
Abstract
Cannabis use is a common risk factor for psychoses. But although prevalence of consumption as well as potency of cannabis increased, the incidence of schizophrenia remained stable. The discontinuation hypothesis suggests that a potential increase of psychoses incidence may be relativized by more frequent cessation of consumption due to higher rates of adverse psychosis-like intoxication effects (PLE), caused by stronger cannabis. A mixed methods online survey was administered to 441 current and past users to analyze the predictive impact of different acute intoxication effects regarding abstinence motivation/cessation of use. Our hypothesis was that PLE would be experienced as the most aversive intoxication effect and therefore have the highest predictive significance. Possible confounds were included (craving, patterns of consumption and sociodemographics). Further analyzes compared past versus current users regarding the quality of intoxication effects, suggesting that past users retrospectively experienced more unpleasant experiences than current users. Free-text data explored subjective reasons for abstinence. We found that paranoid/dysphoric intoxication effects were most predictive for abstinence motivation. Less predictive were psychosis-like intoxication effects such as hallucinations. Group comparisons revealed significant more unpleasurable and less positive intoxication effects in past users compared with current users. Current users with the intention to stop consumption showed significantly more paranoia/dysphoria intoxication compared to users with no intention to stop use. As a conclusion, different intoxication experiences have different effects on abstinence motivation and substance use behavior. They therefore provide a focus that should be increasingly integrated into treatment concepts.
Similar content being viewed by others


Introduction
Psychotic experiences range from schizophrenia to psychotic-like experiences (PLE) in the general population without an underlying mental disorder1,2. Around 2–16% of the general population report lifetime PLE, such as hallucinations, delusions or depersonalization, usually transient or attenuated in nature3. Such experiences are associated with increased risk for psychosis2 and therefore may reflect an enhanced vulnerability4.
Cannabis users report various acute intoxication effects that range from relaxation to stimulation and from euphoria to anxiety. In higher doses and/or in vulnerable users, PLE may also occur in the context of acute intoxication5,6. According to preliminary estimates, cannabis users who experience PLE in the context of acute intoxication have an up to fivefold increased risk of developing psychosis compared to users without PLE experiences7. Among the latter, the risk of psychosis was similar to that of individuals who never use cannabis7. To explain the relation between cannabis and PLE, a complex interplay between neurobiological vulnerability of psychosis and cannabinoids or the endogenous cannabinoid system (ECS) is assumed8,9.
During the past decade, past-month prevalence of cannabis use increased by 27% in European adults up to 3.9%10, especially among younger people11. Concurrently, concentrations of delta-9-tetrahydrocannabinol (THC) in cannabis worldwide increased by 0.29% per year12. Such enhanced consumption of high-potency cannabis, considering complex interaction effects between cannabinoids and psychosis, leads to the suggestion that the incidence of schizophrenia will increase. Instead, incidence and prevalence of schizophrenia has remained quite stable13. To explain the unexpected stability of incidence rates, the discontinuation hypothesis is discussed14. Accordingly, high-potency cannabis is suggested to induce more PLE in users – and instead of continued use, which could be associated with a higher number of psychotic decompensations, increased adverse PLE-intoxication experiences would have led to increased cessation of use. Such discontinuation, especially in vulnerable persons with high sensitivity to cannabinoids may put a potential increase in incidence of schizophrenia into perspective14. Accordingly, it was confirmed that first-manifest schizophrenia patients who stopped consumption of cannabis subsequently had fewer psychotic relapses compared with patients who continued use15.
Thus, the central question is whether adverse intoxication experiences, and PLE in particular, lead to increased cessation of cannabis use, or at least to increased motivation to reduce use. Most previous studies on reasons for cessation of substance use or change motivation disregard acute intoxication effects. Continued use is often associated with social context, poor mental health, prior drug use and school failure14. Cessation is usually discussed as a consequence of increasing age and maturity16. As a psychological reason for maintaining substance use, craving is often considered as a predictor of relapse, frequency of use, and low abstinence rates17. In mental disorders, craving generally appears to be a factor maintaining substance use, according to the affect regulation hypothesis18. This is supported by the fact that substance use is generally more common in psychiatric patients than in the general population19. Accordingly, patients use drugs to reduce nonspecific dysphoric states. The corresponding type of craving is called relief craving, in contrast to reward craving, the hedonistic urge to use drugs17. The disregard of acute intoxication effects is also reflected by the fact that in German-speaking countries it was not even possible to operationalize these effects until the recent publication of a corresponding instrument20. However, in recent years, international research has turned to the subject, whose significance can be derived from the theory of operant learning: Accordingly, acute consequences of a behavior explain whether or not the behavior will be exhibited again, and the more immediately a reinforcement or punishment follows a behavior, the more predictively effective is the operant effect21. Pleasant acute intoxication experiences are accordingly associated with higher frequency of use, low abstinence motivation, and later dependence22,23,24. However, it is unclear whether the reverse is also true, that negative acute effects reduce or even terminate substance use behavior. In the case of addictive behaviors, additional neurobiological and psychological aspects come in to explain the maintenance of the behavior25. Accordingly, acute effects were found to be predictively relevant, particularly in the early stages of a substance use history, associating early positive, but not negative, acute use effects with continued heavy use23,26. At later stages of use, acute effects appear to be less effective. In summary, findings on adverse intoxication effects regarding consumption behavior are heterogeneous, ranging from decreased27 to increased use24,28. This heterogeneity may be explained by the fact that unpleasant intoxication effects represent a wide range of experiences from sleepiness, confusion and nausea to PLE. Experts suggest that especially PLE may be most aversive for users and PLE would have the greatest impact on consumers behavior14. In a recently reported study, authors confirmed their hypothesis that especially cannabis-induced PLE are associated with cessation of use14. If this finding can be replicated, this would be quite relevant, as close to 15% of users report such experiences29, which are also associated with increased risk of psychosis7.
Since abstinence motivation is a precondition for cessation of cannabis use, we first investigate the relation between different potentially predictors for stages of change motivation in a non-clinical sample. Of primary predictive interest are different intoxication effects. Our hypothesis is that aversive acute intoxication effects (and especially PLE) are associated with stronger abstinence motivation compared to positive effects. Based on the findings presented above, we also investigate the predictive value of sociodemographic variables, craving, and cannabis use parameters (frequency of use, duration of use and age at first use). Second, we compare three groups in terms of potential factors influencing cannabis use: Individuals who have stopped consumption, present users with intention to stop using, and present users without intention to change. Past users will be asked to retrospectively indicate their former consumption experiences. Our hypothesis is that aversive experiences of intoxication are found to be most pronounced among former users, followed by users with intention to change use. Regarding users without intention to change use, we hypothesize that positive intoxication experiences are more prominent.
Methods
We developed a web-based version of the questionnaires used, referring to other research groups that use electronic versions in online samples and report acceptable psychometric properties30,31.
Our sample consisted of healthy people in the general population who volunteered to participate in the survey. Before the survey started, participants were explicitly informed by an introductory text that participation was voluntary and could be discontinued at any time. It was pointed out that only complete data sets would be processed. It was also emphasized that the data collection would be completely anonymous, i.e. no data would be collected and/or stored that could allow any reference to the individual person. We informed that the data would be used exclusively for scientific purposes. Finally, participants could only start the survey if they gave their written consent, by marking a corresponding field, placed at the end of the information page. This way, written consent was obtained from all participants included in the study. We did not obtain a further vote of an ethics committee in accordance with the regulations applicable in Germany, as we did not investigate a clinical trial with patients or any other vulnerable group.
Sample selection and study procedures
Quantitative data were collected online using three self-report questionnaires via the survey site Unipark. In addition, qualitative data were collected using free-text fields, for a deeper understanding of abstinence motivation/reasons to stop cannabis use. The survey took place between November 2020 and April 2021. Recruitment of participants was performed by advertising the study via public notices. In addition, the link to the survey was sent out via social media (Facebook, Twitter, Reddit) and relevant cannabis forums. Inclusion criteria were that participants were German-speaking adults (minimum age of 18 years) and that they had previously used cannabis. No reward in form of an incentive was given.
Survey questionnaires/measures
Sociodemographic data, substance use data and mental health
Information on sociodemographics included age, gender, education level and occupation status. Lifetime diagnosis of a mental disorder was recorded as self-report using a dichotomous item (yes/no; wording of the question: “have you ever been diagnosed with a mental disorder?”). Cannabis use patterns were collected, i.e. age at onset of use, time since last dose (days) and abstinent weeks within the last year, duration of regular use (month) and average frequency of use (joints per month). Regarding the latter, past users were asked to estimate their average use at the time of active use. The use of substances other than cannabis was also recorded by means of a dichotomous item (yes/no).
Cannabis intoxication effects (CanTox-17)
CanTox-17 is the German version of the original Cannabis Experiences Questionnaire (CEQ). Developed initially by Barkus and colleagues32, different English-language factor solutions have been subsequently published31,33,34. The German version was developed by our group20 and it consists of three negative dimensions and one positive dimension of acute cannabis intoxication effects: (1) “psychotic-like experiences/loss of reality” (feeling threatened, hearing voices, losing ones sense of reality, feeling like going crazy); (2) “paranoia/dysphoria” (feeling paranoid, anxious, nervous, depressed); (3) “confusion/disorientation” (speech becoming slurred, time slowing down, disturbed in thinking, not aware of what was going on); (4) “euphoria/creativity” (understanding the world better, feeling energized, full of ideas and more creative). Items were scored on a Likert scale with five graduations. Since CanTox-17 was just developed and evaluated within in a recent study20, the presented factor structure is to be considered as preliminary result. So, we again analyzed and replicated sufficient goodness-of-fit indices of the instrument and the internal consistency of the factors (cronbach´s alpha). Since the χ2-test is considered to be sample sensitive, the ratio between χ2- and the degrees of freedom was formed (χ2/df), with good to acceptable fit that is suggested to be 0 ≤ χ2 /df ≤ 335. A χ2/df value of 1.91 in the previous evaluation study and 2.81 in the present study represent a good to acceptable fit. The root mean square error of approximation (RMSEA) < 0.08 indicates satisfactory model fit. The respective value of 0.058 within the evaluation study and the present value of 0.064 are in line with this criterion. In accord with Browne and Cudeck’s and Vandenberg and Lance criterion36,37, the comparative fit index (CFI), and the Tucker Lewis index (TLI) each > 0.90 also indicate a satisfactory model fit. The preliminary evaluation study identified a CFI = 0.93 and TLI = 0.92, compared with CFI = 0.92 and TLI = 0.91 in the present study. To determine the internal consistency of the four factors, Cronbach’s alpha was applied38. Within the previous evaluation study, values ranged between 0.74 and 0.78, whereas the present data reveal values between 0.70 and 0.79, representing an acceptable to good internal consistency.
Craving parameters
Cannabis craving was assessed using the Cannabis Craving Screening-7 questionnaire (CCS-7)39. CCS-7 consists of seven items, three items for the (1) “reward dimension”, and four items for the (2) “relief dimension” of craving. Participants had to rate each item on a Likert-scale with seven graduations. Various studies indicate that these dimensions can be reliably measured with the CCS-717,39.
Stages of abstinence motivation
Motivation for abstinence was determined by using the SOCRATES (Stages of Change Readiness and Treatment Eagerness Scale) questionnaire consisting of 19-items related to three subscales, each capturing different aspects of patients’ motivation. These are (1) “ambivalence” (indicator for the process of balancing two options—namely, to remain or become abstinent versus continued substance use), (2) “recognition” (indicator for awareness of problem), and (3) “taking steps” (indicator for the concrete efforts to remain abstinent)40, Participants rate each item on a likert-scale with five graduations. In their assessment of psychometric criteria of the original version, authors conclude that SOCRATES questionnaire can be considered promising41. The instrument was subsequently used many times in empirical investigations.
Qualitative data on reasons to stop cannabis use
Qualitative methods (free text input fields in the questionnaire) were used to collect the specific reasons of past cannabis users that led them to stop consumption.
Statistics
First, preparatory analyzing ensured the quality of applied instruments and managed missing values. Analyzing missing values revealed a proportion of missing values of 0.71% (minimum value = 0.2%; maximum value = 2.6%) at the case and variable levels. To analyze random occurrence of missing values, Little’s MCAR test was performed. Values of the questionnaires did not reveal significance as predicted. Consequently, missing values could be imputed using the expectation–maximization method. Respective CanTox-17 questionnaire, we analyzed goodness of fit criteria (see section above).
Second, we aimed to identify predictors of abstinence motivation. In a first step, we correlated potential predictors with each of the three stages of SOCRATES change motivation. Following findings of other groups14, key potential predictors were different cannabis intoxication effects, but also sociodemographic parameters such as age and gender. In addition, as craving is considered a key indicator of consumption relapse, both relief and reward craving were included in the analyzes. Finally, we analyzed specific cannabis use patterns. Those potential predictors that correlated significantly with motivational stages were then integrated into multiple stepwise regression analyzes with SOCRATES-dimensions as criterion (dependent variables). Cohen’s f2 was calculated as the effect size42, with a value of 0.02 corresponding a small effect, 0.15 representing a medium effect, and 0.35 representing a strong effect.
Third, complementing findings on abstinence motivation according to SOCRATES-data and following previous findings of expert colleagues14, we compared acute and past cannabis users. We divided the sample into three groups: Group 1 integrated acute cannabis users without intention to quit. Group 2 consisted of acute users with intention to discontinue cannabis use, and group 3 consisted of individuals who had already discontinued consumption. Descriptive analyzes and significance tests examined whether the groups differed significantly with respect to sociodemographic parameters, i.e., whether they were comparable with respect to the target parameters. The latter focused on group comparison with respect to acute cannabis intoxication effects, craving, and cannabis use parameters. Finally, we compared groups using multiple analyzes of variance (MANOVAs) including post-hoc analyzes with pairs of groups. To indicate the effect sizes, partial eta2 was calculated.
Quantitative analyzes were complemented by qualitative (free-text) information provided by past users in the questionnaire on their reasons for discontinuing consumption. Statements were transcribed, collated and inductively coded by an independent researcher. According to the thematic approach43, themes were derived naturally from the data. Second, instead of an a priori coding structure, themes were grouped in meaningful ways. This was followed by content interpretation of data. Results were discussed and verified within team meetings of our group. If the interpretation of the items differed among group members, discussions were held with the group until a solution was found. Experienced psychological psychotherapists with a high level of clinical expertise, especially with psychotic disorders and substance use disorders, were always present at the discussions.
Ethics approval
All procedures of the study were carried out in compliance with the latest revision of the Declaration of Helsinki.
Results
Demographics and cannabis use patterns
Descriptive data of our sample regarding the parameters collected are presented in Table 1.
Cannabis intoxication effects and motivational stages (change motivation)
To identify potential predictors for different motivational stages (SOCRATES scales), we first investigated associations between motivational stages and potential predictors using correlative analyzes. Following previous findings by other groups14, we correlated motivational stages with cannabis intoxication effects, with craving as a key factor explaining consumption relapse, and also with frequency of cannabis use, age at onset of use and sociodemographic data. Parameters that significantly correlated with amotivational stage were integrated into multiple regression analyzes. Table 2 presents the significant predictors for each of the three motivational stages, as well as parameters included in the analyzes but not significantly predicting the criterion (the latter listed under “excluded parameters” in Table 2).
Regarding cannabis intoxication effects, paranoia/dysphoria in particular emerges as relevant positive predictor of motivation to change. At the highest and the middle motivational stage, it is in each case the strongest predictor. In addition, the remaining two unpleasant acute effects are also significant as positive predictors in the middle and lowest stages of change motivation. Pleasant cannabis acute effects, on the other hand, are not predictive of change motivation.
It is also interesting that hedonistic reward craving is positively associated with the low motivational stage of ambivalence, whereas relief craving acts as a positive predictor at the next-highest stage of recognition. The highest motivational stage (taking steps), where steps of change have already taken place, is not predicted by craving anymore.
All three regression models include the variable gender as a significant predictor. In each case, the male gender predicts the outcome parameter. To provide arguments for the subsequent discussion of this finding, we retrospectively analyzed male and female users regarding potential differences in patterns of cannabis use and acute intoxication effects. We found significant differences in the average duration of regular use (males: 33.83 months with a standard deviation of 60.06; females: 17.70 months with a standard deviation of 24.71 (p ≤ 0.001)). Further differences were found in the average abstinence time within the last year (males: 18.33 weeks with a standard deviation of 17.42; females: 23.10 weeks with a standard deviation of 18.96 (p = 0.006)). Regarding acute intoxication effects, only positive effects (euphoria/creativity) differed with a higher mean average for men of 3.52 and standard deviation of 0.68, and a lower mean average for women of 3.26 and standard deviation of 0.87 (p ≤ 0.001).
In addition, all regression models include the number of abstinent weeks as a negative predictor for motivation to change. Thus, the more regular the use, the stronger the desire to change. This is most pronounced in the motivational stage of ambivalence, followed by recognition, and the predictive value is lowest in the highest motivational stage.
Effect size calculations for “taking steps”: The effect size f2 according to Cohen42 is 0.143 for the overall model, which corresponds to a medium effect. Regarding individual predictors, the intoxication effect “paranoia/dysphoria” represents an almost medium effect (f2 = 0.103). The other two influencing factors have only a very small effect (each f2 = 0.02).
Effect size calculations for “recognition”: The overall model reveals a medium to strong effect with f2 = 0.24. Individual predictors range between small to medium effect sizes f2 between 0.05 and 0.07, while the acute intoxication effect “psychosis like experience/loss of reality” has a small effect with f2 = 0.02.
Effect size calculations for “ambivalence”: The effect size for the overall model is f2 = 0.3, which almost corresponds to a strong effect. With regard to the individual predictors, small to medium effects can be observed in each case.
Group comparison of current versus past users
We compared three groups: Current cannabis users were divided into two groups (with and without intention to stop cannabis use), past users were the third group. Multivariate analyzes of variance (MANOVA) and Chi2-tests revealed no significant group differences regarding sociodemographic data except for age (which, however, was not found to be predictive with respect to the target parameters), employment status, diagnoses with mental disorder (self-report) and age at onset of cannabis use.
Significant group differences were identified in all acute cannabis intoxication effects and both variants of craving. Further, average frequency of cannabis use was about twice as pronounced in the group with current users (with intention to stop consumption), compared with the other groups.
Table 3 displays group differences.
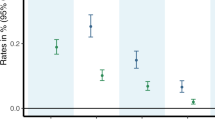
Effect size for group comparisons regarding paranoia/dysphoria (partial eta2 = 0.13) indicates a large effect; regarding psychosis-like/loss of reality (partial eta2 = 0.094) it indicates a medium to large effect; regarding confusion/disorientation (partial eta2 = 0.044) it indicates a small to medium effect; regarding euphoria/creativity (partial eta2 = 0.040) it indicates a small to medium effect. The effect size for the group comparisons regarding reward-craving (partial eta2 = 0.20) indicates a large effect and regarding relief-craving (partial eta2 = 0.05) it indicates a medium effect. The effect size for the group comparisons regarding average frequency of cannabis use (partial eta2 = 0.02) indicates a small effect.
Post-hoc analyzes reveal significant group differences regarding paranoia/dysphoria between all groups: Past versus current users without intention to stop use (p ≤ 0.001), between past and current users with intention to stop use (p = 0.001) and between current users with versus without intention to stop use (p ≤ 0.001). Respective descriptive results, the past users reported the highest adverse effects, followed by users who intend to change their consumption. The lowest aversive effects reported current users without any intention to change use.
Significant group differences regarding psychosis-like/loss of reality were seen between past and both groups of current users (both p ≤ 0.001). Respective descriptive results, the past users reported higher adverse effects compared with current users.
Significant group differences regarding confusion/disorientation were also seen between past and both groups of current users (without intention to stop use: p ≤ 0.001; with intention to stop use: p = 0.007). Respective descriptive results, the past users again reported higher adverse effects compared with current users.
Significant group differences regarding positive intoxication effects, euphoria/creativity, were seen between past and both groups of current users (without intention to stop use: p = 0.001; with intention to stop use: p ≤ 0.001). Respective descriptive results, the past users reported lower positive effects compared with current users.
Regarding reward-craving, post-hoc analyzes revealed significant group differences between past and both groups of current users (both p ≤ 0.001). Respective descriptive results, past users reported less craving compared with current users.
Regarding relief-craving, past users were different from both groups of current users (without intention to stop use: p = 0.002; with intention to stop use: p ≤ 0.001). Respective descriptive results, past users reported less craving compared with current users.
Finally, respective average frequency of cannabis use, just both current users present significant different results (p = 0.028), due to the high standard deviations respective mean values.
Qualitative information on reasons for abstinence in past users
Qualitative statements of past users on reasons for abstinence were assigned to seven thematic groups (multiple answers were allowed). In addition to the following presentation of the qualitative categories, a quantitative indication is given of how many of the respondents’ statements could be assigned to the corresponding category (in percent):
-
(1)
Lack of energy, such as sluggishness, fatigue, indifference, and unproductivity. Some example statements from subjects assigned to this category are: “It makes you too indifferent”; “sluggishness in everyday life”; “listlessness”; “I could not get up for anything anymore”; “side effect lethargy and lack of drive”. 41.7% of the statements were assigned to this category.
-
(2)
Anxiety symptoms Some example statements from subjects assigned to this category are: “Anxiousness and self doubt, especially in groups”; “had anxiety too often”; “I had panic attacks”. 25% of the statements were assigned to this category.
-
(3)
Financial problems Some example statements from subjects assigned to this category are: “Costs too high”; “no more money”; “too expensive”. 20% of the statements were assigned to this category.
-
(4)
Neurocognitive deficits (concentration performance) Some example statements from subjects assigned to this category are: “Memory performance worsened”; “difficulty concentrating”; “memory loss”. 12.2% of the statements were assigned to this category.
-
(5)
Occupational problems Some example statements from subjects assigned to this category are: “When gliding as a pilot, smoking pot is bad”; “focusing on work was difficult”; “professional careers became more important”. 12.1% of the statements were assigned to this category.
-
(6)
Psychosis-like experiences like the feeling, things would increasingly refer to oneself, or other people would look at them threateningly. Some example statements from subjects assigned to this category are: “Impression, others are talking about me”; “feeling like I’m losing control, going crazy”; “paranoia, feeling like someone is there, following me”. 10% of the statements were assigned to this category.
-
(7)
Horror trip-intoxications with still ongoing psychological consequences. Some example statements from subjects assigned to this category are: “Horror trip and perceived start of psychosis”; “paranoia that then didn’t go away”. 3.8% of the statements were assigned to this category.
Discussion
We analyzed the predictive impact of cannabis intoxication effects on abstinence-motivational stages in an online sample. Potentially influencing parameters were included, such as craving, patterns of cannabis use and sociodemographics. Further analyzes compared past and current users (with and without intention to stop consumption) regarding outcome parameters with special focus on different intoxication effects.
Experiencing paranoia/dysphoria as a quality of cannabis intoxication was most predictive for abstinence motivation, especially for the higher motivational stages such as taking steps and recognition. Compared to other acute intoxication effects, paranoia/dysphoria also differentiated most clearly and with the highest effect size between the three groups: Among former users who retrospectively reported their past cannabis use experiences, paranoia and dysphoria were most pronounced, followed by present users with the intention to stop consumption. In present users without intention to stop cannabis use, paranoia and dysphoria seem to be least pronounced as acute intoxication effect.
Slightly less predictive for abstinence motivation was craving and male gender, as well as the two further negative acute intoxication effects (psychosis-like/loss of reality and confusion/disorientation), reaching significance only in the motivational stages recognition and ambivalence. Pleasant intoxication effects were not associated with abstinence motivation. These quantitative findings correspond with qualitative statements of past users: Lack of energy was the primary reason for abstinence, indicating a depressive symptom or part of the “a motivational syndrome”44. Lack of energy was followed by anxiety symptoms, both in turn corresponding with paranoia/dysphoria as quality of intoxication with the highest predictive impact for abstinence.
The less pronounced but nevertheless significant predictive impact of psychosis-like intoxication effects with respect to abstinence motivation indicated by our quantitative data corresponds with the 10–15% of persons qualitatively stating such experiences (PLE and “horror-trip”). This is in line with previous research stating that close to 15% of cannabis users report such experiences29.
The group comparison between current users (with versus without intention to quit use) versus past users revealed overall significant more unpleasurable intoxication effects in past users, whereas current users presented more pleasurable effects. Current users with versus without intention to quit were similar regarding most intoxication effects (apart from the above mentioned significant more paranoia/dysphoria within the intention to quit group). These findings highlight the importance of the specific quality of acute intoxication, especially with regard to the discussion of cannabis induced PLE, particularly emphasized in research literature14. In order to place the present findings comprehensibly in existing literature, the discussion regarding PLE must be elevated to the level of the individual items/symptoms. As previously criticized by colleagues45, the PLE-concept is poorly defined respective its content and time criteria. In the present operationalization, loss of reality and hallucinations are included in a dimension that we called the PLE/loss of reality-dimension (when beginning with our study). Other researchers present a dimension of the Cannabis Experiences Questionnaire, called “paranoia/dysphoria,” largely corresponding to the present dimension “paranoia/dysphoria”10. However, these authors refer to this dimension also as PLE, according to other groups stating that depressive and certain anxiety symptoms are intrinsic to the psychotic illness45.
Thus, we may consider now that it is essential to specify the dimensions of PLE. We may postulate that, in the sense of our research colleagues, we ultimately have two present PLE-dimensions: Besides our initially named PLE-dimension psychosis-like/loss of reality, also the dimension paranoia/dysphoria may be defined as part of a PLE-spectrum, the latter with even higher impact for abstinence or change motivation.
Corresponding, the PLE dimension in the study of Sami and colleagues14 integrates items that were presently factorized into the two so-called PLE-dimensions: PLE items of Sami and colleagues “fearfulness” and “feeling nervous” are assigned to the present paranoia/dysphoria dimension (present PLE-dimension 1), and PLE items of Sami and colleagues “feeling of going crazy”, “hearing voices” are assigned to the present psychosis like experiences/loss of reality dimension (present PLE-dimension 2).
Thus, respective its specific content, the present paranoia/dysphoria dimension (PLE 1) could be labeled as the “affective PLE dimension”, whereas the present PLE/loss of reality-dimension (PLE 2) could be labeled as the “perceptual PLE dimension” since it describes changes on the perceptual level, typically occurring in the context of hallucinogenic substances. Of course, it is extremely scary if psychotic experiences, such as hallucinations, occur in an individual, seemingly “out of nowhere” as part of a mental illness. However, some psychosis-like experiences are intentionally caused by some users of hallucinogenic substances such as psilocybin to alter consciousness46. Approximately 15.9% of the U.S. population older than 12 years ever used a hallucinogenic drug46. The dimension paranoia/dysphoria, however, describes affective changes towards a pole that may generally experienced as aversive. We suggest that presumably no person would take a substance with the a priori aim to induce paranoia and/or dysphoria. Instead, this is called a “horror trip” when it occurs, and according to the present qualitative evaluation, it represents a reason for cessation of consumption.
Regarding craving, it is remarkable that hedonistic reward craving is associated with the low motivation stage of ambivalence, whereas relief craving acts as a predictor at the next-highest stage of recognition. At the highest stage, taking steps, in which decisive steps of change have already taken place, craving is no longer significant. This suggests that craving for cannabis strongly decreases when users have succeeded in discontinuing consumption. But in current users, relief craving may be associated with some insight into problems caused by cannabis use, so that abstinence is considered.
In addition, gender was a predictor for all three motivational stages. Studies on cannabis predominantly examine men47. However, gender differences in cannabis use seem to exist. A research team found that women experience the effects of cannabis more pleasantly compared to men. Thus, women seem to be more receptive to further use than men after first use48. The present findings that male gender is associated with higher motivation to change cannabis use could be explained in this context. Therefore, if women experience cannabis effects as more pleasant on average, they may be less motivated to change use. However, the present data tend to indicate the opposite. Women differ from men with regard to acute intoxication effects only in that they experience fewer positive effects. An alternative explanation could be that men show more problematic patterns of use and thus have stronger subsequent problems, which then justify a motivation to change. This would be supported by the present data, with males using cannabis for significantly longer periods of time and showing shorter periods of abstinence than females. Other research data also point to stronger patterns of use among men. For example, Khan and colleagues report that men have longer episodes of cannabis use disorders compared to woman49, and Kerridge and colleagues report higher 12-month prevalences of cannabis use disorders in men50.
Furthermore, present data found that the number of abstinent weeks is negatively predictive associated with motivation to change. That is, the more regular the use, the more pronounced are the motivational stages of ambivalence and recognition. This fits with the finding of other researchers that higher severity of substance use predicts higher motivation to change51, as heavy use in particular will be associated with subsequent problems.
Finally, with regard to the clinical relevance of the present work, therapeutic approaches aiming to build up or maintain abstinence motivation could be highlighted on the one hand. Working on craving is common in the treatment of substance use disorders, for example in the dialectic behavioral therapy for substance use disorders. Here, craving is treated with anti-craving skills, similar to dealing with stress and inner tension52. Acute cannabis intoxication and the question of whether cannabis is fulfilling the user’s expectations fits well with the concept of motivational interviewing (MI). Our findings emphasize the importance of systematically integrating the acute intoxication effects into the training of MI professionals53.
In addition to the issue of cessation of cannabis use, another interesting question regarding intoxication effects is whether they are useful as predictors in the early detection of psychosis. This would make it possible to identify at-risk individuals among users, which would be a real gain for psychosis prevention. However, in order to increase the predictive value for psychosis, further criteria would probably have to be defined, such as the frequency of occurrence and their temporal persistence, as Schulze-Lutter and colleagues criticize the PLE-concept and in accordance with the risk symptoms attenuated psychotic symptoms (APS) and brief intermittent psychotic symptoms (BIPS)45. Another aspect that should be specified in the PLE concept is its content, i.e. the question of which symptoms are included and which are not. In this regard, the present study delivers a real benefit by differentiating PLE dimensions into the aforementioned affective and perceptual dimensions. We were at least able to show that these dimensions have different predictive values with regard to the motivation to change consumption. Further studies could investigate whether there is also a different predictive value with regard to cannabis use disorder and/or potential psychotic decompensation.
Limitations
The primary limitation of our study is the cross-sectional design, which only allows a limited interpretation of a cause-and-effect relationship between the variables. Moreover, the available data are based on retrospective estimates and are therefore prone to recall errors. Another potential source of error is the use of self-report instruments, which are prone to certain perceptual errors. Regarding the question of present mental disorders, self-report is not very reliable compared to the use of established diagnostic instruments. Further, THC levels of cannabis used by subjects were not recorded, whereas Freeman and colleagues12 postulated an increased THC level in cannabis and other researchers54 reported increased psychosis-like intoxication effects at elevated THC levels. In addition, data on subjective intoxication effects may be biased because subjects retrospectively estimate a state in which they were acutely intoxicated. Moreover, the survey was conducted online. The prevailing pandemic corona situation did not allow for any other format. Thus, finally, it cannot be ruled out that individual participants provided implausible information, which would have been more noticeable in a face-to-face situation.
Conclusions
Not all phenomena subsumed under cannabis induced psychosis-like experiences are experienced by users as aversive per se. Hallucinations, for example, can be fascinating, at least as long as they can be attributed to a hallucinogenic drug. Paranoia and dysphoria, on the other hand, are apparently unpleasant. This distinction proved crucial in the present study with regard to the predictive significance of PLE for abstinence motivation. Further studies should clarify the extent to which aversively experienced acute intoxication effects can be integrated into psychotherapeutic settings when working abstinence-oriented. In addition, the significance of certain cannabis-induced PLE should be investigated more closely with regard to the early detection of psychoses. For this purpose, however, PLE probably need to be specified by additional criteria, especially time criteria.
Data availability
The datasets generated during the current study are available from the corresponding author on reasonable request.
References
Lee, K. W. et al. A systematic review on definitions and assessments of psychotic-like experiences. Early Interv. Psychiatry 10(1), 3–16 (2016).
Cowan, H. R. & Mittal, V. A. Three types of psychotic-like experiences in youth at clinical high risk for psychosis. Eur. Arch. Psychiatry Clin. Neurosci. 271(4), 733–744 (2021).
van Os, J., Myin-Germeys, I., Delespaul, P. & Krabbendam, L. A systematic review and meta-analysis of the psychosis continuum: evidence for a psychosis proneness–persistence–impairment model of psychotic disorder. Psychol. Med. 39, 179–195 (2009).
Unterrassner, L. et al. Psychotic-like experiences at the healthy end of the psychosis continuum. Front. Psychol. 8, 775 (2017).
Baggio, S. et al. The relationship between subjective experiences during first use of tobacco and cannabis and the effect of the substance experienced first. Nicotine Tob. Res. 16(1), 84–92 (2014).
Schmid, Y. et al. Emergency department presentations related to acute toxicity following recreational use of cannabis products in Switzerland. Drug Alcohol Depend. 206, 107726. https://doi.org/10.1016/j.drugalcdep.2019.107726 (2020).
McHugh, M. J. et al. Cannabis-induced attenuated psychotic symptoms: implications for prognosis in young people at ultra-high risk for psychosis. Psychol. Med. 47(4), 616–626 (2017).
Hamilton, I. Cannabis, psychosis and schizophrenia: unravelling a complex interaction. Addiction 112(9), 1653–1657 (2017).
Takahashi, T. et al. Increased Heschl’s gyrus duplication in schizophrenia spectrum disorders: a cross-sectional MRI study. J. Personal. Med. 11(1), 40 (2021).
Manthey, J., Freeman, T. P., Kilian, C., López-Pelayo, H. & Rehm, J. Public health monitoring of cannabis use in Europe: prevalence of use, cannabis potency, and treatment rates. Lancet Reg. Health Eur. 10, 100227 (2021).
Orth, B. & Merkel, C. Der Cannabiskonsum Jugendlicher und junger Erwachsener in Deutschland. Ergebnisse des Alkoholsurveys 2018 und Trends [Cannabis use among adolescents and young adults in Germany. Results of the Alcohol Survey 2018 and trends]. Retrieved from Colonia: Bundeszentrale für gesundheitliche Aufklärung, BzgA (2019).
Freeman, T. P. et al. Changes in delta-9-tetrahydrocannabinol (THC) and cannabidiol (CBD) concentrations in cannabis over time: systematic review and meta-analysis. Addiction 116(5), 1000–1010 (2021).
Charlson, F. J. et al. Global epidemiology and burden of schizophrenia: findings from the global burden of disease study 2016. Schizophr. Bull. 44(6), 1195–1203 (2018).
Sami, M., Notley, C., Kouimtsidis, C., Lynskey, M. & Battahcharyya, S. Psychotic-like experiences with cannabis use predict cannabis cessation and desire to quit: a cannabis discontinuation hypothesis. Psychol. Med. 49(1), 103–112 (2019).
Schoeler, T. et al. Continued versus discontinued cannabis use in patients with psychosis: a systematic review and meta-analysis. Lancet Psychiatry 3(3), 215–225 (2016).
Kandel, D. B. & Logan, J. A. Patterns of drug-use from adolescence to young adulthood. 1. Periods of risk for initiation, continued use, and discontinuation. Am. J. Public Health 74, 660–666 (1984).
Schnell, T., Becker, T., Thiel, M. C. & Gouzoulis-Mayfrank, E. Craving in patients with schizophrenia and cannabis use disorders. Can. J. Psychiatry 58(11), 646–649 (2013).
Blanchard, J. J., Squires, D. & Henry, T. Examining an affect regulation model of substance abuse in schizophrenia: the role of traits and coping. J. Nerv. Ment. Dis. 187, 72–79 (1999).
Regier, D. A., Farmer, M. E. & Rae, D. S. Comorbidity of mental disorders with alcohol and other drug abuse. Results from the Epidemiologic Catchment Area (ECA) Study. J. Am. Med. Assoc. 264(19), 2511–2518 (1990).
Schüler, M., Moritz, S. & Schnell, T. Development and initial validation of a reliable German self-report measure to assess acute cannabis intoxication-effects (CanTox-17). Int. J. Methods Psychiatr. Res. 31(3), e1925 (2022).
Bak, P. M. Assoziatives Lernen in Lernen, Motivation und Emotion [Associative learning in Learning, Motivation and Emotion] 9–38 (Springer, 2019).
Bianconi, F. et al. Differences in cannabis-related experiences between patients with a first episode of psychosis and controls. Psychol. Med. 46(5), 995–1003. https://doi.org/10.1017/S0033291715002494 (2016).
Le Strat, Y. et al. First positive reactions to cannabis constitute a priority risk factor for cannabis dependence. Addiction 104(10), 1710–1717 (2009).
Scherrer, J. F. et al. Subjective effects to cannabis are associated with use, abuse and dependence after adjusting for genetic and environmental influences. Drug Alcohol Depend. 105(1–2), 76–82 (2009).
Lüscher, C., Robbins, T. W. & Everitt, B. J. The transition to compulsion in addiction. Nat. Rev. Neurosci. 21(5), 247–263 (2020).
Fergusson, D. M., Horwood, L. J., Lynskey, M. T. & Madden, P. A. Early reactions to cannabis predict later dependence. Arch. Gen. Psychiatry 60(10), 1033–1039. https://doi.org/10.1001/archpsyc.60.10.1033 (2003).
Zeiger, J. S. et al. Subjective effects to marijuana associated with marijuana use in community and clinical subjects. Drug Alcohol Depend. 109(1–3), 161–166 (2010).
Grant, J. D. et al. Subjective reactions to cocaine and marijuana are associated with abuse and dependence. Addict. Behav. 30, 1574–1586 (2005).
Thomas, H. A community survey of adverse effects of cannabis use. Drug Alcohol Depend. 42, 201–207 (1996).
Barkus, E. & Lewis, S. Schizotypy and psychosis-like experiences from recreational cannabis in a non-clinical sample. Psychol. Med. 38(9), 1267–1276 (2008).
Quinn, C. A., Wilson, H., Cockshaw, W., Barkus, E. & Hides, L. Development and validation of the cannabis experiences questionnaire-Intoxication effects checklist (CEQ-I) short form. Schizophr. Res. 189, 91–96 (2017).
Barkus, E. J., Stirling, J., Hopkins, R. S. & Lewis, S. Cannabis-induced psychosis-like experiences are associated with high schizotypy. Psychopathology 39(4), 175–178 (2006).
Stirling, J. et al. Cannabis-induced psychotic-like experiences are predicted by high schizotypy. Confirmation of preliminary results in a large cohort. Psychopathology 41(6), 371–378 (2008).
Birnbaum, M. L., Cleary, S. D., Ramsay Wan, C., Pauselli, L. & Compton, M. T. Factor structure of the Cannabis Experiences Questionnaire in a first-episode psychosis sample. Early Interv. Psychiatry 13(3), 495–501 (2017).
Schmermelleh-Engel, K., Moosbrugger, H. & Müller, H. Evaluating the fit of structural equation models: tests of significance and descriptive goodness-of-fit measures. Methods Psychol. Res. Online 8(2), 23–74 (2003).
Browne, M. W. & Cudeck, R. Alternative ways of assessing model fit. In Testing Structural Equation Models (eds Bollen, K. A. & Long, J.) 136–162 (Sage, 1993).
Vandenberg, R. J. & Lance, C. E. A review and synthesis of the measurement invariance literature: suggestions, practices and recommendations for organizational research. Org. Res. Methods 3, 4–70 (2000).
Nunnally, J. C. & Bernstein, I. H. Psychological Theory (MacGraw-Hill, 1994).
Schnell, T., Münchenhagen, L., Tersudi, K., Daumann, J. & Gouzoulis-Mayfrank, E. Entwicklung und Evaluation eines deutschsprachigen Instruments zur Erfassung von Cannabis-Craving (CCS-7) [Development and evaluation of a German language instrument for the assessment of cannabis craving]. Z. Klin. Psychol. Psychother. 40(1), 33–41 (2011).
Miller, W. R. & Tonigan, J. S. Assessing trinker’s motivation for change: The stages of readiness and treatment eagerness scale (Socrates). Psychol. Addict. Behav. 10, 81–89 (1996).
Carey, K. B., Purnine, D. M., Maisto, S. A. & Carey, M. P. Assessing readiness to change substance abuse: a critical review of instruments. Clin. Psychol. Sci. Pract. 6(3), 245 (1999).
Cohen, J. Statistical Power Analysis for the Behavioral Sciences 2nd edn. (Academic Press, 1988).
Braun, V. & Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 3(2), 77–101 (2006).
Lac, A. & Luk, J. W. Testing the amotivational syndrome: Marijuana use longitudinally predicts lower self-efficacy even after controlling for demographics, personality, and alcohol and cigarette use. Prev. Sci. 19(2), 117–126 (2018).
Schultze-Lutter, F., Klosterkötter, J., Gaebel, W. & Schmidt, S. J. Psychosis-risk criteria in the general population: frequent misinterpretations and current evidence. World Psychiatry 17(1), 107–108 (2018).
Jahn, Z. W., Lopez, J., de la Salle, S., Faber, S. & Williams, M. T. Racial/ethnic differences in prevalence of hallucinogen use by age cohort: findings from the 2018 National Survey on Drug Use and Health. J. Psychedelic Stud. 5(2), 69–82 (2021).
Rubino, T. & Parolaro, D. Sex-dependent vulnerability to Cannabis abuse in adolescence. Front. Psychiatry 6, 56 (2015).
Cooper, Z. D. & Haney, M. Investigation of sex-dependent effects of cannabis in daily cannabis smokers. Drug Alcohol Depend. 136, 85–91 (2014).
Khan, S. S. et al. Gender differences in cannabis use disorders: results from the National Epidemiologic Survey of Alcohol and Related Conditions. Drug Alcohol Depend. 130(1–3), 101–108 (2013).
Kerridge, B. T., Pickering, R., Chou, P., Saha, T. D. & Hasin, D. S. DSM-5 cannabis use disorder in the National Epidemiologic Survey on Alcohol and Related Conditions-III: gender-specific profiles. Addict. Behav. 76, 52–60 (2018).
Slesnick, N. et al. Troubled parents, motivated adolescents: predicting motivation to change substance use among runaways. Addict. Behav. 34(8), 675–684 (2009).
Warner, N. & Murphy, M. Dialectical behaviour therapy skills training for individuals with substance use disorder: a systematic review. Drug Alcohol Rev. 41(2), 501–516 (2022).
Madson, M. B., Villarosa-Hurlocker, M. C., Schumacher, J. A., Williams, D. C. & Gauthier, J. M. Motivational interviewing training of substance use treatment professionals: a systematic review. Subst. Abuse (2018).
Marconi, A., Di Forti, M., Lewis, C. M., Murray, R. M. & Vassos, E. Meta-analysis of the association between the level of cannabis use and risk of psychosis. Schizophr. Bull. 42, 1262–1269 (2016).
Funding
Open Access funding enabled and organized by Projekt DEAL. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
T.S. contributed to conception and design of the study, coordinated the study and wrote the manuscript. C.-M.G. recruited data and performed statistical analyzes. N.K. contributed to the interpretation of the results and supervised statistics. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Schnell, T., Grömm, CM. & Klöckner, N. Predictive impact of different acute cannabis intoxication effects with regard to abstinence motivation and cessation of use. Sci Rep 13, 709 (2023). https://doi.org/10.1038/s41598-023-27592-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-27592-6
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
