
Abstract
Myocardial infarction (MI) affects many molecular pathways in heart cells, including the Ido1-KYN-Ahr axis. This pathway has recently been introduced as a valuable therapeutic target in infarction. We examined the effects of moderate-intensity continuous training (MICT) and high-intensity interval training (HIIT) on the axis in the heart tissue of male Wistar rats with occluded left anterior descending (OLAD). Thirty rats (age 10–12 weeks, mean weight 275 ± 25 g) were divided into five groups with 6 animals: Control (Ct) group, MICT group, rats with OLAD as MI group, rats with OLAD treated with MICT (MIMCT group) and rats with OLAD treated with HIIT (MIHIIT group). Rats performed the training protocols for 8 weeks, 5 days a week. HIIT included 7 sets of 4 min running with an intensity of 85–90% VO2max and 3 min of recovery activation between sets. MICT included continuous running at the same distance as HIIT with an intensity of 50–60% VO2max for 50 min. The expressions of Ahr, Cyp1a1, and Ido1 were assayed by real-time PCR. Malondialdehyde (MDA) and Kynurenine levels, and AHR, CYP1A1, and IDO1 proteins were detected using ELISA. Data were analyzed using the ANOVA and MANOVA tests. Compared to the CT group, MI caused an increase in all studied factors, but only statistically significant (P < 0.05) for MDA and IDO1. With a greater effect of HIIT, both protocols significantly lowered the proteins expressions in the MIHIIT and MIMCT groups, compared with the MI group (P < 0.001). In healthy rats, only AHR protein significantly decreased in the MICT group compared to the Ct group (P < 0.05). HIIT and MICT protocols significantly reduced the gene and protein expression of Cyp1a1 (P < 0.05) and Ido1 (P < 0.01), and HIIT had a greater effect. In conclusion, both protocols were effective at reducing the levels of Ido1-Kyn-Ahr axis components and oxidative stress in the infarcted heart tissue and HIIT had a higher significant effect.
Similar content being viewed by others


Introduction
Myocardial infarction (MI) as a type of ischemic cardiovascular disease promotes adverse remodeling of the left ventricle by affecting cardiomyocytes and vascular cells, which altogether develop the first cause of morbidity and mortality worldwide1. These cellular changes involve a wide range of molecular pathways including the Kynurenine (KYN) metabolism and Ido1-KYN-Ahr axis2. KYN is a metabolite produced from the amino acid tryptophan (TRP) by the activity of tryptophan 2,3-dioxygenase and indoleamine 2,3-dioxygenase 1 (IDO1) and 2 enzymes, which regulates various immune and physiological responses via binding to and activation of the aryl hydrocarbon receptor (AHR)3,4. AHR is a ligand-activated transcription factor with myriad functions in health and diseases, which works upon binding to many intrinsic and extrinsic chemicals in physiological and immune responses and Cyp1a1 upregulation is one of the main hallmarks of its activation5,6. Ahr knockout in a mouse model has been shown that it has highly crucial roles in maintaining the function, health, and physiological homeostasis of cardiac cells and tissues7. In MI, the Ido1-KYN-Ahr axis has paracrine effects on cardiomyocyte apoptosis and contractility and cardiac remodeling and function2. Furthermore, the levels of catabolites of this pathway in body fluids have been suggested as markers positively associated with MI and associated mortality2. KYN generation through IDO is markedly induced after MI and KYN metabolites may increase inflammation, oxidative stress, and apoptosis of smooth muscle cells and endothelial cells including cardiomyocytes8,9,10. It is shown that IDO1 activity has an inverse association with ischemic heart disease and therefore it has been introduced as a potential therapeutic target for this disease11.
Recently, it has been shown that exercise affects the Ido1-KYN-Ahr axis in different cells and tissues. Physical exercise has been shown to impact the KYN pathway (KP) in response to both acute and chronic exercise training stimuli and currently, it is accepted that exercise-induced KP may contribute to the prevention and treatment of chronic diseases12,13. Surprisingly, due to the effects of KP metabolites on skeletal muscle, adipose tissue, the immune system, and brain physiology, some researchers proposed that some of these metabolites could be suggested as exercise-induced myokines14. Also, other members of the Ido1-KYN-Ahr axis have been shown to interact with exercise metabolism. Pal et al., found that both acute and chronic endurance training may regulate NK cell function via the AHR/IDO axis15.
Increasing evidence confirmed exercise has improving effects on the cardiac function of MI patients16,17. All types of exercise can effectively inhibit skeletal muscle atrophy via reducing oxidative stress and protein degradation, increasing the antioxidant capacity, and regulating the growth factors expression18. However, there are different opinions about the impacts of exercise types on MI improvement. Cai et al. believe that in the early stages of MI, moderate-intensity exercise is the best choice to improve the outcomes for MI patients18. And Dun et al., reported that compared to moderate-intensity continuous training (MICT), supervised high-intensity interval training (HIIT) results in greater improvements in MI patients with metabolic syndrome16. Also, Moholdt et al. found that in MI patients aerobic interval training increases peak oxygen uptake more than usual exercise training19. Furthermore, different types of exercise affect KP in different ways. Joisten et al., reported that HIIT consistently led to greater effects than MICT on KP in persons with multiple sclerosis20. Currently, experimental studies aiming for a deeper understanding of cellular and molecular mechanisms underlying exercise interaction with the Ido1-KYN-Ahr axis in heart tissues of MI patients are still lacking. To fill some gaps in the current knowledge, here we conducted an in vivo investigation to compare the effects of MICT and HIIT on the axis in the heart tissue of rats with occlusion of the left anterior descending artery.
Material and methods
Experimental animals
Thirty male Wistar rats (age 10–12 weeks, mean weight 275 ± 25 g) were purchased from the Pasteur institute of Iran. Rats were kept in polycarbonate cages (Three rats per cage) on a 12 h light/dark cycle and a humidity of 65 ± 5% and a temperature of 25 °C and were provided food (rat chow) and water ad libitum. All experimental protocols were approved by the Committee on the Care of Laboratory Animal Resources, Semnan university of medical science (IR.SEMUMS.REC.1399.158) and were carried out following the Declaration of Helsinki, the ARRIVE guidelines and the Guide for the Care and Use of Laboratory Animals published by the US National Institutes of Health. Eighteen rats underwent surgery for occlusion of the left anterior descending (LAD). After evaluating and confirming MI using echocardiography, based on ejection fraction and fractional shortening the rats were divided into five groups including six members in each: Control group (Ct), a group treated with MICT, rats with occluded LAD (OLAD) as a model of MI, rats with OLAD and treated with MICT (MIMCT), and a group with OLAD and treated with HIIT (MIHIIT). Care of the animals was performed according to the European Convention for the Protection of Vertebrate Animals (ECPVA). The number of members in the groups was calculated following Charan and Biswas’s descriptions21.
Occlusions of left anterior descending
After anesthesia of the animal using a combination of ketamine and xylazine, the surgical site on the animal’s chest was disinfected with 70% alcohol. After keeping the animal fixed on the operating desk, using an otoscope number 3 and a green angiocatheter, the animal was intubated and connected to a ventilator (inter med Bear) (inhaul to exhalation ratio of 1 to 2 and 80–90 breaths per minute with a volume of 8 ml). In the space between the third and fourth ribs, the chest was cut to a length of 10 mm. With this incision, the LAD vessel was identified as a bright red pulsating spike that flows in the middle of the heart wall from under the left atrium to the apex of the heart. The LAD vessel was closed with the help of 0.6 mm polypropylene suture 1–2 mm below the level of the tip of the left atrium and was completely closed by tying two knots at this point. Left ventricular anterior wall infarction was confirmed by sudden myocardial coloration (discoloration). An increase in ST was also observed after ligation. Then, the chest, muscle layers, and skin were sewn in three layers using 0.5 proline suture and the animal's skin was sutured with 0.3 proline suture. When the rats regained consciousness, they were removed from the ventilator. After 48 h, the rats were anesthetized again and with echo vivid7 probe 10 s (MHz), an echo was performed to determine MI. In addition, cefazolin and tramadol as antibiotics and analgesics were injected twice a day, 1 day before surgery and 3 days after surgery. Rats in the MI group underwent all surgeries without occlusion of the left coronary artery. Also, Ct group rats did not receive any intervention and were kept only in the laboratory.
Exercise training
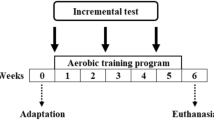
After evaluating and confirming MI and a week of rest MIHIIT, MICT, and MIMCT groups trained for three sessions per week for 2 weeks (each session 10–15 min at speed of 10 to 15 m per minute with a treadmill) to get acquainted with the training protocols. After 2 weeks of initial familiarization with the treadmill, the intensity of the training program was obtained in terms of VO2max and the relationship between VO2max and the speed and incline of the treadmill22. The aerobic capacity of the rats was evaluated after the initial warm-up. The test started with an initial speed of 6 m/min. The speed of the treadmill was increased every 2 min by 1.8–2 m/min until the rats reached the exhaustive stage. After obtaining the test speed and time, their average was calculated, and based on it, the protocol of training was designed. Then, the rats performed the two designed protocols of training based on previous reports22,23,24 for 8 weeks, 5 days a week with a slope of zero degrees (Table 1): (A) HIIT, which consisted of seven sets of four minutes running with the intensity of 85–90% VO2max and three minutes of recovery activation between sets with the intensity of 50–60% VO2max. (B) MICT, which consisted of continuous running in the same distance as HIIT with the intensity of 50–60% VO2max for 50 min. In both groups, warming and cooling down periods were performed for 5 min before and after the training with an intensity of 40% VO2max. The intensity.
Tissue sample preparation
Tissue resection was performed at the end of the eighth week and 72 h after the last training session. This was after performing anesthesia with CO2 gas and blood sampling from the heart. Then, heart tissue was extracted and after washing in physiological serum placed in microtubes and transferred to − 70 °C.
Determination of malondialdehyde and KYN
For quantitative assay of KYN and malondialdehyde (MDA) in the heart tissue lysate, Kynurenine ELISA Kit, ZellBio GmbH (Cat. No: ZB-11203C-R9648; Germany) and MDA Assay kit (CAT No. ZB-MDA-96A; Germany) were used following the manufacturer’s instruction.
Gene expression analysis
Total RNA was isolated from heart samples using TRIzol Reagent (Invitrogen, USA), treated with Dnase I, and quantified by NanoDrop (Thermo Fisher Scientific). RNA quality was determined by examining the 260/280 ratio > 1.8. A total of 1 µg RNA was then reverse transcribed to cDNA using the RevertAid First Strand cDNA Synthesis kit (Thermo Scientific) according to the manufacturer’s instructions. Expression of Ahr, Cyp1a1, and Ido1, was measured using specific primers produced by SinaColon, Iran (Table 2). Amplification was performed in ABI Prism 7500 sequence detection system; Life Technologies real-time RT-PCR device using the condition: initial denaturation (95 °C for 15 min for all genes); start of the cycle with denaturation (95 °C for 30 s for Gapdh, and 95 °C for 5 min for Ahr, Cyp1a1, and Ido1); annealing (55 °C for 30 s for Gapdh, 48 °C for 105 s for Ido1, 56 °C for 90 s for Cyp1a1and 60 °C for 90 s for Ahr); and extension (60 °C for 30 min for all genes). At the end of amplification cycles, reactions were given a final extension step at 60–95 °C. All data were analyzed with the ΔΔCt method and the expression of glyceraldehyde-3-phosphate dehydrogenase (Gapdh) was used as the internal standard.
Protein expression analysis by ELISA methods
ELISA kits ZellBio GmbH (Germany) were used for determining AHR (Cat. No: ZB-16349C-R), CYP1A1 (Cat. No: ZB-11059C-R9648), and IDO1 (Cat. No: ZB-10730C-R9648) levels in the heart tissue lysate following the manufacturer’s protocol.
Statistical analysis
For data analysis, we used multivariate analysis of variance (MANOVA), which was previously reported as an efficient test for assessing multiple dependent variables simultaneously25. Data are presented as means ± standard deviation in the text and tables. The Pearson and partial correlation coefficients were used to measure the relationship between MDA, KYN, and protein levels. A one-way MANOVA was first performed to determine the effect of the factor ‘group’ on the latent variable. Since the result of the multivariate analysis was significant, univariate analyses were done to discover the effect of a significant factor on each indicator variable (AHR, CYP1A1, IDO1, KYN, and MDA) of the latent variable, which was followed by the Tukey’s post hoc test. Assumptions of analysis of variance were verified with the Shapiro–Wilk test, Levene’s test, Doornik-Hansen test, Box's M-test, and evaluation of the homogeneity of covariance matrices. The results were considered significant with P ≤ 0.05. All statistical computations were done using Stata version 16 (College Station, TX: Stata Corp LLC; 2019) and GraphPad Prism version 9.0.0 for Windows, GraphPad Software, San Diego, California USA, www.graphpad.com.
Ethics approval
All experimental protocols were approved by the Regional Research Ethics Committee of Semnan University of Medical Sciences and Health Services (IR.SEMUMS.REC.1399.291) and were carried out following the Declaration of Helsinki, the ARRIVE guidelines and the Guide for the Care and Use of Laboratory Animals published by the US National Institutes of Health.
Informed consent
Informed consent was obtained from animal’s owner involved in the study.
Results
Effect of MI and exercise on components of Ido1-KYN-Ahr axis
The results in Fig. 1 depict that MI increased the level of KYN, but this increase was not statistically significant compared to the Ct group. Both training protocols significantly reduced the level of KYN in the heart tissues of rats with MI (P < 0.05) and the effect of HIIT was greater than MICT (Table 3B). Also, MICT significantly reduced KYN in healthy rats (P = 0.003), which in general shows that exercise reduces KYN in heart tissue (Fig. 1A). MI significantly increased the level of MDA in the heart tissue of rats with MI (P < 0.011) and both HIIT (P < 0.001) and MICT (P = 0.001) significantly reduced its level.

KYN (A), and MDA (B) levels in heart tissue of rats. MDA and KYN levels of the heart tissue were affected by the MI condition. Training had different effects on the treated groups. Abbreviations: Ct control group, MI the group with occlusion of the left coronary artery, MICT the group treated with moderate intensity of continuous training, MIMCT rats with left coronary artery occlusion treated with moderate intensity of continuous training, MIHIIT rats with left coronary artery occlusion treated with high-intensity interval training.
The results in Fig. 2, indicated that the MI increased the mRNA levels of Ahr, Ido1, and Cyp1a1 compared to the control group, but this increase was not statistically significant. Also, the changes in proteins level were not significant except for IDO1, and only levels of this protein significantly (P < 0.027) increased in the MI group in comparison to Ct rats (Fig. 2F). Both training protocols significantly reduced the levels of AHR, IDO, and CYP1A1 proteins in MIHIIT and MIMCT groups, compared with the MI group (P < 0.001), in which HIIT training had a greater effect than MICT. In healthy male rats, only protein expression of AHR significantly (P < 0.05) decreased in the MICT group compared to the control group (Fig. 2D). Both HIIT and MICT training protocols significantly reduced the Cyp1a1 and Ido1 expressions and CYP1A1 and IDO1 proteins levels in heart tissue, and a greater effect of HIIT was observed (Fig. 2B,C,E,F).

Ahr (A), Ido1 (B), and Cyp1a1 (C) gene expression, and AHR (D), IDO1 (E), and CYP1A1 (F) protein levels in the heart tissue of rats. Gene expressions and protein levels were increased in the MI condition and training showed decreasing effects in them. Abbreviations: Ct control group, MI the group with occlusion of the left coronary artery, MICT the group treated with moderate intensity of continuous training, MIMCT rats with left coronary artery occlusion treated with moderate intensity of continuous training, MIHIIT rats with left coronary artery occlusion treated with high-intensity interval training.
Effects of interventional factors on variables
Box’s M-test showed the observed covariance matrices of the dependent variables are equal across groups (P = 0.064). The significant effect of the group on the latent variables (AHR, CYP1A1, KYN, IDO1, and MDA simultaneously) was observed (Wilks’ λ = 0.027, Partial Eta Square = 0.60, P < 0.001). Considering the significant effect on the latent variable, individual univariate analysis was done and showed that there is a significant effect of group on variables as AHR (F5,42 = 10.32, P < 0.001), CYP1A1 (F5,42 = 37.71, P < 0.001), KYN (F5,42 = 10.36, P < 0.001), IDO1 (F5,42 = 13.52, P < 0.001) and MDA (F5,42 = 12.70, P < 0.001).
According to Table 3A, based on the r coefficient there was a highly positive significant correlation between the studied factors. Also, in the bivariate analysis, there was a moderate positive correlation between factors (based on the rp coefficient), however, it was significant just for some of them (Table 3A). The results of the Sidak post hoc test and pairwise comparison of groups are presented in Figs. 1 and 2.
Table 3B presented the parameter estimates of variables that the control group was considered as a reference and other groups were compared to it. This test showed that MI resulted in the elevation of all variables and HIIT and MICT significantly reduced these factors levels and only in the CYP1A1 variable, MICT couldn’t exert a significant effect. It seems that between the two types of exercise, HIIT had better performance (Table 3B).
Discussion
The evidence has confirmed that exercise training can improve cardiac function in heart diseases such as MI and improve the quality of life in patients. Although for the early exercise rehabilitation following MI, resistance training and MICT have been proposed as beneficial choices18 supervised HIIT was reported to result in greater improvements in MI patients16. A randomized controlled study found that aerobic interval training increases peak oxygen uptake more than usual exercise training in myocardial infarction patients19. It has been shown that aerobic exercise with moderate intensity could improve physical capacity and other cardiovascular variables26. However, HIIT has shown a relatively low rate of major adverse cardiovascular events for patients with coronary artery disease or heart failure when applied within cardiac rehabilitation settings17. Exercise intensity is an important factor for reversing left ventricular remodeling and improving aerobic capacity, endothelial function, and quality of life in patients with postinfarction heart failure27.
The results of the present study showed that both training protocols significantly reduced the level of KYN in the heart tissue of rats with MI, however, the effect of HIIT was greater than MICT (Fig. 1A). KYN is a new and valuable biomarker of chronic heart failure, with the ability to predict mortality and reflect exercise capacity28. Impairment of heart rhythm and observations of myocardial cell failure induced by KYN have been reported earlier and elevated plasma levels of KP metabolites and their ratios are associated with increased mortality, independent of coronary artery disease, in patients with heart failure10,29. Considering that KYN metabolites may increase inflammation, oxidative stress, and apoptosis of smooth muscle cells and endothelial cells it has been suggested that alterations of tryptophan metabolism might have an impact on the bioenergetic activities of heart mitochondria and might be involved in the development of clinical symptoms such as cardiomyopathy8,30,31. KYN generation through IDO is markedly induced after MI and genetic deletion or pharmacological inhibition of IDO limits cardiac injury and cardiac dysfunction after MI9, and here we showed that exercise reduces KYN levels in heart tissue significantly.
Exercise-induced KP modulates energy homeostasis and may contribute to the prevention and treatment of chronic diseases. Physical exercise has been shown to impact the KP in response to both acute and chronic exercise training stimuli12. Physical exercise can modulate KP metabolism in skeletal muscle and thus change the concentrations of select compounds in peripheral tissues and the central nervous system14. The effects of KP metabolites on skeletal muscle, adipose tissue, the immune system, and the brain suggest that some of these compounds could qualify as exercise-induced myokines14. Endurance exercise training can change KP metabolites by changing the levels of KP enzymes in skeletal muscle. This leads to a metabolite pattern that favors energy expenditure and an anti-inflammatory immune cell profile and reduces toxic metabolites32.
MI significantly increases MDA levels in heart tissue and here we showed that MICT and HIIT significantly reduced the levels (Fig. 1B). MDA is a known oxidative stress marker for coronary artery disease severity and plaque sensitivity33 and its reduction is considered to be an indicator of the healing of myocardial ischemia injuries34.
Also, the AHR pathway has been reported to exert cardioprotective effects against cardiotoxicity and produce heart-specific transcriptional responses35,36. KYN induces cardiomyocyte apoptosis through reactive oxygen species production in an AHR–dependent mechanism9. The expression level of circulating AHR may affect the susceptibility and progression of coronary arterial disease37 and it participates in myocardial ischemia–reperfusion injury by regulating mitochondrial apoptosis38. The results of the present study showed that OLAD resulted in an increase of Ahr gene expression in the heart tissue of rats with MI and MICT decreased it but none of these changes were statistically significant. However, at the protein level, both training protocols significantly reduced the level of AHR in the heart tissue of rats with OLAD. Additionally, even in healthy controls, MICT reduced the level of AHR protein in cardiac tissue. In general, both training protocols were able to reduce the AHR protein level in heart tissue. Previous studies have reported that in the myocardial ischemia model with OLAD, AHR is abundantly expressed in necrotic myocardium and it is shown that acute myocardial ischemia can activate AHR and induce inflammation39. Also, some animal studies reported a decrease in AHR after improvement of cardiac condition40. It seems that some AHR ligands, such as BaiCalin1, could reduce myocardial necrosis and inflammation by inhibiting the cardiac expression of AHR38,41. The heart and its vasculature system express all AHR-regulated genes and cardiac AHR-regulated CYPs are involved in the pathogenesis of cardiovascular diseases42. Increased gene expression of Cyp1a1 with MI was not statistically significant. However, in comparison to MICT HIIT reduces Cyp1a1 expression significantly. Regarding protein levels, both exercise protocols significantly reduce CYP1A1, although the effect of HIIT was greater (Fig. 2C,F). Parameter Estimation in Table 3 shows that among protein expressions HIIT had the greatest effect and only in CYP1A1, MICT training was most effective. It has been clearly shown that cardiac AHR-regulated CYPs are involved in the pathogenesis of cardiovascular diseases42.
In the present study, MI increased the level of Ido1 gene expression but it was not statistically significant. Both types of HIIT and MICT significantly reduced the Ido1 gene expression in heart tissue, however, HIIT had a greater effect and the same changes were observed for IDO1 protein levels (Fig. 2B and E). IDO1 and the IDO1-associated pathway constitute critical mediating agents associated with immunoinflammatory responses such as atherosclerosis in the heart tissue43. IDO1 promotes cardiomyocyte hypertrophy partially via PI3K-AKT-mTOR-S6K1 signaling44 and its suppression could potentially reduce the inflammatory response in cardiomyocyte injury45. IDO1 was inversely associated with ischemic heart disease with a directionally consistent estimate for stroke and might be a potential therapeutic target for this disease11. Based on the results in Table 3A, the protein expression of the studied variables is significantly correlated with each other. Also, it is shown that these variables are significantly related and affected by each other. A decrease in AHR led to a decrease in IDO1 and IDO1 had a significant relationship with KYN and CYP1A1 (Table 3A).
It is reported previously that HIIT was more effective than moderate-intensity training for improving oxygen pulse (O2P) slope in coronary heart disease patients, while ventilation and carbon dioxide production (VE/VCO2) slope and oxygen uptake efficiency slope were similarly improved by aerobic training regimens versus controls46. A systematic review and meta-analysis reported that HIIT is superior to MICT in improving cardiorespiratory fitness in participants of cardiac rehabilitation47. Our results are somehow consistent with the finding of these studies, however, there were some limitations. Measuring the slopes related to oxygen physiology, analyzing the activity of the enzymes involved in the oxidative/antioxidative system in heart tissue, assessing other components of the Ido1-Kyn-Ahr axis and immunohistochemical studies could add highly valuable data to future studies on this topic.
In conclusion, based on this study, it is possible to conclude that myocardial infarction alters the Ido1-Kyn-Ahr axis in heart tissue cells and imbalances it, as well as triggering oxidative stress. Both high-intensity interval training and moderate-intensity continuous training were effective at reducing the levels of the axis components and HIIT had a more significant effect. The intensity of exercise appears to be a prominent factor in ameliorating this molecular axis in cells of the infarcted heart.
Data availability
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Abbreviations
- AhR:
-
Aryl hydrocarbon receptor
- Ct:
-
Control group
- HIIT:
-
High-intensity interval training
- IDO1:
-
Indoleamine 2,3-dioxygenase 1
- KYN:
-
Kynurenine
- KP:
-
KYN pathway
- LAD:
-
Left anterior descending
- MDA:
-
Malondialdehyde
- MICT:
-
Moderate-intensity continuous training
- MANOVA:
-
Multivariate analysis of variance
- MI:
-
Myocardial infarction
- OLAD:
-
Occluded LAD
- MIHIIT:
-
Rats with OLAD and treated with HIIT
- MIMCT:
-
Rats with OLAD and treated with MICT
References
Contessotto, P. & Pandit, A. Therapies to prevent post-infarction remodelling: From repair to regeneration. Biomaterials 275, 120906 (2021).
Melhem, N. J. & Taleb, S. Tryptophan: From diet to cardiovascular diseases. Int. J. Mol. Sci. 22, 9904 (2021).
Wirthgen, E., Hoeflich, A., Rebl, A. & Günther, J. Kynurenic acid: The Janus-faced role of an immunomodulatory tryptophan metabolite and its link to pathological conditions. Front. Immunol. 8, 1957 (2018).
Seok, S. H. et al. Trace derivatives of kynurenine potently activate the aryl hydrocarbon receptor (AHR). J. Biol. Chem. 293, 1994–2005 (2018).
Rothhammer, V. & Quintana, F. J. The aryl hydrocarbon receptor: An environmental sensor integrating immune responses in health and disease. Nat. Rev. Immunol. 19, 184–197 (2019).
Kou, Z. & Dai, W. Aryl hydrocarbon receptor: Its roles in physiology. Biochem. Pharmacol. 185, 114428 (2021).
Vasquez, A. et al. A role for the aryl hydrocarbon receptor in cardiac physiology and function as demonstrated by AhR knockout mice. Cardiovasc. Toxicol. 3, 153–163 (2003).
Metghalchi, S. et al. Indoleamine 2 3-dioxygenase knockout limits angiotensin II-induced aneurysm in low density lipoprotein receptor-deficient mice fed with high fat diet. PLoS One 13, e0193737 (2018).
Melhem, N. J. et al. Endothelial cell Indoleamine 2, 3-dioxygenase 1 alters cardiac function after myocardial infarction through kynurenine. Circulation https://doi.org/10.1161/CIRCULATIONAHA.120.050301 (2021).
Lund, A. et al. Plasma kynurenines and prognosis in patients with heart failure. PLoS ONE 15, 1–15 (2020).
Li, M., Kwok, M. K., Fong, S. S. M. & Schooling, C. M. Indoleamine 2,3-dioxygenase and ischemic heart disease: A Mendelian randomization study. Sci. Rep. https://doi.org/10.1038/s41598-019-44819-7 (2019).
Joisten, N., Walzik, D., Metcalfe, A. J., Bloch, W. & Zimmer, P. Physical exercise as kynurenine pathway modulator in chronic diseases: Implications for immune and energy homeostasis. Int. J. Tryptophan Res. 13, 117864692093868 (2020).
Agudelo, L. Z. et al. Erratum: Skeletal muscle PGC-1α1 modulates kynurenine metabolism and mediates resilience to stress-induced depression (Cell (2014) 159 (33–45)). Cell 160, 351 (2015).
Martin, K. S., Azzolini, M. & Ruas, J. L. The kynurenine connection: How exercise shifts muscle tryptophan metabolism and affects energy homeostasis, the immune system, and the brain. Am. J. Physiol. Cell Physiol. 318, C818–C830 (2020).
Pal, A. et al. Different endurance exercises modulate NK cell cytotoxic and inhibiting receptors. Eur. J. Appl. Physiol. 121, 3379–3387 (2021).
Dun, Y. et al. High-intensity interval training improves metabolic syndrome and body composition in outpatient cardiac rehabilitation patients with myocardial infarction. Cardiovasc. Diabetol. 18, 1–11 (2019).
Wewege, M. A., Ahn, D., Yu, J., Liou, K. & Keech, A. High-intensity interval training for patients with cardiovascular disease-is it safe? A systematic review. J. Am. Heart Assoc. 7, e009305 (2018).
Cai, M. et al. Effects of different types of exercise on skeletal muscle atrophy, antioxidant capacity and growth factors expression following myocardial infarction. Life Sci. 213, 40–49 (2018).
Moholdt, T. et al. Aerobic interval training increases peak oxygen uptake more than usual care exercise training in myocardial infarction patients: A randomized controlled study. Clin. Rehabil. 26, 33–44 (2012).
Joisten, N. et al. Exercise Diminishes Plasma Neurofilament Light Chain and Reroutes the Kynurenine Pathway in Multiple Sclerosis. Neurol. Neuroimmunol. neuroinflammation 8, (2021).
Charan, J. & Biswas, T. How to calculate sample size for different study designs in medical research?. Indian J. Psychol. Med. 35, 121–126 (2013).
Høydal, M. A., Wisløff, U., Kemi, O. J. & Ellingsen, Ø. Running speed and maximal oxygen uptake in rats and mice: Practical implications for exercise training. Eur. J. Prev. Cardiol. 14, 753–760 (2007).
Wang, B. et al. Effect of high-intensity interval training on cardiac structure and function in rats with acute myocardial infarct. Biomed. Pharmacother. 131, (2020).
Khalafi, M. et al. The impact of moderate-intensity continuous or high-intensity interval training on adipogenesis and browning of subcutaneous adipose tissue in obese male rats. Nutrients 12, 925 (2020).
Gilani, N., Haghshenas, R. & Esmaeili, M. Application of multivariate longitudinal models in SIRT6, FBS, and BMI analysis of the elderly. Aging Male 22, 260–265 (2019).
Izeli, N. L. et al. Aerobic training after myocardial infarction: Remodeling evaluated by cardiac magnetic resonance. Arq. Bras. Cardiol. 106, 311–318 (2016).
Wisløff, U. et al. Superior cardiovascular effect of aerobic interval training versus moderate continuous training in heart failure patients: A randomized study. Circulation 115, 3086–3094 (2007).
Dschietzig, T. B. et al. Plasma kynurenine predicts severity and complications of heart failure and associates with established biochemical and clinical markers of disease. Kidney Blood Press. Res. 44, 765–776 (2019).
Rudzite, V. et al. Bradyarrythmias and myocardial cell failure induced By kynurenine. Prog. Tryptophan Serotonin Res. 1986, 131–136. https://doi.org/10.1515/9783110854657-038 (2019).
Wang, Q. et al. Activation of NAD(P)H oxidase by Tryptophan-derived 3-Hydroxykynurenine accelerates endothelial apoptosis and dysfunction in Vivo. Circ. Res. 114, 480–492 (2014).
Baran, H. et al. Effects of various kynurenine metabolites on respiratory parameters of rat brain, liver and heart mitochondria. Int. J. Tryptophan Res. 9, 17–29 (2016).
Valente-Silva, P. et al. Effects of tryptophan supplementation and exercise on the fate of kynurenine metabolites in mice and humans. Metabolites 11, 508 (2021).
Matsuo, Y. et al. Circulating malondialdehyde-modified low-density lipoprotein levels are associated with the presence of thin-cap fibroatheromas determined by optical coherence tomography in coronary artery disease. Eur. Heart J. Cardiovasc. Imaging 14, 43–50 (2013).
Liu, C. et al. Protective Effects and Mechanisms of Recombinant Human Glutathione Peroxidase 4 on Isoproterenol-Induced Myocardial Ischemia Injury. Oxid. Med. Cell. Longev. 2021, (2021).
Volkova, M., Palmeri, M., Russell, K. S. & Russell, R. R. Activation of the aryl hydrocarbon receptor by doxorubicin mediates cytoprotective effects in the heart. Cardiovasc. Res. 90, 305–314 (2011).
Carney, S. A. et al. Aryl hydrocarbon receptor activation produces heart-specific transcriptional and toxic responses in developing zebrafish. Mol. Pharmacol. 70, 549–561 (2006).
Huang, S. et al. AhR expression and polymorphisms are associated with risk of coronary arterial disease in Chinese population. Sci. Rep. 5, 8022 (2015).
Wang, B. & Xu, A. Aryl hydrocarbon receptor pathway participates in myocardial ischemia reperfusion injury by regulating mitochondrial apoptosis. Med. Hypotheses 123, 2–5 (2019).
Yi, T. et al. Aryl hydrocarbon receptor: A new player of pathogenesis and therapy in cardiovascular diseases. Biomed. Res. Int. 2018, 1–11 (2018).
Vilahur, G. et al. Reperfusion-triggered stress protein response in the myocardium is blocked by post-conditioning. Systems biology pathway analysis highlights the key role of the canonical aryl-hydrocarbon receptor pathway. Eur. Heart J. 34, 2082–2093 (2013).
Xue, Y. et al. Baicalin inhibits inflammation and attenuates myocardial ischaemic injury by aryl hydrocarbon receptor. J. Pharm. Pharmacol. 67, 1756–1764 (2015).
Korashy, H. & El-Kadi, A. The role of aryl hydrocarbon receptor in the pathogenesis of cardiovascular diseases. Drug Metab. Rev. 38, 411–450 (2006).
Liu, G., Chen, S., Zhong, J., Teng, K. & Yin, Y. Crosstalk between tryptophan metabolism and cardiovascular disease, mechanisms, and therapeutic implications. Oxid. Med. Cell. Longev. 2017, 1–5 (2017).
Liu, Y. et al. Indoleamine 2,3-dioxygenase 1 (IDO1) promotes cardiac hypertrophy via a PI3K-AKT-mTOR-dependent mechanism. Cardiovasc. Toxicol. 21, 655–668 (2021).
Guo, G., Sun, L., Yang, L. & Xu, H. IDO1 depletion induces an anti-inflammatory response in macrophages in mice with chronic viral myocarditis. Cell Cycle 18, 2598–2613 (2019).
Cardozo, G. G., Oliveira, R. B. & Farinatti, P. T. V. Effects of high intensity interval versus moderate continuous training on markers of ventilatory and cardiac efficiency in coronary heart disease patients. Sci. World J. 2015, 1–8 (2015).
Hannan, A. et al. High-intensity interval training versus moderate-intensity continuous training within cardiac rehabilitation: A systematic review and meta-analysis. Open Access J. Sport. Med. 9, 1–17 (2018).
Brauze, D., Widerak, M., Cwykiel, J., Szyfter, K. & Baer-Dubowska, W. The effect of aryl hydrocarbon receptor ligands on the expression of AhR, AhRR, ARNT, Hif1α, CYP1A1 and NQO1 genes in rat liver. Toxicol. Lett. 167, 212–220 (2006).
Kanth, V. R., Lavanya, K., Srinivas, J. & Naga Raju, T. Elevated expression of indoleamine 2,3-dioxygenase (IDO) and accumulation of kynurenic acid in the pathogenesis of STZ-induced diabetic cataract in wistar rats. Curr. Eye Res. 34, 274–281 (2009).
Acknowledgements
The authors offer their sincere thanks to the Histogenotech Research Center staff.
Funding
This study was supported by Semnan University and Basic Medical Science Research Center Histogenotech (No: 992124).
Author information
Authors and Affiliations
Contributions
Y.A. and R.H.: The conception and design of the study, analysis, and interpretation of data; P.N.: Methodology and acquisition of data; Y.A., R.H., H.A.: Drafting the article and revising it; Y.A., R.H., H.A., P.N.: Final approval of the version to be submitted.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Nori, P., Haghshenas, R., Aftabi, Y. et al. Comparison of moderate-intensity continuous training and high-intensity interval training effects on the Ido1-KYN-Ahr axis in the heart tissue of rats with occlusion of the left anterior descending artery. Sci Rep 13, 3721 (2023). https://doi.org/10.1038/s41598-023-30847-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-30847-x
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
