
Abstract
The Korean Intermittent Exotropia Multicenter Study (KIEMS) was a retrospective, cross-sectional and multicenter study for the investigation of intermittent exotropia involved 65 strabismus specialists from 53 institutions in Korea. Purpose of this study was to present ophthalmologic findings of intermittent exotropia from the KIEMS. Consecutive patients with intermittent exotropia of ≥ 8 prism diopters (PD) at distance or near fixation were included. Best-corrected visual acuity, cycloplegic refraction data, angles of deviation at several cardinal positions, ocular dominance, fusion control, oblique muscle function, and binocular sensory outcomes were collected. A total of 5385 participants (2793 females; age 8.2 years) were included. Non-dominant eye was more myopic than the dominant eye (− 0.60 vs. − 0.47 diopters, P < 0.001). Mean exodeviation angles were 23.5 PD at distance and 25.0 PD at near fixation. Basic type (86.2%) was the most, followed by convergence insufficiency (9.4%) and divergence excess (4.4%) types. Alternating ocular dominance and good fusion control were more common at near than at distance fixation. Good stereopsis at 40 cm was observed in 49.3% in Titmus stereo test (≤ 60 arcsec) and in 71.0% in Randot stereo test (≤ 63 arcsec). Intermittent exotropia was mostly diagnosed in childhood and patients with the condition showed relatively good binocular functions. This study may provide objective findings of intermittent exotropia in a most reliable way, given that the study included a large study population and investigated comprehensive ophthalmology examinations.
Similar content being viewed by others

Introduction
Intermittent exotropia is an outward drifting of either eye in a latent or intermittent form1,2. It is a predominant form of strabismus in East Asian countries3,4,5,6, including Korea7,8, and is also common in the United States9 and some European countries10. Although many clinical studies have been conducted on this common disease entity, many questions remain unanswered11. The interpretations of the results of many clinical studies on intermittent exotropia have been confusing owing to variable study settings, different study protocols, and the clinical variability of this condition12. Mostly, previous studies focused on the surgical results and included patients with relatively large angle of exotropia requiring surgery13,14,15,16,17, which might exclude the clinical findings of relatively small angle intermittent exotropia. Also, those studies reported various types of stereoacuity, binocularity, ocular dominance and fusion control tests11,12, which were not interchangeable for comparison. Most ophthalmologic examinations for diagnosis of intermittent exotropia depended largely on the examiners’ skill because those examinations can be performed only manually. To obtain comprehensive and convincing information about the clinical characteristics of intermittent exotropia, a large-scale study, regardless of clinical considerations, such as age, amount of exotropia angle, and necessity of surgical intervention, is needed. Also, the ophthalmologic examinations need to be conducted by strabismus specialists using a standardized protocol.
The Korean Intermittent Exotropia Multicenter Study (KIEMS) is a large-scale nationwide and multicenter study investigating the clinical features of intermittent exotropia using a standardized protocol. It was initiated by the Korean Association of Pediatric Ophthalmology and Strabismus (KAPOS), whose members are strabismus specialists. The KIEMS is one of the largest clinical studies on intermittent exotropia to date and is expected to present the overall features, including the subjective and objective features, of intermittent exotropia. This study was conducted to present the objective ophthalmologic findings from the KIEMS.
Results
Baseline characteristics of participants
A total of 5385 participants were included in this study with age of 8.2 ± 7.6 years (mean ± standard deviation; range, 0.3–106.7 years). The age distribution of all participants has been previously described18. The mean spherical equivalent (SE) was – 0.57 ± 1.89 diopters (D) (range, + 7.0 to − 12.88 D) in the right eye and -0.61 ± 1.96 D (range, + 8.75 to − 14.00 D) in the left eye (P = 0.666, paired t-test). The non-dominant eye at distance fixation tended to be more myopic than the dominant eye (SE: − 0.60 ± 1.98 vs. − 0.47 ± 1.74 D, P < 0.001, paired t-test) (Table 1).
Of the 5385 participants, 2793 (51.9%) were females and 2592 (48.1%) were males, showing a slight female predominance. Male participants were older than female participants (8.6 ± 7.3 vs. 7.8 ± 7.8 years, independent t-test, P < 0.001). According to the mean SE, the right and left eyes of male participants were more myopic than those of female participants (independent t-test, P < 0.001). Hyperopia (mean SE > + 1 D), emmetropia (≤ + 1 and ≥ − 1 D), and myopia (< − 1 D) were observed in 12.0% (507/4219), 55.4% (2338/4219), and 32.6% (1374/4219) participants, respectively. The mean exodeviation angle in the primary position at distance fixation was 23.2 ± 9.0 PD in males, which was smaller than that in females (23.7 ± 8.6 PD) (independent t-test, P = 0.036). With respect to the mean exodeviation angle at near fixation, no sex difference was observed (25.0 ± 9.4 vs. 25.1 ± 9.3 PD, independent t-test, P = 0.543).
Angles of exodeviation
The mean angle of exodeviation in the primary position was 23.5 ± 8.8 (range, 0–85) PD at distance fixation and 25.0 ± 9.3 (range, 0–90) PD at near fixation. Basic-type exotropia (difference between distant and near angles ≤ 10 PD), convergence insufficiency-type exotropia (near–distant angle < 10 PD), and divergence excess-type exotropia (distant–near angle > 10 PD) were observed in 86.2% (4599/5331), 9.4% (500/5331), and 4.4% (232/5331), respectively. Participants with convergence insufficiency-type exotropia were older than those with basic- and divergence excess-type exotropia (independent t-test, Bonferroni corrected P < 0.001). The exodeviation angles in the secondary and head-tilted positions were smaller than those in the primary position (Table 2, paired t-test, P < 0.001).
Lateral incomitance was present in 2.3% (95/4164) in right gaze and in 2.0% (83/4166) in left gaze. Lateral incomitance in both right gaze and left gaze was present in 1.5% (63/4163). The A and V patterns of exotropia were observed in 0.9% (35/3889) and 1.1% (44/3889), respectively.
Ocular dominance and fusion control
Ocular dominance in the right or left eye was present in 51.7% (29.1% for the right eye, 22.6% for the left eye, 2407/4655) at distance fixation and in 39.0% (22.1% for the right eye, 16.9% for the left eye, 1725/4422) at near fixation. Alternating ocular dominance was observed in 48.3% (2248/4655) and 61.0% (2697/4422) at distance and near fixation, respectively. The ratio of alternating ocular dominance was significantly higher at near than at distance fixation (P < 0.001, Pearson’s chi-square test).
In the assessment of fusion control, the proportion of participants with good and fair control was 27.6% (1336/4835) and 41.6% (2010/4835) at distance fixation and 42.6% (1977/4641) and 37.1% (1723/4641) at near fixation, respectively. The proportion of participants who showed poor fusion control was 30.8% (1489/4835) at distance fixation and 20.3% (941/4641) at near fixation. Fusion control was better at near than at distance fixation (P < 0.001, Pearson’s chi-square test).
Associated strabismus
Inferior oblique overaction (IOOA) was present in 25.5% of the participants (1092/4278), whereas superior oblique overaction (SOOA) was observed in only 6.0% (249/4120). Bilateral IOOA and SOOA (15.5% and 3.4%, respectively) were more common than unilateral IOOA and SOOA (10.0% and 2.6%, respectively). In contrast, inferior and superior oblique under actions were relatively rare (0.4% and 2.5%, respectively) (Table 3). Vertical deviation of ≥ 5 PD in the primary position was present in 4.9% (266/5385) (Table 1). Dissociated vertical deviation was present in 0.6% of the participants (35/5385) (Table 1).
Sensory status evaluations
In the Worth four-dot test at 6 m, 49.6% of the participants (1924/3881) saw four lights, which was interpreted as “fusion” if normal retinal correspondence existed; 35.7% (1385/3881) saw two or three lights, recorded as “suppression”; and 14.7% (572/3881) saw five lights, recorded as “diplopia.”
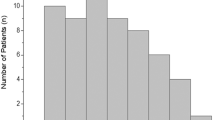
Histograms of the Titmus (circles) and Randot stereo test results at 40 cm are shown in Fig. 1A and B. “Good stereopsis,” defined as ≤ 60 arcsec in the Titmus stereotest and as ≤ 63 arcsec in the Randot stereo test, was observed in 49.3% (1657/3358) and 71.0% (697/982), respectively.

Histograms of near stereoacuity results. Most participants showed good stereoacuity results: 49.3% with ≤ 60.
Discussion
This study described the objective examination findings from the KIEMS, which is one of the largest clinical studies on intermittent exotropia to date. Although many previous studies on the clinical characteristics of intermittent exotropia have been conducted, the KIEMS is expected to provide the most comprehensive and reliable overview of the clinical spectra of intermittent exotropia in terms of sample size and study parameters.
In this study, the number of female participants (51.9%) was comparable to that of male participants (48.1%). In a previous population-based cohort study including participants aged < 19 years in the United States, a female predominance (64.1%) was reported19. Another multicenter cohort study in the United Kingdom also reported a slight female predominance (55.9%) in children aged < 12 years with untreated intermittent exotropia20. In contrast, in Singaporean4 and Chinese5 population-based studies in children aged < 6 years (mostly of Chinese ethnicity), the prevalence of exotropia showed no sex difference when compared with the general population. In addition, a previous population-based study in Korea reported that sex was not significantly associated with clinically significant intermittent exotropia (≥ 15 PD) in adolescence7. Studies in Asian countries including our study have found no sex predominance in the prevalence of intermittent exotropia, whereas Western studies tended to show a female predominance. Future studies with age or ethnicity standardization are needed to clarify the sex differences in intermittent exotropia.
In this study, basic-type exotropia (86.2%) was the predominant type followed by convergence insufficiency-type (9.4%) and divergence excess-type (4.4%) exotropia when classified based on a ≥ 10 PD difference between the distant and near exotropia angles. Patients with the convergence insufficiency type were older than those with the other two types. Similarly, a recent study in Korea reported that basic-type exotropia was the most prevalent type (79.2%) in 355 patients with exotropia14. A population-based study from China reported a 74.7% prevalence of basic-type exotropia in 166 patients with intermittent exotropia aged 3–6 years5. Rutstein and Corliss also reported basic-type exotropia as the most common type in 73 patients21. A study from Singapore reported that divergence excess-type exotropia had a higher prevalence (59.5%) than basic-type exotropia (27%) in 453 patients with intermittent exotropia; however, the authors speculated that some patients with basic-type exotropia may have been inadvertently classified to the divergence excess type, as the children were not routinely patched to eliminate tenacious proximal fusion22. However, Burian and Franceschetti observed basic-type exotropia in 33% and convergence insufficiency-type exotropia in 55% of 237 prospectively collected consecutive patients, although they used stricter standards in classifying cases as convergence insufficiency-type exotropia23. Kushner and Morton observed divergence excess-type exotropia in 48.5%, which was the most prevalent type, although it included 80 patients (39.6% of the total participants) with simulated divergence excess (within a distant–near angle difference of 10 PD after 1 h of monocular patching), and basic-type exotropia in 38.6% of 202 patients with intermittent exotropia24. They reported that convergence insufficiency-type exotropia was more common in older participants, consistent with the current study (Table 4). The proportion of intermittent exotropia types may be affected by the inclusion criteria used or the clinical characteristics of the participants.
Alternating ocular dominance (48.3% at distance, 61.0% at near) was more common than right or left dominance (29.1% for the right eye and 22.6% for the left eye at distance; 22.1% for the right eye and 16.9% for the left eye at near) in this study. The proportion of alternating ocular dominance at near fixation was larger than that at distance fixation. Similarly, fusion control was better under the near viewing condition than under the distant viewing condition in this study. Previous studies investigating fusion control in patients with intermittent exotropia showed similar results25,26,27. In monocular dominance, there is a preference for one eye over the other eye under the binocular viewing condition, whereas no such preference exists in alternating ocular dominance28. It is well known that patients with intermittent exotropia rarely manifest amblyopia in either eye (if amblyopia occurs, it mostly manifests in the non-dominant eye) because the eyes can remain aligned at least in the near fixation condition29. Therefore, the result of this study confirmed that patients with intermittent exotropia show good binocular interaction.
More than 60% of the participants saw four or five lights in the distant Worth four-dot test, which suggests that patients with intermittent exotropia have relatively good binocular function at distant fixation, in which the sensory function of one eye does not overwhelm that of the other eye; however, seeing four lights in the test does not necessarily mean that the participants had central foveal fusion30. Monocular suppression was observed in < 40% of the patients, evenly in each eye. In the Titmus stereotest at 40 cm, approximately 50% of the participants showed good stereopsis of ≤ 60 arcsec, reflecting central fusion at near fixation. Moreover, in the Randot stereoacuity test at near fixation, > 70% of the participants showed ≤ 63 arcsec of stereopsis. Romanchuk et al. reported that 72.5% of their 109 patients showed better stereopsis than 60 arcsec in the Titmus stereo test even after ≥ 9 years follow-up from the initial visit31. Similarly, Mohney et al. reported that 63% of 152 patients showed 60 arcsec or better stereopsis in the Randot stereo test in a Pediatric Eye Disease Investigator Group study32. It is well known that patients with intermittent exotropia have relatively good near stereopsis1. The participants in this study can be assumed to have similarly good binocular functions, as previously reported.
This study should be viewed in the light of its limitations. Owing to the retrospective study design, data collection could not be performed as strictly as in a prospective study, which may have inevitably biased the patient selection or data collection process. Moreover, data were collected from 65 strabismus specialists from 53 different institutions and the circumstances of ophthalmologic examinations may have been different among the investigators, possibly affecting the study results. Despite efforts to reduce variability through the use of a standardized protocol and standardized case report forms, this study had the same limitations as many other multicenter studies.
In conclusion, this large observational study that included 5385 participants reported the objective findings of intermittent exotropia. In most of the study participants, intermittent exotropia was diagnosed during childhood (age, 8.2 ± 7.6 years). Basic-type exotropia was the most common type, followed by the convergence insufficiency and divergence excess types. In the assessment of fusion control, good to fair control was observed in 69.2% at distance fixation and in 79.8% at near fixation, and “good stereopsis” (\(\le\) 60 arcsec in the Titmus stereotest and ≤ 63 arcsec in the Randot stereo test) was observed in 49.3% and 71.0%, respectively. This study potentially provides the most reliable information on the general clinical spectra of intermittent exotropia thus far, given the large study size and the coordination among many specialized investigators. Future studies using the KIEMS data are expected to provide more information about various aspects of intermittent exotropia.
Methods
The KIEMS is a nationwide, retrospective, observational, cross-sectional, and multicenter study. The protocol of the KIEMS has been described elsewhere18. Briefly, the study was conducted as a collaboration among 65 strabismus specialists who were members of KAPOS and affiliated with 53 institutions in Korea. The medical records of patients who visited the eye clinic of each institution for the first time between March 1, 2019, and February 29, 2020, were reviewed. Participants with intermittent exotropia with ≥ 8 prism diopters (PD) at distance fixation (at 6 m) or near fixation (33 cm) in the prism and alternate cover test (PACT), regardless of age, were included in this study. Participants who had previous strabismus surgery history were excluded. Participants were excluded if they had signs of incomitant strabismus, ocular conditions affecting vision or prior ocular surgical history, chromosomal anomalies, or systemic disorders such as congenital anomalies or neurologic disorders. The KIEMS protocol conformed to the tenets of the Declaration of Helsinki. The protocol was approved by the Institutional Review Board of Kim’s Eye Hospital (KEH 2020-05-007) and by each participating institution. The requirement for informed consent was waived by the Institutional Review Board of Kim’s Eye Hospital because the study used retrospectively collected clinical data and the data were accessed anonymously.
The KIEMS collected data from subjective questionnaires completed by patients or guardians and from the results of objective ophthalmologic examinations conducted by strabismus specialists. In this study, we collected and analyzed the following objective data from ophthalmologic examinations in the KIEMS: age, sex, best-corrected visual acuity, refractive errors measured using cycloplegic refraction with 1% cyclopentolate hydrochloride (Cyclogyl; Alcon Lab. Inc., Fort Worth, TX, USA) and 1% tropicamide (Mydriacyl, Alcon Lab. Inc.), angles of deviation in PACT (in the primary, secondary, and head-tilted positions under distant [6 m] and near [33 cm] viewing conditions using accommodative targets with the patients’ best optical correction), and associated strabismus (e.g., dissociated vertical deviation, vertical deviation, and oblique muscle dysfunction). Vertical deviation was defined as hypertropia/hypotropia of ≥ 5 PD in the primary position. Lateral incomitance was defined as a decrease in the exo-angle of ≥ 20% in the right or left gaze, as compared with that in the primary position. “A” pattern exotropia was defined as a condition in which the exotropia angle at down gaze was higher by ≥ 10 PD than that at up gaze. Likewise, “V” pattern exotropia was defined as a condition in which the exotropia angle at up gaze was higher by ≥ 15 PD than that at down gaze. Right or left ocular dominance was determined to be present when the right or left eye had a shorter duration of dissociation during the uncover test, and alternating ocular dominance was identified when the duration of dissociation was similar between the two eyes. Fusion control under the distant and near viewing conditions was also investigated and classified as follows: good control, when ocular fusion was disrupted only after the cover test at distance fixation and was rapidly regained without blinking or fixating ocular movements; fair control, when ocular fusion was regained only after blinking or fixating movements after disruption with cover testing at distance fixation; and poor control, when ocular fusion was spontaneously broken without fusion disruption or was not regained despite blinking or refixation33. For sensory status evaluation, the Worth four-dot test (Richmond Products, Albuquerque, NM, USA) under the distant viewing condition and either the Titmus stereotest (Stereo Optical Co., Inc., Chicago, IL, USA) or Randot stereotest (Vision Assessment Corporation, Elk Grove Village, IL, USA) under the near viewing condition were performed. Stereoacuity of ≤ 60 arcsec in the Titmus stereotest or ≤ 63 arcsec in the Randot stereo test was defined as “good stereopsis.” More detailed findings of the ophthalmologic examinations are provided in an article describing the KIEMS methodology18.
Statistical analysis was performed using SPSS (version 21.0; IBM Corporation, Armonk, NY, USA). Statistical significance was set at P < 0.05. Bonferroni correction was applied to the P value for subgroup analyses. Mean ages were compared between male and female participants using an independent t-test. Exodeviation angles in the secondary positions and in the right and left head-tilted positions, compared with the exodeviation angle in the primary position, were analyzed using a paired t-test. The differences in the ratios of ocular dominance and fusion control at distant and near fixation conditions were compared using Pearson’s chi-square test.
Data availability
Data supporting the findings of the current study are available from the corresponding author upon reasonable request.
Change history
14 February 2023
A Correction to this paper has been published: https://doi.org/10.1038/s41598-023-29515-x
References
Hoyt, C. S. & Taylor, D. Intermittent exotropia. in Pediatric Ophthalmology and Strabismus 783–791 (Elsevier, 2013).
von Noorden, G. K. & Campos, E. C. Exodeviation. in Binocular Vision and Ocular Motility, 356–376 (2002).
Matsuo, T. & Matsuo, C. The prevalence of strabismus and amblyopia in Japanese elementary school children. Ophthalmic Epidemiol. 12, 31–36 (2005).
Chia, A. et al. Prevalence of amblyopia and strabismus in young singaporean chinese children. Invest. Ophthalmol. Vis. Sci. 51, 3411–3417 (2010).
Pan, C.-W. et al. Epidemiology of intermittent exotropia in preschool children in China. Optom. Vis. Sci. 93, 57–62 (2016).
Goseki, T. & Ishikawa, H. The prevalence and types of strabismus, and average of stereopsis in Japanese adults. Jpn. J. Ophthalmol. 61, 280–285 (2017).
Han, K. E., Baek, S.-H., Kim, S.-H., Lim, K. H., Epidemiologic Survey Committee of the Korean Ophthalmological Society. Prevalence and risk factors of strabismus in children and adolescents in South Korea: Korea National Health and Nutrition Examination Survey, 2008–2011. PLoS ONE 13, e0191857 (2018).
Choi, K. W., Koo, B. S. & Lee, H. Y. Preschool vision screening in Korea: Results in 2003. J. Korean Ophthalmol. Soc. 47, 112–120 (2003).
Govindan, M., Mohney, B. G., Diehl, N. N. & Burke, J. P. Incidence and types of childhood exotropia: A population-based study. Ophthalmology 112, 104–108 (2005).
Hashemi, H. et al. Global and regional prevalence of strabismus: A comprehensive systematic review and meta-analysis. Strabismus 27, 54–65 (2019).
Lavrich, J. B. Intermittent exotropia: Continued controversies and current management. Curr. Opin. Ophthalmol. 26, 375–381 (2015).
Chiu, A. K. C. C., Din, N. & Ali, N. Standardising reported outcomes of surgery for intermittent exotropia: A systematic literature review. Strabismus 22, 32–36 (2014).
Bae, G. H., Bae, S. H. & Choi, D. G. Surgical outcomes of intermittent exotropia according to exotropia type based on distance/near differences. PLoS ONE 14, 1–10 (2019).
Bae, S. H. et al. Postoperative changes of intermittent exotropia type as classified by 1-hour monocular occlusion. PLoS ONE 13, 1–10 (2018).
Feng, X., Zhang, X. & Jia, Y. Improvement in fusion and stereopsis following surgery for intermittent exotropia. J. Pediatr. Ophthalmol. Strabismus 52, 52–57 (2015).
Lee, D. S., Kim, S.-J. & Yu, Y. S. The relationship between preoperative and postoperative near stereoacuities and surgical outcomes in intermittent exotropia. Br. J. Ophthalmol. 98, 1398–1403 (2014).
Kim, H. J. & Choi, D. G. Consecutive esotropia after surgery for intermittent exotropia: The clinical course and factors associated with the onset. Br. J. Ophthalmol. 98, 871–875 (2014).
Kim, D. H. et al. An overview of the Korean intermittent exotropia multicenter study by the Korean association for pediatric ophthalmology and strabismus. Korean J. Ophthalmol. 35, 355–359 (2021).
Nusz, K. J., Mohney, B. G. & Diehl, N. N. Female predominance in intermittent exotropia. Am. J. Ophthalmol. 140, 546–547 (2005).
Buck, D. et al. Presenting features and early management of childhood intermittent exotropia in the UK: Inception cohort study. Br. J. Ophthalmol. 93, 1620–1624 (2009).
Rutstein, R. P. & Corliss, D. A. The clinical course of intermittent exotropia. Optom. Vis. Sci. 80, 644–649 (2003).
Chia, A., Roy, L. & Seenyen, L. Comitant horizontal strabismus: An Asian perspective. Br. J. Ophthalmol. 91, 1337–1340 (2007).
Burian, H. M. & Franceschetti, A. T. Evaluation of diagnostic methods for the classification of exodeviations. Trans. Am. Ophthalmol. Soc. 68, 56–71 (1970).
Kushner, B. J. & Morton, G. V. Distance/near differences in intermittent exotropia. Arch. Ophthalmol. 116, 478–486 (1998).
Watts, P., Tippings, E. & Al-Madfai, H. Intermittent exotropia, overcorrecting minus lenses, and the newcastle scoring system. J. AAPOS 9, 460–464 (2005).
Mohney, B. G. & Holmes, J. M. An office-based scale for assessing control in intermittent exotropia. Strabismus 14, 147–150 (2006).
Kim, H., Kim, D. H., Ahn, H. & Lim, H. T. Proposing a new scoring system in intermittent exotropia: Towards a better assessment of control. Can. J. Ophthalmol. 52, 235–239 (2017).
Porac, C. & Coren, S. The dominant eye. Psychol. Bull. 83, 880–897 (1976).
Clarke, M. P. Intermittent exotropia. J. Pediatr. Ophthalmol. Strabismus 44, 153–159 (2007).
von Noorden, G. K. & Campos, E. C. Examination of the Patient-III. in Binocular Vision and Ocular Motility, 211–45 (2002).
Romanchuk, K. G., Dotchin, S. A. & Zurevinsky, J. The natural history of surgically untreated intermittent exotropia-looking into the distant future. J. AAPOS https://doi.org/10.1016/j.jaapos.2006.02.006 (2006).
Pediatric Eye Disease Investigator Group et al. Three-year observation of children 3 to 10 years of age with untreated intermittent exotropia. Ophthalmology 126, 1249–1260 (2019).
Santiago, A. P., Ing, M. R., Kushner, B. J. & Rosenbaum, A. L. Intermittent exotropia. In Clinical Strabismus Management: Principles and Surgical Techniques (eds Santiago, A. P. & Rosenbaum, A. L.) 163–175 (Saunders, 1999).
Acknowledgements
The Korean Intermittent Exotropia Multicenter Study (KIEMS) was initiated and financially supported by the Korean Association of Pediatric Ophthalmology and Strabismus.
Author information
Authors and Affiliations
Consortia
Contributions
Design and conduct of the study (D.H.K., J.H.J., M.Y.C., J-M.H., S.J.K., Y-h.L., S.-H.H., D.G.C.); collection of data (D.H.K., J.H.J., M.Y.C., J-M.H, S.J.K., Y-h.L., S.-H.H., D.G.C.); analyses and interpretation of data (D.H.K, J.H.J., M.Y.C., J-M.H., S.J.K., Y-h.L., S.-H.H., D.G.C.); writing the manuscript (D.H.K., D.G.C.); critical revision of the manuscript (D.H.K., J.H.J., M.Y.C., J.-M.H, S.J.K., Y-h.L., S.-H.H., D.G.C.); and final approval of the manuscript (D.H.K., J.H.J., M.Y.C., J.-M.H., S.J.K., Y-h.L., S.-H.H., D.G.C.).
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this Article was revised: The original version of the Article contained errors in the Consortia author list of The Korean Association of Pediatric Ophthalmology and Strabismus (KAPOS), where author names Dong Gyu Choi and Dae Hee Kim were duplicated in the KIEMS writing committee, and Jae Ho Jung, Mi Young Choi, Jeong Min Hwang, Su Jin Kim, Yeon hee Lee, Sueng Han Han and Dong Gyu Choi were duplicated in KIEMS investigators in the KAPOS.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kim, D.H., Jung, J.H., Choi, M.Y. et al. A cross-sectional study of ophthalmologic examination findings in 5385 Koreans presenting with intermittent exotropia. Sci Rep 13, 1329 (2023). https://doi.org/10.1038/s41598-023-28015-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-28015-2
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
