
Abstract
This study aimed to measure the socio-economic inequalities in having minimum dietary diversity (MDD) among Bangladeshi children aged 6–23 months as well as to determine the factors that potentially contribute to the inequity. The Bangladesh Demographic and Health Survey (BDHS) 2017–2018 data were used in this study. A sample of 2405 (weighted) children aged 6–23 months was included. The overall weighted prevalence of MDD was 37.47%. The concentration index (CIX) value for inequalities in MDD due to wealth status was positive and the concentration curve lay below the line of equality (CIX: 0.1211, p < 0.001), where 49.47% inequality was contributed by wealth status, 25.06% contributed by the education level of mother, and 20.41% contributed by the number of ante-natal care (ANC) visits. Similarly, the CIX value due to the education level of mothers was also positive and the concentration curve lay below the line of equality (CIX: 0.1341, p < 0.001), where 52.68% inequality was contributed by the education level of mother, 18.07% contributed by wealth status, and 14.69% contributed by the number of ANC visits. MDD was higher among higher socioeconomic status (SES) groups. Appropriate intervention design should prioritize minimizing socioeconomic inequities in MDD, especially targeting the contributing factors of these inequities.
Similar content being viewed by others

Introduction
Malnutrition among children and infants is a leading public health dilemma that causes half of all death of children each year, which may occur due to a lack of diversity, quantity, and quality of food intake1,2,3. Children with malnutrition are at greater risk of childhood diseases like diarrheal illnesses and contaminations, reduced adult height, and mental and physical growth hindrance, which may hamper educational accomplishment, consequently leading to minimal economic efficiency4,5,6. In several countries, nearly one-fourth of these children are not receiving the balanced nutrition they require to grow appropriately, specifically in the first 1000 days3,7. Balanced nutrition through optimum infant and young child feeding (IYCF) practices2, particularly in the early stages of life, ensure growth and increases the children's survival rate8 by reducing the risk of several chronic and lifestyle-related diseases9,10,11. Additionally, appropriate IYCF practices are significantly related to children's social, educational, and cognitive growth and improvement9,12. According to World Health Organization (WHO) and the United Nations Children’s Fund (UNICEF), minimum dietary diversity includes eight food groups, from which a child needs to take at least five food groups to receive the optimal level of food required for their overall growth13. Increasing dietary diversity is essential for sufficient intake of vital nutrients and ensuring a high-quality diet14,15, which is the key to evaluating nutritional sufficiency among young children and infants16. Thus, to ensure enough nutrition, prevent malnutrition, and promote healthy growth and development from infancy to adulthood, a diet from diversified food groups is essential15,17.
Even though dietary diversity is well recognized as an essential component, only 29 percent of children aged 6–23 months get the facility of the criteria of dietary diversity around the world18. Due to this problem, approximately149 million (22%), 45 million (7%), and 39 million (6%) under-five children are affected by stunting, wasting, and overweight, respectively, across the world19,20. In Bangladesh, among children aged under five years old, 31% are stunted, 8% are wasted, 2% are overweighted, and 22% are underweighted, respectively21. Although the fourth Health, Population, and Nutrition Sector Program (HPNSP) aims to decline stunting from 36 to 25% by 2022, the rate is still not yet achieved and remains unacceptable21. Nguyen et al., argued that socioeconomic status has a crucial impact in ensuring MDD and the households with richest quintiles has more access to and ability to afford the foods from diversified groups than the lowest quintiles22. While a previous study conducted in rural Bangladesh found a causal association between low dietary diversity and child stunting23. Understanding the socioeconomic disparities in having MDD might be crucial for improving child health and well-being given the high rates of malnutrition, stunting, underweight, and wasting in Bangladesh24. Hence, knowing the reasons behind inadequate diet and socioeconomic inequalities in MDD is a possible way to find solutions to mitigate these problems.
The MDD in South Asia varies across countries25, while MDD in Bangladesh is increased from 23.8% in 2011 to 28.8% in 201824. The MDD and, eventually, child nutrition has been found to be closely correlated with a number of factors in previous research. According to previous studies in Bangladesh, dietary diversity is associated with age of the child, maternal age, family income, and place of residence17. Another study by Sarah and Tina found that household wealth status, maternal education, antenatal care visit, and exposure to media were significant determinants of MDD among Bangladeshi children24.
Although some studies have estimated the influencing factors of children's minimum dietary diversity utilizing Demographic and Health Survey (DHS) data24,26,27, there exists little information on socioeconomic inequalities in minimum dietary diversity among Bangladeshi children aged 6–23 months. Even, as per our knowledge, no research in Bangladesh has been conducted to examine whether socioeconomic inequalities in MDD among children exists or not. However, understanding inequalities in MDD is needed in order to develop comprehensive intervention to improve child health and nutritional status. To enhance the understanding of the socioeconomic inequality gap, this study aimed to assess the prevalence of minimum dietary diversity among Bangladeshi children aged 6–23 months and evaluate the inequalities and relative significance of socioeconomic resources. Our focus was to create evidence and a baseline by identifying the contributing factors of socioeconomic inequalities in MDD among Bangladeshi children so that the policymakers and public health experts can design appropriate intervention focusing on the most contributing factors of inequalities to enhance the children’s dietary diversity and hence the overall child health.
Methods
Data source and sampling method
The study used the data of 2017–2018 Bangladesh Demographic and Health Survey. The survey was conducted under the National Institute of Population Research and Training (NIPORT), Research and Development operational plan of 4th Health, Population and Nutrition Sector Program (HPNSP), and Health education and Family welfare Division of the Ministry of Health and Family Welfare under Training. The sampling frame used in the survey is the list of enumeration areas (EAs) of the 2011 Population and Housing Census of the People’s Republic of Bangladesh which was given by the Bangladesh Bureau of Statistics (BBS). The two-stage stratification of households were done in which in the first stage using probability proportional to EA size 675 EAs (425 from rural areas and 250 from urban areas) were selected. To obtain sampling frame for second stage a complete household listing was carried out in the selected EAs. In the second stage, on an average 30 households were selected in every EAs to provide an estimate of all the demographic and health indicators. Then all the eligible women aged 15–49 years were interviewed to obtain the data. More information regarding the sampling methodology can be found in 2017–2018 BDHS report21. Data regarding child nutritional status were asked to the ever married women having children.
Outcome variable
Minimum dietary diversity is the outcome variable of the study. The variable was coded as “Yes” if the child aged 6–23 months received food from at least 5 groups out of 8 groups of food in the previous day of the survey otherwise the variable was coded as “No”21. The eight food groups are (1) Breastfeeding (2) Grains, roots and tubers (3) Legumes and nuts (4) Dairy products (milk, yogurt, cheese) (5) Flesh foods (meat, fish, poultry and liver/organ meats) (6) Eggs (7) Fruits and vegetables rich with vitamin A (8) Other fruits and vegetables.
Explanatory variables
Household wealth status (Poorest, poorer, middle, higher, highest) and mother education level (No education, primary, secondary, higher) are considered as the main explanatory variables as these variables were considered to calculate the concentration index of dietary diversity. Along with mother education level and wealth status, age group (15–19, 20–24, 25–29, 30–49), residence (urban, rural), partner education level (No education, primary, secondary, higher), currently working (Yes, No), post-natal visited (Yes, No), number of ANC visits (< 4 visits, ≥ 4 visits), sex of the child (Male, Female), number of living children (1, 2, ≥ 3 children), media exposure (Yes, No), and division (Barisal, Chittagong, Dhaka, Khulna, Mymensingh, Rajshahi, Rangpur, Sylhet) are also considered to conduct the decomposition of the observed concentration index. In addition, child’s age was also categorized into 6–12, 13–18, and 19–23 to observe the concentration in the age groups. BDHS calculated the wealth index based on several indicator variables. These indicators consisted of the variables relating household’s asset, characteristics, ownerships and utility services; such as materials of floor, materials of roof, availability of technological assets like television, mobile phones, and refrigerators, water source for drinking, cooking and washing, type of cooking fuel used, toilet facilities, and land ownership, livestock ownership, etc. Then principal component analysis was used on those indicator variables after standardizing the variables and wealth index was calculated using the calculated factor loadings. Then the wealth index was ordered and divided into five twenty percent sections. The sections are named as poorest, poorer, middle, richer, richest where lowest section was termed as poorest and the highest section was termed as richest28. The variable media exposure was coded as “Yes” if the woman reads newspaper/magazine at least once a week or watches television at least once a week or listens to radio at least once a week otherwise the variable was coded as “No”. The variable number of living children was categorized into 1, 2, and ≥ 3 children using the variable v218 in the child dataset. Number of ANC visits for the recent child of the respondent was categorized into < 4 visits and ≥ 4 visits using the variables m14 in the child dataset. The variable currently working and post-natal visited was coded using the variable v714 and m70 in the child dataset respectively. The rest of the variables are used as recorded by BDHS. All the variables in the study are selected based on the previous literatures addressing minimum dietary diversity or any Infant and Young Child Feeding (IYCF) practices15,17,24,29,30.
Statistical analysis
Before conducting the analysis the raw data was filtered such as at the first stage data of 6–23 months aged child were filtered. The second sage filtration is that the missing and don’t know responses deletion regarding the variables used to compute dietary diversity. Then in the successive stages some other filtration were applied. At last data of size 2,385 children (unweighted) were obtained. The complete process of filtration and how many data deleted in each stage of filtration is depicted in Fig. 1. The characteristics of the data and the distribution of dietary diversity among the explanatory variables are tabulated and mapped.

Flowchart of the how the used sample size ultimately reached.
To see whether there is an inequality in having minimum dietary diversity with respect to mother education level and wealth status, concentration curves were plotted. The concentration curve of minimum dietary diversity was also obtained with respect to mother’s education level and wealth status for each age group of the child. Concentrative curve with respect to wealth status shows the inequality in minimum dietary diversity by plotting the cumulative proportion of having minimum dietary diversity against the cumulative proportion of respondents regarding wealth status. A 45° line indicates the line of equality and any deviation from the line indicates the presence of inequality. If the concentration curve is below the line of equality it indicates that having minimum dietary diversity is concentrated among the respondents with higher wealth status and the concentration curve above the line of equality indicates that having minimum dietary diversity is concentrated among the respondents with lower wealth status. Similarly the concentrative curve with respect to mother education level is plotted and interpreted in similar way.
To quantify the level of concentration, concentration index (CIX) was calculated. The formula developed by Kakwani31, Jenkins32, and Kakwani et al.33 was used to calculate the CIX which is known as convenient covariance approach. The formula as follows-
where \(\mu\) is the weighted mean of the indicator which concetration to be caculated in this case it is the dietary diversity; r is the fractional rank of people in the distribution of variable by which concentration will be calculated (Here it is education level and wealth status); h represents the variable which concentration is to be calculated in this study it is media exposure; \(cov(h,r)\) represents the covariance between h and r. CIX takes values within the closed interval of -1 and + 1. The closer the value of CIX to + 1 the higher the concentration in the upper quantile of the variable by which concentration is calculated and closer the value of CIX to -1 the higher the concentration in the lower quantile of the variable by which concentration is calculated.
Finally, to see the contribution of explanatory variables on the CIX, decomposition of CIX with respect to the explanatory variables were conducted. To do the decomposition the method developed by O’Donnell et al.34 was used. The method starts by fitting the following regression line-
where \({\beta }_{k}\) is the coefficient of kth explanatory variable, \({X}_{k}\) is the kth explanatory variable and \(\varepsilon\) is the random error term.
Now using the results from above regression model the CIX for dietary diversity can be decomposed as
where \({\overline{X} }_{k}\) is the average of kth explanatory variable, \({C}_{k}\) is the concentration for kth explanatory variable, \({\beta }_{k}{\overline{X} }_{k}/\mu\) is the elasticity of dietary diversity with respect to kth explanatory variable, \({GC}_{\epsilon }/\mu\) represents the part of CIX that cannot be explained by the explanatory variables and all other notations hold their usual meaning. After performing the decompostion the percentage of contribution of each variables were plotted. Furthermore the concentration of the components of minimum dietary diversity was observed through calculating concentration curve and index with respect to wealth status and education level of the mothers. All the analysis were conducted using software R version 4.1.3 and Stata version 16. All the p-values where compared with 0.05 level of significance.
Ethical approval
Secondary data set was used from the Demographic and Health Surveys (DHS) Programme for this study which is publicly available upon suitable request; therefore, further ethical approval was not required. Details of the ethical procedures followed by the DHS Program can be found in the BDHS report. All the procedures were performed in accordance with the relevant guidelines and regulations.
Results
Background characteristics
After the data cleaning data of 2,405 (weighted) children along with the characteristics of their parents are obtained. In the sample, 35.21% women belonged to age group 20–24 years, 48.86% women had secondary level of education, 74.01% resided in rural areas, and 55.80% were media exposed. Data contained information about 51.81% male children and 48.19% female children. There was 38.98% child belonging to age group 6–12 months, 34.47% belonging to 13–18 months age group, and rest 26.55% belonged to 19–23 months. Detailed presentation of the characteristics of the sample can be found in Table 1.
Prevalence of minimum dietary diversity
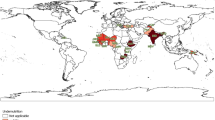
The overall weighted prevalence of minimum dietary diversity was 37.47%. Dietary diversity of children is 39.32% prevalent with mother’s belonging to age group 20–24, 54.52% prevalent with mother’s having higher education level, and 52.16% prevalent with mother’s having wealth status (Table 1). From Fig. 2, it can be seen that minimum dietary diversity in Bangladeshi children was most prevalent in Rangpur division (47.08%) and least in Sylhet division (30.21%).

Distribution of minimum dietary diversity across eight divisions of Bangladesh. The map was created using R version 4.2.1 (https://cran.r-project.org).
Inequalities in minimum dietary diversity
From the concentration curve of dietary diversity against the wealth status it can be observed that the curve is below the 45° line so the minimum dietary diversity of children is more concentrated among the mother with higher wealth status (Fig. 3). The CIX regarding wealth status was 0.1211 and the p-value (< 0.05) indicates the significance of CIX. Therefore, minimum dietary diversity of children is significantly concentrated among the higher wealth status respondents. Similarly, from the Fig. 4 with the value of CIX and associated p-value, it can be concluded that minimum dietary diversity of children is significantly concentrated among the mother with upper education level.

Concentration curve of dietary diversity against the wealth status.

Concentration curve of dietary diversity against the education level.
Inequalities in the components of minimum dietary
From the concentration curve of breastfeeding against the wealth status and education level of mothers, breasting is significantly concentration among the lower wealth status respondents whereas with the education level of the mothers it is not significantly concentrated. The foods groups dairy products, eggs, Vitamin A rich vegetables and fruits, other vegetables and fruits, legumes are significantly concentrated among higher wealth status and higher education level mothers. The food groups flesh and grains are not significantly concentrated with respect to wealth status but significantly concentrated with respect to education level (please see Supplementary Figs. S1–S16 online).
Inequalities in minimum dietary diversity by age group
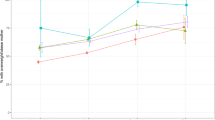
From the concentration curve of minimum dietary diversity with respect to both wealth and educational status of mother, we observed that MDD is concentrated among the children having mothers with higher educational and wealth status in each age group of the child. The value of CIX was highest in the 6–12 months child age group with respect to both educational and wealth status and lowest in 13–18 months age group for both educational and wealth status (please see Supplementary Figs. S17–S22 online).
Decomposition of concentration index
The decomposition of CIX in respect to wealth status and education level were presented in Tables 2 and 3, respectively. Decomposition of CIX was done to see the contribution of different explanatory variables on inequalities. The column percentage of contribution in both the table represents the relative contribution of each explanatory variables on the overall CIX. A negative percentage of contribution indicates that the factor helps to decrease the concentration and a positive percentage of contribution indicates that the variable helps to increase the observed inequality. In the observed CIX due to wealth status which is 0.1211, 49.47% contributed by wealth status, 25.06% contributed by education level of mother, 20.41% contributed by the number of ANC visits, 11.07% contributed by media exposure, and 9.75% contributed by mother’s partner education level. Overall, those were the factor which contributed most and increased the observed inequality regarding wealth status. The contribution of post-natal visit is − 6.69% which indicating that post-natal visit helps to decrease the observed CIX. Furthermore, only 2.08% of the observed CIX cannot be explained by the explanatory variables.
Similarly, the decomposition of CIX computed regarding education level of mother can be interpreted. From Table 3 it can be found that in the CIX = 0.1341, 52.68% contributed by education level of mother, 18.07% contributed by wealth status, 14.69% contributed by the variable number of ANC visits, 10.79% contributed by mother’s partner education level and 5.36% contributed by media exposure. These explanatory variables contributed most in the inequality and on its increase. Similar scenario can be observed regarding variable post-natal care visit. The percentage of contribution of the variables are presented in an order in the Figs. 5 and 6. Only 0.95% of this CIX could not be explained by the explanatory variables.

Percentage of contribution of variables on the Concentration Index of dietary diversity resulting from education level.

Percentage of contribution of variables on the Concentration Index of dietary diversity resulting from wealth status.
Discussion
In the current study utilizing the large survey data from Bangladesh, we observed significant wealth-based and education-based inequality in children’s MDD. The factors such as parental (mothers’ and fathers’) education level, household wealth status, number of ANC visits and media exposure were found to be major contributors to the socioeconomic inequality in a child's MDD.
The results of our study are consistent with other national-level investigations conducted in other countries35,36, indicating a substantial relationship between the age of the child and dietary diversity. Older infants' readiness to take food in a variety of forms (such as tastes and textures) and their better acquaintance with food than younger infants could be two possible explanations for why they consume a more varied diet37. When looking at the inequalities by age groups of children with respect to both maternal education and household wealth status, higher disparities was observed among children from 6 to 12 months age group. This higher socioeconomic inequalities could be another explanation of why MDD was lower among children of lower age group; this finding may indicate the importance of education and socio-economic status in relation to meet the MDD among Bangladeshi children. Besides, further investigation is warranted to find out the in-depth reasons of higher inequalities in having MDD among children from lower age group in Bangladesh.
In this study, mothers’ and their partners’ education played a substantial role in the SES-related discrepancy for MDD among children. Educated caregivers may recognize the importance of food diversity in their children's development. This finding is consistent with the findings of other investigations38,39. A similar study in India found that maternal education was associated with consumption of essential food items and all food groups, and showed higher odds of adequately diversified dietary intake40.
The media as a source of information was also found to have a substantial contribution in SES-related inequalities in MDD. Media exposure has recently been suggested as an important predictor of women's empowerment, which may increase women's access to and control over resources41. Previous research has shown that the media can help people get better information and promote dietary diversity42,43. The circulation through mass media in many countries is shown to be a reliable source of delivering nutrition-related information and influence individuals’ behaviours44,45. In this regard, in the decomposition of contributing factors to education-based inequalities in receiving MDD, wealth status contributed only 18.07% whereas, in case of wealth-based inequalities, education contributed 25.06%. This suggests that education can play an important role than wealth in bringing positive outcomes related to MDD. Therefore, as reported in previous intervention studies46, counseling through post-natal care centres and media exposure may improve child dietary diversity even in areas with no food security activities.
The worst wealth status was linked to a low MDD in the current study, whereas the children from highest wealth quintile were observed to have a higher prevalence of MDD. This finding may be attributed to the resource availability where a wealthy family might have the financial capacity to buy a variety of items and feed their children a diversified diet. This is supported by previous evidence in other low- and middle-income countries where children from the poorest households being most at risk of not receiving the MDD11,36,45,47,48. Income has a good effect on children's intake of a variety food, according to other studies in India40,49,50,51. It is also evident from previous studies that people from lowest wealth quintile in Bangladesh do not utilize the health-care services if their children’s particular health problem is not severe because of not having proper financial security52.
Post-natal visits and ANC visits had a significant contribution to SES-related inequality in MDD. This may be because during these visits, mothers get nutrition awareness which helps in better MDD outcome53,54. Previous studies also suggested that access to ANC during pregnancy is indicative of meeting MDD25. Similarly, maternal visits to ANC reflected maternal access to services related to health and nutrition and they might obtain information about appropriate child feeding through a counselling session during ANC55.
Furthermore, children from urban communities in Bangladesh were more likely to receive MDD. This might be due to the fact that poor nutritional knowledge and awareness, poor resources, lower education rate and limited income opportunity are available in rural areas. Therefore, awareness building interventions and income-generating activities among people in rural areas may enrich the nutritional status of the children27. However, rural region was found to be a protective factor for MDD in multiple previous studies in Bangladesh, which is attributed to the increased access to livestock or home-grown produce with relatively low inputs by rural mothers24,26,56. Thus, future studies are warranted that focus on factors influencing rural–urban gradient in attaining MDD among Bangladeshi children. Further, administrative regions were significant influencing factors of SES-based differences in MDD in this study, and this suggests the need for studies based on regional disparities in MDD among children in Bangladesh.
The important limitations of this study include the cross‐sectional design which limits the causal direction of observed factors and the use of 24‐h recall data for MDD. Although 24-h maternal recall is recommended by the WHO to assess child dietary intake57, the measurement is subject to response bias, including errors in recall and social desirability. Similarly, the dietary diversity also relates to the aspects of food security, affordability and accessibility which are not covered in this study. Moreover, because this was a secondary data analysis, we were limited in the measurements available for women empowerment and are not included in the analyses. Future studies could expand on these, and bring out the influence of maternal decision-making power and other aspects of woman empowerment on SES- and education-based differences in children’s MDD. Despite the abovementioned limitations, inclusion of a large number of factors in the multivariable analysis that strengthens the validity of the findings was a major strength of this study. Also, in addition to the SES-related inequality in MDD, the current study analyzed the education-based inequality in MDD which provides a clearer picture of the contribution of several factors to differences in MDD among Bangladeshi children. Finally, since the study utilized data of a large sample from a nationally representative household survey, the results can be generalized at the country level.
In conclusion, there was significant wealth- and education-based inequalities in MDD among Bangladeshi children aged 6–23 months. The significant contributors to such inequalities included parents’ education, household wealth status, mothers’ media exposure, ANC visits and residential status. The findings suggest that these can be possible targets of future interventions to improve MDD among Bangladeshi children, particularly among those who belong to economically poor households or born to less educated mothers.
Data availability
This study utilized publicly available Demographic and Health Surveys Program dataset of Bangladesh. The dataset of BDHS 2017-18 is available upon request in the following website: http://dhsprogram.com/data/available-datasets.cfm. As a third-party user, we do not have permission to share the data publicly on any platform.
Abbreviations
- MDD:
-
Minimum dietary diversity
- SES:
-
Socioeconomic status
- BDHS:
-
Bangladesh demographic and health survey
- IYCF:
-
Infant and young child feeding
- NIPORT:
-
National institute for population research and training
- EAs:
-
Enumeration areas
- PSU:
-
Primary sampling unit
- CIX:
-
Concentration Index
- CI:
-
Confidence interval
- ANC:
-
Antenatal care
References
Arsenault, J. E. et al. Very low adequacy of micronutrient intakes by young children and women in rural Bangladesh is primarily explained by low food intake and limited diversity. J. Nutr. 143, 197–203 (2013).
Gizaw, G. & Tesfaye, G. Minimum acceptable diet and factor associated with it among infant and young children age 6–23 months in north Shoa, Oromia region, Ethiopia. Int. J. Homeop. Nat. Med. 5, 1 (2019).
UNICEF. The State of the World’s Children 2019: Children, Food and Nutrition: Growing Well in a Changing World (UNICEF, 2019).
Lomborg, B. Global Crises, Global Solutions (Cambridge University Press, 2004).
Maluccio, J. & Flores, R. Impact Evaluation of a Conditional Cash Transfer Program: The Nicaraguan Red de Protección Social (Intl Food Policy Res Inst, 2005).
World Health Organization. Improving Nutrition Outcomes with Better Water, Sanitation and Hygiene: Practical Solutions for Policies and Programmes (WHO, 2015).
Nkoka, O., Mhone, T. G. & Ntenda, P. A. Factors associated with complementary feeding practices among children aged 6–23 mo in Malawi: An analysis of the Demographic and Health Survey 2015–2016. Int. Health 10, 466–479 (2018).
Black, R. E. et al. Maternal and child undernutrition: Global and regional exposures and health consequences. Lancet 371, 243–260 (2008).
Black, R. E. et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 382(9890), 427–451. https://doi.org/10.1016/S0140-6736(13)60937-X (2013).
Gluckman, P. D. et al. Towards a new developmental synthesis: Adaptive developmental plasticity and human disease. Lancet 373, 1654–1657 (2009).
Harvey, C. M., Newell, M.-L. & Padmadas, S. S. Socio-economic differentials in minimum dietary diversity among young children in South-East Asia: Evidence from Demographic and Health Surveys. Public Health Nutr. 21, 3048–3057 (2018).
Belay, D. G., Taddese, A. A. & Gelaye, K. A. Does socioeconomic inequality exist in minimum acceptable diet intake among children aged 6–23 months in sub-Saharan Africa? Evidence from 33 sub-Saharan African countries’ demographic and health surveys from 2010 to 2020. BMC Nutr. 8, 1–13 (2022).
World Health Organization. Global Nutrition Monitoring Framework: Operational Guidance for Tracking Progress in Meeting Targets for 2025 (WHO, 2017).
Habte, T. Y. & Krawinkel, M. Dietary diversity score: A measure of nutritional adequacy or an indicator of healthy diet. J. Nutr. Health Sci. 3, 303 (2016).
Solomon, D., Aderaw, Z. & Tegegne, T. K. Minimum dietary diversity and associated factors among children aged 6–23 months in Addis Ababa, Ethiopia. Int. J. Equity Health 16, 1–9 (2017).
Sekartaji, R. et al. Dietary diversity and associated factors among children aged 6–23 months in Indonesia. J. Pediatr. Nurs. 56, 30–34 (2021).
Kundu, S. et al. Exploring the factors associated with dietary diversity of children aged 6–59 months in some rural and slum areas of Bangladesh amid the COVID-19 pandemic: A mixed-effect regression analysis. Curr. Dev. Nutr. 6, 109 (2022).
Who, U., Usaid, A. & Aed, U. Indicators for Assessing Infant and Young Child Feeding Practices (World Health Organization, 2008).
Paramashanti, B. A., Dibley, M. J., Alam, A. & Huda, T. M. Wealth-and education-related inequalities in minimum dietary diversity among Indonesian infants and young children: a decomposition analysis. Glob. Health Action 15, 2040152 (2022).
World Health Organization, U. N. C. & Fund, W. B. Levels and Trends in Child Malnutrition: UNICEF/WHO/The World Bank Group Joint Child Malnutrition Estimates: Key Findings of the 2021st edn. (WHO, 2021).
National Institute of Population Research and Training & ICF. Bangladesh Demographic and Health Survey 2017–2018: Key Indicators (WHO, 2019).
Nguyen, P. H. et al. Maternal and child dietary diversity are associated in Bangladesh, Vietnam, and Ethiopia. J. Nutr. 143, 1176–1183 (2013).
Rah, J. H. et al. Low dietary diversity is a predictor of child stunting in rural Bangladesh. Eur. J. Clin. Nutr. 64, 1393–1398 (2010).
Blackstone, S. & Sanghvi, T. A comparison of minimum dietary diversity in Bangladesh in 2011 and 2014. Matern. Child Nutr. 14, e12609 (2018).
Senarath, U. et al. Comparisons of complementary feeding indicators and associated factors in children aged 6–23 months across five South Asian countries. Matern. Child Nutr. 8, 89–106 (2012).
Sheikh, N. et al. Infant and young child feeding practice, dietary diversity, associated predictors, and child health outcomes in Bangladesh. J. Child Health Care 24, 260–273 (2020).
Kabir, I. et al. Determinants of inappropriate complementary feeding practices in infant and young children in Bangladesh: secondary data analysis of demographic health survey 2007. Matern. Child Nutr. 8, 11–27 (2012).
Rutstein, S. O. & Johnson, K. The DHS Wealth Index DHS Comparative Reports No. 6 (ORC Macro, 2004).
Jemal, K. & Awol, M. Minimum dietary diversity score and associated factors among pregnant women at Alamata General Hospital, Raya Azebo Zone, Tigray Region, Ethiopia. J. Nutr. Metab. 2019, 1–10 (2019).
Demilew, Y. M., Tafere, T. E. & Abitew, D. B. Infant and young child feeding practice among mothers with 0–24 months old children in Slum areas of Bahir Dar City, Ethiopia. Int. Breastfeed. J. 12, 1–9 (2017).
Kakwani, N. C. Income Inequality and Poverty (World Bank, 1980).
Jenkins, S. Calculating income distribution indices from micro-data. Natl. Tax J. 41, 139–142 (1988).
Kakwani, N., Wagstaff, A. & Van Doorslaer, E. Socioeconomic inequalities in health: measurement, computation, and statistical inference. J. Econ. 77, 87–103 (1997).
Wagstaff, A., O’Donnell, O., Van Doorslaer, E. & Lindelow, M. Analyzing Health Equity Using Household Survey Data: A Guide to Techniques and their Implementation (World Bank Publications, 2007).
Aemro, M., Mesele, M., Birhanu, Z. & Atenafu, A. Dietary diversity and meal frequency practices among infant and young children aged 6–23 months in Ethiopia: A secondary analysis of Ethiopian demographic and health survey 2011. J. Nutr. Metab. 2013, 1–10 (2013).
Senarath, U., Godakandage, S. S., Jayawickrama, H., Siriwardena, I. & Dibley, M. J. Determinants of inappropriate complementary feeding practices in young children in Sri Lanka: Secondary data analysis of demographic and health survey 2006–2007. Matern. Child Nutr. 8, 60–77 (2012).
Mura Paroche, M., Caton, S. J., Vereijken, C. M., Weenen, H. & Houston-Price, C. How infants and young children learn about food: A systematic review. Front. Psychol. 8, 1046 (2017).
Harding, K. L., Aguayo, V. M., Masters, W. A. & Webb, P. Education and micronutrient deficiencies: An ecological study exploring interactions between women’s schooling and children’s micronutrient status. BMC Public Health https://doi.org/10.1186/s12889-018-5312-1 (2018).
Srivastava, S. & Kumar, S. Does socio-economic inequality exist in micro-nutrients supplementation among children aged 6–59 months in India?. Evid. Natl. Fam. Health. 1, 1–12 (2021).
Agrawal, S. et al. Socio-economic patterning of food consumption and dietary diversity among Indian children: Evidence from NFHS-4. Eur. J. Clin. Nutr. 73, 1361–1372 (2019).
Mahmud, S., Shah, N. M. & Becker, S. Measurement of women’s empowerment in rural Bangladesh. World Dev. 40, 610–619 (2012).
Tegegne, M., Sileshi, S., Benti, T., Teshome, M. & Woldie, H. Factors associated with minimal meal frequency and dietary diversity practices among infants and young children in the predominantly agrarian society of Bale zone, Southeast Ethiopia: A community based cross sectional study. Arch. Public Health https://doi.org/10.1186/s13690-017-0216-6 (2017).
Belew, A. K., Ali, B. M., Abebe, Z. & Dachew, B. A. Dietary diversity and meal frequency among infant and young children: A community based study. Ital. J. Pediatr. https://doi.org/10.1186/s13052-017-0384-6 (2017).
Dafursa, K. & Gebremedhin, S. Dietary diversity among children aged 6–23 months in Aleta Wondo District, Southern Ethiopia. J. Nutr. Metab. 2019, 1–10 (2019).
Paramashanti, B. A., Huda, T. M., Alam, A. & Dibley, M. J. Trends and determinants of minimum dietary diversity among children aged 6–23 months: A pooled analysis of Indonesia demographic and health surveys from 2007 to 2017. Public Health Nutr. 1, 1–12 (2021).
Kuchenbecker, J., Reinbott, A., Mtimuni, B., Krawinkel, M. B. & Jordan, I. Nutrition education improves dietary diversity of children 6–23 months at community-level: Results from a cluster randomized controlled trial in Malawi. PLoS ONE 12, e0175216 (2017).
Joshi, N., Agho, K. E., Dibley, M. J., Senarath, U. & Tiwari, K. Determinants of inappropriate complementary feeding practices in young children in Nepal: Secondary data analysis of demographic and health survey 2006. Matern. Child Nutr. 8, 45–59 (2012).
Na, M., Aguayo, V. M., Arimond, M. & Stewart, C. P. Risk factors of poor complementary feeding practices in Pakistani children aged 6–23 months: A multilevel analysis of the demographic and health survey 2012–2013. Matern. Child Nutr. 13, e12463 (2017).
Agrawal, S. & Agrawal, P. Vitamin A supplementation among children in India: Does their socioeconomic status and the economic and social development status of their state of residence make a difference?. Int. J. Med. Public Health https://doi.org/10.4103/2230-8598.109322 (2013).
Patel, A. et al. Determinants of inappropriate complementary feeding practices in young children in India: Secondary analysis of national family health survey 2005–2006. Matern. Child Nutr. https://doi.org/10.1111/j.1740-8709.2011.00385.x (2012).
Ng, C. S., Dibley, M. J. & Agho, K. E. Complementary feeding indicators and determinants of poor feeding practices in Indonesia: A secondary analysis of 2007 demographic and health survey data. Public Health Nutr. https://doi.org/10.1017/S1368980011002485 (2012).
Mahumud, R. A., Sultana, M. & Sarker, A. R. Trend of healthcare expenditures in Bangladesh over last decades. Am. J. Econ. Financ. Manag. 1, 97–101 (2015).
Hidru, H. D., BerwoMengesha, M., Hailesilassie, Y. & TekuluWelay, F. Burden and determinant of inadequate dietary diversity among pregnant women in Ethiopia: A systematic review and meta-analysis. J. Nutr. Metab. 2020, 1–10 (2020).
Tilahun, A. G. & Kebede, A. M. Maternal minimum dietary diversity and associated factors among pregnant women, Southwest Ethiopia, 2021. BMC Nutr. 7, 1–10 (2021).
Sebayang, S. K. et al. Determinants of age-appropriate breastfeeding, dietary diversity, and consumption of animal source foods among Indonesian children. Matern. Child Nutr. 16, e12889 (2020).
Stewart, C. P., Iannotti, L., Dewey, K. G., Michaelsen, K. F. & Onyango, A. W. Contextualising complementary feeding in a broader framework for stunting prevention. Matern. Child Nutr. 9, 27–45 (2013).
World Health Organization. Indicators for Assessing Infant and Young Child Feeding Practices: Part 2: Measurement (WHO, 2010).
Acknowledgements
Authors want to thank Demographic Health Surveys (DHS) for providing the datasets with no cost and permit us for using the data for independent research.
Author information
Authors and Affiliations
Contributions
S.K.: Conceptualization, methodology, data curation, formal analysis, writing-original draft, writing-review & editing, supervision; P.D.: Conceptualization, methodology, data curation, formal analysis, writing-original draft, writing-review & editing, supervision; M.A.R.: Writing-original draft, writing-review & editing; M.H.A.B.: Writing-original draft, writing-review & editing; K.F.: Writing-review & editing; M.A.I.: Writing-original draft, writing-review & editing; S.S.: Writing-original draft, writing-review & editing; T.M.: Writing-original draft, writing-review & editing; R.D.: Writing-original draft, writing-review & editing; A.H.: Writing-review & editing, supervision. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kundu, S., Das, P., Rahman, M.A. et al. Socio-economic inequalities in minimum dietary diversity among Bangladeshi children aged 6–23 months: a decomposition analysis. Sci Rep 12, 21712 (2022). https://doi.org/10.1038/s41598-022-26305-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-26305-9
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
