
Abstract
Cataract surgery is among the most common medical procedures, and accurate ocular biometry measurements are key for successful visual outcome. The current study evaluated data obtained by the Eyestar 900, Anterion, IOLMaster700 biometers and the Pentacam corneal topographer. Compared values were axial length (AL), anterior chamber depth (ACD), steep- and flat-K, cylinder and axis. Clinical impact was assessed by calculating intraocular lens (IOL) power using the mean values of every parameter and the Barrett and Kane formulas, stratified by device and amount of cylinder. IOL was re-calculated for each device substituting Pentacam K-values. This study included 196 eyes (98 participants) of cataract surgery candidates. When comparing the IOLMaster to the Eyestar (157 eyes), no difference was found in mean AL or ACD measurements (P > 0.05). Steep-K measurements differed between these devices and the Pentacam (P = 0.01). AL and ACD measurements differed between the IOLMaster and Anterion (38 eyes; P < 0.05). Strong correlations (range 0.72–0.99) were found between all four devices. Bland–Altman analysis demonstrated excellent agreement between biometry devices other than ACD between the IOLMaster and Eyestar. Calculated IOL power was 0.50–1.00 diopter (D) lower with the IOLMaster. Cylinder power was 0.75D higher in all biometers when Pentacam K-values were substituted.
Similar content being viewed by others


Introduction
Cataract surgery, in which the opaque crystalline lens is replaced with an artificial intraocular lens (IOL), is one of the most common and successful medical procedures performed worldwide1,2. Ocular biometric parameters are measured before surgery in order to calculate the optimal IOL for the individual patient. The axial length (AL) of the eye, anterior chamber depth (ACD) and corneal curvature (K) measurements strongly impact the calculated IOL3. Accurate pre-operative biometric measurements are considered one of the most important factors for successful surgical result4, especially with the evolution of toric and multifocal IOLs which require the utmost surgical precision. As new or updated biometric devices are brought into clinical practice, it is important to thoroughly understand their capabilities, agreement with existing devices, and impact on IOL selection.
Swept-source optical coherence tomography (SS-OCT) is a non-invasive imaging modality that scans biological structures at high resolution, speed and sensitivity. The output volume of scans enables three-dimensional analysis of the given structure5. Anterior segment OCT (ASOCT) scans the cornea, sclera and lens, thereby providing vital information for IOL selection in cataract surgeries. The Eyestar 900 (Haag Streit Diagnostics, Koeniz, Switzerland) and Anterion (Heidelberg Engineering, Heidelberg, Germany) are two recently developed biometers based on the SS-ASOCT technology. In contrast, the Pentacam corneal tomographer (Oculus Inc., Wetzlar, Germany) measures the K values using a rotating Sheimpflug camera that acquires cross-sectional scans of the cornea6. In the clinic, when biometric devices fail to produce K-readings due to highly irregular corneas, corneal topography values are obtained and used to calculate the suggested IOL. While several studies evaluating the ocular measurements have already shown good repeatability and agreement between established biometers7,8, differences in specific parameters such as anterior chamber depth (ACD) and corneal curvatures (K) have been reported relative to SS-ASOCT devices such as the IOLMaster 700 and corneal tomographers such as the Pentacam9,10,11. Additionally, there is limited data in the literature as to whether these differences have any clinical impact, i.e., whether they affect the final selection of IOL12,13. The purpose of this study was therefore to compare the ocular parameters measured by these two recent biometers to those measured by the IOLMaster 700 (Carl Zeiss Meditec, Jena, Germany), the first SS-OCT-based biometric device and one of the most commonly used devices for pre-cataract surgery measurements14. To further investigate the accuracy of SS-OCT corneal measurements, these values were also compared to those obtained by the Pentacam (Oculus, Wetzlar, Germany) topographer. The final lens power calculations based on the measurements of each biometric device were compared to examine the clinical impact.
Methods
This retrospective study followed the tenants of the Helsinki declaration and was approved by the institutional Helsinki Committee of Hadassah Medical Center (study number HMO-0459-18). The committee exempts retrospective research from informed consent by the participants. Data was collected from the Ophthalmology Department database and anonymized before analysis. Before biometric measurements, each participant underwent ophthalmic examination including best-corrected visual acuity (BCVA) with and without pinhole and full slit-lamp evaluation.
Ocular measurements
Identical ocular parameters were measured using three different ocular biometry devices: the The Eyestar 900 (Haag Streit Diagnostics, Koeniz, Switzerland), the Anterion (Heidelberg Engineering, Heidelberg, Germany) and the IOLMaster 700 (Carl Zeiss Meditec, Jena, Germany). The parameters compared were axial length (AL), anterior chamber depth (ACD), anterior corneal values (steep- and flat-K), cylinder (cyl) and axis. Additionally, K values were compared to those obtained by the Pentacam corneal tomographer (Oculus Inc., Wetzlar, Germany). Measurements in all four devices were performed by optometrists with both the participants’ eyes open during each measurement. In cases where more than one measurement was performed for a single participant using the same instrument, only the most recent complete measurement was included in the final analysis.
The parameters included in this study have the greatest impact on IOL calculation. Therefore, in order to assess whether any discrepancies between the different devices would result in differences in the recommended IOL, the mean values of every parameter for each biometry device were entered in the Barrett Universal II Formula15, Barrett Toric Calculator16 and Kane Formula 17 and the final IOLs were compared. Monofocal IOL formulas were used for eyes with less than 1.00 diopter (D) cylinder, and toric IOL formulas were used for eyes with ≥ 1.00D cylinder. Since corneal topographers are commonly used in cases where biometers fail to provide the K-values, such as very steep or distorted corneas, IOL calculations were repeated with the Pentacam K-values substituting the different biometers’ K-values in order to assess the impact on the final power of the suggested IOL.
Participants
All participants included in this study were cataract surgery candidates who presented at the clinic for standard biometric measurements before surgery. Excluded were participants under age 40, with missing study parameters, and/or whose ocular measurements had a standard deviation greater than 0.05 (mm or D). Participants were measured using the Eyestar 900 and IOLMaster 700 (Group A) or the Anterion and IOLMaster 700 (Group B). A subset of each group had corneal values measured also with the Pentacam. Participants were also stratified by amount of cylinder, with a cut-off level of 1.00D.
Sample size
Assuming average absolute difference between devices of 0.024 mm for AL with SD of 0.05 mm to the greatest difference in mean measurements18, the minimal paired sample size that is required is 73 eyes for each group to achieve a power of 80% and a level of significance of 5%, two sided, using the statulator sample size calculator.
Statistical analysis
The normality of the data was confirmed using the Shapiro–Wilk test. AL, ACD, flat- and steep-K, cylinder and axis were compared using paired sample t-test or Friedman test, according to the sample size. Cohen's d was performed on values that were significantly different in pairwise analysis in order to examine effect size and clinical significance. Correlation between parameters measured by different devices was evaluated with Pearson's coefficient. Mean values of AL, ACD and K’s of each device were used to calculate the recommended IOL by the Barrett Universal II Formula, Barrett Toric and the Kane calculators. IOL power was calculated using the mean parameters of each biomter and stratified by device and amount of cylinder. Bland and Altman analysis was used to identify systematic agreement between the measurements by the different devices and to identify outliers. Linear regression was used to assess the significance of agreement level between biometry devices. The analysis was performed using SPSS software (IBM SPSS Statistics, Version 27.0, Chicago. Armonk, NY: IBM Corp).
Ethical considerations
The institutional Helsinki committee exempts retrospective research from informed consent by the participants.
Results
Patient characteristics
Records of 238 eyes (119 participants) were extracted from the Eyestar 900 and Anterion devices. This data was filtered for the current study based on age and data completeness, resulting in the exclusion of 42 eyes (17.6%). Ultimately, a total of 196 eyes (98 participants, 47.9% female, mean age 68.8 ± 9.7 years, range 42–88 years) were included in this study. Participants were divided to two groups: Group A consisted of 157 eyes (79 participants, 80.6%) measured with the Eyestar and IOLMaster, with 48 eyes (24.4%) also measured by Pentacam. Group B consisted of 38 eyes (19 participants, 19.3%) measured with the Anterion and IOLMaster, with 22 eyes (11.2%) also measured by Pentacam. Table 1 describes the demographic characteristics of the study population.
Biometry results
In Group A there was no difference in mean AL values when comparing the IOLMaster (24.22 ± 2.0 mm) to the Eyestar 900 (24.2 ± 2.04 mm; P = 0.79; Cohen’s d 0.009). Mean ACD was also similar (3.34 ± 0.56 mm vs. 3.36 ± 0.56 mm, respectively; P = 0.09; Cohen’s d 0.03). No differences were found in mean flat and steep K values or in cylinder axis (Table 2). A sub-group of 48 eyes in Group A were also measured using the Pentacam. In this comparison, a difference was found in mean steep K measurements between the IOLMaster (45.02 ± 1.84D), the Eyestar (44.99 ± 1.85D) and the Pentacam (44.88 ± 1.76D) (P = 0.01). No differences were found in mean flat K values or in cylinder axis (Table 2).
In Group B, mean AL values were different when comparing the IOLMaster to the Anterion (23.68 ± 1.27 mm vs. 23.57 ± 1.27 mm, respectively; P = 0.006; Cohen’s d 0.08). Mean ACD was also different (3.27 ± 0.73 mm vs. 3.38 ± 0.78 mm; P = 0.04; Cohen’s d 0.14). No differences were found in mean flat and steep K values or in cylinder axis (Table 3). A sub-group of 22 eyes in Group B were also measured using the Pentacam. No significant differences were found in any corneal parameter between the IOMaster, Anterion and Pentacam (Table 3).
Analysis of correlations and agreements across devices
When testing the correlations between the different devices, strong correlations were found between all four devices in AL, ACD, flat and steep K values and cylinder, ranging from R = 0.72 to 0.99. (Table 4) Comparison of cylinder axes between the different devices yielded weaker correlations, ranging from R = 0.32 to 0.95 (Table 4).
Bland and Altman analysis was performed in order to assess the agreement between the biometry devices. A preliminary analysis demonstrated no difference between the IOLMaster and Eyestar and therefore AL, ACD, and flat and steep K values were all included in the agreement analysis. However, a difference between the IOLMaster and Anterion in mean AL and ACD values (P = 0.006, P = 0.04; respectively) was observed. Because these parameters did not show a useful level of agreement, there were not included in the Bland and Altman analysis.
When analyzing the linear regression line of the Bland and Altman scatter plot, IOLMaster and Eyestar values demonstrated no difference of proportional bias of scatter dots above and below the mean difference line for AL and flat and steep K values (P = 0.54, P = 0.69, P = 0.21, respectively). These devices differed in ACD values (P < 0.001), with a higher amount of ACD observations above the mean difference line. IOLmaster and Anterion flat and steep K plots were equally distributed above and below the mean difference line (P = 0.23, P = 0.18, respectively) (Fig. 1).

Bland and Altman agreement analysis of IOLMaster700, Eyestar900 and Anterion. Bland and Altman analysis of axial length, anterior chamber depth and flat and steep K in the IOLMaster vs. the Eyestar (a–d), and flat and steep K in the IOLMaster vs. the Anterion (e,f). Axial length and anterior chamber depth are measured in millimeters, and flat and steep K in diopters. (a ) No significant difference between IOLMaster and Eyestar scatter dots in axial length measurements, P = 0.54. (b) Significant difference between IOLMaster and Eyestar scatter dots in anterior chamber depth measurements, P < 0.001. (c) No significant difference between IOLMaster and Eyestar scatter dots in flat K measurements, P = 0.69. (d) No significant difference between IOLMaster and Eyestar scatter dots in steep K measurements, P = 0.21. (e) No significant difference between IOLMaster and Anterion scatter dots in flat K measurements, P = 0.23. (f) No significant difference between IOLMaster and Eyestar scatter dots in steep K measurements, P = 0.18. D Diopters, ACD anterior chamber depth, AL Axial length.
Effect of biometry measurements on IOL power calculation
In order to investigate whether the minor differences observed between the devices impacted the suggested IOL power, the mean output values of each device (Tables 2 and 3) were inserted to the Barrett Universal II Formula, Barrett and Kane toric online calculators. Parameters were consistent between calculators: Bausch & Lomb MX60 and MX60T lenses, A-Constant 119.15, surgical induced astigmatism (SIA) 0, target refraction plano, and incision location at 100° for right eye of each IOL calculation.
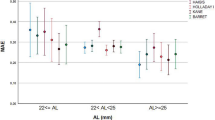
When comparing the IOLMaster and Eyestar (Group A) using the Barrett toric calculator, the calculated IOLs were 18.50/2.00D and 19.00/2.00D, respectively. Using the Kane toric calculator, both IOLs were 19.00/2.25D. In Group B, comparison of the IOLMaster and Anterion with the Barrett toric calculator yielded calculated IOLs of 19.50/2.75D and 20.00/2.75D, respectively, and with the Kane toric calculator 20.00/2.25D and 20.50/2.25D, respectively. It can be seen that the power of the suggested IOL based on the Barrett toric calculator was 0.50D lower in the IOLMaster relative to the Eyestar, but no difference was found using the Kane toric calculator. This same 0.50D difference was again found with both calculators when comparing the IOLMaster and Anterion. (Table 5) IOL calculation was then repeated with Pentacam K-values inserted in place of the K-values of each device. This resulted in a consistent increase of 0.75D in the cylinder power in all biometers with both formulas (Table 5).
Table 6 describes the calculation of suggested IOL power stratified by amount of cylinder. The cut-off was 1.00D cylinder; eyes with < 1.00D were classified as ‘low’ cylinder and monofocal IOL formulas were used to calculate the suggested IOL. Eyes with ≥ 1.00D cylinder were classified as ‘moderate-high’ cylinder and toric IOL formulas were used. In the Group A low cylinder eyes, it was found that all suggested monofocal IOLs were identical across both biometers and formulas. However, in the moderate-high cylinder eyes, the same trend observed in the non-stratified calculation was again apparent, with the IOLMaster yielding a 0.50D lower power in the suggested IOL. In the Group B low cylinder eyes, the suggested power was 0.50–1.00D lower with the IOLMaster than the Anterion. In the moderate-high cylinder eyes, the suggested IOL power was 0.50D lower with the IOLMaster than the Anterion when applying the Barrett toric calculator.
Discussion
The primary aim of this study was to compare ocular parameters measured by three recent biometers and assess the effects of any difference on the calculated IOL power for implantation in cataract surgery. The biometers’ K-values were also compared to K-values measured by a Scheimpflug-based corneal topographer.
When comparing AL and ACD measurements, a statistically significant difference was found between IOLMaster and Anterion but not between the IOLMaster and Eyestar. However, Cohen’s d analysis demonstrated that these differences were not clinically significant, and all values were highly correlated. These results are in line with recent findings by Fişuş and collaborators, which revealed discrepancies between measurements of the Anterion and IOLMaster9. Similarly, Tañá-Rivero et et al. also reported shorter ACD measurements with the IOLMaster relative to the Anterion10. Like in the current study, the differences in measurements were found to be statistically significant but were minor enough to most likely be clinically insignificant.
In addition to comparing between the different biometry devices, this study also compared K-readings of the three biometers to those of the Pentacam corneal topographer. There is clinical importance in understanding the correlation between the two modalities, because biometers can be limited in their ability to produce K-readings in cases of highly irregular corneas. In such cases, these values are often extracted from a corneal topographer or keratometer. No differences were found in the current study between any of the biometers in flat and steep K values or axes, yet when comparing these values to the Pentacam measurements, a statistically significant difference was observed between the IOLMaster, Eyestar and Pentacam in steep K values. Interestingly, the flat and steep K values were strongly correlated between all devices while axis values demonstrated low to medium correlations. Fişuş et al. did report significant differences in flat and steep K values9, but this may be due to differences in sample size. This is supported by the results presented by Tañá-Rivero et al., which did not find significant differences in K-values and were based on a sample size similar to that of the current study10. The matter of K axes has not yet been sufficiently studied and must be further investigated, as accurate axis measurements are vital for successful toric lens implantation.
In order to establish interchangeability of the devices, Bland and Altman analysis was performed. Our results indicated good agreement between all three biometers on most parameters, with a minor offset in ACD measurements between the IOLMaster and the Eyestar. Although Fişuş et al. advised against using the Anterion and IOLMaster interchangeably9, the lack of clinically significant differences between the devices leads us to suggest that these two devices can be used interchangeably, between themselves as well as with the Eyestar.
An additional aspect of the primary aim was to evaluate the clinical impact of the differences between the devices. This was achieved by calculation of the suggested IOL power based on the mean values of each device, and re-calculating with the substitution of Pentacam K-readings. Applying two commonly used IOL calculators to the entire study group, i.e., with no stratification by cylinder amount, the IOLMaster tended to yield a suggested IOL with 0.50D lower power relative to the Eyestar and Anterion. Tañá-Sanz et al. and Shetty et al. reported differences in the calculated IOL between the IOLMaster and Anterion which were statistically significant but clinically insignificant12,13. As the post-cataract surgery refractive targets suggested by the Royal College of Ophthalmology are within ± 1.00D for 85% of patients and within ± 0.50D for 55% of patients19, a difference of 0.50D can be viewed as clinically insignificant. When Pentacam K-values were inserted into the IOL calculation, the cylinder power was consistently 0.75D higher across all biometric devices. As mentioned previously, in a similar comparison Tañá-Rivero et et al. did not find significant differences in the K-values, however this study did not assess the effect on the selected IOL10. In a systematic review, Kane and Chang18 also found minor differences in measured values and calculated IOL. However, they emphasize that while devices may not differ statistically in the overall mean, they cannot be considered interchangeable due to the differences that can occur in the same eye between devices. Additionally, while this review concludes that differences between devices rarely affect the suggested IOL, there is almost no data on the Eyestar and Anterion devices that were assessed in the current study.
Further calculations were performed on sub-groups stratified by amount of cylinder. These analyses revealed differences between devices of up to 1.00D in the suggested IOL among the low cylinder eyes. While still technically acceptable according to the Royal College of Ophthalmology guidelines19, in an era where cataract surgeries can be considered refractive surgeries rather than just rehabilitative procedures, it is vital to take note of these differences and perform further studies to validate this preliminary data.
This study had several limitations, primarily due to the retrospective study design which strongly influenced the data available for analysis and caused limited and unequal sample sizes between groups. Additionally, because the study was not built prospectively, many viable measurements could not be included in the study since the patients had only undergone measurements by one biometric device. The Pentacam sub-groups and stratification by cylinder amount further limited the sample size, and therefore this data should be viewed as a preliminary basis for further research. It is worth noting that the IOLMaster and Pentacam were consistent in their biases relative to other devices in the suggested IOL power, despite the limited sample group. The main strength of this study, however, is the comparison of three biometry devices, two of which are quite recent with limited data in the literature. Moreover, the comparison of corneal measurements between SS-OCT devices and a Scheimpflug-based device further validates both technologies and also provides a quality assessment of these devices as well as clinical impact.
In conclusion, all three biometers compared in this study demonstrated strong agreement in their individual parameters, with corneal measurements correlating well to the Pentacam. However, it is important to note that the Eyestar was more similar to the IOLMaster in both AL and ACD, which are critical features in IOL calculation. Additionally, the devices differed in the suggested IOL, particularly when looking at calculations based on K-values taken from a corneal topographer, and when the study group was divided to low and moderate-high cylinder sub-groups. While these differences may not technically be considered clinically significant, they are worth consideration as the world progresses towards minimal residual post-operative refraction. Further investigation is required in order to assess the clinical impact on post-cataract surgery patients.
Data availability
The data set generated during the current study is available from the corresponding authors on reasonable request.
References
Jaycock, P. et al. The Cataract National Dataset electronic multi-centre audit of 55,567 operations: Updating benchmark standards of care in the United Kingdom and internationally. Eye (London). 23, 38–49 (2009).
Ambulatory Surgery in U.S. Hospitals, 2003: HCUP Fact Book No. 9. https://archive.ahrq.gov/data/hcup/factbk9/factbk9b.htm#common. Accessed 15 May 2022.
Melles, R. B., Holladay, J. T. & Chang, W. J. Accuracy of intraocular lens calculation formulas. Ophthalmology 125, 169–178 (2018).
Sahin, A. & Hamrah, P. Clinically relevant biometry. Curr. Opin. Ophthalmol. 23, 53 (2012).
Choma, M. A., Hsu, K. & Izatt, J. A. Swept source optical coherence tomography using an all-fiber 1300-nm ring laser source. 10, 044009 (2005).
O’Donnell, C., Hartwig, A. & Radhakrishnan, H. Comparison of central corneal thickness and anterior chamber depth measured using LenStar LS900, Pentacam, and Visante AS-OCT. Cornea 31, 983–988 (2012).
Schiano-Lomoriello, D., Hoffer, K. J., Abicca, I. & Savini, G. Repeatability of automated measurements by a new anterior segment optical coherence tomographer and biometer and agreement with standard devices. Sci. Rep. 11, (2021).
Kim, K. Y., Choi, G. S., Kang, M. S. & Kim, U. S. Comparison study of the axial length measured using the new swept-source optical coherence tomography ANTERION and the partial coherence interferometry IOL Master. PLoS One 15, (2020).
Fişuş, A. D., Hirnschall, N. D. & Findl, O. Comparison of 2 swept-source optical coherence tomography-based biometry devices. J. Cataract Refract. Surg. 47, 87–92 (2021).
Tañá-Rivero, P., Aguilar-Córcoles, S., Tello-Elordi, C., Pastor-Pascual, F. & Montés-Micó, R. Agreement between 2 swept-source OCT biometers and a Scheimpflug partial coherence interferometer. J. Cataract Refract. Surg. 47, 488–495 (2021).
Tañá-Rivero, P., Aguilar-Córcoles, S., Rodríguez-Prats, J. L., Montés-Micó, R. & Ruiz-Mesa, R. Agreement of white-to-white measurements with swept-source OCT, Scheimpflug and color LED devices. Int. Ophthalmol. 41, 57–65 (2021).
Shetty, N. et al. Repeatability of biometry measured by three devices and its impact on predicted intraocular lens power. J. Cataract Refract. Surg. 47, 585–592 (2021).
Tañá-Sanz, P. et al. Agreement of predicted intraocular lens power using swept-source optical coherence tomography and partial coherence interferometry. Expert Rev. Med. Devices 18, (2021).
Yang, C. M., Lim, D. H., Kim, H. J. & Chung, T. Y. Comparison of two swept-source optical coherence tomography biometers and a partial coherence interferometer. PLoS One 14, (2019).
Barrett Universal II Formula V1.05. https://calc.apacrs.org/barrett_universal2105/. Accessed 17 August 2022.
Barrett Toric Calculator | ASCRS. https://ascrs.org/tools/barrett-toric-calculator. Accessed 17 August 2022.
Kane Formula. https://www.iolformula.com/. Accessed 17 August 2022.
Kane, J. X. & Chang, D. F. Intraocular lens power formulas, biometry, and intraoperative aberrometry: A review. Ophthalmology 128, e94–e114 (2021).
Standards & Guidance|The Royal College of Ophthalmologists. https://www.rcophth.ac.uk/standards-and-guidance/. (2021) Accessed 22 August 2022.
Acknowledgements
The authors thank Heidelberg Engineering and Haag Streit Diagnostics for the loan of the Anterion and Eyestar devices, and ARVO for the presentation of parts of this manuscript as an Annual Meeting abstract.
Author information
Authors and Affiliations
Contributions
R.L. and H.B. wrote the main manuscript text. H.B. performed the statistical analysis and R.L. prepared the figures and tables. R.G., Z.B., L.B., I.N. and S.S. operated the instruments and performed the measurements. D.M. and C.K. collected the data and performed data entry. I.C. provided the design of the study and reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Lender, R., Mirsky, D., Greenberger, R. et al. Evaluation of three biometric devices: ocular parameters and calculated intraocular lens power. Sci Rep 12, 19478 (2022). https://doi.org/10.1038/s41598-022-24017-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-24017-8
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
