
Abstract
The relationship between current dietary caffeine intake and severe headache or migraine is controversial. Therefore, we investigated the association between dietary caffeine intake and severe headaches or migraines among American adults. This cross-sectional study included 8993 adults (aged ≥ 20 years) with a dietary caffeine intake from the National Health and Nutrition Examination Surveys of America from 1999 to 2004. Covariates, including age, race/ethnicity, body mass index, poverty-income ratio, educational level, marital status, hypertension, cancer, energy intake, protein intake, calcium intake, magnesium intake, iron intake, sodium intake, alcohol status, smoking status, and triglycerides, were adjusted in multivariate logistic regression models. In US adults, after adjusting for potential confounders, a 100 mg/day increase in dietary caffeine intake was associated with a 5% increase in the prevalence of severe headache or migraine (odds ratio [OR] 1.05, 95% confidence interval [CI] 1.02–1.07). Further, the prevalence of severe headache or migraine was 42% higher with caffeine intake of ≥ 400 mg/day than with caffeine intake of ≥ 0 to < 40 mg/day (OR 1.42, 95% CI 1.16–1.75). Conclusively, dietary caffeine intake is positively associated with severe headaches or migraines in US adults.
Similar content being viewed by others


Introduction
Severe headache or migraine is a common neurological disorder that can seriously affect people's daily lives and heavily burden individuals and society1. Globally, severe headache or migraine ranks second among the causes of years lived with disability, with the greatest age-standardized prevalence in 1990 and 20172. It is three times more common in women than men, with a lifetime prevalence of 43% and 18%, respectively3. It remains a serious public health issue in the United States (US), with an age-adjusted prevalence of 15.9% across all adults in 20184. The financial strain of migraine is enormous; approximately 40% of US adults with migraine were unemployed in 2018, and a similar percentage were classified as poor or “near poor”5. Therefore, effective preventive measures and modifiable risk factors for severe headaches or migraines should be investigated.
Recent studies have shown that genetics, sleep, and diet are contributing factors to headaches6,7,8. Caffeine is an important area of concern in diet, and it occurs naturally in various foods, such as coffee beans, tea, kola nuts, mate leaves, and cocoa nuts9. Caffeine is an antagonist of adenosine, inhibiting the release of excitatory neurotransmitters, resulting in decreased cortical excitability10,11. Additionally, caffeine has psychostimulant effects via the modulation of dopaminergic neurons, and dopamine plays a role in the pathogenesis of migraine12,13. Headache attacks are related to changes in cerebral blood flow, and caffeine intake or withdrawal can change the speed of cerebral blood flow and aggravate headaches14,15, since it significantly affects the central nervous system16,17.
Previous studies have reported the wide use of caffeine for patients with headaches, either alone or in combination with other treatments18. The American Headache Society recommends over-the-counter (OTC) nonsteroidal anti-inflammatory drugs (NSAIDs) and combinations such as acetaminophen, aspirin, and caffeine as Level A recommendations for reducing migraine and other symptoms19. Derry et al. reported in a randomized double-blinded study that the addition of caffeine (≥ 100 mg) to standard doses of commonly used analgesics improved pain relief20; however, this finding varies among studies. Shirlow et al. conducted a study on Australians and reported that the proportion of participants with headaches increased significantly with average caffeine intake21. However, Boardman et al. found no clear relationship between caffeine intake and headache in a cross-sectional study in the United Kingdom (UK)22. In another study, Hoy et al. reported that caffeine preparations were effective and generally well tolerated in treating migraine and episodic tension-type headache (TTH) in adult patients enrolled in a randomized, multicenter, active-comparison study23. Most previous studies are based on surveys of small samples, and studies on adults are insufficient24,25,26,27. Therefore, it is necessary to further investigate the relationship between dietary caffeine and severe headaches or migraines and explore the underlying mechanisms. Ultimately, we used data from the National Health and Nutrition Examination Survey (NHANES) database to explore the association of dietary caffeine intake with severe headaches or migraine in adults.
Methods
Study design and participants
The data on study participants were obtained from the NHANES, a major program conducted by the Centers for Disease Control and Prevention (CDC) to assess the health and nutritional status of adults and children in the US28. The NHANES database contains demographic, dietary, examination, laboratory, and questionnaire data. Study protocols for NHANES were approved by the National Center for Health Statistics (NCHS) Ethics Review Board (Protocol #98-12, https://www.cdc.gov/nchs/nhanes/irba98.htm). All the participants signed the informed consent before participating in the study. This study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). All information from the NHANES program is available and free to the public; therefore, the agreement of the medical ethics committee board was not necessary.
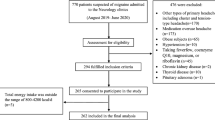
Participants in our study were screened according to the following inclusion criteria: (1) aged 20 years or above, (2) caffeine intake was obtained through at least one 24-h recall, and (3) information on whether they had severe headaches or migraines.
Assessment of severe headache or migraine
Severe headache or migraine was assessed using a questionnaire that consisted of one question: “During the past 3 months, did you have severe headaches or migraines?” Participants who answered yes were considered to have severe headaches or migraine, and participants who answered no were considered not to have severe headaches or migraine.
Assessment of dietary caffeine
Dietary caffeine intake was collected through two 24-h dietary recall interviews. The first 24-h dietary recall was conducted in person, and the second was conducted 3–10 days later via telephone. The in-person interview was conducted in a private room in the NHANES mobile examination centre using a computer-assisted dietary interview system, which an NHANES interviewer administered. The amount of caffeine consumed (mg/day) was estimated from all caffeine-containing foods and beverages, including coffee, tea, soda, and chocolate. The caffeine content of all foods consumed by participants was estimated using the United States Department of Agriculture’s Food and Nutrient Database. We obtained the daily caffeine intake based on the sum of the caffeine content of all foods consumed in a single 24-h dietary review. Detailed information on the assessment of caffeine intake can be found at: https://wwwn.cdc.gov/Nchs/Nhanes/1999-2000/DRXIFF.htm#DRXICAFF.
In this study, we extracted the mean caffeine intake between the first and second dietary recalls as participants’ dietary caffeine intake. For participants who only attended one 24-h dietary recall, caffeine intake was defined as the day's caffeine intake.
Assessment of covariates
Covariates in this study, including age, triglycerides (TG), energy intake, protein intake, calcium intake, magnesium intake, iron intake, and sodium intake, were used as continuous variables. Categorical variables included education level (< high school, completed high school, > high school), race/ethnicity (non-Hispanic white, non-Hispanic black, or others), and marital status (married/living with a partner or widowed/divorced/separated/never married). Poverty-income ratio (PIR) was defined as the ratio of family income to poverty threshold (< 1 indicating an income below the poverty threshold and ≥ 1 indicating an income above the poverty threshold; the latter category was further divided into two groups: 1.00 to < 2.00, ≥ 2.00). Body mass index (BMI) was measured as weight (kg) divided by height (m) squared (< 25.0 kg/m2 indicating normal, 25.0 to < 30.0 kg/m2 indicating overweight, ≥ 30.0 kg/m2 indicating obese). Smoking status (never smoking, < 100 cigarettes; former smoker, not currently smoking but ≥ 100 cigarettes consumed previously; current smoker, ≥ 100 cigarettes and currently smoking every day or some days). Alcohol status was determined by whether the participant had at least 12 alcoholic drinks per year (yes or no). Cancer was judged by answering the following question: “Have you ever been told by a doctor or other health professional that you had cancer or a malignancy of any kind?” (yes or no). Hypertension (defined as systolic blood pressure ≥ 140 mmHg or diastolic blood pressure ≥ 90 mmHg) was determined by either three blood pressure measurements at different times, an existing diagnosis, or evidence of an existing antihypertensive medication regimen.
Statistical analysis
The main concern was whether dietary caffeine intake was associated with severe headaches or migraine after adjusting for other factors that may influence severe headaches or migraines. Continuous variables are expressed as mean ± standard deviation, and categorical variables are expressed as percentages. The χ2 test was used to compare categorical variables between groups, a one-way analysis of variance was employed to compare normally distributed variables between groups, and the Kruskal–Wallis H test was utilized to compare variables with a skewed distribution between groups. Multivariable logistic regression analysis was performed to evaluate the independent association between dietary caffeine intake and severe headaches or migraine. Meet the methodological requirements. We used four levels of adjustment: Model 1 was adjusted for age and race/ethnicity; Model 2 was adjusted for the variables in Model 1 plus BMI, PIR, educational level, marital status, alcohol status, and smoking status; Model 3 was adjusted for the variables in Model 2 plus hypertension, cancer, and triglycerides; Model 4 was adjusted for the variables in Model 3 plus energy intake, protein intake, calcium intake, magnesium intake, iron intake, and sodium intake. Missing values were assigned as dummy variables and included in the regression equation; the missing values are presented in Table S1.
All analyses were performed using R (The R Foundation, Vienna, Austria) and Empower (X&Y Solutions, Boston, MA, USA). Statistical significance was defined as a two-sided P value of < 0.05.
Results
Participant characteristics
In this study, 8993 participants were included (Figure S1). Table 1 shows the characteristics of the participants according to their dietary caffeine intake. We grouped the participants according to their caffeine intake based on previous literature. Walter’s study defined 40–200 mg of caffeine per day as a "moderate" amount29. Further, Nawrot and van Dam RM research pointed out that more than 400 mg of caffeine daily is harmful to health30,31. Accordingly, we divided caffeine intake into four groups: ≥ 0 to < 40 mg/day, ≥ 40 to < 200 mg/day, ≥ 200 to < 400 mg/day, and ≥ 400 mg/day. Statistically significant differences were observed in age, educational level, race/ethnicity, marital status, PIR, BMI, smoking status, alcohol status, cancer, TG, energy intake, protein intake, calcium intake, magnesium intake, iron intake, and sodium intake in the different dietary caffeine intake groups (P < 0.05).
Participants with the lowest dietary caffeine intake in group 1 (≥ 0 to < 40 mg/day) were likely to be younger, non-Hispanic white, less educated, living alone, poorer, and underweight, with less smoking, less drinking, no cancer, no hypertension, lower TG, and lower energy, protein, calcium, magnesium, iron, and sodium intake.
Association between dietary caffeine intake and severe headache or migraine
We investigated the individual effects of each covariate on severe headaches or migraine using univariate analyses separately for the males and females in Table 2. In males, the incidence of severe headaches or migraines was likely to be with higher education, married/living with a partner, relatively wealthy, with greater BMI, drinking, hypertension, and cancer patients. Also, the higher incidence of severe headaches or migraines in females may be higher education, those who lived alone, were relatively wealthy, with less BMI, drinking, hypertension, and cancer patients.
The fully adjusted model observed a linear relationship between dietary caffeine intake and severe headaches or migraines in US adults (males and females) (Figure S2). A scatter plot of dietary caffeine intake and severe headaches or migraine is shown in Figure S3.
The results of the multivariate logistic regression analysis are shown in Table 3. After adjusting for confounders, a significant association between dietary caffeine intake and severe headaches or migraines was detected in Models 1–4. In Model 4, all variables were adjusted; for every 100 mg/day increase in dietary caffeine intake, severe headache or migraine incidence increased by 5% (OR 1.05, 95% CI 1.02–1.07, P < 0.001) in all adults. Notably, for every 100 mg/day increase in dietary caffeine intake, severe headache or migraine incidence increased by 5% (OR 1.05, 95% CI 1.01–1.08, P = 0.006) and 7% (OR 1.07, 95% CI 1.02–1.11, P = 0.002) in males and females, respectively.
Among the groups of dietary caffeine intake in Model 4 compared with participants in the first group of dietary caffeine intake (≥ 0 to < 40 mg/day), while the fourth group of dietary caffeine intake (≥ 400 mg/day) was associated with severe headaches or migraine (OR 1.42, 95% CI 1.16–1.75, P < 0.001). These relationships are also found in males and females.
The results of subgroup analyses by age, educational level, race/ethnicity, marital status, BMI, cancer, and energy intake are presented in Table S2. A significant interaction of dietary caffeine intake with age was found (P < 0.05).
Discussion
The results of this cross-sectional study of adult males in the US showed the association between dietary caffeine intake and severe headaches or migraine for the first time in a nationally representative sample. After adjusting for other variables, we found a linear relationship between dietary caffeine intake and severe headaches or migraines from 1999 to 2004. We also found that age modified the association.
The study investigated increased odds of severe headaches or migraine with increasing dietary caffeine intake in adults.
Our data were obtained from the NHANES database, which surveys a nationally representative sample of various health and nutrition measures covering diverse demographic characteristics such as multi-ethnicity28. Furthermore, the database is comprehensive, and its results are representative.
Caffeine is structurally similar to adenosine12, which plays important roles in regulating neurotransmitter release in the brain, movement, reward, sleep/wakefulness, cognition, and analgesia32. When caffeine binds to adenosine receptors on the cell surface, it acts as an adenosine receptor antagonist, which in turn induces cortical hyperexcitability and maintains arousal in the brain11,13. The main effect of caffeine in the neuroendocrine control system is the activation of distinct neuronal pathways by altering neurotransmitter release, which causes headaches and dependence33. Dehydration is also considered a possible contributor to migraine, and higher doses of caffeine can induce acute diuresis, which may subsequently lead to dehydration34,35. Chronic caffeine intake promotes a nociceptive state of cortical hyperexcitability and excitable neurons by antagonizing G protein-coupled purinergic (P1) receptors, which induces or exacerbates headaches14,36. In addition, chronic repetitive exposure to caffeine increases the risk of developing analgesic-overuse headaches, chronic daily headaches, and physical dependency37,38,39.
Age may affect the relationship between dietary caffeine intake and severe headaches or migraine; in the subgroup analysis, we found a stronger relationship in age < 60 years, and the interaction is significant among females. Hormones, such as menarche, oral contraceptive use, pregnancy, menopause, etc., greatly influence females’ migraines40, mainly involving young and middle-aged people ≥ 20 to < 60 years. Studies also have shown that caffeine intake affects the levels of luteal progesterone levels, luteal total, and free estradiol in premenopausal women; in postmenopausal females, no significant associations were detected with these hormones41, which may have implications for the relationship between dietary caffeine intake and severe headaches or migraine in adults non-elderly. However, its impact mechanism is still unclear, and it is necessary to conduct further studies to explore this conclusively.
This study had some limitations. First, this was a cross-sectional study; thus, we could not determine a causal relationship between dietary caffeine intake and severe headaches or migraine. Second, the data were obtained from questionnaires; therefore, there could be significant recall bias. Third, severe headache or migraine is based on self-reports and cannot be distinguished by type. Fourth, the caffeine intake calculated by food conversion may be inaccurate. However, the data used in this study came from the NHANES database, a research program designed to assess the health and nutritional status of adults and children in the US, and is intended to be accurate42. Fifth, the results may have been influenced by uncontrolled confounding, such as non-alcoholic fatty liver disease (NAFLD)43. Sixth, the data is nearly 20 years old at this point and may not be reflective of the current population, so our next study will include more recent data.
Conclusions
Our study showed that higher dietary caffeine intake is positively associated with a higher prevalence of severe headaches or migraines in US adults. However, further prospective studies are needed to clarify whether increased dietary caffeine intake increases the risk of severe headaches or migraine.
Data availability
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Change history
29 September 2023
A Correction to this paper has been published: https://doi.org/10.1038/s41598-023-43648-z
References
Blumenfeld, A. M. et al. Disability, HRQoL and resource use among chronic and episodic migraineurs: Results from the International Burden of Migraine Study (IBMS). Cephalalgia 31, 301–315 (2011).
WHO Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 392, 1789–1858 (2018).
Stewart, W., Wood, C., Reed, M., Roy, J. & Lipton, R. Cumulative lifetime migraine incidence in women and men. Cephalalgia 28, 1170-s1178 (2008).
Peters, G. L. Migraine overview and summary of current and emerging treatment options. Am. J. Manage. Care 25, S23–S34 (2019).
Burch, R., Rizzoli, P. & Loder, E. The prevalence and impact of migraine and severe headache in the United States: Updated age, sex, and socioeconomic-specific estimates from government health surveys. Headache 61, 60–68 (2021).
Charles, A. The pathophysiology of migraine: Implications for clinical management. Lancet Neurol. 17, 174–182 (2018).
Kim, S. J., Han, K. T., Jang, S. Y., Yoo, K. B. & Kim, S. J. The association between migraine and types of sleep disorder. Int. J. Environ. Res. Public Health 15, 2648 (2018).
RazeghiJahromi, S. et al. (EHF-SAS). Association of diet and headache. J. Headache Pain 20, 106 (2019).
Frary, C. D., Johnson, R. K. & Wang, M. Q. Food sources and intakes of caffeine in the diets of persons in the United States. J. Am. Diet. Assoc. 105, 110–113 (2005).
Ashihara, H., Sano, H. & Crozier, A. Caffeine and related purine alkaloids: Biosynthesis, catabolism, function and genetic engineering. Phytochemistry 69, 841–856 (2008).
Nestler, E., Hyman, E. & Malenka, R. Molecular Neuropharmacology: A Foundation for Clinical Neuroscience 2nd edn. (McGraw-Hill, 2008).
Ferre, S. et al. Adenosine A1–A2A receptor heteromers: New targets for caffeine in the brain. Front. Biosci. 13, 2391–2399 (2008).
Akerman, S. & Goadsby, P. J. Dopamine and migraine: Biology and clinical implications. Cephalalgia 27, 1308–1314 (2007).
Micieli, G. et al. Cerebral hemodynamics in primary headaches: The transcranial Doppler experience. Cephalalgia 18(Suppl 21), 17–22 (1998).
Sigmon, S. C., Herning, R. I., Better, W., Cadet, J. L. & Griffiths, R. R. Caffeine withdrawal, acute effects, tolerance, and absence of net beneficial effects of chronic administration: Cerebral blood flow velocity, quantitative EEG, and subjective effects. Psychopharmacol. (Berl.) 204, 573–585 (2009).
Iranpour, S. & Sabour, S. Inverse association between caffeine intake and depressive symptoms in US adults: Data from National Health and Nutrition Examination Survey (NHANES) 2005–2006. Psychiatry Res. 271, 732–739 (2019).
Dong, X., Li, S., Sun, J., Li, Y. & Zhang, D. Association of coffee, decaffeinated coffee and caffeine intake from coffee with cognitive performance in older adults: National Health and Nutrition Examination Survey (NHANES) 2011–2014. Nutrients 12, 840 (2020).
Lipton, R. B., Diener, H. C., Robbins, M. S., Garas, S. Y. & Patel, K. Caffeine in the management of patients with headache. J. Headache Pain 18, 107 (2017).
Ruoff, G. M. OTC analgesics vs opioids for pain management. J. Fam. Pract. 71, S29–S33 (2022).
Derry, C. J., Derry, S. & Moore, R. A. Caffeine as an analgesic adjuvant for acute pain in adults. Cochrane Database Syst. Rev. 2019, CD009281 (2014).
Shirlow, M. J. & Mathers, C. D. A study of caffeine consumption and symptoms; indigestion, palpitations, tremor, headache and insomnia. Int. J. Epidemiol. 14, 239–248 (1985).
Boardman, H. F., Thomas, E., Millson, D. S. & Croft, P. R. Psychological, sleep, lifestyle, and comorbid associations with headache. Headache 45, 657–669 (2005).
Hoy, S. M. & Scott, L. J. Indomethacin/prochlorperazine/caffeine: A review of its use in the acute treatment of migraine and in the treatment of episodic tension-type headache. CNS Drugs 25, 343–358 (2011).
Holle, D. & Obermann, M. Hypnic headache and caffeine. Expert Rev. Neurother. 12, 1125–1132 (2012).
Hering-Hanit, R. & Gadoth, N. Caffeine-induced headache in children and adolescents. Cephalalgia 23, 332–335 (2003).
Anderson, B. L., Juliano, L. M. & Schulkin, J. Caffeine’s implications for women’s health and survey of obstetrician-gynecologists’ caffeine knowledge and assessment practices. J. Womens Health (Larchmt) 18, 1457–1466 (2009).
Oberstar, J. V., Bernstein, G. A. & Thuras, P. D. Caffeine use and dependence in adolescents: One-year follow-up. J. Child Adolesc. Psychopharmacol. 12, 127–135 (2002).
Fain, J. A. Nhanes & Nhanes. Nhanes. Diabetes Educ. 43, 151 (2017).
Walter, K. Caffeine and health. JAMA 327, 693 (2022).
Nehlig, A. Effects of coffee/caffeine on brain health and disease: What should I tell my patients?. Pract. Neurol. 16, 89–95 (2016).
van Dam, R. M. et al. Coffee, caffeine, and health. N. Engl. J. Med. 383, 369–378 (2020).
Chen, J. F., Eltzschig, H. K. & Fredholm, B. B. Adenosine receptors as drug targets—what are the challenges?. Nat. Rev. Drug Discov. 12, 265–286 (2013).
Kirkland, A. E., Sarlo, G. L. & Holton, K. F. The role of magnesium in neurological disorders. Nutrients 10, 730 (2018).
Wöber, C. et al. Prospective analysis of factors related to migraine attacks: The PAMINA study. Cephalalgia 27, 304–314 (2007).
Seal, A. D. et al. Coffee with high but not low caffeine content augments fluid and electrolyte excretion at rest. Front. Nutr. 4, 40 (2017).
Alstadhaug, K. B. & Andreou, A. P. Caffeine and primary (migraine) headaches-friend or foe?. Front. Neurol. 10, 1275 (2019).
Feeney, R. Medication overuse headache due to butalbital, acetaminophen, and caffeine tablets. J. Pain Palliat. Care Pharmacother. 30, 148–149 (2016).
Scher, A. I. et al. Lipton RB: Caffeine as a risk factor for chronic daily headache. Neurology 63, 2022–2027 (2004).
Paluska, S. A. Caffeine and exercise. Curr. Sports Med. Rep. 2, 213–219 (2003).
Silberstein, S. D. Menstrual migraine. J. Womens Health Gend. Based Med. 8, 919–931 (1999).
Kotsopoulos, J. et al. Relationship between caffeine intake and plasma sex hormone concentrations in premenopausal and postmenopausal women. Cancer 115, 2765–2774 (2009).
Marriott, B. P. et al. Intake of added sugars and selected nutrients in the United States, National Health and Nutrition Examination Survey (NHANES) 2003–2006. Crit. Rev. Food Sci. Nutr. 50, 228–258 (2021).
Martins, I. Caffeine with Links to NAFLD and Accelerated Brain Aging (InTech, 2017).
Acknowledgements
We specifically thank Professor Yuanxiang Liu and Professor Jiguo Yang for their guidance and all the friends who helped.
Funding
This research was funded by Shandong Traditional Chinese Medicine Science and Technology. Development Project, Grant number 2019-0178.
Author information
Authors and Affiliations
Contributions
Conceptualization, L.Z., J.Y., J.L..; methodology, L.Z.; software, J.Y.; validation, H.S., Y.L. and J.Y.; formal analysis, L.Z., J.Y., and H.S.; investigation, L.Z.; resources, L.Z.; data curation, H.S.; writing—original draft preparation, L.Z.; writing—review and editing, Y.L. and J.Y.; visualization, J.Y.; supervision, Y.L. and J.Y.; project administration, L.Z. All authors have read and agreed to the published version of the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this Article was revised: In the original version of this Article Jinling Li was incorrectly affiliated with “The Second Clinical Medical College, Guangzhou University of Chinese Medicine, Guangzhou, China”. The correct affiliation is “College of Acupuncture and Massage, Shandong University of Traditional Chinese Medicine, Jinan, China.” Also, Haiyang Sun was incorrectly affiliated with “College of Acupuncture and Massage, Shandong University of Traditional Chinese Medicine, Jinan, China.” The correct affiliation is “The Second Clinical Medical College, Guangzhou University of Chinese Medicine, Guangzhou, China.”
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Zhang, L., Yin, J., Li, J. et al. Association between dietary caffeine intake and severe headache or migraine in US adults. Sci Rep 13, 10220 (2023). https://doi.org/10.1038/s41598-023-36325-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-36325-8
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
