
Abstract
To compare spectacle lenses with highly aspherical lenslets (HAL) versus defocus incorporated multiple segments (DIMS) on myopia progression control in 1 year. This retrospective cohort study involved data from children prescribed HAL or DIMS spectacle lenses in Guangzhou Aier Eye Hospital, China. To address the discrepancy that some children followed up at less than or more than 1 year, the standardized 1-year spherical equivalent refraction (SER) and axial length (AL) changes from baseline were calculated. The mean differences in the changes between the two groups were compared with linear multivariate regression models. Age, sex, baseline SER/AL, and treatment were included in the models. A total of 257 children who qualified for the inclusion criteria were included for the analyses (193 in the HAL group and 64 in the DIMS group). After controlling baseline variates, the adjusted mean (standard error, SE) of the standardized 1-year changes in SER for HAL and DIMS spectacle lens users were − 0.34 (0.04) D and − 0.63 (0.07) D, respectively. HAL spectacle lenses reduced myopia progression by 0.29 D (95% confidence interval [CI] 0.13 to 0.44 D) at 1 year compared to DIMS lenses. Accordingly, the adjusted mean (SE) ALs increased by 0.17 (0.02) and 0.28 (0.04) mm for children wearing HAL lenses and DIMS lenses, respectively. HAL users had 0.11 mm less AL elongation (95% CI − 0.20 to − 0.02 mm) than DIMS users. Age at baseline was significantly associated with AL elongation. Chinese children wearing spectacle lenses designed with HAL had less myopia progression and axial elongation than those wearing spectacle lenses designed with DIMS.
Similar content being viewed by others


Introduction
Myopia prevalence has been increasing dramatically in recent decades worldwide, particularly in East Asian countries, such as China1. By 2020, the prevalence of myopia among teenagers reached approximately 70% in urban cities in China2,3. It is estimated that by 2050, 50% of the population will have myopia, and 10% will have high myopia worldwide4. In particular, the predicted prevalence of myopia in China is even higher, with 84% of Chinese people having myopia5.
Multiple interventions have been shown to significantly slow myopia progression, including the use of some specifically designed spectacle lenses, orthokeratology lenses, multifocal soft contact lenses, etc6. With easy adaptation features, no ocular infection concern, and lower cost compared to contact lenses, spectacles are the most common choice for myopia control7,8.
Several types of spectacles have been developed to slow myopia progression6,9,10. Among specifically designed lenses, recent research has shed light on two types of anti-myopic spectacle lenses11. In 2019, the effect on myopia control with defocus incorporated multiple segments (DIMS) spectacle lenses was published. The DIMS group delayed myopia progression by 52% compared to single-vision lenses in 2 years12. DIMS spectacle lenses have a 9-mm central single-vision zone surrounded by a honeycomb area consisting of multiple 1.03 mm width, + 3.5 D myopic defocus segments. Later, another 2-year clinical trial found that children wearing spectacle lenses comprising rings with highly aspherical lenslets (HAL) reduced myopia progression by 55% compared with those wearing single-vision lenses13. Outside the central normal refractive correction zone, the HAL lenses consist of 11 rings of continuous lenslets. The lenslet produces a volume of myopic defocus image with 0.7 mm depth and approximately 1.2 mm before the retina14.
The two types of lenses both produce myopic defocus in the peripheral retina while maintaining a clear central vision. The two separate studies showed comparable effects of spectacles lenses with HAL or DIMS for preventing myopia progression. Since there are notable differences in the design of the lenses, we aimed to compare the myopia control efficacy between these two types of lenses.
Methods
This was a retrospective cohort study. The ethics committee of Guangzhou Aier Eye Hospital approved the study protocol, including the waiver of informed consent (GZAIER2022IRB11). The study was performed while observing the tenants of the Declaration of Helsinki. Data were collected from the Guangzhou Aier Eye Hospital database between September 2020 and March 2022. The children were selected if they were prescribed either HAL or DIMS, were younger than 16 years, and were without strabismus, amblyopia, or other ocular or systematic abnormalities. In addition, only those who had a refraction test between 6 and 18 months after the baseline visit without changing the type of spectacles were included in the analyses.
Cycloplegic autorefraction using Topcon KR 800 (Japan) followed by subjective refraction was performed at baseline. Noncycloplegic auto- and subjective refraction were examined during the follow-up visit. If the results were ambiguous, cycloplegic refraction was conducted. Cycloplegia was induced in each eye with three drops of 0.5% tropicamide administered 5 min apart. Refraction tests were performed 15 min after the last drop. The results from subjective refraction were used for the analyses. The axial length (AL) was measured at least three times with a ZEISS IOLMaster 500 (Germany), and the average was calculated.
The primary outcome was the spherical equivalent refraction (SER) change from baseline. SER was calculated with spherical power plus half cylinder power. The secondary outcomes included the AL, spherical power, and cylinder power differences. The follow-up records within 12 ± 6 months were used to standardize the changes from baseline to 1 year according to the following calculation: changes in outcome values × (12/actual months between baseline and follow-up).
Only the results of the right eyes were reported as significant correlations were observed between the two eyes for the changes in SER (r = 0.58, P < 0.001), AL (r = 0.78, P < 0.001), spherical power (r = 0.75, P < 0.001), and cylinder power (r = 0.30, P < 0.001). To compare the baseline characteristics between the two groups, unpaired t-tests were used for continuous variables, and the chi-square test was used for the categorical variable. The differences in the outcomes between the two groups were analyzed with unpaired t-tests and linear multivariate regression models. The models included age, sex, baseline refractive values or AL, and treatment as covariates. Age, refractive values, and AL were treated as continuous variables, while sex and treatment were treated as categorical variables in the models. The linear regression models with the same covariates were repeated for the observations without any missing values as sensitivity analyses. The analyses were performed with SAS 9.4 software. Results with a two-sided P value ≤ 0.05 were considered statistically significant.
Results
A total of 403 children were prescribed HAL (n = 296) or DIMS (n = 107) lenses within the study period. There were 193 of 296 (65%) children in the HAL group and 64 of 107 (60%) children in the DIMS group who met the inclusion criteria for the final analyses. There were missing values of axial length (AL) for some observations, leaving 102 in the HAL group and 33 in the DIMS group with complete data for the sensitivity analyses. The distributions of baseline prescription dates were comparable between the two groups. The peaks of starting dates were in October 2020 and January to February 2021 (Fig. 1).

Distributions of baseline prescription dates in the two groups. DIMS defocus incorporated multiple segments, HAL highly aspherical lenslets.
Children prescribed HAL lenses were younger than those offered DIMS lenses, with a mean (standard error, SE) age of 9.57 (0.16) years versus 10.29 (0.26) years (mean difference, − 0.72 years; 95% confidence interval, [CI], − 1.34 to − 0.09 years; P = 0.03). Sex, baseline refractive values, and AL were comparable between the two groups (Table 1). The mean (SE) follow-ups were 274.2 (5.5) days and 267.3 (9.3) days for the HAL and DIMS groups,respectively, and the difference was not statistically significant (mean difference, 6.9 days; 95% CI − 14.7 to 28.5 days; P = 0.53). Twenty-one (11%) children in the HAL group and 7 (11%) children in the DIMS group were prescribed the cycloplegic refraction at the follow-up visit.
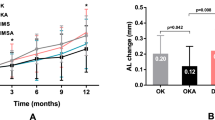
The unadjusted, standardized, 1-year mean (SE) change in SER was − 0.34 (0.04) D for the HAL group and − 0.63 (0.08) D for the DIMS group. The 95% CI of the mean difference (0.29 D) between the two groups was 0.13 to 0.44 D (P < 0.001). After controlling for age, sex, and baseline SER, the adjusted SER change difference showed a similar result (Table 2). Accordingly, the adjusted mean (SE) difference in the spherical power change was 0.32 (0.08) D (95% CI 0.17 to 0.47 D; P < 0.001). In contrast, the changes in cylinder power were not significantly different between the two groups (95% CI − 0.15 to 0.06 D; P = 0.42). The unadjusted, standardized, 1-year mean (SE) axial elongations for children using the HAL lenses and DIMS lenses were 0.17 (0.02) mm and 0.27 (0.04) mm, respectively. The HAL group exhibited slower AL increase than the DIMS group, with a mean difference of − 0.10 mm (95% CI − 0.19 to − 0.01 mm; P = 0.03). The adjusted mean difference in AL change was − 0.11 mm (95% CI − 0.20 to − 0.02 mm; P = 0.02).
In the sensitivity tests without missing records for SER or AL, the adjusted, standardized, 1-year mean (SE) changes in SER were − 0.31 (0.05) D and − 0.59 (0.09) D in the HAL (n = 102) and DIMS (n = 33) groups, respectively. The mean (SE) difference between the two groups was 0.27 (0.10) D (95% CI 0.08 to 0.47 D; P = 0.008). The adjusted, standardized, 1-year mean (SE) ALs increased by 0.17 (0.02) mm and 0.28 (0.04) mm for children wearing HAL and DIMS lenses, respectively. DIMS users had significantly greater AL increase with a mean (SE) difference of − 0.11 (0.05) mm (95% CI − 0.20 to 0.02 mm; P = 0.02).
In the linear multivariate regression model, baseline age was negatively associated with axial lengthening. The standardized AL showed a 0.02 mm less increase with 1 year older at baseline (P = 0.03). In contrast, age was not significantly associated with SER change. Sex and baseline SER or AL values were not associated with SER or AL changes during the study period.
Discussion
In this study, children using highly aspherical lenslets (HAL)-designed spectacle lenses reduced 0.29 D myopia progression and 0.11 mm axial length (AL) elongation compared to those wearing DIMS lenses over a standardized 1-year period after adjusting for age, sex, and baseline spherical equivalent refraction (SER) or AL. Significant differences in SER and AL changes were also detected in sensitivity tests including records without missing outcome values.
Hyperopic defocus images captured by retinal neurons can trigger eye growth, while myopic defocus inhibits eye enlargement15,16. Although the density of neurons in the central retina is the greatest, the accumulated number of neurons in the peripheral retina is larger than that in the fovea16. The area of the functional zone that creates peripheral myopic defocus is larger in the HAL lens than in the DIMS lens, which might lead to better myopia control. In addition, peripheral myopic defocus power was negatively associated with axial growth, which has been confirmed by previous studies on spectacle lenses and orthokeratology contact lenses14,17. It is possible that the degree of myopic defocus is different between the two lenses. Overall, the whole myopic defocus volume is assumed to be higher in the HAL lens than in the DIMS lens, which leads to slower myopia progression and axial growth using HAL lenses.
In this study, we observed that the unadjusted, standardized, 1-year mean myopia progression for HAL lens wearers was − 0.34 D with an AL increase of 0.17 mm. The outcomes are slightly higher than those of the previous 1-year 3-arm randomized control trial (RCT) comparing HAL, slightly aspherical lenslets (SAL), and single-vision lenses (− 0.27 D SER change and 0.13 mm AL increase in the HAL group)14. The raw mean SER and AL changes were − 0.63 D and 0.28 mm for the children wearing DIMS lenses in the present study. In contrast, a previous RCT comparing DIMS lenses and single-vision lenses showed less myopia progression as well as AL increase at the 1-year follow-up for DIMS users (− 0.17 D, 0.11 mm)12. Table 3 summarises the characteristics and outcomes of the present and previous studies.
We assumed that the study period and region are the two main factors that caused the notable discrepancy in the effect for DIMS lenses between the study of Lam et al. and ours. Between 2020 and 2021, because of the COVID-19 pandemic, web-based education was promoted and even required in affected regions, including China18. Several studies have shown a myopia surge during this period19,20,21. The DIMS study by Lam et al. was conducted from 2014 to 2017, which was before the COVID-19 pandemic, while the HAL studies of Bao et al. and the present study were conducted mainly during the pandemic. In addition, both the HAL RCT and the present study observed children in mainland China, which has numerous differences in its education system, living environment, and lifestyle compared with those of Hong Kong, China.
In this study, older children had slower axial elongations but showed similar SER changes compared to younger children. It is possible that the process of emmetropization contributed to a significant AL increase without a comparable degree of SER change in young children22. In this study, neither sex nor baseline myopic indexes (SER and AL) were associated with myopia progression.
Strengths of the study
To the best of our knowledge, this was the first study comparing HAL and DIMS lenses, which are two of the most compelling spectacle lenses for myopia control compared with single-vision spectacle lenses6,11,14,23. We compared these two lenses in the same population and found that HAL-designed lenses had a more substantial effect than DIMS lenses for the prevention of myopia progression as well as AL elongation in Chinese children.
DIMS lenses had been widely used before HAL lenses were introduced to the market. To control the lockdown effect on myopia progression, we chose the starting point when the first qualified HAL lens user was available and obtained a similar baseline date distribution between the two study lenses19,20. Additionally, we found that for the HAL lenses, the average annual change in SER was approximately − 0.34 D, with an increase in AL of 0.17 mm from the real-world data.
Limitations of the study
There are some limitations in this study. Since this is a retrospective study, some confounders could not be identified, such as time spent outdoors, near-work time, myopia in parents, and duration of wearing spectacle lenses. The average follow-up was approximately nine months, and we used a standardized method to predict 1-year outcomes, which might be slightly different from the actual results for 1 year24. However, since the follow-up duration was similar between the two groups, this method should not affect the comparisons between the two types of lenses. Some children did not have cycloplegic refraction in the follow-up tests, and the results might overestimate the progression of myopia. However, we found a corresponding axial elongation associated with SER progression in children25. In addition, the data were from Chinese children in only one region. Thus, the results may not be applied to other ethnic children or other areas. Although the study had some limitations, we found a significant difference in myopia control between the two most effective spectacle lenses. Future studies with randomized designs or with locations in other regions are encouraged.
Conclusion
Spectacle lenses with highly aspherical lenslets (HAL) were more effective in delaying myopia progression and axial elongation than defocus incorporated multiple segments (DIMS) lenses in Chinese children.
Data availability
The data that support the findings in this study are available from the corresponding authors on reasonable request.
References
Foster, P. J. & Jiang, Y. Epidemiology of myopia. Eye (Lond) 28, 202–208. https://doi.org/10.1038/eye.2013.280 (2014).
Guo, L. et al. Prevalence and associated factors of myopia among primary and middle school-aged students: A school-based study in Guangzhou. Eye (Lond) 30, 796–804. https://doi.org/10.1038/eye.2016.39 (2016).
He, X. et al. Prevalence of myopia and high myopia, and the association with education: Shanghai Child and Adolescent Large-scale Eye Study (SCALE): A cross-sectional study. BMJ Open 11, e048450. https://doi.org/10.1136/bmjopen-2020-048450 (2021).
Holden, B. A. et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology 123, 1036–1042. https://doi.org/10.1016/j.ophtha.2016.01.006 (2016).
Dong, L., Kang, Y. K., Li, Y., Wei, W. B. & Jonas, J. B. Prevalence and time trends of myopia in children and adolescents in China: A systemic review and meta-analysis. Retina 40, 399–411. https://doi.org/10.1097/IAE.0000000000002590 (2020).
Jonas, J. B. et al. IMI prevention of myopia and its progression. Invest. Ophthalmol. Vis. Sci. 62, 6. https://doi.org/10.1167/iovs.62.5.6 (2021).
Lim, M. C., Gazzard, G., Sim, E. L., Tong, L. & Saw, S. M. Direct costs of myopia in Singapore. Eye (Lond) 23, 1086–1089. https://doi.org/10.1038/eye.2008.225 (2009).
Wolffsohn, J. S. et al. Global trends in myopia management attitudes and strategies in clinical practice - 2019 Update. Cont. Lens Anterior Eye 43, 9–17. https://doi.org/10.1016/j.clae.2019.11.002 (2020).
Walline, J. J. et al. Interventions to slow progression of myopia in children. Cochrane Database Syst. Rev. 1, CD004916. https://doi.org/10.1002/14651858.CD004916.pub4 (2020).
Sankaridurg, P. et al. Spectacle lenses designed to reduce progression of myopia: 12-month results. Optom. Vis. Sci. 87, 631–641. https://doi.org/10.1097/OPX.0b013e3181ea19c7 (2010).
Carla, M. M. et al. Overview on defocus incorporated multiple segments lenses: A novel perspective in myopia progression management. Vision (Basel) 6. https://doi.org/10.3390/vision6020020(2022).
Lam, C. S. Y. et al. Defocus incorporated multiple segments (DIMS) spectacle lenses slow myopia progression: a 2-year randomised clinical trial. Br. J. Ophthalmol. 104, 363–368. https://doi.org/10.1136/bjophthalmol-2018-313739 (2020).
Bao, J. et al. Spectacle lenses with aspherical lenslets for myopia control vs single-vision spectacle lenses: a randomized clinical trial. JAMA Ophthalmol. 140, 472–478. https://doi.org/10.1001/jamaophthalmol.2022.0401 (2022).
Bao, J. et al. One-year myopia control efficacy of spectacle lenses with aspherical lenslets. Br. J. Ophthalmol. https://doi.org/10.1136/bjophthalmol-2020-318367 (2021).
Russo, A. et al. Myopia: Mechanisms and strategies to slow down its progression. J. Ophthalmol. 2022, 1004977. https://doi.org/10.1155/2022/1004977 (2022).
Wallman, J. & Winawer, J. Homeostasis of eye growth and the question of myopia. Neuron 43, 447–468. https://doi.org/10.1016/j.neuron.2004.08.008 (2004).
Zhong, Y., Chen, Z., Xue, F., Miao, H. & Zhou, X. Central and peripheral corneal power change in myopic orthokeratology and its relationship with 2-year axial length change. Invest. Ophthalmol. Vis. Sci. 56, 4514–4519. https://doi.org/10.1167/iovs.14-13935 (2015).
Fan, Q. et al. Online learning-related visual function impairment during and after the COVID-19 pandemic. Front. Public Health 9, 645971. https://doi.org/10.3389/fpubh.2021.645971 (2021).
Choi, K. Y. et al. Evaluation of an optical defocus treatment for myopia progression among schoolchildren during the COVID-19 Pandemic. JAMA Netw. Open 5, e2143781. https://doi.org/10.1001/jamanetworkopen.2021.43781 (2022).
Rosenfield, M. COVID-19 and myopia. Ophthal. Physiol. Opt. 42, 255–257. https://doi.org/10.1111/opo.12944 (2022).
Limwattanayingyong, J., Amornpetchsathaporn, A., Chainakul, M., Grzybowski, A. & Ruamviboonsuk, P. The association between environmental and social factors and myopia: A review of evidence from COVID-19 pandemic. Front. Public Health 10, 918182. https://doi.org/10.3389/fpubh.2022.918182 (2022).
Brown, N. P., Koretz, J. F. & Bron, A. J. The development and maintenance of emmetropia. Eye (Lond) 13(Pt 1), 83–92. https://doi.org/10.1038/eye.1999.16 (1999).
Lam, C. S. et al. Myopia control effect of defocus incorporated multiple segments (DIMS) spectacle lens in Chinese children: Results of a 3-year follow-up study. Br. J. Ophthalmol. 106, 1110–1114. https://doi.org/10.1136/bjophthalmol-2020-317664 (2022).
Brennan, N. A., Toubouti, Y. M., Cheng, X. & Bullimore, M. A. Efficacy in myopia control. Prog. Retin. Eye Res. 83, 100923. https://doi.org/10.1016/j.preteyeres.2020.100923 (2021).
Liu, S. et al. Association between axial length elongation and spherical equivalent progression in Chinese children and adolescents. Ophthal. Physiol. Opt. 42, 1133–1140. https://doi.org/10.1111/opo.13023 (2022).
Funding
This study was supported in part by the Medical Science and Technology Research Grant in Guangdong Province (A2021368) and the Panyu Science and Technology Project (2020-Z04-046).
Author information
Authors and Affiliations
Contributions
All the authors in this study were involved in protocol preparation (H.G., X.X.Z., J.H.L.), data collection (H.G., X.F.L., X.X.Z., J.H.L.), data analysis (H.G., H.Z.W.), and manuscript editing (H.G., X.F.L., X.X.Z., H.Z.W., J.H.L.).
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Guo, H., Li, X., Zhang, X. et al. Comparing the effects of highly aspherical lenslets versus defocus incorporated multiple segment spectacle lenses on myopia control. Sci Rep 13, 3048 (2023). https://doi.org/10.1038/s41598-023-30157-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-30157-2
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
