
Abstract
Objectives
A remarkable increase in the number and proportion of surgical patients with acute acquired concomitant esotropia (AACE) has been noted in our hospital in recent years. We aimed to analyse the clinical characteristics and associated risk factors of this increasing number of strabismus in last 5 years.
Methods
Medical information was obtained in 62 AACE patients and 73 orthotropic patients as control group completed questionnaires and examination items from March 2017 to May 2020. Data included age at onset, refractive error, angle of deviation, binocular vision, eye care habits, and optical quality of spectacles.
Results
Of the 62 AACE patients, the mean ± standard deviation age at onset was 25.3 ± 8.5 years, with 47 (75.8%) cases showing myopia, 9 (14.5%) showing emmetropia, and 6 (9.7%) showing hypermetropia. Among the AACE patients, 35 (56.5%) performed >8 h of close work daily and 36 (58.1%) reported late-night use of digital devices. When compared with the control group, the risk factors identified for AACE included long durations of close work (odds ratio [OR], 11.72; 95% confidence interval [CI], 3.53–38.91; P < 0.001) and immoderate late-night use of digital devices (OR, 14.29; 95% CI, 4.10–49.72; P < 0.001).
Conclusion
Our study demonstrated that young adults accounted for the majority of the growing number of individuals affected by AACE in last 5 years, and excessive close visual activities and immoderate late-night use of digital devices were found to be associated with the onset of AACE.
Similar content being viewed by others

Introduction
Acute acquired concomitant esotropia (AACE) is thought to be an uncommon presentation of concomitant esotropia, which has a late age of onset, minimal accommodative element and good potential for binocular cooperation [1,2,3,4]. The proportion of late sudden-onset esotropia in children strabismus was reported to be 0.3% [5]. The aetiology of AACE remains elusive, as does the reason why concomitant esotropia occurs in patients whose bilateral visual acuity and binocular vision show effective development. Previous attempts to define its classification and postulate its pathogenesis are based on the clinical characteristics of a small number of cases. However, within our hospital (Zhongshan Ophthalmic Center, ZOC) we have observed a marked increase in the number and proportion of surgical patients with AACE in recent years. Un-published internal data tracking at our institution indicated that AACE surgery accounted for only 0.26% (24/9109) of all strabismus surgeries in our hospital from October 2010 to November 2014, while this ratio increased to 1.81% (189/10399) from January 2015 to April 2018 and 4.71% (258/5472) from May 2018 to December 2019. The reason for this striking increase remains unknown. In this study, we paid specific attention to patients’ comprehensive medical histories, including eye-care habits and optical quality of spectacles, to describe the clinical characteristics and investigate the potential risk factors for the onset of AACE in last 5 years.
Materials and methods
This was a retrospective case–control study involving 62 AACE patients who visited Dr. Chen at the ZOC from March 2017 to May 2020 and 73 orthotropic volunteers who were recruited from schools and companies. This study adhered to the tenets of the Declaration of Helsinki and was approved by the ethics committee of the ZOC. Written informed consent was obtained from all patients and volunteers or their guardians.
Patients
The inclusion criteria for AACE patients were as previously reported [3]: (1) concomitant esotropia with acute onset (deviation in all directions of gaze differing by ≤2 prism dioptres [PD] when primary deviations were less than 20PD and by ≤5PD when primary deviations were more than 20PD, (2) an accompanying diplopia or visual confusion, (3) best-corrected visual acuity of not less than 0.5 in each eye and (4) ≧5 years old at the time of onset. Patients were excluded from the study if they had a reduction of >10PD in their esotropia with a full hyperopic spectacle correction for 1 month or if inferior displacement of the lateral rectus muscle was revealed in their orbital images or if they had diplopia or visual confusion before 2015. The inclusion criteria for control volunteers: (1) best-corrected visual acuity of not less than 0.5 in each eye, (2) orthotropia on cover test, (3) no diplopia or asthenopia, (4) no obvious ocular diseases except for refractive error, (5) 5–50 years old. Those with a history of strabismus, amblyopia, or ocular surgery were also excluded from both the patient and control group.
General information, additional medical information and ophthalmological examination
General information derived from the medical records included age, age at diplopia onset, gender and occupation. The age at onset was determined by the ophthalmologist according to the medical history, past ocular records and patient photographs. Additional medical information was obtained from questionnaires for AACE patients and control volunteers. These questionnaires included the type and duration of close visual activities (<50 cm), the frequency of weekly digital device use late at night, and whether the individual often used their glasses.
Comprehensive ophthalmologic and orthoptic examinations were performed by Dr. Chen. Cycloplegic refraction was performed after administration of 1% atropine ointment once daily for 3 days in young patients with AACE (<7 years old), while 1% cyclopentolate eye drops were administered three times 5 min apart for the control group and AACE patients older than 7 years. A full cycloplegic refraction was prescribed for AACE patients with refractive errors >1.0 dioptre (D). The prism and alternate cover test (PACT) were used to determine total deviations at 6 m and 33 cm fixation, and the simultaneous prism cover test was used to determine the manifest deviation. A synoptophore was used to evaluate the 3 grades of binocular single vision. All AACE patients received brain and orbital computed tomography (CT) scans or magnetic resonance imaging (MRI). Comprehensive medical histories were reviewed and neurological examinations were performed for cases with intermittent esotropia or variable deviations to rule out cyclic esotropia and myasthenia gravis. In addition, spectacles were checked to assess optical quality for both control volunteers and AACE patients.
Potential risk factors were based on the AACE patients’ eye care habits, living habits and plausible prior hypotheses [1, 6] and then were applied to design a questionnaire and examination items (Table 1).
Statistical analysis
Continuous variables were presented as the mean ± standard deviation (SD) and analysed using the independent samples t-test. Classification data were analysed using the chi-square test. The risk factors for AACE were analysed using multiple logistic regression analysis. The feature variables were considered as odds ratio (OR) having a 95% confidence interval (CI) and P value. Statistical analysis was performed using the SPSS 20.0 software for Windows (SPSS China, Inc.). Two-tailed P values of <0.05 were considered statistically significant.
Results
Baseline characteristics
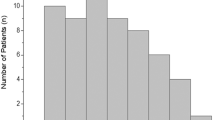
62 AACE cases (45 males and 17 females) were included. Overall, the mean ± SD age at onset was 25.3 ± 8.5 years (range: 5.0–47.0 years), with 3(4.8%) patients 5–9 years of age, 4 (6.5%) patients 10–17 years of age, 42(67.7%) patients 18–30 years of age and 13(20.9%) patients older than 30 years. The duration from the initial onset of diplopia to the first clinic visit ranged from 2 months to 51 months. The number of patients suffering from diplopia (both at distance and near) was 53 (85.5%), while 8 (12.9%) patients had distance diplopia and single vision at near, and 1 (1.6%) initially had distance diplopia and later developed near diplopia. Two patients (3.2%) initially had intermittent diplopia that transitioned to constant diplopia within a few months. There were 32 (51.6%) patients whose occupations required excessive near work, including college students, precision parts installers, staff accounts, office staff members, network practitioners and E-commerce employees. Two patients had a history of fever before the onset of diplopia. None of the cases involved occlusion therapy, head injury, psychological shock, heroin intake or withdrawal, or family histories of strabismus.
The corrected visual acuity of all patients was ≧0.8. Slitlamp and funduscopy examinations were unremarkable, and ocular versions and ductions were normal in all patients. There were no statistically significant differences in the deviations with corrected spectacles between near (35.3 ± 14.7PD) and distance (34.5 ± 12.8PD) fixations (t-test, P = 0.41). All AACE patients showed normal brain and orbital CT or MRI scans, in which inferior displacement or marked elongation and thinning of lateral rectus muscle was not revealed
Refractive status in different age groups
Among the 62 AACE cases, 6 (9.7%) were hyperopic, 9 (14.5%) were emmetropic, and 47 (75.8%) had myopia. Hypermetropia ranged from +0.75 D to +2.5 D (mean ± SD = + 1.3 D ± 0.7 D), while myopia ranged from −0.75 D to −10.25 D (−4.5 ± 2.3 D). Among the myopia cases, the refraction of 12 (25.5%) patients was <3.0 D, in 22 (46.8%) it was between 3.0–6.0 D, and in 13 (27.7%) it was >6.0 D. Hyperopia was more frequently observed in young patients (5–9 years of age), while myopia was more common in patients ≥18 years of age (Table 2). In patients with AACE, the refractive status ratios differed significantly among the different age groups (χ2 test, P < 0.001).
Relationships among diplopia, angle of deviation, and refractive status
The distance deviation (21.4 ± 11.3PD) of the eight patients who experienced diplopia at distance but fusion at near was significantly less (t-test, P < 0.001) than those with diplopia at both distance and near (36.8 ± 13.0PD). Deviations of ≤20PD were present in 16 cases, while 46 patients showed deviations of >20PD. There were no statistically significant differences between these two groups in the ratios of refractive status (χ2 test, P = 0.77) (Table 3).
Treatment and prognosis
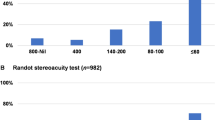
A total of 16 patients with deviations ≤20 PD received conservative treatments such as prism prescription, spectacle adjustment, and restriction of their close work. Following conservative treatments, two (12.5%) patients recovered, three subsequently underwent surgery for deviation enlargement, and others remained stable. Patients with deviations >20 PD underwent surgery after more than 3 months of observation or conservative treatment. Surgical target angle was augmented by an additional 5–10 PD to the distance deviation determined by PACT and surgical dosage followed the table recommended by Wright et al. [7]. All double vision or binocular vision in these patients was resolved or improved following surgery except for two with residual esotropia. 96.8% (60/62) showed normal retinal correspondence or fusionor stereopsis in the synoptophore following conservative or surgical correction.
Risk factors associated with the onset of AACE
Additional medical information and examinations were obtained in 62 patients and 73 control volunteers. Those two groups were matched for age, gender, and corrected visual acuity (Table 4).
Of these 62 patients, 35 (56.5%) reported more than 8 h of daily near-work for more than 3 months, while only 7 (9.6%) comparable cases were present in the control group. The number of patients participating in late-night (after 12 a.m.) digital device use for not less than twice a week and for longer than 3 months was 36 (58.1%), while there were only 12 (16.4%) such cases in the control group. In addition, nine AACE patients showed an oversized pupillary distance of ≧3 mm in their frame spectacles, ten had overcorrection for myopia of ≧0.5 D, two showed a misalignment of ≧10° in the astigmatism axis and nine AACE patients with myopia did not wear glasses or wear glasses for less than 4 h a day. Results from the multiple logistic regression analysis indicated that the risk factors included long durations of close visual work (odds ratio [OR], 11.72; 95% confidence interval [CI], 3.53–38.91; P < 0.001) and immoderate late-night use of digital devices (OR, 14.29; 95% CI, 4.10–49.72; P < 0.001). No risks were found to be associated with an oversized pupillary distance in spectacles, myopic overcorrection, uncorrected myopia, or myopia (Table 5).
Discussion
AACE was first defined by Burian and Miller [1] and categorised into three types based upon hypothetical causes and the refractive status. These include: (1) Swan type, which results from interruption of binocular vision, (2) Franceschetti type, characterised by low hyperopia and minimal accommodative element, and (3) Bielschowsky type, present in patients with uncorrected myopia (≤5 D), which is thought to be associated with an increased tonus of the medial rectus. Subsequently, brain tumours, heroin withdrawal, decompensated esophoria and excessive smartphone use have also been reported to be associated with the onset of AACE based on limited number of cases [3, 6, 8,9,10,11,12,13,14,15,16,17]. However, we have noticed that the incidence of AACE has a tendency to increase in recent years, and it does not seem to be fully explained by past views. Therefore, larger cases and controls were included in our studies to further explore the clinical characteristics, potential risk factors and mechanisms that may be involved with the onset of AACE. As some patients with partially accommodative esotropia, acquired nonaccommodative esotropia, sagging eye syndrome and heavy eye syndrome can also have double vision, all these types of strabismus were excluded in the study.
Patients in present study showed clinical features of a relatively late age of onset and potentially normal binocular vision. In our study, 88.7% of the patients experienced AACE onset at ≧18 years of age, and 96.8% of the AACE patients showed normal retinal correspondence or fusion or stereopsis in the synoptophore following treatment. In addition, myopia was found to be the most common condition in AACE, followed by emmetropia and hyperopia. There were no significant differences in ratios of refractive status between the small and large deviation groups; however, statistically significant differences were present among the different age groups. Patients presenting with diplopia at distance but fusion at near showed deviations that were significantly less than those with diplopia at both distance and near. Based on these findings, it seems that refractive status may be associated with the age of onset and fusion at near as related to small deviations. Therefore, it does not appear that refractive status should serve as a basis for AACE classification.
Excessive close visual activities were found to be a risk factor responsible for the onset of AACE in the current study. Notably, 32 of the patients (51.6%) had occupations associated with close work (less than 50 cm) and 35 (56.5%) patients reported more than 8 h of daily close work for longer than 3 months. Close work in this study included use of digital devices, book reading and assembly/repair of precision instruments. All of these activities require use of near visual acuity. Similarly, in Lee’s study [6], 12 of 19 AACE cases were identified as smartphone users. In recent years, digital devices have become more a part of daily life, work, and study and have become popular outlets for entertainment among adolescents and young adults in China. As we found this to be a risk factor, this increase in digital-device use may provide one explanation for the rapid increase in AACE onset in young adults. Skeletal muscles have been shown to adapt and respond to mechanical and biochemical stimuli [18], and adaptations in extraocular muscle length or structure have also been reported [19, 20]. As a result, the mechanical tonus of medial rectus muscles can increase and disrupt motor fusion following excessive close visual activities and thus may lead to the development of AACE.
Late-night video display use was identified as another risk factor responsible for the onset of AACE in our study. Of the 62 patients with extensive documented histories prior to the presence of diplopia, 36 patients (58.1%) indicated a habit of late-night use not less than twice a week of digital devices such as smartphones, computers, or iPads. Such disruptions in biological rhythms have been shown to exert adverse impacts on brain function [21]. In addition, visual motion processing and coordinated eye movements were reported to be significantly impaired when performed after acute sleep loss and circadian misalignment [22]. Therefore, these late-night visual activities may not only aggravate the burden of motor fusion, but also impact sensory fusion, leading to the occurrence of AACE.
Nineteen of the 62 patients were wearing spectacles with optical quality problems when their diplopia occurred, including wider pupillary distance, overcorrection for myopia, and incorrect astigmatism axis. Though no risks were found to be related to oversized pupillary distance or overcorrection for myopia in this study, two patients recovered following spectacle adjustments and restrictions of their close work: one patient had an overcorrection of 0.75 D for myopia and 1500 of misalignment in the astigmatism axis; the other patient had reversed left (−5.0 D) and right (−4.25 D) myopic powers. The common features of these two cases include incorrect spectacle prescriptions, more than 4 h of daily smartphone use, late-night smartphone use once or twice a week, small deviation, and a less-than-4-month period prior to accepting treatment. It seems that patients with small deviations can recover if these risk factors are corrected in time. Therefore, incorrect spectacle prescriptions may increase the burden of sensory or motor function and, in this way, also be a potential risk factor for the onset of AACE.
Myopia or uncorrected myopia was not shown to be a potential risk factor for AACE in the study. As a high rate of myopia was present in both AACE and control patients, it would not be able to assess an association between AACE and myopia. The prevalence of myopia in China is increasing. For example, a study from a city in southern China reported the prevalence of myopia among high school students increased from 79.5% in 2001 to 87.7% in 2015 [23]. This might be the explanation of the high rate of myopia in both groups but not the striking increase of AACE. Cohort studies are needed to further clarify the relationship between myopia and AACE.
This was a preliminary study on the risk factors associated with AACE. The main limitation was that the number of cases in the risk-factor analysis was relatively small. Prospective cohort studies are warranted to further clarify the risk factors related to AACE. Despite these limitations, we believe our findings provide valuable insight regarding the increasing incidence and the underlying mechanisms involved in AACE.
In conclusion, we do not consider AACE to be a single cause; there are numbers of factors that may deteriorate sensory or motor fusion and contribute to this condition. Young adults were found to be the main group affected in the growing numbers of AACE in last 5 years. Moreover, excessive close visual activities and immoderate late-night digital device use were found to be associated with AACE onset. Therefore, reductions in close visual activities, especially late-night use of digital devices, and high-quality spectacle prescriptions are recommended to prevent the onset of AACE.
Summary
What was known before
-
The aetiology of AACE remains elusive, as does the reason why concomitant esotropia occurs in patients whose bilateral visual acuity and binocular vision show effective development.
What this study adds
-
Excessive close visual activities and immoderate late-night use of digital devices were found to be associated with growing numbers of acute acquired concomitant esotropia in last 5 years.
References
Burian HM, Miller JE. Comitant convergent strabismus with acute onset. Am J Ophthalmol. 1958;45:55–64.
Clark AC, Nelson LB, Simon JW, Wagner R, Rubin SE. Acute acquired comitant esotropia. Br J Ophthalmol. 1989;73:636–8.
Chen J, Deng D, Sun Y, Shen T, Cao G, Yan J, et al. Acute acquired concomitant esotropia: clinical features, classification, and etiology. Medicines. 2015;94:e2273.
Spierer A. Acute concomitant esotropia of adulthood. Ophthalmology. 2003;110:1053–6.
Mohney BG. Common forms of childhood strabismus in an incidence cohort. Am J Ophthalmol. 2007;144:465–7.
Lee HS, Park SW, Heo H. Acute acquired comitant esotropia related to excessive Smartphone use. BMC Ophthalmol. 2016;16:37.
Wright KW, Strube, Yi Ning J. Color atlas of strabismus surgery: strategies and techniques., 4th. edn. © Springer Science+Business Media: New York; 2015.
Ali MH, Berry S, Qureshi A, Rattanalert N, Demer JL. Decompensated esophoria as a benign cause of acquired esotropia. Am J Ophthalmol. 2018;194:95–100.
Williams AS, Hoyt CS. Acute comitant esotropia in children with brain tumors. Arch Ophthalmol. 1989;107:376–8.
Lee JM, Kim SH, Lee JI, Ryou JY, Kim SY. Acute comitant esotropia in a child with a cerebellar tumor. Korean J Ophthalmol. 2009;23:228–31.
Hoyt CS, Good WV. Acute onset concomitant esotropia: when is it a sign of serious neurological disease? Br J Ophthalmol. 1995;79:498–501.
Simon JW, Waldman JB, Couture KC. Cerebellar astrocytoma manifesting as isolated, comitant esotropia in childhood. Am J Ophthalmol. 1996;121:584–6.
Versino M, Hurko O, Zee DS. Disorders of binocular control of eye movements in patients with cerebellar dysfunction. Brain. 1996;119:1933–50.
Liu GT, Hertle RW, Quinn GE, Schaffer DB. Comitant esodeviation resulting from neurologic insult in children. J AAPOS: Off Publ Am Assoc Pediatr Ophthalmol Strabismus. 1997;1:143–6.
Patel VR, Zee DS. The cerebellum in eye movement control: nystagmus, coordinate frames and disconjugacy. Eye. 2015;29:191–5.
Sutter FK, Landau K. Heroin and strabismus. Swiss Med Wkly. 2003;133:293–4.
Firth AY. Heroin withdrawal as a possible cause of acute concomitant esotropia in adults. Eye. 2001;15:189–92.
Lieber RL, Roberts TJ, Blemker SS, Lee SSM, Herzog W. Skeletal muscle mechanics, energetics and plasticity. J Neuroeng rehabilitation. 2017;14:108.
Scott AB. Change of eye muscle sarcomeres according to eye position. J Pediatr Ophthalmol strabismus. 1994;31:85–8.
Wright WW, Gotzler KC, Guyton DL. Esotropia associated with early presbyopia caused by inappropriate muscle length adaptation. J AAPOS: Off Publ Am Assoc Pediatr Ophthalmol Strabismus. 2005;9:563–6.
Facer-Childs ER, Campos BM, Middleton B, Skene DJ, Bagshaw AP. Circadian phenotype impacts the brain’s resting-state functional connectivity, attentional performance, and sleepiness. Sleep. 2019;42:zsz033.
Stone LS, Tyson TL, Cravalho PF, Feick NH, Flynn-Evans EE. Distinct pattern of oculomotor impairment associated with acute sleep loss and circadian misalignment. J Physiol. 2019;597:4643–60.
Chen M, Wu A, Zhang L, Wang W, Chen X, Yu X, et al. The increasing prevalence of myopia and high myopia among high school students in Fenghua city, eastern China: a 15-year population-based survey. BMC Ophthalmol. 2018;18:159.
Acknowledgements
We would like to thank Dr. Zhigang Fan for his valuable comments on our paper and Editage (www.editage.com) for English language editing.
Funding
The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
MZ, YT and JC designed the clinical study. MZ, YT and JC recruited volunteers. MZ, YT, ZW, TS, XQ, JY and JC analysed and interpreted the dada. MZ, YT, and JC wrote the manuscript. JC directed the project.
Corresponding author
Ethics declarations
Competing interests
There are not any competing financial interests in relation to the present work described.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Zhu, M., Tang, Y., Wang, Z. et al. Clinical characteristics and risk factors of acute acquired concomitant esotropia in last 5 years: a retrospective case–control study. Eye 37, 320–324 (2023). https://doi.org/10.1038/s41433-022-01939-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41433-022-01939-1
This article is cited by
-
Clinical characteristics of acute acquired concomitant esotropia before and after the COVID-19 pandemic: a retrospective analysis
Graefe's Archive for Clinical and Experimental Ophthalmology (2024)
-
Comment on: Clinical characteristics and risk factors of acute acquired concomitant esotropia in last 5 years: a retrospective case—control study
Eye (2023)
