
Abstract
This study was conducted to investigate the relationship between serum endothelial dysfunction-related biomarker levels and organ dysfunction severity in septic patients and the predictive value of these levels during sepsis. In total, 105 patients admitted to the Department of Critical Care Medicine were enrolled between September 2020 and November 2021. Serum syndecan-1 and soluble thrombomodulin(sTM) levels were measured by enzyme-linked immunosorbent assay, and clinical and laboratory data were recorded. Enroll patients were divided into the infection (n = 28), septic nonshock (n = 31), and septic shock (n = 46) groups . Serum syndecan-1 (102.84 ± 16.53 vs. 55.38 ± 12.34 ng/ml), and sTM(6.60 ± 1.44 ng/ml vs. 5.23 ± 1.23 ng/ml, P < 0.01) levels were increased in the septic group compared with those in the infection group. Serum syndecan-1 levels were closely positively correlated with serum sTM (rs = 0.712, r2 = 0.507, P < 0.001). Additionally, serum syndecan-1(rs = 0.687, r2 = 0.472, P < 0.001) and sTM levels (rs = 0.6, r2 = 0.36, P < 0.01) levels were significantly positively correlated with the sequential organ failure assessment scores respectively. Syndecan-1 (AUC 0.95 ± 0.02, P < 0.0001) was more valuable for prediction sepsis than was sTM (AUC 0.87 ± 0.04, P < 0.0001). Compared with sTM (AUC 0.88 ± 0.03, P < 0.001), syndecan-1 (AUC 0.95 ± 0.02, P < 0.001) and SOFA score (AUC 0.95 ± 0.02, P < 0.001) were better predictors of septic shock. Serum syndecan-1 and sTM levels were associated with organ dysfunction severity in septic patients, and both were good predictors for early identification of sepsis, particularly in patients undergoing septic shock.
Similar content being viewed by others

Introduction
Sepsis is a life-threatening organ dysfunction caused by a dysregulated host response to infection and is associated with significant morbidity and mortality1. The pathogenetic mechanism of sepsis is highly complex, and endothelial dysfunction is an important factor leading to organ dysfunction2. Endothelial cells shift toward a proinflammatory, proadhesive, and procoagulant phenotype during sepsis. Moreover, the endothelial cells' functional modifications are initially adaptive but ultimately become harmful leading to multiorgan dysfunction during sepsis3.
The glycocalyx is the constituent of the endothelial surface layer, which regulates vascular permeability, adhesion of leukocytes and platelets, shear stress, and inflammatory processes4.
Syndecan-1 is a member of the polysaccharide syndecan family, which belongs to the family of transmembrane heparan sulfate proteins in the glycocalyx, and circulating syndecan-1 is a marker of endothelial glycocalyx degradation5. Previous studies have shown that syndecan-1, is shed and released into the bloodstream during severe infection, reflecting glycocalyx damage and hence a superficial endothelial disruption6,7. Studies have demonstrated that syndecan-1 shedding is associated with both sepsis presence and severity8,9. Thrombomodulin (TM), an integral endothelial cell membrane protein, is critical in maintaining vascular thrombus resistance10. TM has anticoagulant activity as well as anti-inflammatory and cytoprotective effects11. Previous studies have shown that TM is enzymatically cleaved from endothelial cells and released into the bloodstream under direct endothelial cell damage, thereby reflecting profound endothelial dysfunction12.
As the innermost layer of the arterial wall, the syndecan-1 is the first protein to be affected13. However, soluble thrombomodulin (sTM) is derived from direct damage to endothelial cells, not through secretion, which appears later in the circulating. Syndecan-1 and sTM serve as markers of endothelial cell injury in humans but to varying degrees. Furthermore, circulating syndecan 1 and sTM levels have been independently associated with mortality in patients with both trauma and acute myocardial infarction14,15. However, limited data exist regarding the relationship between syndecan-1, sTM, and organ dysfunction severity and their predictive value in sepsis. This study was conducted to investigate the relationship between syndecan-1, sTM, and organ dysfunction severity in septic patients, and the predictive value of these biomarkers during sepsis.
Methods
Participants
ThE study was conducted at the Department of Critical Care Medicine between September 2020 and November 2021, approved by the hospital institutional review board (Ethics Approval No. JS-3283) and performed following the Declaration of Helsinki. All enrolled patients or their families provided written informed consent. Patients were screened for enrolment within the first 24 h of admission.
Patients were divided into the infection, septic nonshock, and septic shock groups. The infection group comprised patients admitted to the intensive care unit (ICU) for an active infection. The septic nonshock group comprised patients with an acute change in Sequential Organ Failure Assessment (SOFA) score ≥ 2 points consequent to the infection and for whom septic shock was ruled out. The septic shock group comprised patients requiring the administration of vasopressors and had lactate levels > 2 mmol/l on the day of ICU admission1. Sepsis/septic shock was diagnosed according to The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis 3.0)1. We excluded patients who were aged < 18 years, had ICU stays of < 24 h, had massive bleeding or pulmonary embolism, had a heart attack or acute exacerbation of previous heart disease in the previous week, had heart surgery in the prior week or lacked informed consent.
Data collection
Baseline clinical and laboratory data were collected within 24 h after ICU admission, including patient age, sex, hemodynamic parameters, blood chemistry, SOFA scores, and Acute Physiology and Chronic Health Evaluation (APACHE) II scores.
Blood sample collection
Peripheral blood samples were collected within the first 24 h of ICU admission and immediately centrifuged. Serum was separated by centrifugation at 2500×g for 15 min and stored immediately at −80 °C until assessment by enzyme-linked immunosorbent assay (ELISA).
ELISA measurements
The soluble biomarkers, serum syndecan-1 and sTM, established biomarkers of endothelial glycocalyx and cell injury, respectively, were measured using commercially available immunoassays, the Human Syndecan-1 ELISA kit (CUSABIO, Catalog No. CSB-E1498h, Wu Han, China) and Human soluble Thrombomodulin ELISA kit (Abcam, Catalog No. ab214029, Cambridge, England).
Statistical analysis
Normally distributed data are expressed as the mean and standard deviation and were compared using Student’s t-test or one-way analysis of variance. Non-normally distributed data are presented as the median and interquartile intervals and were compared using the Mann–Whitney U test. Categorical variables were compared using the chi-square test and are recorded as proportions. Correlations between normally distributed data were analyzed using the Pearson method. Spearman correlation analysis was performed on non-normally distributed data. Statistical analysis was performed using SPSS 23 (SPSS, IBM, Armonk, NY, USA) and GraphPad Prism 8.0 (GraphPad Software Inc., San Diego, CA, USA). Two-tailed P values ≤ 0.05 were considered statistically significant. Sample size was estimated based on a priori power calculation indicating an 80% power to detect differences in syndecan-1 and soluble thrombomodulin(sTM) (effect size 0.7) among groups at a 0.05 significance level using a power and sample size website.
Ethics approval and consent to participate
The study was approved by the PUMCH institutional review board (Ethics Approval No.JS-3283). All subjects provided written informed consent.
Results
Patients’ general and clinical characteristics
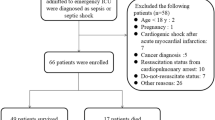
We screened 131 patients for enrolment, and 105 were included in this study (Fig. 1). The patients were divided into the infection (n = 28), septic nonshock (n = 31), and septic shock (n = 46) groups. Age, sex, venous-to-arterial carbon dioxide difference (Pv-aCO2), central venous blood oxygen saturation (ScvO2), mean arterial blood pressure (MAP), and central venous pressure (CVP) did not significantly differ among the groups. Patients with septic shock had significantly higher SOFA scores and lactate levels than did the septic nonshock group. Table 1 shows the basic characteristics of all enrolled patients.

Screening flowchart of patients.
Serum levels of endothelial damage-related biomarkers in a derivation cohort
Figure 2 and Table 2 show the changes in endothelial damage-related biomarkers in the progression from infection to septic shock. Serum syndecan-1 and sTM levels increased progressively from infected patients to septic nonstock patients to septic shock patients. The syndecan-1 and sTM level variation tendencies were similar among the groups. Serum syndecan-1 concentrations on ICU admission were significantly increased in the septic shock group and septic nonshock groups compared with those of the infection group.

Comparison of serum syndecan-1 levels (a) and sTM (b) levels among groups. Comparisons among multiple groups were conducted by one-way analysis of variance, and those between two groups were carried out with the Least Significant Difference (LSD) post hoc test. P < 0.05 were considered statistically significant. *Denotes P < 0.05, ***Denotes P < 0.001. sTM serum thrombomodulin.
Syndecan-1 levels were significantly increased in the septic shock group (102.84 ± 16.53 ng/ml) compared with those of the septic nonshock (76.06 ± 10.51 ng/ml) and infection (55.38 ± 12.34 ng/ml) groups. Serum sTM concentrations were significantly increased in the septic shock and septic nonshock groups compared with those of the infection group.
The septic shock group had higher sTM levels than did the septic nonshock group (9.67 ± 3.38 ng/ml vs. 6.60 ± 1.44 ng/ml, P < 0.01), and patients with septic nonshock had higher sTM levels than did patients with infection (6.60 ± 1.44 ng/ml vs. 5.23 ± 1.23 ng/ml, P < 0.01).
However, as result shown, no statistical difference in the serum syndecan-1 and sTM was seen when all patients (including infection ,sepsis non-shock and septic shock patients) were stratified by bacteremia and non-bacteremia (syndecan-1 82.47(61.14,103.07) vs. 75.84(69.13,87.33) ng/ml), P = 0.924; sTM 6.75(5.26,8.70) vs.7.39(5.81,8.89) ng/ml, P = 0.711). Moreover, no significant difference was observed according to the identified pathogens (gram-positive vs. gram-negative) involved in all patients (syndecan-1 86.48(66.24,99.17) vs.79.67(59.14,103.98) ng/ml, P = 0.684; sTM 6.89(5.34,8.92) vs.6.68(5.23,8.65) ng/ml, P = 0.927).
Serum syndecan-1 and sTM levels were associated with organ function and disease severity
To establish whether serum syndecan-1 and sTM levels could determine organ function and disease severity, we assessed the correlations between these levels and the SOFA and APACHE II scores on ICU admission.
Serum syndecan-1 levels were positively correlated with serum sTM (rs = 0.712, r2 = 0.507, P < 0.001, Fig. 3a), the both serum syndecan-1 (rs = 0.687, r2 = 0.472, P < 0.001, Fig. 3b) and sTM (rs = 0.6, r2 = 0.36, P < 0.01, Fig. 3c) levels were positively correlated with SOFA scores respectively. Additionally, serum syndecan-1 levels were weakly associated with APACHE II score (rs = 0.286, r2 = 0.082, P = 0.0049, Fig. 3d); however, we found no correlation between serum sTM levels and APACHE II score (r = 0.184, r2 = 0.034, P = 0.073).

Correlation analysis. (a) Correlation between serum syndecan-1 and sTM in all the patients enrolled on ICU admission. (b) Correlation between serum syndecan-1 and SOFA score in all the patients enrolled on ICU admission. (c) Correlation between serum sTM and SOFA score in all the patients enrolled on ICU admission. (d) Correlation between serum syndecan-1 and APACHE II score in all the patients enrolled on ICU admission. P < 0.05 were considered statistically significant. sTM serum thrombomodulin, SOFA sequential organ failure assessment score, ICU intensive care unit.
We further assessed whether serum syndecan-1 and sTM levels were correlated with organ dysfunction at study enrollment and found that neither serum syndecan1 levels nor sTM levels were significantly correlated with oxygen index, total bilirubin, or creatinine (data not shown).
Serum syndecan-1 and sTM levels were associated with tissue perfusion
To assess the relationship between endothelial damage and tissue perfusion, we assessed the association between serum syndecan-1 and sTM levels and lactate (lac). Serum syndecan-1 (rs = 0.574, r2 = 0.329, P < 0.001, Fig. 4a) and sTM (rs = 0.458, r2 = 0.210, P < 0.001, Fig. 4b) levels in all patients admitted to the ICU were significantly positively correlated with lactate, demonstrating that endothelial damage was closely related to tissue perfusion(Fig. 4).

Serum syndecan-1 and sTM levels were associated with tissue perfusion. (a) Correlation between serum syndecan-1 and Lac in all the patients enrolled on ICU admission. (b) Correlation between serum sTM and Lac in all the patients enrolled on ICU admission. P < 0.05 were considered statistically significant. sTM serum thrombomodulin, ICU intensive care unit.
Serum syndecan-1 was associated with coagulation function
Endothelial injury induces coagulation abnormalities during sepsis; therefore, we assessed the association between serum syndecan-1 and sTM levels and coagulation function parameters.
Correlation analysis showed that serum syndecan-1 levels were weakly correlated with prothrombin time (PT) (rs = 0.286, r2 = 0.082, P = 0.003) and international normalized ratio (INR) (rs = 0.337, r2 = 0.114, P = 0.0004) and not correlated with activated partial thromboplastin time (APTT) (rs = 0.063, P = 0.526), D-dimer (rs = 0.173, P = 0.087), or fibrinogen(Fib) (rs = − 0.054, P = 0.584). Serum sTM levels were not correlated with PT (rs = 0.096, P = 0.331), APTT (rs = 0.038, P = 0.704), D-dimer (rs = 0.040, P = 0.698), Fib (rs = − 0.190, P = 0.053), or INR (rs = 0.191, P = 0.051).
Ability of endothelial damage biomarkers to predict the incidence of sepsis and septic shock
We calculated the cut-off value, sensitivity, and specificity of syndecan1 and sTM as predictors of sepsis or septic shock for the enrolled patients using the receiver operating characteristic curve(Tables 3, 4 and Fig. 5).

Receiver operating characteristic curve analysis. The ability of Syndecan1 and sTM on ICU admission to predict the incidence of sepsis (a) or septic shock (b). sTM serum thrombomodulin, ICU intensive care unit, ICU intensive care unit, APACHE II score Acute Physiology and Chronic Health Evaluation II score, SOFA sequential organ failure assessment score, Lac lactate, PCT Procalcitonin.
For diagnosing sepsis(Fig. 5a, Table 3), SOFA score was the best predictor (AUC 0.99 ± 0.001, P < 0.0001), and syndecan-1 (AUC 0.95 ± 0.02, P < 0.0001) was a better predictor than was sTM (AUC 0.87 ± 0.04, P < 0.0001), Procalcitonin (PCT) (AUC 0.66 ± 0.06, P = 0.0135), Lac (AUC 0.70 ± 0.05, P < 0.001), or APACHE II score (AUC 0.70 ± 0.06, P = 0.0025).
To diagnose septic shock, syndecan-1 (AUC 0.95 ± 0.02, P < 0.001) and SOFA score (AUC 0.95 ± 0.02, P < 0.001) were better predictors than were sTM (AUC 0.88 ± 0.03, P < 0.001), Lac (AUC 0.85 ± 0.04, P < 0.001), PCT (AUC 0.67 ± 0.05, P < 0.01), APACHE II score (AUC 0.65 ± 0.06, P = 0.01).
Discussion
Our results indicated the following. First, both syndecan-1 and sTM levels were significantly increased in the septic shock group compared with those of the septic nonshock and the infection groups. The syndecan-1 and sTM levels gradually increased as the disease progressed, suggesting that endothelial injury was gradually aggravated. Syndecan-1 and sTM levels were significantly higher in patients with septic shock than in patients with infection and septic nonshock.
Moreover, serum syndecan-1 and sTM levels were elevated as the disease severity increased. Notably, serum syndecan-1 and sTM levels were positively correlated with both SOFA score and lactate. These results demonstrated the value of syndecan-1 and sTM levels as predictors of sepsis or septic shock incidence on the day of ICU admission.
Endothelial dysfunction is common in adult ICU patients, especially in critical patients with infection. Endothelial injury is a well-known hallmark of sepsis, but new data continue to emerge that further reveal the pathophysiology of endothelial damage in sepsis and its association with disease severity, including the applicability of biomarkers for outcomes16,17. However, different studies have yielded varying conclusions.
Anand et al. reported significant correlations between syndecan-1 levels and disease severity18. Deng et al. found that patients with sepsis had significantly higher serum sTM levels that were positively correlated with the disease severity19. Here, we revealed that the serum syndecan-1 and sTM levels were elevated with the disease severity, which is consistent with previous findings, but the molecular mechanism of this elevation remains undefined.
Syndecan-1 is a proteoglycan in the endothelial glycocalyx. Circulating syndecan-1 is a marker of endothelial glycocalyx degradation, which reflects superficial endothelial damage20. However, the mechanism underlying the endothelial glycocalyx during sepsis remains unclear. Metalloproteinases are activated in inflammatory states by reactive oxygen species and proinflammatory cytokines, which cleave proteoglycans directly from the endothelial cell membrane during sepsis4. The degraded glycocalyx layer leads to an increased permeability to plasma proteins and fluids, causing interstitial leakage. Several studies have demonstrated elevated syndecan-1 levels as a marker of glycocalyx degradation in patients with sepsis21,22.
Furthermore, endothelial dysfunction ultimately contributes to ending multiorgan damage during sepsis or septic shock. Considering the close relationship between endothelial function and organ function during sepsis1, we also explored the correlation between serum endothelial dysfunction biomarker levels and the SOFA scores and found that serum syndecan-1 and sTM levels were closely related to SOFA scores. Previous studies have shown that plasma syndecan-1 and sTM increased progressively and significantly across groups with increasing infectious severity and correlated significantly with organ failure as measured by SOFA scores in patients with varying degrees of infectious disease23.
Similarly, a large multicenter study of 1103 critically ill patients predominantly suffering from sepsis showed a strong association between epitheliopathy and organ failure17, demonstrating that patients with sepsis had higher plasma syndecan-1 and sTM levels than did non-infected patients. These results are consistent with the above idea and support our conclusion. Although the correlation was low in previous studies, our results showed a stronger correlation, which may be related to patient and sample heterogeneity and requires further confirmation.
Previous studies indicated that high syndecan-1 and sTM levels independently predicted liver and renal failure, respectively, and high sTM was further associated with an increased risk of developing multiple organ failure24. However, further analysis showed no significant correlations between syndecan-1, sTM, and organ function-related biomarker levels in septic patients. Moreover, endothelial dysfunction shifts toward a proapoptotic, proinflammatory, proadhesive, and procoagulant phenotype during sepsis, thus indicating the central role of endothelial dysfunction in the cross-talk during inflammation coagulation25,26. A previous study found an independent association between high circulating syndecan-1 levels and coagulopathy in a smaller cohort of 184 patients with severe sepsis or septic shock23.
Nevertheless, the correlations between endothelial dysfunction and coagulation found in the present study were relatively weak; thus, this correlation remains uncertain.
Sepsis-induced organ dysfunction is associated with inflammatory and coagulation responses in the endothelium as described above. Previous studies showed that endothelial dysfunction may result in decreased blood perfusion and therefore may aggravate lactic acidemia27. Microvascular obstruction and systemic endothelial dysfunction have been independently associated with plasma lactate in patients with falciparum malaria28. Here, we revealed that serum syndecan-1 and sTM levels were significantly correlated with lactate, which was consistent with previous findings, indicating that endothelial damage was closed correlated with tissue perfusion. Perfusion abnormalities caused by endothelial dysfunction may be another important cause of sepsis-related organ failure. Our previous study proposed mitochondrial dysfunction as an important cause of sepsis-related organ failure29. Thus, endothelial function induced by mitochondrial dysfunction might be an additional mechanism during sepsis.
Although clinicians know that endothelial activation and dysfunction play critical roles in the pathophysiology of sepsis and represent important therapeutic targets for reducing sepsis mortality, a large gap remains between basic research and clinical applications of endothelial activation and dysfunction. Thus, endothelial damage must be identified early in sepsis or septic shock. Elevated serum syndecan-1 and sTM levels could be used to alert clinicians of endothelial injury, and in clinical treatment, clinicians should put more emphasis on endothelial function and protecting endothelial cells from injury during sepsis.
Limitations
This study has several limitations. First, our sample size was limited, and replication studies with a larger sample size are needed. Second, our findings were observational, hence, no causality can be inferred. Third, the results should be interpreted with caution owing to the heterogeneity of enrolled patients. Fourth, we analyzed only blood taken from the initial draw and did not follow the biomarker dynamics over time. Fifth, we included no healthy control group, and the serum syndecan-1 and sTM levels at baseline need to be measured.
Conclusion
Syndecan-1 and sTM levels were positively associated with organ damage in patients with sepsis and septic shock. Serum syndecan-1 and sTM may be promising biomarkers for early diagnosis of sepsis, particularly for patients with septic shock.
Data availability
Data are available on request from the corresponding author.
References
Singer, M. et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA 315(8), 801–810 (2016).
Ince, C. et al. The endothelium in sepsis. Shock 45(3), 259–270 (2016).
Joffre, J., Hellman, J., Ince, C. & Ait-Oufella, H. Endothelial responses in sepsis. Am. J. Respir. Crit. Care Med. 202(3), 361–370 (2020).
Uchimido, R., Schmidt, E. P. & Shapiro, N. I. The glycocalyx: A novel diagnostic and therapeutic target in sepsis. Crit. Care 23(1), 16 (2019).
Dogné, S. & Flamion, B. Endothelial glycocalyx impairment in disease: Focus on hyaluronan shedding. Am. J. Pathol. 190(4), 768–780 (2020).
Ikeda, M. et al. Circulating syndecan-1 predicts the development of disseminated intravascular coagulation in patients with sepsis. J. Crit. Care 43, 48–53 (2018).
Smart, L. et al. Glycocalyx biomarker syndecan-1 is a stronger predictor of respiratory failure in patients with sepsis due to pneumonia, compared to endocan. J. Crit. Care 47, 93–98 (2018).
Nelson, A., Berkestedt, I., Schmidtchen, A., Ljunggren, L. & Bodelsson, M. Increased levels of glycosaminoglycans during septic shock: Relation to mortality and the antibacterial actions of plasma. Shock 30(6), 623–627 (2008).
Sallisalmi, M., Tenhunen, J., Yang, R., Oksala, N. & Pettilä, V. Vascular adhesion protein-1 and syndecan-1 in septic shock. Acta Anaesthesiol. Scand. 56(3), 316–322 (2012).
La Mura, V. et al. Resistance to thrombomodulin is associated with de novo portal vein thrombosis and low survival in patients with cirrhosis. Liver Int. 36(9), 1322–1330 (2016).
Shrestha, B. et al. Recombinant thrombomodulin suppresses histone-induced neutrophil extracellular trap formation. Front. Immunol. 10, 2535 (2019).
Ishii, H., Uchiyama, H. & Kazama, M. Soluble thrombomodulin antigen in conditioned medium is increased by damage of endothelial cells. Thromb. Haemost. 65(5), 618–623 (1991).
Marechal, X. et al. Endothelial glycocalyx damage during endotoxemia coincides with microcirculatory dysfunction and vascular oxidative stress. Shock 29(5), 572–576 (2008).
Johansson, P. I., Stensballe, J., Rasmussen, L. S. & Ostrowski, S. R. High circulating adrenaline levels at admission predict increased mortality after trauma. J. Trauma Acute Care Surg. 72(2), 428–436 (2012).
Ostrowski, S. R., Pedersen, S. H., Jensen, J. S., Mogelvang, R. & Johansson, P. I. Acute myocardial infarction is associated with endothelial glycocalyx and cell damage and a parallel increase in circulating catecholamines. Crit. Care 17(1), R32 (2013).
Pons, S. et al. Immune consequences of endothelial cells’ activation and dysfunction during sepsis. Crit. Care Clin. 36(2), 401–413 (2020).
Johansen, M. E. et al. Profound endothelial damage predicts impending organ failure and death in sepsis. Semin. Thromb. Hemost. 41(1), 16–25 (2015).
Anand, D., Ray, S., Srivastava, L. M. & Bhargava, S. Evolution of serum hyaluronan and syndecan levels in prognosis of sepsis patients. Clin. Biochem. 49(10–11), 768–776 (2016).
Yue, L., Deng, X., Yang, M. & Li, X. Elevated B-type natriuretic peptide (BNP) and soluble thrombomodulin (sTM) indicates severity and poor prognosis of sepsis. Ann. Palliat. Med. 10(5), 5561–5567 (2021).
Piotti, A. et al. Endothelial damage in septic shock patients as evidenced by circulating syndecan-1, sphingosine-1-phosphate and soluble VE-cadherin: A substudy of ALBIOS. Crit. Care 25(1), 113 (2021).
Huang, X. et al. Plasma endothelial glycocalyx components as a potential biomarker for predicting the development of disseminated intravascular coagulation in patients with sepsis. J. Intensive Care Med. 36(11), 1286–1295 (2021).
Saoraya, J., Wongsamita, L., Srisawat, N. & Musikatavorn, K. Plasma syndecan-1 is associated with fluid requirements and clinical outcomes in emergency department patients with sepsis. Am. J. Emerg. Med. 42, 83–89 (2021).
Ostrowski, S. R. et al. Association between biomarkers of endothelial injury and hypocoagulability in patients with severe sepsis: A prospective study. Crit. Care 19, 191 (2015).
Johansson, P. I., Stensballe, J. & Ostrowski, S. R. Shock induced endotheliopathy (SHINE) in acute critical illness: A unifying pathophysiologic mechanism. Crit. Care 21, 25 (2017).
Levi, M. & van der Poll, T. Inflammation and coagulation. Crit. Care Med. 38(2 Suppl), S26-34 (2010).
Joffre, J. & Hellman, J. Oxidative stress and endothelial dysfunction in sepsis and acute inflammation. Antioxid. Redox Signal. 35, 1291–1307 (2021).
El-Hattab, A. W. et al. Restoration of impaired nitric oxide production in MELAS syndrome with citrulline and arginine supplementation. Mol. Genet. Metab. 105(4), 607–614 (2012).
Hanson, J. et al. Microvascular obstruction and endothelial activation are independently associated with the clinical manifestations of severe falciparum malaria in adults: An observational study. BMC Med. 13, 122 (2015).
Liu, J. et al. Mitochondrial Sirt3 serves as a biomarker for sepsis diagnosis and mortality prediction. Sci. Rep. 12, 10414 (2022).
Funding
This work was supported by capital clinic research and demonstration application of diagnosis and treatment project (No. Z201100005520038).
Author information
Authors and Affiliations
Contributions
G.Z. designed the study, performed the statistical analysis, and drafted the manuscript. J.L. Collected serum samples and collated the clinical and laboratory data. H.Z. contributed to the analytic strategy and statistical analyses. X.W. conceived and designed the study, and revised the manuscript. D.L. designed the study and revised the manuscript. All authors take responsibility for all aspects of the reliability and freedom from bias of the data presented and their discussed interpretation. All authors read and approved the final manuscript. The patients gave written informed consent for clinical data use and publication.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Zhou, G., Liu, J., Zhang, H. et al. Elevated endothelial dysfunction-related biomarker levels indicate the severity and predict sepsis incidence. Sci Rep 12, 21935 (2022). https://doi.org/10.1038/s41598-022-26623-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-26623-y
This article is cited by
-
Assessment of soluble thrombomodulin and soluble endoglin as endothelial dysfunction biomarkers in seriously ill surgical septic patients: correlation with organ dysfunction and disease severity
European Journal of Trauma and Emergency Surgery (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
