers are represented as circles. Outliers above 500 ms are not displayed for visual reasons. Blue boxplots indicate the distribution of non-MCI participants and red boxplots of MCI participants. The width of each boxplot reflects the relative proportion of the number of participants. The notches reflect the estimator of the 95% confidence interval of the median. The dashed line in B indicates the classification threshold of 100.4 ms.
A comparison of the cognitive scales MoCA and MMSE as well as the years of education divided by cognitive status and sex shows that women had significant fewer years of education (Kruskal–Wallis test, χ2(1) = 27.647, P < 0.001, φ = 0.35), and higher MoCA score (Kruskal–Wallis test, χ2(1) = 11.523, P < 0.001, φ = 0.23) than men (Table 1). It further evidences that for the MMSE score, there is a significant difference between non-MCI and MCI females (Kruskal–Wallis test, χ2(1) = 8.387, P < 0.001, φ = 0.19) and for the MoCA score, there is a significant difference between non-MCI and MCI participants in both females and males (Kruskal–Wallis test, χ2(3) = 114.72, P < 0.001, φc = 0.41) (Table 1). Examination of participants’ the fine motor skills (see “Methods” section) revealed a significant difference between non-MCI and MCI participants only for the CERAD TMT A score independent of the sexes (Kruskal–Wallis test, χ2(1) = 4.6286, P = 0.031, φ = 0.14). Regression analysis between ISIs and the TMT A score show that the differences are given by the MCI men (slope = 2.76, P = 0.006, F(1, 36) = 9.993, adjusted R2 = 0.20).
Comparison of tapping and aiming arm behavior
In a recently published study26, we reported the possibility of classifying participants based on selected movement parameters of a tapping task during self-selected or fast pace. For the 116 male participants from this current study, the tapping parameters were additionally analyzed and the participants were classified accordingly. Classification using tapping algorithm classified 93 participants as non-MCI (of which 70 were correctly classified) and 23 participants as MCI (of which 15 were correctly classified, φ = 0.32, Table 3A), giving it a sensitivity of 39% and a specificity of 90%. When the aiming behavior of the same 116 male participants in the current study was examined, 61 participants were classified as non-MCI (of which 48 were correctly classified) and 55 participants as MCI (of which 25 were correctly classified φ = 0.29, Table 3A). In summary, the sensitivity was 66% and the specificity 62%. Combining both algorithms in the form of a logical AND, that is, those classified as non-MCI in the tapping algorithm must additionally have ISIs < 100.4 ms and those classified as MCI must also have ISIs ≥ 100.4 ms could be performed on a subset of 70 participants. This resulted in 54 participants classified as non-MCI and 16 classified as MCI. The total sensitivity was 12/22 (55%) and the specificity 44/48 (92%) with an effect size of φ = 0.48 (Table 3B: combining both tasks). Thus, it appears that the combination of the two examinations improved the classification of the male participants.
Discussion
This study examined the performance of participants over 80 years old when making linear and curvilinear aiming arm movements. Results showed that some of the differences between female and male participants could be attributed to a change in behavior of MCI males. They performed the curvilinear movement more haltingly and with longer ISIs. Based on this time difference, a simple classifier could be developed that correctly classified 63% of the men. Combining this classification with the classification based on tapping parameters26, such that participants were classified as either non-MCI or MCI in both algorithms, showed that of the men so classified, 44 of the 54 (81%) classified as non-MCI men and 12 of the 16 (75%) classified as MCI men were correctly identified. On the other hand, it should be noted that no acceptable identification was found for 46 out of 116 men performing both tests.
Our study design was guided by the study of Yan21, who measured linear and curvilinear arm movements in 20 participants over 80 years old. For a total distance of 20 cm, his participants needed ~ 700 ms for the linear and about 1330 ms for the curvilinear condition (Fig. 5 in Ref.21). This was significantly faster than what was found in this study. It should be noted that in Yan’s study21, the older participants had 3–8 practice trials and then repeated the task until 10 successful trials per condition were measured. They also had to respond to a start signal in a range of 150 to 500 ms. In our study, the subjects had no practice trials, and 7 trials without repetition were measured. In addition, participants started each trial independently. It can therefore be assumed that the participants in our study performed the task with more calmness and caution. Another difference is the index of difficulty (ID) according to Fitt’s law30. With higher ID, the movement duration increases and the ISI increases, especially in older subjects31. In the linear condition, the ID in Yan’s study was 4.321, whereas in this study it was 4.7. For the curvilinear condition, the ID for the movement to the middle circle in Yan’s study was 2.5 and for the subsequent movement to the target 3.521. In our study, the corresponding values were 4.2 and 3.9. Hence, movements were more difficult in our study, and this might explain the temporal differences.
Few studies have investigated hand movements in the prodromal stage of dementia such as MCI (for review, see23). Kinematic parameters such as outcome measure in aiming movements have only been used in two studies to discriminate healthy older participants from MCI participants. Comarda et al.22 showed in a comparable task for the linear condition that MCI patients (N = 11) took significantly longer to perform the movement than non-MCI participants (N = 11). Yan et al.25 came to the same conclusion when they studied a group of 10 non-MCI participants and 9 MCI participants. Thus, the results of our studies confirmed the previous exploratory studies on smaller groups. Furthermore, our experiments showed that there was a sex difference in the performance of the curvilinear condition. A significant difference was found for male participants in the total duration of ISIs between non-MCI and MCI participants. This difference allowed for separation of the two groups. A comparable difference was not found for female participants.
Our previous study on tapping behavior had shown that the force used for tapping was a relevant factor for distinguishing between groups as well as sexes26. It is therefore possible that the overall longer ISIs of the MCI men were caused by an excessive grip force and higher contact pressure of the pen on the tablet. Hertzum and Hornbaek32 showed that the movement parameters in aiming tasks differ when using a tablet and pen or an optical mouse, as they found that the use of a mouse required less force to move or hold. They also showed that movements with a pen were performed significantly slower than with a mouse, whereby this occurred more in older subjects32. Force measuring films have been shown to be suitable for measuring the grip forces and position of individual fingers33,34 as well as their dynamics during movement35. Findings from writing studies have shown that applying these films on a pen is possible36,37. Therefore, it is recommended that such systems are used in the future to further elucidate the forces during the drawing behavior of MCI men. That MCI males show a different drawing behavior is also evident from the TMT A scores. Only for this subgroup a correlation between ISIs and the TMT A score could be shown. Therefore, it can be assumed that the measurement of ISIs in drawing movements with multiple directional changes, as they occur in the TMT A, allows a better discrimination of MCI males. That there are no other correlations with the other two fine motor skill measures is due to the respective assessment of these measures. For example, the CERAD drawing score assesses the quality of a drawing and not its execution. The FM score is a self-reported frequency of performing at least one of a selection of fine motor skills (playing a musical instrument, typing on a keyboard, writing, needlework, model building or other fine motor skills). The high values of the FM score are noteworthy (Table 1). This is an indication that there is a selection bias in the recruitment of participants. Thus, an explicit inclusion criterion was that the participants manage the way to and from the laboratory by means of self-organized transport. Thus, they are not representative of all people over 80 years of age. On the other hand, the entire study protocol was explicitly developed for this group12.
A limitation of this study is the discontinuous data collection of the tablet. This resulted in an uneven and unpredictable loss of data points over time. Therefore, higher mathematical techniques such as jerk analysis were not useful. Nevertheless, a simple technique for evaluating target movements can be derived from this study. Effectively, the non-transmission of the data acts as a high-pass filter of velocity, since a continuous transmission of the pen position only occurred for a minimum movement speed of the pen. It is technically possible to set up a filter even with continuous data acquisition. By doing so, the duration of falling below the velocity threshold can simply be measured, and the sum of the ISIs can be read.
In addition to the experimental conditions, the neurological status of the participants must also be considered. All participants reported no neurological deficits (an exclusion criterion; see “Methods” section). However, individuals may have had varying degrees of age-related degeneration and in different relevant areas of the CNS (e.g., cortex, spinal cord, basal ganglia, cerebellum). It is known that the cerebellum is generally important for the coordination of motor performance, such as diadochokinesis. Limitations in aiming behavior can be explained not only by cognitive impairment but also by age-related cerebellar decline38,39,40,41. Different portions of the cerebellum correlate with motor abilities than correlate with cognitive abilities (reviewed in Ref.26). Age-related degeneration of the motor cerebellum is comparable to degeneration in cerebellar diseases39. In the aiming task, it can be assumed that the degeneration of the motor cerebellum has an influence on performance. Therefore, the lack of definite classification in 46 of 116 men may be explained by varying degrees of cerebellar degeneration. Overall, the two tasks differ in their use of arm/hand muscles, with a greater emphasis on finger muscles in tapping. Considering the different innervation of cortical and sub-cortical areas of the arms and fingers42, the individual variations in task performance may indicate different impairments of brain areas.
Overall, the possible degeneration of relevant motor systems (e.g., the cerebellum) should be considered when examining the cognitive state by means of movements. First, additional motor tests can be performed to specifically determine the degeneration of the above mentioned areas26. Second, different tasks can be combined whose results allow the construction of a classifier (e.g., tapping behavior, aiming arm behavior) to increase sensitivity or specificity.
Methods
This study is part of the SENDA study (Sensor-based systems for early detection of dementia, registered in the German Clinical Trials Register under DRKS00013167), which was conducted at Chemnitz University of Technology, Germany. The detailed study protocol was published earlier12. Sample size calculation showed that 200 participants are required for analysis with α = 0.05 and power = 0.8012. Only information relevant to the current research question is described here.
Participants
The SENDA study was advertised by local general practitioners and in newspapers. In total, 244 participants (123 males; age 79–93 years; M = 82.5; SD = 2.5) took part in the study and were recruited from January 2018 to March 2020. Study participation required walking ability, sufficient German language skills, residence in or around Chemnitz, Germany, and a self-organized means of travel to and from the laboratory. Volunteers were excluded before testing if any of the following criteria applied: (1) acute psychological disorder; (2) diagnosis of any neurocognitive or neurological disorder; (3) past traumatic head injury; (4) substance abuse; (5) participation in other clinical studies; (6) a physician-directed ban from physical activities; (7) severe restrictions due to cardiovascular, pulmonary, or orthopedic diseases; or (8) failure to reach the minimum required score of 19 during screening with the Montreal Cognitive Assessment (MoCA)27. Each participant received a total of 25 EUR compensation for each measurement time point with three individual appointments for their participation.
The analysis for this article included 224 participants who took part at the baseline measurement. Exclusion from analysis was due to dropout from the study before all needed testing was completed (n = 18) or technical issues during the recording (n = 2). Due to the participants’ old age, many followed a medication regimen (n = 200), which most often included medication for high blood pressure, thrombosis prophylaxis, cholesterol reduction, stomach acid reduction, or thyroid function.
Neuropsychological testing and MCI classification
The neuropsychological testing and MCI classification are described in detail elsewhere43. Briefly, all participants went through an intensive neuropsychological test battery, which was carried out by trained testing staff at the university lab. The tests included the German version of the MoCA27 and the German version of the Consortium to Establish a Registry for Alzheimer’s Disease Neuropsychological Test Battery (CERAD-NP)28. The MoCA was used to measure global cognitive functioning and to screen for MCI. The MoCA is the second-most-utilized geriatric cognitive screening tool after the Mini-Mental State Examination (MMSE) and has superior sensitivity to mild cognitive impairments29. The CERAD-NP examines the cognitive domains of memory, language, executive functions, and visuo-construction. MCI classification was based on the recommendations of The National Institute on Aging and the Alzheimer’s Association44 and in accordance with the criteria proposed by45. Cognitive impairments were determined according to performance in MoCA (one sum score) and CERAD-NP (nine separate test scores). The following CERAD-NP scores were used: verbal fluency, Boston naming test, phonematic, constructional praxis, word list learning, word list recall, word list recognition, constructional praxis recall, and trail making test. We followed a two-step procedure recommended for diagnosis of MCI in the general population, which states that, first, a screening should be used, and, second, in the case of abnormal findings, in-depth cognitive testing should follow46. A MoCA score below 26 points and at least one CERAD-NP test performance at least 1.5 standard deviations below the normative mean (taking into consideration age, sex, and education level) resulted in classifying the participant as having mild cognitive impairments (MCI). All other participants were considered non-MCI according to Ref.46, because these individuals did not have abnormal values in screening (MoCA > 25) or show cognitive impairment in the in-depth clinical tests.
Tasks and recording
Participants carried out three fine motor tasks12, including (1) force modulation of a precision grip with the thumb and index finger47; (2) tapping with the index finger of the right hand26; and (3) aiming arm movements by connecting dots on a touchscreen with a pen as studied by Yann21. Here we report the results of the third motor task, experiment (3) and compared them to the results of experiment (2). In experiment (2) participants tapped with one’s dominant index finger on the force transducer in two different conditions: at a self-selected pace or as fast as possible (see26). Task and experimental setup of experiment (3) have been reported elsewhere12 and are briefly summarized here. A touch monitor (Manufacturer: Hannstar Display Corp., 23.0 in., hardware resolution 1920 × 1080 pixels, Taipei City, Taiwan; Modell: HSG 1353) and a touch pen (WACOM Bamboo-Stylus Alpha CS-180, length 130 mm, diameter 9 mm, weight 12 g) were used. The monitor was placed horizontally on a table in front of the participant. The pen was held in the participant’s dominant hand (see Fig. 1B). The data acquisition and visual feedback during the experimental procedures in real time were programmed using a customized script for LabView 2015 (National Instruments, Austin, TA, USA). The program recorded the x and y positions of the pen and the time stamp of the measurement at an average sampling frequency of 175 Hz. Participants had to connect points on the touchscreen (black desktop background) with the pen by drawing a line. There were two tasks: drawing a linear and a curvilinear line. For the linear condition, two green dots (diameter 15 mm) were displayed on the screen aligned vertically, one marked ’Start’ and one ‘Target’ (see Fig. 1B). In the curvilinear condition, a third white intermediate point (diameter 12.5 mm) was presented halfway between the ‘Start’ and ‘Target’ dots (horizontal distance 25% of the ‘Start’–‘Target’ distance to the right), through which participants had to draw a curved line in one stroke (see Fig. 1B). Participants received feedback by having a white line displayed on the tablet’s screen. In both conditions (linear and curvilinear), two different distances (50 mm and 200 mm) between the ‘Start’ and ‘Target’ points were tested. In total, four conditions (linear short, linear long, curvilinear short, and curvilinear long) were performed as a block with seven trials in each condition, and the conditions appeared in a random order. Overall time to perform all four blocks was less than 8 min.
Data analysis
The data analysis included two measurement variables: the movement duration and the inter-segment intervals (ISIs) for the fluidity of the individual movement. Each trial was started independently by the participants by placing the pen on the tablet. Some participants simultaneously placed the pen and their hand on the tablet when starting the trial; therefore, it was not always possible to clearly determine the start of the movement. While performing the task, the participant received visual feedback in the form of the drawn line, shown in white. The correct execution of the task with only the pen touching the tablet is shown in Fig. 1B. At the moment the pen touched the circular line of the circle ‘Target’, both the white line and the ‘Start’ and ‘Target’ circles disappeared. Therefore, visuomotor control at the end of the movement was different from that during the movement, and analysis of the movements was not comparable. To ensure that the movement analysis was not influenced by effects at ‘Start’ or around ‘Target’, a safety distance of 15 mm from the center of the ‘Start’/‘Target’ circles was excluded for analysis. As such, of the original 50 mm distance for the short conditions (linear short, curvilinear short), only a distance of 20 mm was available for analysis. This was too short, and these conditions were excluded from further analysis. For the 200 mm conditions, to exclude effects of the ‘Target’ and ‘Start’ areas on the movement, only the middle half of the movement (8–18 cm) for the long conditions was used for analysis. This area contained the position of the laterally offset circle in the center of the curvilinear condition. The movement duration resulted from the difference of the time stamps between the first measuring point above the 8-cm y position and the last measuring point below the 18-cm y position. The total duration of inter-segmental intervals (ISIs) was used as a measure of the fluidity of the movement. The detailed calculation of this measure is described in the following paragraph and was developed to fit the data-recording properties of the tablet.
The tablet measured a pen position only if the position changed by more than one pixel (0.265 mm edge length) within the average sampling interval of ~ 5.7 ms. This meant that if the pen was not moved by at least 1 pixel within a scan interval, no new data was transmitted from the tablet and captured. As a result, very slow or halting movements led to discontinuous recording of the measured values. For steady movements (in one stroke), the time difference between two consecutive data points was equal to the average sampling time, while it was larger for halting movements. Figure 1C,D show the time differences of the individual measurement points of the two characteristic line traces in Fig. 1A for a participant with MCI (1C, red line in Fig. 1A) and a non-MCI participant (1D, blue line in Fig. 1A). A movement was considered halting if time differences exceeded 1.5 times the sampling interval, i.e., 8.6 ms (horizontal dashed line in Fig. 1C,D). For the calculation of the ISI per trial, the difference between the actual movement duration and the number of time stamps × sampling interval (theoretical minimum movement duration) within the analysis range of the movement (y position 8–18 cm, vertical dashed lines in Fig. 1C,D) was calculated.
For further analysis, only data from subjects from whom at least four valid trials could be analyzed were used48. The mean value per subject and condition was calculated for all valid trials for further comparisons. Data analysis as well as statistical analysis was performed using the R 3.6.3 base package49. Since the data were not normally distributed, group comparisons were made using the Kruskal–Wallis test with the factors cognitive state (non-MCI and MCI) and sex (female and male). For pairwise post-hoc comparisons, Wilcoxon rank sum tests were computed. Multiple testing was performed with Bonferroni correction. Effect sizes are given as Phi coefficient (φ) and Cramer’s V (φc) when appropriated. To calculate the probability of correctly classifying a participant by chance, the original classification labels were randomly redistributed 100,000 times and the proportion of correctly assigned participants was calculated for each run. The theoretical probability is given as the mean of all runs as a percentage.
To assess fine motor skills, we calculated three scores. The FM score (Table 1) is derived from the frequency of performing different tasks (answered on a 6-point Likert scale for each task, with 1 = never to 6 = very often) that require fine motor skills (playing a musical instrument, typing on a keyboard, writing, needlework, model building or other fine motor skills). The highest score for each subject was scored regardless of the task. Based on the drawing task of the CERAD-NP test battery, a drawing ability score was calculated as the sum of the 4 tests for drawing a circle, rhombus, rectangle and cube (CERAD drawing score, Table 1). Furthermore, the ratio of the duration of Trail Making Test B to Trail Making Test A was calculated (CERAD TMT B/A, Table 1).
Ethical approval
The study was approved by the Ethics Committee of Chemnitz University of Technology, Germany, Faculty of Behavioral and Social Sciences (V232-17-KM-SENDA-07112017, approved on 19 December 2017). All methods and procedures were performed in accordance with the ethical standards of the Helsinki Declaration of the World Medical Association.
Informed consent
Each participant signed a written in-formed consent form.
Data availability
The datasets analyzed during the current study are not publicly available but are available from the corresponding author on reasonable request.
References
Boccardi, V., Comanducci, C., Baroni, M. & Mecocci, P. Of energy and entropy: The ineluctable impact of aging in old age dementia. Int. J. Mol. Sci. 18, 2672 (2017).
Behfar, Q., Ramirez Zuniga, A. & Martino-Adami, P. V. Aging, senescence, and dementia. J. Prev. Alzheimer’s Dis. 9, 523–531. https://doi.org/10.14283/jpad.2022.42 (2022).
Hedden, T. & Gabrieli, J. D. E. Insights into the ageing mind: A view from cognitive neuroscience. Nat. Rev. Neurosci. 5, 87–96. https://doi.org/10.1038/nrn1323 (2004).
Ishii, R. et al. Healthy and pathological brain aging: From the perspective of oscillations, functional connectivity, and signal complexity. Neuropsychobiology 75, 151–161. https://doi.org/10.1159/000486870 (2017).
Sánchez-Izquierdo, M. & Fernández-Ballesteros, R. Cognition in healthy aging. Int. J. Environ. Res. Public Health 18, 962 (2021).
Pierce, A. L., Bullain, S. S. & Kawas, C. H. Late-onset Alzheimer disease. Neurol. Clin. 35, 283–293. https://doi.org/10.1016/j.ncl.2017.01.006 (2017).
Corrada, M. M., Brookmeyer, R., Paganini-Hill, A., Berlau, D. & Kawas, C. H. Dementia incidence continues to increase with age in the oldest old: The 90+ study. Ann. Neurol. 67, 114–121. https://doi.org/10.1002/ana.21915 (2010).
e.V., D. A. G. Informationsblatt 1 Die Häufigkeit von Demenzerkrankungen 10. https://www.deutsche-alzheimer.de/fileadmin/Alz/pdf/factsheets/infoblatt1_haeufigkeit_demenzerkrankungen_dalzg.pdf (2020).
Morris, J. C. et al. Mild cognitive impairment represents early-stage Alzheimer disease. Arch. Neurol. 58, 397–405. https://doi.org/10.1001/archneur.58.3.397 (2001).
Petersen, R. C. Mild cognitive impairment. N. Engl. J. Med. 364, 2227–2234. https://doi.org/10.1056/NEJMcp0910237 (2011).
Bennett, D. A. et al. Natural history of mild cognitive impairment in older persons. Neurology 59, 198–205. https://doi.org/10.1212/wnl.59.2.198 (2002).
Müller, K. et al. Sensor-based systems for early detection of dementia (SENDA): A study protocol for a prospective cohort sequential study. BMC Neurol. 20, 84. https://doi.org/10.1186/s12883-020-01666-8 (2020).
Frank, L., Lenderking, W. R., Howard, K. & Cantillon, M. Patient self-report for evaluating mild cognitive impairment and prodromal Alzheimer’s disease. Alzheimers Res. Ther. 3, 12. https://doi.org/10.1186/alzrt97 (2011).
Vogel, A. et al. Awareness of deficits in mild cognitive impairment and Alzheimer’s disease: Do MCI patients have impaired insight? Dement. Geriatr. Cogn. Disord. 17, 181–187. https://doi.org/10.1159/000076354 (2004).
Farias, S. T., Mungas, D. & Jagust, W. Degree of discrepancy between self and other-reported everyday functioning by cognitive status: Dementia, mild cognitive impairment, and healthy elders. Int. J. Geriatr. Psychiatry 20, 827–834. https://doi.org/10.1002/gps.1367 (2005).
Walker, N., Philbin, D. A. & Fisk, A. D. Age-related differences in movement control: Adjusting submovement structure to optimize performance. J. Gerontol. Ser. B 52B, P40–P53. https://doi.org/10.1093/geronb/52B.1.P40 (1997).
Yan, J. H., Thomas, J. R. & Stelmach, G. E. Aging and rapid aiming arm movement control. Exp. Aging Res. 24, 155–168. https://doi.org/10.1080/036107398244292 (1998).
Yan, J. H., Thomas, J. R., Stelmach, G. E. & Thomas, K. T. Developmental features of rapid aiming arm movements across the lifespan. J. Mot. Behav. 32, 121–140. https://doi.org/10.1080/00222890009601365 (2000).
Meyer, D., Abrams, R., Kornblum, S., Wright, C. & Smith, J. Optimality in human motor performance: Ideal control of rapid aimed movements. Psychol. Rev. 95, 340–370. https://doi.org/10.1037/0033-295X.95.3.340 (1988).
Rand, M. K., Alberts, J. L., Stelmach, G. E. & Bloedel, J. R. The influence of movement segment difficulty on movements with two-stroke sequence. Exp. Brain Res. 115, 137–146. https://doi.org/10.1007/PL00005673 (1997).
Yan, J. H. Effects of aging on linear and curvilinear aiming arm movements. Exp. Aging Res. 26, 393–407. https://doi.org/10.1080/036107300750015778 (2000).
Camarda, R. et al. Movements execution in amnestic mild cognitive impairment and Alzheimer’s disease. Behav. Neurol. 18, 135–142. https://doi.org/10.1155/2007/845914 (2007).
Ilardi, C. R., Iavarone, A., La Marra, M., Iachini, T. & Chieffi, S. Hand movements in mild cognitive impairment: Clinical implications and insights for future research. J. Integr. Neurosci. 21, 17. https://doi.org/10.31083/j.jin2102067 (2022).
Wu, Q., Chan, S.-Y. & Yan, J. Mild cognitive impairment affects motor control and skill learning. Rev. Neurosci. 27, 20. https://doi.org/10.1515/revneuro-2015-0020 (2015).
Yan, J. H., Rountree, S., Massman, P., Doody, R. S. & Li, H. Alzheimer’s disease and mild cognitive impairment deteriorate fine movement control. J. Psychiatr. Res. 42, 1203–1212. https://doi.org/10.1016/j.jpsychires.2008.01.006 (2008).
Kutz, D. F., Fröhlich, S., Rudisch, J., Müller, K. & Voelcker-Rehage, C. Finger tapping as a biomarker to classify cognitive status in 80+-year-olds. J. Person. Med. 12, 286 (2022).
Nasreddine, Z. S. et al. The Montreal cognitive assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 53, 695–699. https://doi.org/10.1111/j.1532-5415.2005.53221.x (2005).
Moms, J. C. et al. The Consortium to establish a registry for Alzheimer’s Disease (CERAD). Part I. Clinical and neuropsychological assesment of Alzheimer’s disease. Neurology 39, 1159–1159. https://doi.org/10.1212/wnl.39.9.1159 (1989).
Breton, A., Casey, D. & Arnaoutoglou, N. A. Cognitive tests for the detection of mild cognitive impairment (MCI), the prodromal stage of dementia: Meta-analysis of diagnostic accuracy studies. Int. J. Geriatr. Psychiatry 34, 233–242. https://doi.org/10.1002/gps.5016 (2019).
Fitts, P. M. The information capacity of the human motor system in controlling the amplitude of movement. J. Exp. Psychol. 47, 381–391. https://doi.org/10.1037/h0055392 (1954).
Ketcham, C. J., Seidler, R. D., Van Gemmert, A. W. A. & Stelmach, G. E. Age-related kinematic differences as influenced by task difficulty, target size, and movement amplitude. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 57, P54–P64. https://doi.org/10.1093/geronb/57.1.P54 (2002).
Hertzum, M. & Hornbæk, K. How age affects pointing with mouse and touchpad: A comparison of young, adult, and elderly users. Int. J. Hum. Comput. Interact. 26, 703–734. https://doi.org/10.1080/10447318.2010.487198 (2010).
Kutz, D. F., Wölfel, A., Timmann, D. & Kolb, F. P. Detection of changes in grip forces on a sliding object. J. Neurosci. Methods 166, 250–258. https://doi.org/10.1016/j.jneumeth.2007.07.014 (2007).
Kutz, D. F., Wölfel, A., Timmann, D. & Kolb, F. P. Dynamic torque during a precision grip task comparable to picking a raspberry. J. Neurosci. Methods 177, 80–86. https://doi.org/10.1016/j.jneumeth.2008.09.031 (2009).
Kutz, D. F., Wölfel, A., Meindl, T., Timmann, D. & Kolb, F. P. Spatio-temporal human grip force analysis via sensor arrays. Sensors 9, 6330–6345 (2009).
Chau, T., Ji, J., Tam, C. & Schwellnus, H. A novel instrument for quantifying grip activity during handwriting. Arch. Phys. Med. Rehabil. 87, 1542–1547 (2006).
Ghali, B., Mamun, K. A. & Chau, T. Long term consistency of handwriting grip kinetics in adults. J. Biomech. Eng. Trans. ASME 136, 7. https://doi.org/10.1115/1.4026641 (2014).
Gellersen, H. M., Guell, X. & Sami, S. Differential vulnerability of the cerebellum in healthy ageing and Alzheimer’s disease. NeuroImage Clin. 30, 102605. https://doi.org/10.1016/j.nicl.2021.102605 (2021).
Hulst, T. et al. Ageing shows a pattern of cerebellar degeneration analogous, but not equal, to that in patients suffering from cerebellar degenerative disease. Neuroimage 116, 196–206. https://doi.org/10.1016/j.neuroimage.2015.03.084 (2015).
Koppelmans, V. et al. Regional cerebellar volumetric correlates of manual motor and cognitive function. Brain Struct. Funct. 222, 1929–1944. https://doi.org/10.1007/s00429-016-1317-7 (2017).
Koziol, L. F. et al. Consensus paper: The Cerebellum’s role in movement and cognition. Cerebellum 13, 151–177. https://doi.org/10.1007/s12311-013-0511-x (2014).
Kutz, D. F., Schmid, B. C., Meindl, T., Timmann, D. & Kolb, F. P. Contribution of the cerebellum in cue-dependent force changes during an isometric precision grip task. Cerebellum 15, 439–450. https://doi.org/10.1007/s12311-015-0707-3 (2016).
Fröhlich, S., Kutz, D. F., Müller, K. & Voelcker-Rehage, C. Characteristics of resting state EEG power in 80+-year-olds of different cognitive status. Front. Aging Neurosci. 13, 689. https://doi.org/10.3389/fnagi.2021.675689 (2021).
Albert, M. S. et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: Recommendations from the National Institute on aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 7, 270–279. https://doi.org/10.1016/j.jalz.2011.03.008 (2011).
Petersen, R. C. et al. Mild cognitive impairment: A concept in evolution. J. Intern. Med. 275, 214–228. https://doi.org/10.1111/joim.12190 (2014).
Petersen, R. C. et al. Practice guideline update summary: Mild cognitive impairment. Rep. Guideline Dev. Dissem. Implement. Subcommit. Am. Acad. Neurol. 90, 126–135. https://doi.org/10.1212/wnl.0000000000004826 (2018).
Rudisch, J. et al. How age, cognitive function and gender affect bimanual force control. Front. Physiol. 11, 245. https://doi.org/10.3389/fphys.2020.00245 (2020).
Kutz, D. F., Fattori, P., Gamberini, M., Breveglieri, R. & Galletti, C. Early- and late-responding cells to saccadic eye movements in the cortical area V6A of macaque monkey. Exp. Brain Res. 149, 83–95. https://doi.org/10.1007/s00221-002-1337-9 (2003).
R: A Language and Environment for Statistical Computing (R Foundation for Statistical Computing, 2020).
Acknowledgements
The authors would like to thank all the participants for their contribution. Further thanks go to Dr. Brennecka from the Scientific Editorial Service of the University of Münster for proofreading the manuscript.
Funding
Open Access funding enabled and organized by Projekt DEAL. This work was supported by the European Social Fund for Germany, the Sächsische Aufbaubank-Förderbank (SAB) of the Free State of Saxony (Grant No. 100310502), and Deutsche Forschungsgemeinschaft (DFG, German Research Foundation) under DFG Project-ID 416228727- SFB 1410. This funding source had no role in the study design, in the collection, analysis, and interpretation of data, or in the writing of the report.
Author information
Authors and Affiliations
Contributions
S.F.: data collection; K.M.: project administration; J.R.: data revision, conceptualization of analysis; C.V.-R.: project conceptualization and administration, funding acquisition; S.F., K.M., J.R., C.V.-R. and D.F.K.: writing, review and editing; D.F.K., conceptualization, performance of the analysis, and writing of the first version of the manuscript. All authors contributed to manuscript revision and read and approved the submitted version. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kutz, D.F., Fröhlich, S., Rudisch, J. et al. Sex-dependent performance differences in curvilinear aiming arm movements in octogenarians. Sci Rep 13, 9777 (2023). https://doi.org/10.1038/s41598-023-36889-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-36889-5
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
