
Abstract
Challenges in social communication is one of the core symptom domains in autism spectrum disorder (ASD). Novel therapies are under development to help individuals with these challenges, however the ability to show a benefit is dependent on a sensitive and reliable measure of treatment effect. Currently, measuring these deficits requires the use of time-consuming and subjective techniques. Objective measures extracted from natural conversations could be more ecologically relevant, and administered more frequently—perhaps giving them added sensitivity to change. While several studies have used automated analysis methods to study autistic speech, they require manual transcriptions. In order to bypass this time-consuming process, an automated speaker diarization algorithm must first be applied. In this paper, we are testing whether a speaker diarization algorithm can be applied to natural conversations between autistic individuals and their conversational partner in a natural setting at home over the course of a clinical trial. We calculated the average duration that a participant would speak for within their turn. We found a significant correlation between this feature and the Vineland Adaptive Behaviour Scales (VABS) expressive communication score (r = 0.51, p = 7 × 10–5). Our results show that natural conversations can be used to obtain measures of talkativeness, and that this measure can be derived automatically, thus showing the promise of objectively evaluating communication challenges in ASD.
Similar content being viewed by others


Introduction
Autism Spectrum Disorder (ASD) is a neurodevelopmental condition characterised by persistent deficits in social communication and interaction, the presence of repetitive and stereotyped patterns of behaviour, and sensory atypicalities1. These symptoms can affect job independence and the ability to form friendships, thus negatively impacting a person’s quality of life2. Novel therapies are under development to treat such deficits in ASD (e.g. NCT03682978; NCT04299464), however the ability to show a response is dependent on a sensitive and reliable measure of treatment effect. Treatment effects are typically assessed using scales or questionnaires that measure core symptoms and adaptive functions, which can be reported either by a patient, caregiver or clinician (e.g. Vineland Adaptive Behaviour Scales [VABS]; Burger-Caplan et al.3; Autism Behavior Inventory [ABI]; Bangerter et al.4). However, these assessments are time-consuming to administer, introduce elements of subjectivity (i.e. they are susceptible to placebo effects and only reflect behaviours observed by the caregiver), do not provide real-time objective information on a person’s current clinical state (and change thereof), are only infrequently administered, and do not map onto likely biological mechanisms that underpin treatment response5,6,7,8. Therefore, there is a critical unmet need for developing reliable and objective clinical trial endpoints that measure social communication abilities in ASD in a remote setting.
Expressive Language Sampling (ELS) through structured conversations has emerged as a promising way to measure expressive communication abilities. ELS is typically performed in a clinical setting with a trained conversation partner or physician. Several studies have utilised automated linguistic and acoustic analysis methods to analyse conversational speech to produce objective measures of speech deficits, such as the mean length of utterance (MLU) in morphemes, the number of different word roots, communication-units (C-units) per minute, and the unintelligible proportion and repetition proportion9,10,11,12. However, these approaches still require manual transcripts by a trained professional. In addition, most of these analyses are performed on standard clinical assessments, which are performed infrequently and in a clinical setting. In order to track changes continuously over time, more frequent speech samples are required, and ideally in a natural environment such as the participant’s home12. Alternative machine learning approaches that are time- and cost-efficient, and capable of analysing feature-rich datasets, have yet to be developed and deployed successfully in the context of assessing speech in individuals with ASD.
As a first step, this requires parsing conversations into segments in which the participant or conversational partner is talking. This process is known as speaker diarization, and has been widely researched with applications in conversation segmentation during meetings, phone conversations, voice verification, speech recognition etc.13. Speaker diarization methods typically iterate through an audio recording via a sliding window, identify the speaker(s) in each segment, and aggregate segments based on whether the same or different speaker is present. The process results in hypothesised segments of varying lengths belonging to each speaker. With the advent of deep learning, speaker diarization has become more successful in recent years14, 15, in part due to extremely large and publicly available training data (e.g. VoxCeleb 16). However, while speaker diarization can automatically parse a conversation into a set of hypothesised speakers, it cannot know which one is the ASD participant, and which is the conversational partner. This requires the additional step of performing speaker identification, which compares the utterances from a diarized conversation with a known example of speech from the participant in question.
The motivation for this study was to assess whether or not it is possible to perform automatic speaker diarization on free-flowing conversations between an ASD participant and a conversation partner in a natural environment at home. To our knowledge, no such dataset has been collected before, and it was unknown whether an open-source pretrained speaker diarization algorithm would work in such a challenging environment. In addition, we hoped to find simple conversational features that could correlate with known clinical scales. Future work will require more advanced features using ASR and NLP to more accurately track any potential treatment effects over time, but this study has provided a proof-of-concept that such an approach could work in future clinical trials.
The goal of this study was to ascertain whether automatic speaker diarization algorithms could succeed in segmenting free-flowing conversations between ASD participants and a conversational partner in a natural environment at home. To do so, we recorded over 500 conversations from 54 ASD and 18 neuro-typical control (NTC) participants. The participants spanned in age from 5 to 45 years old. To automatically segment the conversations, we applied the open-source speaker diarization algorithm Pyannote17, 18. To validate its effectiveness, we manually diarized a subset of conversations. In addition to diarizing conversations, we assessed whether a simple conversation feature (the mean length of each utterance) would correlate with caregiver-reported expressive communication skills. If successful, this would lay the ground-work for future studies where more advanced methods could be applied such as automatic speech recognition (ASR) and natural language processing (NLP) to extract more complex and fine-grained conversational features that could better assess and track treatment effects over time.
Methods
Participant demographics
We obtained recordings from 54 ASD and 18 neurotypical control (NTC) participants, including children (5–12 years) adolescents (13–17 years), and adults (18–45 years) as part of an observational clinical trial (NCT03611075, 02/08/2018)19. We wanted a full span of ages to ensure that the diarization algorithm worked on children as well as adults, because most of the training data available for performing speaker diarization and speaker identification is from adult speech. The study was conducted according to the guidelines of the Declaration of Helsinki. The study has received all necessary Institutional Review Board (IRB) approvals. For the inclusion and exclusion criteria for the clinical trial, please see the Supplementary Information.
Each participant was required to have a single study partner with whom they would record their conversations. The study partners were either a staff member or family member of the participant, who must spend a few hours each day with the participant. For the inclusion criteria for the study partner, please see the Supplementary Information.
The ASD participants had their IQ measured according to the Abbreviated Battery IQ (ABIQ) of the Stanford–Binet intelligence scales fifth edition (SB5)20. This contains a verbal and non-verbal component, which provides an estimate of the full-scale IQ. ASD participants were subsequently placed into two categories, depending on whether their IQ was above or below 70.
While 135 participants were initially recruited into the trial, only 72 completed the conversation task at least once. See Table 1 for a break-down of the participant demographics, showing the sex of the participants (1st row: male/female), the total number of participants with recorded conversations in the study (2nd row), and the number of participants with hand-labelled recordings (3rd row). The number of conversations recorded for each cohort is displayed in brackets. Additional demographic information is shown in Supplementary Table 1.
Audio recordings
We recorded natural conversations between each participant and their study partner (Fig. 1A). The study partners were given 6 suggested topics: school, work, free-time, what they did today, dreams, and things they like or dislike. They were given no other instructions; therefore the conversations were free-flowing and unstructured in every other regard. While we did instruct them to take place in a quiet environment, they often included background noise from everyday living activities, as well as speech from other members of the household. They were instructed to be at least 5 min in length, but were often shorter in practice. We then restricted our analyses to those conversations lasting between 1 and 8 min (an empirical choice to reject accidental recordings). The audio was recorded using a smartphone with 2 microphones. The study partner was instructed to place 1 microphone facing themselves, and the other at the participant.

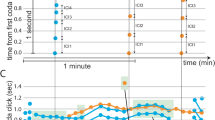
Task design, diarization methods, and feature extraction. Participants took part in (A) a conversation with a study partner, and (B) a Describe the Picture (DtP) task. (C) Conversations were automatically diarized into a hypothesised number of unknown speakers. (D) DtP audio was manually segmented to extract participant speech only. (E,F) The audio for each hypothesised speaker, and for the participant’s speech, were converted into fixed 192 dimensional embeddings. (G) The distances between the speaker embeddings and the participant’s embedding were measured using the cosine distance. (H) Speakers who’s distance was less than a predefined threshold (0.75: Spk1/Spk3 in this example) were assigned to be the participant. (I) The duration of each utterance was measured, and their basic statistics were calculated.
In addition, we recorded a separate task in which the participants were asked to describe the contents of a picture, which we will refer to as the Describe the Picture (DtP) task (Fig. 1B). While this task was designed to obtain different measures of ASD symptoms, it was also useful to use as an independent data set with which to obtain audio samples of the participant’s voice exclusively, so that their voice could be compared with the detected speakers in the conversation task. However, due to the presence of speech from their study partner, as well as other background talkers, we manually listened to this audio and extracted segments of the participant’s speech. We obtained between ~ 30 and 60 s of participant specific speech, depending on the amount available.
17 participants did not record any DtP audio. For these participants, we manually extracted their voice segments from a single conversation. We will refer to the audio from the DtP task (or the single conversation for those participants without DtP audio) as the Speaker ID audio.
Speaker diarization and feature extraction
Our speaker diarization pipeline consisted of 6 steps (Fig. 1C–I):
-
1.
We used the open-source speaker diarization package pyannote17 version 218 to automatically segment each conversation into hypothesised utterances from individual speakers (Fig. 1C). The default parameter settings were used. Given that the audio recordings were obtained in a real-world environment with potentially multiple background talkers, we did not constrain the diarization algorithm to a fixed number of speakers; instead, we allowed the algorithm to automatically estimate that number.
-
2.
We manually extracted segments of the participant’s speech from the DtP audio recordings (Fig. 1D), or from a single conversation when no DtP audio was available (which was the case for 17 participants).
-
3.
We calculated a speaker embedding for the Speaker ID audio (Fig. 1F) using the pretrained model on the hugging face platform21. This embedding is a fixed length 192 dimensional vector that represents any variable length speech utterance. We will refer to this embedding as the Speaker ID embedding. The model is based on the canonical x-vector time delay neural network (TDNN)-based architecture14, but with filter banks replaced with trainable SincNet features22.
-
4.
By having an unconstrained number of speakers automatically detected, it’s possible that the participant’s speech could be mislabeled as 2 (or more) different speakers. To remedy this, we concatenated the audio for each hypothesised speaker together, and calculated their speaker embedding, to obtain a single embedding for each hypothesised speaker (Fig. 1E).
-
5.
We compared the embeddings of the hypothesised speakers with the Speaker ID embedding (from step 3) using the cosine distance. The embeddings with a distance less than a particular threshold were assigned to be the participant (Fig. 1G,H). A threshold value of 0.75 was selected as the lowest threshold which also ensured that every participant had at least 1 conversation that was diarizable (see Supplementary Table 2). Participants can have conversations that are undiarizable if the distance between the embedding of their speaker ID audio and the embeddings of the utterances during the conversation never go below the threshold.
-
6.
Finally, we measured the duration of each utterance belonging to the participant, and calculated their basic statistics: mean, min, max, etc. See Supplementary Table 3 for a full list.
Diarization performance measurement
To test the performance of our diarization pipeline, we hand-labelled 51 conversations from 35 participants. Hand labelling consisted of listening to the conversations and labelling those segments in which either the study partner or participant was talking, or in which other environmental sounds/background talkers were occurring. We measured our ability to identify the participants speech using precision, recall, and the F1-score, which provide a percentage accuracy at identifying a target using a combination of true positives (TP), false positives (FP), and false negatives (FN):
Intuitively, each of these measures can be interpreted as the following:
-
Precision is a measure of how accurate the model is at correctly predicting the presence of participant speech, regardless of failed detections. For example, even if the model only predicts one instance of participant speech, and misses every other instance, as long as that single instance is correct, the ‘precision’ will be 100%.
-
Recall is the opposite. It’s a measure of how accurate the model is at consistently predicting the presence of participant speech, regardless of false-positives. For example, the model could just predict that every speech utterance belongs to the participant, and this would result in a ‘recall’ score of 100%.
-
The F1 score is the harmonic mean of precision and recall. The term ‘harmonic’ in this case means that it is never greater than the arithmetic mean of precision and recall, but is often smaller (i.e. the F1 score is weighted toward the smaller of precision and recall). In fact, it is equal to the arithmetic mean only when precision = recall.
Conversation features
From the diarization output we can extract a measure of talkativeness which is a relevant aspect of expressive communication in ASD23, 24. Therefore, for each conversation, we extracted the duration of each utterance for the participant (segments of speech flanked by either non-speech or speech from another talker). We will refer to this as the Utterance Duration (UD) feature. From this, we calculated basic statistics such as the mean, standard deviation, median, max, etc. (see Supplementary Table 3 for a full list) to obtain a fixed set of features for each conversation. Finally, for each statistic, we took the average across all conversations to obtain a single value per participant. We found that the majority of these statistics provided similar results (Supplementary Table 3), so for the remainder of this paper we will use the mean UD as our feature of interest. In addition, we found no relationship between the length of a conversation, and the mean UD feature (Supplementary Fig. 5).
The phone used for recording the conversations had 2 microphones. The above steps were done separately for both, and then all subsequent results are taken as the average of both microphones, i.e., the features were calculated for the 2 microphones separately, and then averaged together. We did not average together correlation values or statistical results.
Vineland adaptive behaviour scales
The Vineland Adaptive Behaviour Scales (VABS3, 25) are commonly used for assessing various adaptive behaviours in ASD. The VABS-II interview was completed for each ASD participant in this study. All necessary permissions were obtained from Pearson Publishing to administer the questionnaire and report on the results. The communication portion of the VABS contains the subdomains of expressive and receptive communication. Expressive communication refers to the ability to express wants and needs through verbal and nonverbal communication. It is the ability to put thoughts into words and sentences in a way that makes sense and is grammatically correct. Receptive communication refers to the ability to understand and comprehend spoken language that is heard or read. Therefore, since we are using the mean UD as a conversation feature in our study, we are primarily interested in expressive communication, and will report results with regards to this clinical scale (although see Supplementary Fig. 1, Supplementary Table 3). In order to account for age differences, we used the v-scale values as opposed to the raw scores25. The VABS was administered at the start of the study, and 3 months later at the end. To get the most representative estimate of their communication abilities during this period, we took the average of their 2 scores. 4 participants only completed one assessment, so we used their single score.
Statistical analysis
All statistical analyses on group differences were performed using 2-sided Mann–Whitney U (MWU) tests. One-sample comparisons were performed using Wilcoxon Signed-Rank (WSR) tests. All correlations were calculated using Pearson’s correlation. The intraclass correlation coefficients are two-way random, single measures, absolute agreement: ICC(2,1).
Institutional review board statement
Informed consent was obtained from all subjects and/or their legal guardian(s) (incase of minors). The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by Advarra IRB (Pro00035060, May 2018), BRANY IRB (#18-10-193-01, August 2018), Nathan Kline Institute for Psychiatric Research/Rockland Psychiatric Center IRB (1218792-12, August 2018), the Holland Bloorview Research Ethics Board (18-800, November 2018), the Wales Research Ethics Committee 5 Bangor (251572, September 2018), and the Western Institutional Review Board (20191384, August 2019).
Results
Diarization performance
Figure 2 shows the performance of the diarization algorithm (precision, recall, and F1 score) at identifying the participants from the conversation recordings, split into the different cohorts (ASD [IQ < 70 and IQ > 70] and NTC). The precision and F1 scores were lower for IQ < 70 compared with IQ > 70 ASD participants (MWU: p = 0.05 and 0.02, respectively), but not compared with NTC participants (p > 0.05). However, no significant differences remained after correcting for multiple comparisons (Bonferroni-Holm, alpha = 0.05). There were also no significant differences in recall for any cohort. The median performance across all cohorts was 76.5%, 80% and 76.5% for precision, recall and F1 Score, respectively.

Diarization performance. The accuracy at identifying the participant from the conversation recordings using 3 different metrics: precision (A), recall (B) and F1 Score (C; see “Methods” section). Each dot is a participant (35 participants from 51 conversations). ASD = autism spectrum disorder, NTC = neurotypical control. Statistics are calculated using a 2-sided Mann–Whitney U test.
Correlation between true and predicted conversation features
Figure 3A shows a scatter plot and correlation between the true and predicted mean UD conversation feature (r = 0.81, p = 3 × 10–9). Figure 3B shows a boxplot illustrating the difference between the true and predicted mean UD for each cohort. There was no significant difference between the different cohorts (MWU: p > 0.05). The ASD (IQ < 70) cohort was significantly greater than zero (WSR: p = 0.02).

Mean utterance duration (UD)—comparison of true and predicted labels. (A) Pearson’s correlation between the true and predicted (x and y-axes, respectively; both on logarithmic axes) mean UDs. (B) The difference (y-axis) between the true and predicted mean UD for each cohort (x-axis). The ASD (IQ < 70) cohort was significantly greater than zero (Wilcoxon Signed-Rank test: p = 0.02). Each dot is a participant (35 participants from 51 conversations). ASD autism spectrum disorder, NTC neurotypical control.
Comparing ASD and NTC conversation features
Having validated that our speaker diarization method could identify the participants from the hand-labelled conversations (35 participants from 51 conversations) and predict the mean UD conversation feature, we then extended our analyses to the full dataset of participants (72 participants from 652 conversations). We then compared the conversation features between each cohort, after calculating the mean value for each participant. Figure 4 shows a boxplot illustrating the differences in the mean UD between the cohorts, when using the true labels (A; 35 participants from 51 conversations) and the predicted labels (B; 72 participants from 652 conversations). Note that due to the different number of conversations used to calculate the mean value for each participant, the values reported in A and B are not directly comparable. In both cases, ASD (IQ < 70) participants had significantly shorter Mean Response Durations than ASD (IQ > 70) and NTC participants (p < 0.05). There were no significant differences between ASD (IQ > 70) and NTC participants.

Mean utterance duration (UD)—cohort comparison. The mean UD (y-axis; logarithmic scale) for each cohort (x-axis) for the true labels (A; 35 participants from 51 conversations) and predicted labels (B; 72 participants from 652 conversations). ASD autism spectrum disorder, NTC neurotypical control.
After correcting for multiple comparisons (Bonferoni-Holm; n = 3, alpha = 0.05), there was no longer a significant difference between the ASD (IQ < 70) and NTC cohorts for the Predicted Labels (p-corrected = 0.07).
Correlation with VABS communication scores
While categorising ASD participants based on their IQ gives an indication of communication challenges, the VABS expressive communication (EC) score gives a more appropriate clinical measure of communication abilities. Figure 5 shows a scatter plot between the mean UD (x-axis; logarithmic scale) and the VABS EC score (y-axis) for the True labels (A) and the Predicted labels (B). In both cases, there was a significant correlation (r = 0.5, p = 0.007, and r = 0.51, p = 7 × 10–5, respectively).
Given how we observed a significant difference in mean UD between the ASD (IQ < 70) and ASD (IQ > 70) groups (Fig. 4), we wondered if it was primarily IQ that was driving the correlations with the VABS EC score. Indeed, IQ and VABS EC are correlated with each other (r = 0.39, p = 0.004). To take into account this possibility, we performed a partial correlation between the mean UD and the VABS EC score, using the IQ as a covariate. Doing so still resulted in a significant correlation (r = 0.43, CI 95% [0.18, 0.63], p = 0.001).
We also calculated the correlations for each age group separately for the predicted mean UD feature (Supplementary Fig. 4). In spite of the smaller sample sizes, we still found significant correlations for the children (Pearson’s r = 0.44, p = 0.04) and adult groups (r = 0.68, p = 0.002), and a trend towards a significant correlation for the Adolescent group (r = 0.44, p = 0.09).
Test–retest reliability
We calculated the intraclass correlation coefficient (ICC(2,1); two-way random, single measures, absolute agreement) of the predicted mean UD feature to measure its consistency across conversations (r = 0.46). Due to the fact that we only had ~ 1 conversation with hand-labels per participant, we could not calculate an ICC value for the true labels.
Discussion
Using an automatic speaker diarization algorithm, we were able to use natural conversations to identify ASD participants as they conversed with a study partner (Fig. 2). The algorithm could quite accurately capture a conversation feature related to talkativeness, which we refer to as the mean Utterance Duration (UD): the average length of time (in seconds) that a participant would speak for within their turn (Fig. 3). This feature was significantly different between ASD participants with an IQ < 70 and those with an IQ > 70 (Fig. 4), but not between the ASD (IQ > 70) and NTC groups. Finally we found that the mean UD feature exhibited a significant correlation with a clinical measure of communication deficits in ASD: the Vineland Adaptive Behaviour Scales (VABS) expressive communication subdomain score (Fig. 5).

Mean utterance duration (UD)—comparison with VABS. The correlation (Pearson’s r) between the mean UD (x-axis; logarithmic scale) and the VABS expressive communication score (y-axis) for the true labels (A; 28 participants from 42 conversations) and predicted labels (B; 54 participants from 499 conversations). Each dot represents an ASD participant.
Our mean UD feature should be distinguished from the Mean Length of Utterance (MLU) feature that is commonly used in ASD research23. The MLU is the average number of morphemes per utterance. Another measure of talkativeness explored in ASD research calculates the number of ‘Communication-units’ or ‘C-units’ per minute26, which requires knowledge of sentential and phrasal structure9, 24. Both the MLU and C-unit features require manual transcripts in order to be calculated; our mean UD feature is therefore rather simple by comparison, as it only requires the temporal labels from the diarization. They are also technically independent of the duration of the utterance in seconds, but are likely to correlate strongly with it. Further research combining manual transcripts with diarization will be required in order to do a direct comparison.
While the diarization algorithm can automatically segment a conversation into different talkers, identifying the participant’s voice requires the additional manual step of listening to and extracting examples of the participant’s voice from separate recordings. This is necessary because the diarization algorithm can’t know apriori who the participant is. While this means that the analysis can’t be fully automated, it ensures that only a minimal amount of manual labour is required, as only a minute or so of participant speech is required in order to diarize an unlimited amount of conversations. One potential method to automate this step would be for a clinician to record audio of the participant in a controlled environment. Whether or not this would work in practice, and would be cheaper/quicker than manually listening to and diarizing a short amount of audio, remains to be seen. However, recording examples of participant speech at an in-clinic setting would alleviate any privacy concerns of listening to conversations recorded at home.
In order to identify the participant’s voice from the number of hypothesised speakers from the diarization algorithm, we compared the distance of their embedding vectors using the cosine distance. We selected a fixed threshold, which was the lowest value at which every participant had at least one conversation that was diarizable (Supplementary Table 1). However, selecting a fixed threshold is probably not optimal given the heterogeneity of our data (different recording environments, different sexes/ages of the participants and their study partners, and different clinical diagnoses). One possibility is to manually diarize (at least) one conversation per participant, and then choose the threshold to optimise the differentiation between the two talkers. Alternatively one could train a model to optimally differentiate between the two predefined speakers, given that their speech would be known apriori. In addition, the speaker ID network22 could be fine tuned by incorporating ASD speech into its training data.
Despite having 2 microphones on our recording device, we only performed single-channel speaker diarization, and then averaged the results from the 2 microphones. The study partner was instructed to place 1 microphone facing themselves, and the other at the participant, however it was not possible to confirm if this was carried out. Future work could use more sophisticated diarization algorithms that incorporate both channels in the model training, thus resulting in an optimised dual-channel speaker diarization system27, 28.
The expressive communication survey measures a wide variety of communication abilities, including non-verbal communication, so we are unlikely to fully capture this clinical measure using a simple conversation feature such as the mean UD24. In addition, the VABS questionnaire suffers from placebo effects due to its subjective nature8. In future, we will look at additional low-level conversation features such as pitch variation, prosody, speech duration, speech rate, pauses, and turn-taking rate29, as well as high-level features extracted using automatic speech recognition (ASR) such as self-repetition or repeating the study partner (echolalia30), and restricted interests31. This would also help to explain the lack of any difference in mean UD between the ASD (IQ > 70) and NTC groups (Fig. 4); this is probably because the mean UD feature is too simple to detect any differences, with more complex features from ASR being required instead.
It should be noted that there are several limitations with regards to assessing ASD symptoms by recording natural conversations at home. For example, using untrained conversational partners, each with their own unique communication abilities and motivational levels, will undoubtedly have an impact on the conversational style and talkativeness of the participant in question. In addition, environmental noise and background talkers can be distracting when trying to have a conversation, and could lead to reduced social interaction. Future studies will need to carefully consider the effects that these issues may have when assessing any potential drug effects.
The ASD (IQ < 70) cohort had the poorest diarization performance, particularly with regards to precision (Fig. 2). Low precision means that the algorithm would often mistake the study partner speech for participant speech. This led to an overestimation of the UD feature for these participants (Fig. 3). However, this overestimation was not drastic enough to radically alter their resulting features, meaning that we still observed shorter UDs for these participants. One possible explanation for this discrepancy would be that the study partner’s speech mirrored the participant’s speech. Indeed, when comparing the UD features for the 2 groups, we found a small correlation (r = 0.28, p = 0.09, absolute difference = 0.33 ± 1.7 s; Supplementary Fig. 2). In addition, we found a correlation between the study partner’s mean UD feature and the VABS expressive communication score (r = 0.37, p = 0.06; Supplementary Fig. 3). Indeed, prior research has suggested that speech and language features produced by conversational partners can be used to predict an autism diagnosis32, 33. In contrast, ASD participants tend not to adapt their talkativeness based on their partner’s behaviour34. Together, these data suggest that low diarization precision does not necessarily lead to a poor estimation of the UD of a participant. In spite of the mean UD feature being relatively unaffected by poor precision, other higher-level features obtained using automatic speech recognition would be strongly affected.To remedy this, future work will require hand-labelling dozens of conversations with ASD participants in order to fine-tune the diarization algorithm. It should also be noted that the results of our study may not be generalizable to other neurodevelopmental disabilities (e.g., Down syndrome). Further research would be needed to evaluate the efficacy of our algorithm in such contexts. However, the field of automatic speaker diarization is still evolving, and future research may develop more effective and robust algorithms for a wider range of populations and contexts.
Data availability
Anonymized features are available upon reasonable request. Please contact Florian Lipsmeier: florian.lipsmeier@roche.com.
References
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders 5th edn, 2022 (American Psychiatric Association, 2022).
Friedman, L., Sterling, A., DaWalt, L. S. & Mailick, M. R. Conversational language is a predictor of vocational independence and friendships in adults with ASD. J. Autism Dev. Disord. 49, 4294–4305 (2019).
Burger-Caplan, R., Saulnier, C. A. & Sparrow, S. S. Vineland adaptive behavior scales. In Encyclopedia of Clinical Neuropsychology (eds Kreutzer, J. S. et al.) 3597–3601 (Springer, 2018).
Bangerter, A. et al. Autism behavior inventory: A novel tool for assessing core and associated symptoms of autism spectrum disorder. J. Child Adolesc. Psychopharmacol. 27, 814–822 (2017).
Siafis, S. et al. Placebo response in pharmacological and dietary supplement trials of autism spectrum disorder (ASD): Systematic review and meta-regression analysis. Mol. Autism 11, 1–19 (2020).
Jeste, S. S. & Geschwind, D. H. Clinical trials for neurodevelopmental disorders: At a therapeutic frontier. Sci. Transl. Med. 8, 321 (2016).
Abbeduto, L., McDuffie, A., Thurman, A. J. & Kover, S. T. Language development in individuals with intellectual and developmental disabilities: From phenotypes to treatments. Int. Rev. Res. Dev. Disabil. 50, 71–118 (2016).
Anagnostou, E. et al. Measuring social communication behaviors as a treatment endpoint in individuals with autism spectrum disorder. Autism 19, 622–636 (2015).
Salem, A. C. et al. Evaluating atypical language in autism using automated language measures. Sci. Rep. 11, 10968 (2021).
MacFarlane, H. et al. Quantitative analysis of disfluency in children with autism spectrum disorder or language impairment. PLoS ONE 12, e0173936 (2017).
van Santen, J. P. H., Sproat, R. W. & Hill, A. P. Quantifying repetitive speech in autism spectrum disorders and language impairment. Autism Res. 6, 372–383 (2013).
Cho, S. et al. Automatic detection of autism spectrum disorder in children using acoustic and text features from brief natural conversations. In Interspeech 2019 2513–2517. https://doi.org/10.21437/Interspeech.2019-1452 (ISCA, 2019).
Moattar, M. H. & Homayounpour, M. M. A review on speaker diarization systems and approaches. Speech Commun. 54, 1065–1103 (2012).
Snyder, D. et al. Speaker recognition for multi-speaker conversations using x-vectors. In 2019 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP) 5796–5800 (IEEE, 2019).
Park, T. J. et al. A review of speaker diarization: Recent advances with deep learning. Comput. Speech Lang. 72, 101317 (2022).
Nagrani, A., Chung, J. S. & Zisserman, A. Voxceleb: A large-scale speaker identification dataset. Preprint at http://arXiv.org/170608612 (2017).
Bredin, H. et al. Pyannote. audio: Neural building blocks for speaker diarization. In 2020 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP) 7124–7128 (IEEE, 2020).
Bredin, H. & Laurent, A. End-to-end speaker segmentation for overlap-aware resegmentation. In Interspeech 2021 (2021).
Roid, G. H. Stanford-Binet Intelligence Scales-Fifth Edition (Riverside Publ, 2003).
Ravanelli, M. & Bengio, Y. Speaker recognition from raw waveform with sincnet. In 2018 IEEE Spoken Language Technology Workshop (SLT) 1021–1028 (2018). https://doi.org/10.1109/SLT.2018.8639585.
Gabig, C. S. Mean length of utterance (MLU). In Encyclopedia of Autism Spectrum Disorders (ed. Volkmar, F. R.) 1813–1814 (Springer, 2013).
Abbeduto, L. et al. Expressive language sampling as a source of outcome measures for treatment studies in fragile X syndrome: Feasibility, practice effects, test–retest reliability, and construct validity. J. Neurodev. Disord. 12, 1–23 (2020).
Sparrow, S. S. Vineland adaptive behavior scales. In Encyclopedia of Clinical Neuropsychology (eds Kreutzer, J. S. et al.) 2618–2621 (Springer, 2011).
Loban, W. Language development: Kindergarten through grade twelve. NCTE Committee on Research Report No. 18 (1976).
Horiguchi, S., Takashima, Y., Garcia, P., Watanabe, S. & Kawaguchi, Y. Multi-channel end-to-end neural diarization with distributed microphones. Preprint at https://doi.org/10.48550/arXiv.2110.04694 (2022).
Wang, D., Chen, Z. & Yoshioka, T. Neural speech separation using spatially distributed microphones. Preprint at https://doi.org/10.48550/arXiv.2004.13670 (2020).
Fusaroli, R., Lambrechts, A., Bang, D., Bowler, D. M. & Gaigg, S. B. Is voice a marker for Autism spectrum disorder? A systematic review and meta-analysis. Autism Res. 10, 384–407 (2017).
Neely, L., Gerow, S., Rispoli, M., Lang, R. & Pullen, N. Treatment of Echolalia in individuals with autism spectrum disorder: A systematic review. Rev. J. Autism Dev. Disord. 3, 82 (2016).
Spiker, M. A., Lin, C. E., Van Dyke, M. & Wood, J. J. Restricted interests and anxiety in children with autism. Autism 16, 306–320 (2012).
Bone, D. et al. The psychologist as an interlocutor in autism spectrum disorder assessment: Insights from a study of spontaneous prosody. J. Speech Lang. Hear. Res. 57, 1162–1177 (2014).
Gupta, R., Bone, D., Lee, S. & Narayanan, S. Analysis of engagement behavior in children during dyadic interactions using prosodic cues. Comput. Speech Lang. 37, 47–66 (2016).
Cola, M. et al. Conversational adaptation in children and teens with autism: Differences in talkativeness across contexts. Autism Res. 15, 1090–1108 (2022).
Acknowledgements
The authors gratefully acknowledge the individuals with ASD and their families. We also thank the input and support of Federico Bolognani, former employee of F. Hoffmann-La Roche Ltd. and the contribution of the Roche Digital Biomarker team in Pharma Research and Early Development Informatics, in particular Raphael Ullmann, Jan Beckmann, Emma Poon and Samuel Nova, for their various roles in app development, data collection during the clinical trial and input into data analysis.
Author information
Authors and Affiliations
Contributions
J.O.S. and G.B. performed the analyses with support from W.C., D.S., and N.M. J.O.S. wrote the manuscript with support from G.B., W.C., D.N., and F.L. C.C., J.H., F.L., and D.N., conceived the study and analysis plan. P.S., J.T., E.E., T.K., L.M., J.H., M.L., F.L., conceived and implemented the study. All authors discussed the results and contributed to the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing non-financial interests but the following competing financial interests: JOS, GB and JT are full-time contractors of F. Hoffmann-La Roche Ltd. WC, DS, PS, EE, TK, LM, ML, and FL are full-time employees of F. Hoffmann-La Roche Ltd. DN and JH are full-time employees and shareholders of F. Hoffmann-La Roche Ltd. CC is a full-time employee of Genentech, and a shareholder of F. Hoffmann-La Roche Ltd. NM does not possess any competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
O’Sullivan, J., Bogaarts, G., Schoenenberger, P. et al. Automatic speaker diarization for natural conversation analysis in autism clinical trials. Sci Rep 13, 10270 (2023). https://doi.org/10.1038/s41598-023-36701-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-36701-4
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
